
Abstract
Following injury, ligaments and tendons do not regain their normal biological and biomechanical status. This study analyzed whether an injection of human bone marrow stromal cells (BMSC) or human fibroblast in a liquid fibrin matrix influences the histological results, ultrastructural morphology, mRNA expression of essential extracellular matrix proteins, and material properties of the healing tissue. Standardized full-thickness, full-length defects of the central portion of patellar tendons were created in 96 immunodeficient rats, and filled with human BMSC in a fibrin matrix (BMSC group), human fibroblasts in a fibrin matrix (fibroblast group), or fibrin matrix only (matrix group), or left untreated (defect group). Histological sections revealed more mature tissue formation with more regular patterns of cell distribution in the BMSC group, without signs of ectopic tissue formation into bone or cartilage. Mean collagen fibril diameter and relative area covered by collagen fibrils were significantly higher at 10 and 20 days postoperatively in the BMSC group compared to the defect and matrix groups, and comparable to normal tendon tissue. Further, collagen I mRNA expression, collagen I/collagen III mRNA ratio, and Young's modulus were significantly increased at 20 days postoperatively in comparison to the defect and matrix groups. In the fibroblast group, only mean collagen fibril diameter was significantly higher compared to the defect group, whereas the other biological and biomechanical parameters were not significantly improved. This study reveals that an injection of BMSC in a liquid fibrin matrix stimulates histological, ultrastructural, molecular biologic, and biomechanical parameters of patellar tendon healing, whereas injection of fibroblasts in fibrin matrix had only minor effects on the stimulation of tendon healing.
Introduction
Bone marrow stromal cells (BMSC) are undifferentiated, pluripotent cells from the bone marrow, which are capable of differentiating into different mesenchymal tissues such as bone, cartilage, fat, muscle, tendon, and ligament tissue. Additionally, their high proliferation potential and simple acquisition by aspiration from the bone marrow make them attractive for tissue engineering applications.
The ideal matrix for delivery of BMSC has not yet been identified. The matrix should possess material properties similar to those of ligaments and tendons, that is, high ultimate stress and high Young's modulus, and allow homogenous cell/matrix distribution in vitro. However, dense matrices with the above-mentioned biomechanical properties reveal poor cell penetration.3–5 In a study by Cartmell and Dunn, the average maximal depth of penetration of rabbit allograft ligaments by fibroblasts after 14 days was 74 μm, 3 a mere 6% depth penetration if one assumes that the average radius of a rabbit anterior cruciate ligament (ACL) is 1.2 mm. 6 Considering the larger dimensions of human ligaments and tendons, one can assume a much lower relative penetration depth of cells.
Further, the matrix should facilitate safe, exact, and technically simple local application. Liquid fibrin glue may present a suitable matrix for tissue engineering of ligament and tendons. Fibrin glue can be injected into the injury site in a technically simple and minimally invasive fashion. It has the ability to carry a homogenous mixture of cells into the injury site, and can build a stable construct. Further, the fibrin glue matrix has been shown to be biocompatible and bioresorbable. 7 High vitality and proliferation of BMSC in fibrin glue in vivo and of BMSC, fibroblasts, and osteoblasts in vitro have been demonstrated.8–11 Stimulating effects on the healing process by fibrin glue itself have been described. 12 There remains a very low risk of disease transmission, since fibrin glue is derived from pooled human plasma. Constructs of cells and fibrin glue have already been successfully used in the treatment of myocardial infarction. 12
In a preliminary histological study, a homogenous mixture of BMSC in liquid fibrin matrix appeared to lead to more mature tissue formation with more regular patterns of cell distribution. 13 To the best of the our knowledge, no studies have analyzed the effects of a homogenous mixture of cells in a liquid fibrin matrix on the collagen fibril diameter, the mRNA expression of essential extracellular matrix molecules, and the biomechanical material properties for the tissue engineering of ligaments and tendons. Further, no studies have investigated whether BMSC or fibroblasts should be used for in vivo tissue engineering applications.
Therefore, this study analyzed the effect of a mixture of BMSC in liquid fibrin glue on the ultrastructural morphology (average collagen fibril diameter and relative area covered by collagen fibrils), and the relative collagen mRNA expression of collagen I, collagen III, and fibronectin. These molecules are considered to be essential to the extramolecular matrix of ligaments and tendons,14–16 and affect the material properties. An established standardized patellar window defect model was used,17–20 which eases the fixation of patella–tendon–tibia constructs in testing machines compared to clamping of small animal tendons that represent methodological challenges. 15 The use of human-derived bone marrow cells and fibrin glue in the immunodeficient animals allowed long-term vitality of the transplanted tissue constructs seeded with BMSC and progenitor cells.21–23 The ratio of collagen I to collagen III, which has been used as a marker for connective tissue maturation, was analyzed regarding their mRNA expression.15,16 Further, material properties (ultimate stress and Young's modulus) were investigated. In addition, the ultrastructural, molecular biological, and biomechanical results of constructs with BMSC were compared to those of fibroblasts derived from patellar tendons.
Materials and Methods
Acquisition, isolation, and cultivation of BMSC and fibroblasts
Bone marrow aspirates from the iliac crest were collected from six human donors undergoing dorsal or ventral instrumentation and fusion because of vertebral fractures. The donors were otherwise healthy, and their age ranged from 23 to 51 years. All procedures were approved by the institutional ethics committee, and informed consent was obtained from all donors. The specimens were isolated and cultivated according to a standardized protocol. 24 Cells of the third passage were used for the experiments.
Human patellar tendon samples were taken during reconstruction of the ACL. All patients (n = 7; age 21–40 years) had sustained a traumatic tear of the ACL. Only excess material of healthy, trimmed patellar tendon grafts was used. All procedures were approved by the institutional ethics committee, and informed consent was obtained from all donors. The tendon samples were cut into 1 mm2 pieces with a sterile scalpel. Isolation and cultivation was performed according to a protocol published previously. 25
Experimental model
Ninety-six male, immunodeficient, athymic RNU-rnu Lewis rats with a body weight of 228 ± 27 g (191–261 g) and an age of 13.2 ± 2.6 weeks (10–17 weeks) were used for the study. All operations and handling procedures were approved by the local district veterinary administration prior to the study and complied with the animal protection act. The rats were anesthetized by intraperitoneal injection of ketamine (60 mg/kg; Pfizer, Hameln, Germany) and xylocaine (12 mg/kg; Bayer, Leverkusen, Germany). Under sterile conditions, the soft tissue over the right patellar tendon was dissected via a ventral longitudinal incision. A custom-made metal template was placed over the central portion of the patellar tendon. Using the template, two parallel longitudinal incisions with a distance of 1.4 mm were made at the central portion of the patellar tendon. The central tissue between the incisions was carefully excised from the distal pole of the patella to the insertion of the tibial tuberosity. Thus, standardized full-thickness, full-length defects of the patellar tendons were created.17,18,20
The animals were randomly assigned to one of the following four groups: In the defect group, the patellar tendon window defect was left empty. In the matrix group, 10 μL fibrin glue (Tissu Duo-s; Baxter, Heidelberg, Germany) was injected without cells. In the fibroblast group and in the BMSC group, 5 μL of the thrombin component of the fibrin glue containing 105 human fibroblasts or 105 human BMSC, and 5 μL of the fibrin component were injected. After wound closure, the activity of the animals was not restricted. Since the continuity of the medial and lateral part of the patellar tendon was intact, postoperative immobilization and protection of the knee joint were not necessary. The animals were fed on an ordinary laboratory diet. Mobilization, walking pattern, and wound conditions were noted daily.
The 96 animals were killed at either 10 or 20 days postoperatively by a lethal intraperitoneal dose of Eutha 77 (Pentobarbital; Essex, Muenchen, Germany). These time points of tissue removal were chosen according to previous studies of rat mesenchymal tissue healing, where similar time intervals had been adequate.26,27
Bilateral range of motion of the knee joint was measured at the day of sacrifice. After skin incision, any signs of infection, adhesion, or macroscopic abnormalities were noted. The metal template was placed over the central portion of the patella tendon, and longitudinal incisions were made in the way described above. The uninjured medial and lateral patellar tendon tissue was excised. Only the central portion was used for further investigation. Further, 12 tissue samples of the central portion of patellar tendons were taken from the uninjured contralateral knee. Thus, a total of 108 probes resulted. Each 36 probes were used for molecular and biomechanical analyses. For molecular investigation, the patella tendon tissue of the central portion was snap frozen in liquid nitrogen and stored at −80°C. For biomechanical analysis, the central portion of the patellar tendon, including the adjacent patella and the proximal tibia, was stored at −20°C. For ultrastructural and histological analysis, the tissue of 36 probes was divided by a transverse incision into a cranial and caudal portion. The cranial portion was used for histological and the caudal portion for ultrastructural investigations.
Histological analysis
The tissue samples were fixed in 4% neutral-buffered formalin and processed through a gradient of alcohols and embedded in paraffin blocks. Eight-micrometer-thick longitudinal sections were cut, stained with hematoxylin and eosin, and analyzed with a light microscope (Zeiss, Jena, Germany) under 63×, 100×, and 200× magnification. Histological sections of the groups were compared and examined for extracellular matrix staining including ectopic tissue formation (bone and cartilage).
Ultrastructural analysis
Patellar tendon tissue was prepared according to a previously published protocol. 28 Thin transverse sections (60 nm) were cut from each tissue block and stained with uranyl acetate and lead citrate. Electron micrographs of equal-sized fibril fields within the fascicles of the tendon were obtained (20.000× final magnification) using standardized sampling criteria. 29 In four randomly chosen areas, the micrographs were analyzed by an image analysis system (SigmaScan Pro 5; SPSS, Chicago, IL) and their number, diameter, and cross-sectional area were determined. A total of 34,827 fibrils were analyzed (322.5 ± 94.9 fibrils per micrograph and 3869 fibrils per group). From the combined data, the mean collagen fibril diameter and the relative area covered by collagen fibrils were calculated.
Molecular analysis
For RNA isolation the tissue samples were chopped up and homogenized with 1 mL Trizol (Sigma, Deisenhofen, Germany) in a Polytron Homogenizer (Janke & Kunkel, Hamburg, Germany). Subsequently, 1 mL chloroform (Malinckrodt Baker, Deventer, Netherlands) was added. After centrifugation at 13,000 g at 4°C for 5 min, 600 μL isopropanol (Merck, Darmstadt, Germany) was added to the supernatant. After an incubation period of 15 min at room temperature and another centrifugation step for 30 min at 13,000 g, the pellet was washed with 500 μL 75% ethanol and dried in a SpeedVac (Concentrator 5301; Eppendorf, Hamburg, Germany) for 20 min. After addition of 10 μL diethylpropyl carbonate (DEPC)-water, the pellet was dissolved for 10 min on ice. Amount and purity of total RNA were determined in a spectrophotometer (BioPhotometer 6131; Eppendorf) at 260 and 280 nm.
cDNA was synthesized according to a standardized protocol. 24 Primers for collagen I, collagen III, and fibronectin were purchased from IBA (Göttingen, Germany). Primer sequences, PCR conditions, and quantification of mRNA expression were performed according to a protocol published previously. 24 RNA gel loading differences were normalized by GAPDH mRNA content. RT-PCR analysis of every specimen was performed twice for every gene, and the mean value used for further calculation.
Biomechanical investigations
The newly formed tendon tissue, including the adjacent patella and tibia, was thawed at room temperature and kept moist throughout the testing protocol using a buffered physiological saline solution. The tibia and patella were embedded in bronze cylinders using a cold curing methylmethacrylate resin (Technovit 4004; Heraeus Kulzer, Wehrheim, Germany). A noncontact laser micrometer was used (LDM-303H-SP; Takikawa Engineering, Tokyo, Japan) to measure the cross-sectional area for further material properties calculation. The tibia–tendon–patella complex was mounted in axial direction. While the complex was rotating axially, the width of each part of the central patellar tendon portion was measured by collimated laser beams. Finally, the cross-sectional area of the newly formed patellar tendon was determined. 6
The tibia–tendon–patella complex were mounted in a specially constructed fixture, preloaded to 0.1 N, and axially loaded to failure in displacement control at 0.1 mm/s in a materials testing machine (Model 1445; Zwick, Ulm, Germany). Surface strain was measured during elongation by tracking graphite impregnated silicon grease markers attached to the surface of the tendon using a digital video camera. Strain was analyzed using NIH ImageJ (Version 1.24o; www.rsb.info.nih.gov) software and a MultiTracker plugin (Jeffrey Kuhn: jkuhn@ccwf.cc.utexas.edu). Ultimate load and ultimate stress were determined for each specimen. Young's modulus was computed from the slope of the linear portion of the stress–elongation curve.
Results were expressed as mean values ± standard deviation. Statistical analysis to compare results between groups was carried out by multivariate analysis of variance (ANOVA), followed by univariate ANOVA and the Scheffe test (SPSS 11.5; SPSS). A p-level of 0.05 was considered to be statistically significant.
Results
Clinical examination
There was no detectable difference in the activity level of the animals in each group. Macroscopically, no signs of adhesions or inflammation or any other tissue abnormalities were noted. At the time of harvest, bilateral range of motion of the knee joint was equal.
Histological investigations
Ten days after surgery the defect group and the fibrin glue group showed high cell densities, irregular patterns of cell distribution, irregularly formed cell nucleoli with moderate matrix staining, and irregular collagen fiber orientation. Sections in the fibroblast group revealed high cell numbers with mainly spindle-shaped cells. Patellar tendon defects treated by BMSC and fibrin glue also had a more homogenous, spindle-shaped morphology (data not shown).
Twenty days postoperatively histological sections in the defect group and fibrin glue group revealed high number of cells. Collagen fibers were partially orientated parallel to the cells (Fig. 1a, b). In the fibroblast group, spindle-shaped cells were most abundant and mainly orientated parallel to the collagen fibers. Compared to uninjured patellar tendon tissue, cell density was clearly higher, and the matrix was less stained (Fig. 1c). Sections in the BMSC group demonstrated more mature tissue formation dominated by dense collagen fiber bundles. Spindle-shaped cells were orientated parallel to collagen fibers. Compared to normal patellar tendon tissue, matrix staining was less intense, and cell density was higher (Fig. 1d, e).
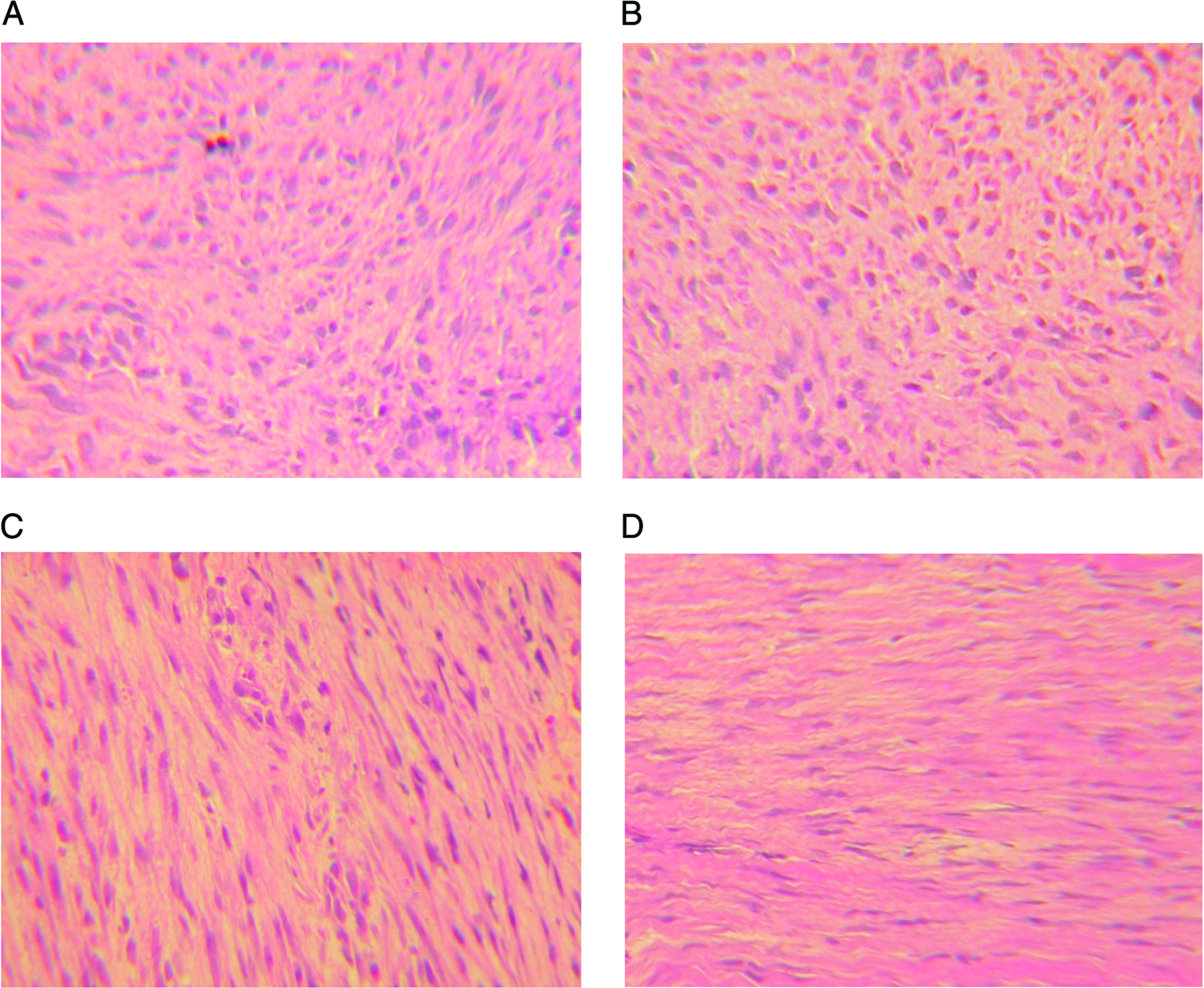
Histological sections (hematoxylin and eosin staining) 20 days after surgery, 63 × magnification. (
No ectopic bone or cartilage tissue formation was observed after 10 and 20 days in any group.
Ultrastructural analysis
Ten days postoperatively, mean collagen fibril diameter was 70.1 ± 16.5 nm in the defect group and 96.6 ± 10.1 nm in the matrix group (p = 0.074). In contrast, injection of BMSC in a liquid fibrin matrix significantly increased collagen fibril diameter to 130.1 ± 10.1 nm (p < 0.001 and p = 0.022 compared to the defect and matrix group). In the fibroblast group, collagen fibril diameter was significantly higher in comparison to the defect group (p = 0.004), but not in comparison to the matrix group (p = 0.591). The mean collagen fibril diameter did not differ significantly in the BMSC group compared to healthy patellar tendon tissue at 10 days after surgery (154.4 ± 7.6 nm; p = 0.093). In relation to healthy tendons, mean fibril diameter in the defect group was 45.4%, in the fibrin group 62.6%, in the fibroblast group 71.2%, and in the BMSC group 84.3% (Figs. 2 and 4).
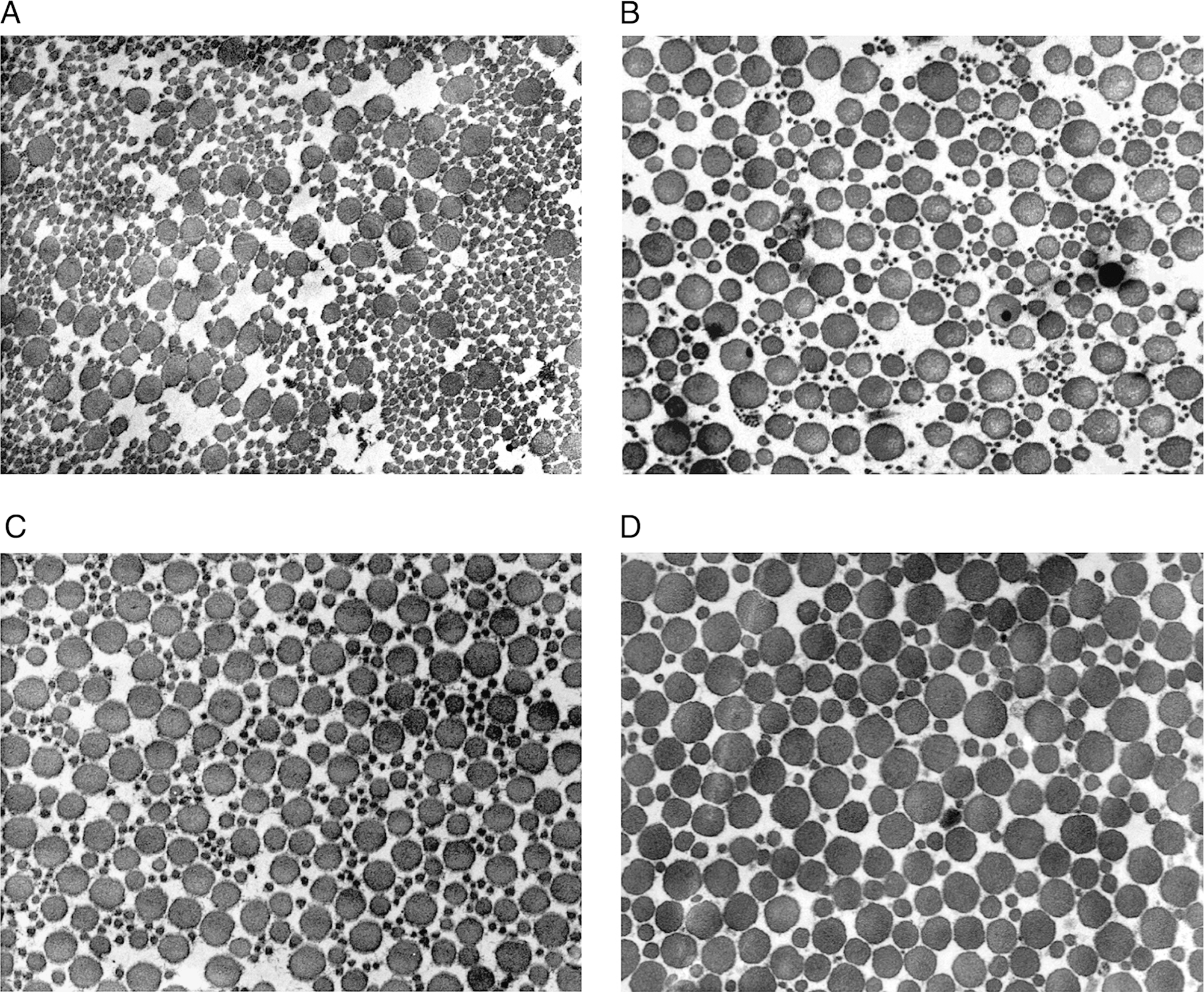
Ultrastructural analysis of standardized full-thickness, full-length defects of the central portion of rat patellar tendons after 10 days. (
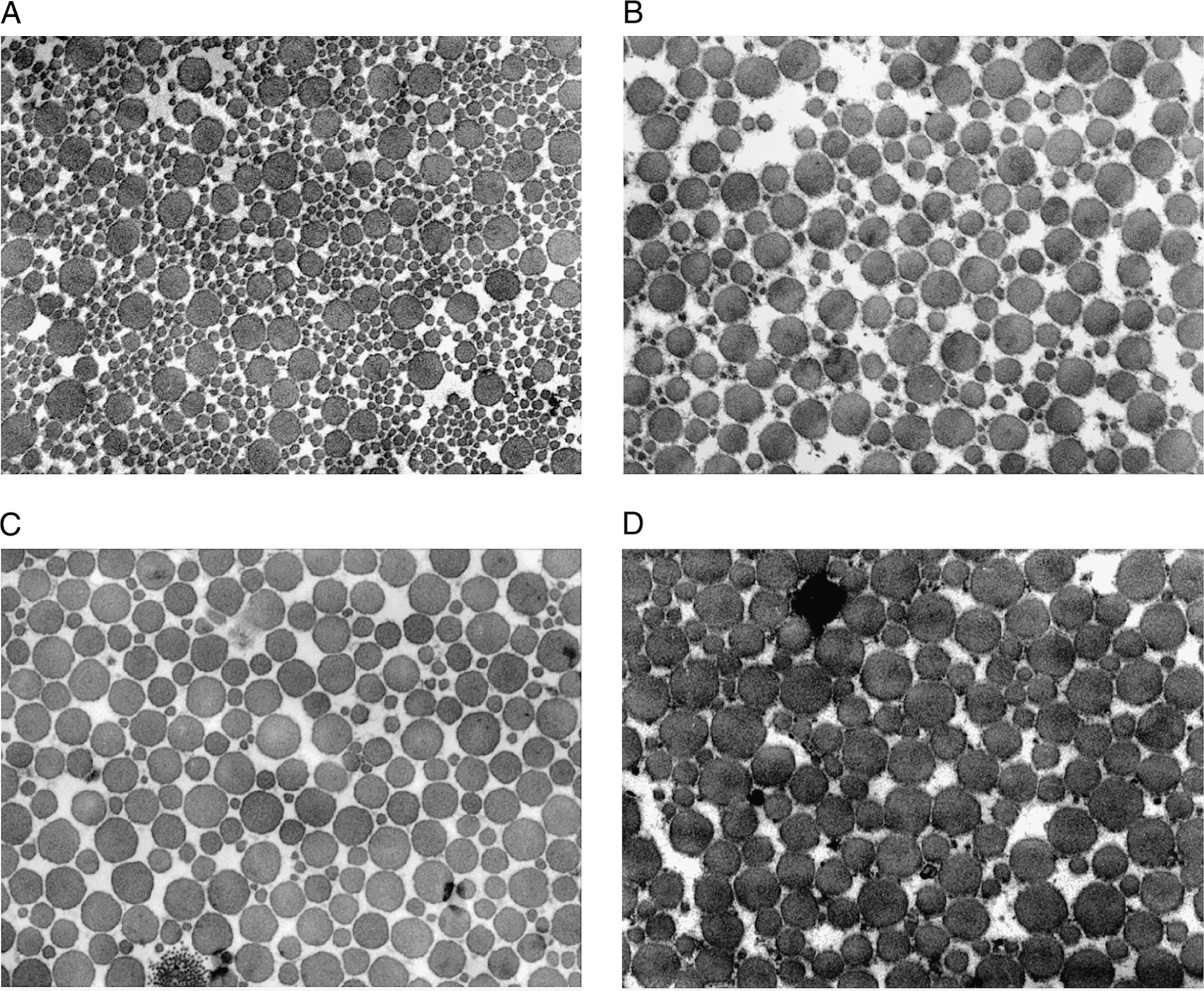
Ultrastructural analysis of standardized full-thickness, full-length defects of the central portion of rat patellar tendons after 20 days. (
Twenty days after surgery, the average collagen fibril diameter increased in all groups. In the BMSC group, an average diameter of 139.9 ± 9.6 nm was determined, which was significantly higher than in the defect and matrix group (p < 0.001 and p = 0.002). In the fibroblast group, significant difference was only detected compared to the defect group (p = 0.044). Average fibril diameter in the BMSC group was 20.7% higher in the BMSC group than in the fibroblast group, without reaching statistical significance (p = 0.059). Fibril diameter in the BMSC group did not differ from healthy tendon tissue (p = 0.407) (Figs. 3 and 4).
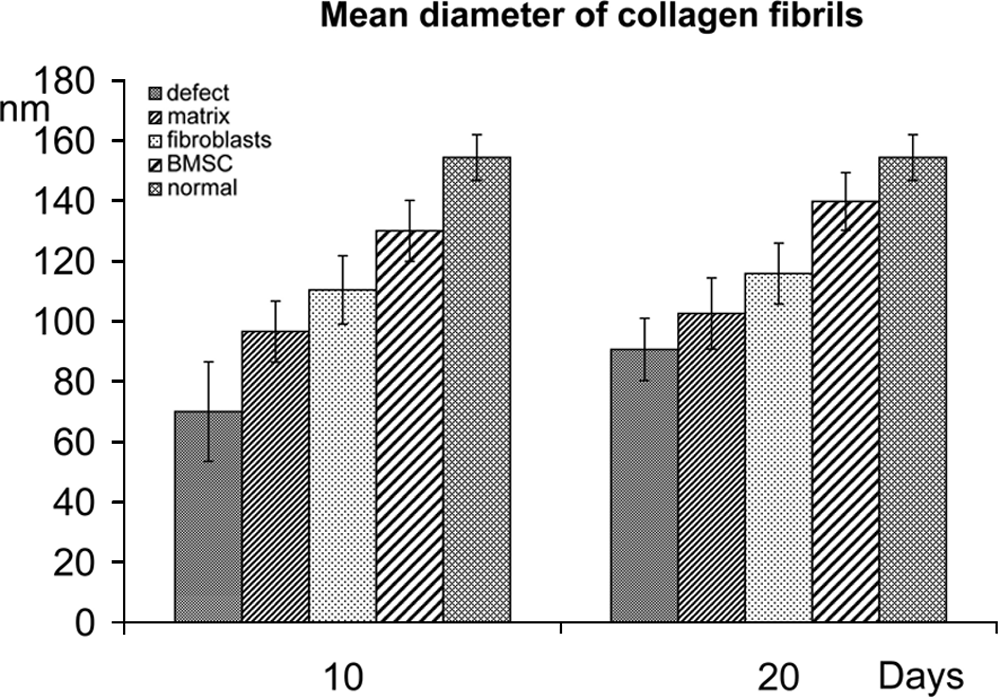
Mean collagen fibril diameter in standardized full-thickness, full-length defects of the central portion of rat patellar tendons ± standard deviation (analysis of a total of 34,827 collagen fibrils). Significant differences on day 10: defect–fibroblast (p = 0.004), defect–BMSC (p < 0.001), defect–normal (p < 0.001), matrix–BMSC (p = 0.022), matrix–normal (p < 0.001), and fibroblast–normal (p = 0.002). Significant differences on day 20: defect–fibroblast (p = 0.044), defect–BMSC (p < 0.001), defect–normal (p < 0.001), matrix–BMSC (p = 0.002), matrix–normal (p < 0.001), and fibroblast–normal (p = 0.002).
The relative area covered by collagen fibrils was between 31.8% and 42.5% in the defect, matrix, and fibroblast group on day 10. In contrast, the area covered by fibrils measured 53.1 ± 5.0% in the BMSC group, which was significantly higher than in the defect (p < 0.001) and fibroblast group (p = 0.018). The value for uninjured patellar tendon was 59.8% and only 12.1% higher compared to the BMSC group (p = 0.448). Twenty days postoperatively, the relative area covered by collagen fibrils increased in all groups, and was higher in the BMSC group in comparison to the defect group (p < 0.001) and matrix group (p = 0.002). Values of the BMSC group and uninjured tissue were on a comparable level. In contrast to the BMSC group, area coverage in the fibroblast group was significantly lower in comparison to uninjured tendon tissue (p = 0.002) (Fig. 5).
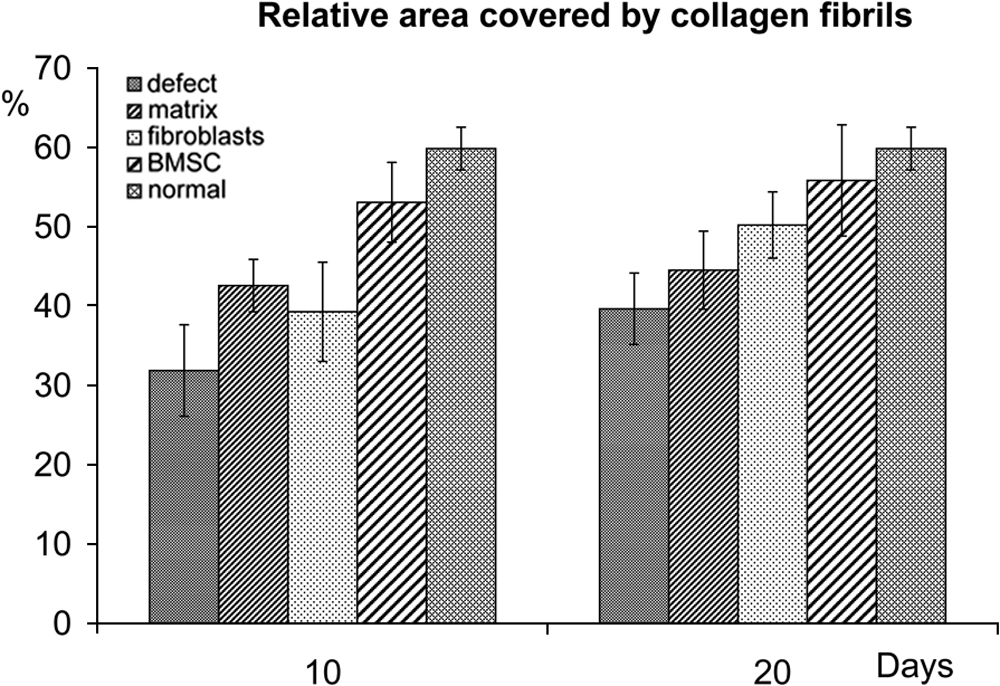
Relative area covered by collagen fibrils in standardized full-thickness, full-length defects of the central portion of rat patellar tendons ± standard deviation (analysis of a total of 34,827 collagen fibrils). Significant differences on day 10: defect–BMSC (p < 0.001), defect–normal (p < 0.001), matrix–normal (p = 0.003), fibroblast–BMSC (p = 0.018), and fibroblast–normal (p = 0.001). Significant differences on day 20: defect–BMSC (p =0.008), defect–normal (p = 0.001), and matrix–BMSC (p = 0.009).
Molecular analysis
Collagen I mRNA was detectable in all groups at all time points. On day 10, collagen I mRNA expression was 69.4% higher in the matrix group than in the defect group. Compared to the matrix group, mRNA level in the fibroblast group and BMSC group increased by 27.7% and 60.2%, respectively. Significant differences were detected between the defect group and BMSC group (p = 0.033), and between the defect group and normal patellar tendon tissue (p = 0.015). On day 20, collagen I mRNA expression level increased by 15.9% in the fibroblast group, and by 14.3% in the BMSC group. In comparison to the normal patellar tendon tissue, the BMSC group revealed 6.3% higher collagen I mRNA levels. The mRNA level for collagen I in the defect group and matrix group were significantly lower than in the BMSC group (p = 0.008 and p = 0.045) (Fig. 6).
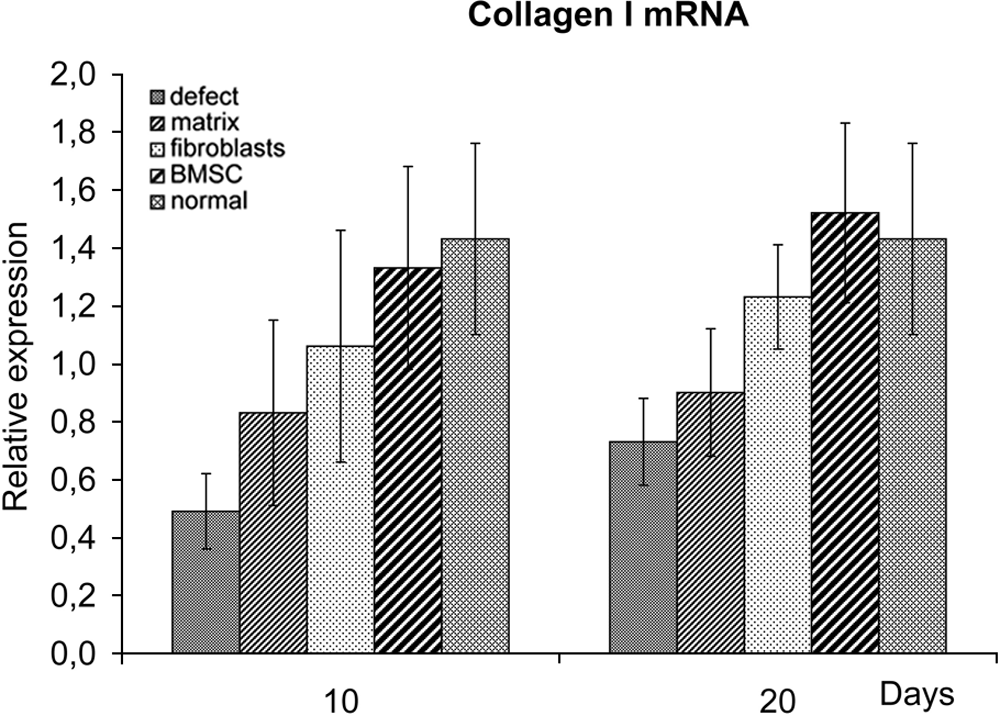
Relative expression of collagen I mRNA in standardized defects of the central portion of rat patellar tendons ±standard deviation. Significant differences on day 10: defect–BMSC (p = 0.033) and defect–normal (p = 0.015). Significant differences on day 20: defect–BMSC (p = 0.008), defect–normal (p = 0.021), and matrix–BMSC (p = 0.045).
In the defect group and matrix group, collagen III mRNA expression was, respectively, 9.7% and 71.0% higher on day 10, and 33.3% and 66.4% higher on day 20 compared to the BMSC group. Uninjured tendons demonstrated the lowest expression of collagen III mRNA. However, the differences were not statistically significant (data not shown).
The ratio of collagen I/collagen III mRNA was the lowest in the defect group and matrix group on day 10. In the fibroblast group 2.52 and 2.41 higher expression ratio, and in the BMSC group 2.96 and 2.84 higher amounts of collagen I/collagen III mRNA were detected. Due to the high variability observed in the data, no significant differences in the ratio between the BMSC group were detected when compared to the defect group and matrix group (p = 0.112 and p = 0.126). In normal tendon tissue, the highest collagen I/collagen III mRNA ratio was noted, which was significantly different compared to the defect group and matrix group (p = 0.002 for both). On day 20, collagen I/collagen III mRNA ratio was similar in the defect group and matrix group. In the BMSC group, the amount increased by 39.6%, and was 62.4% higher than in the fibroblast group (p = 0.092). Compared to normal tendon tissue, the ratio was only 8.2% lower in the BMSC group. Significant differences were noted between the defect group and BMSC group (p = 0.002), matrix group and BMSC group (p = 0.002), and between the defect, matrix, and fibroblast groups compared to normal tendon tissue (p = 0.001, p = 0.001, and p = 0.027) (Fig. 7).
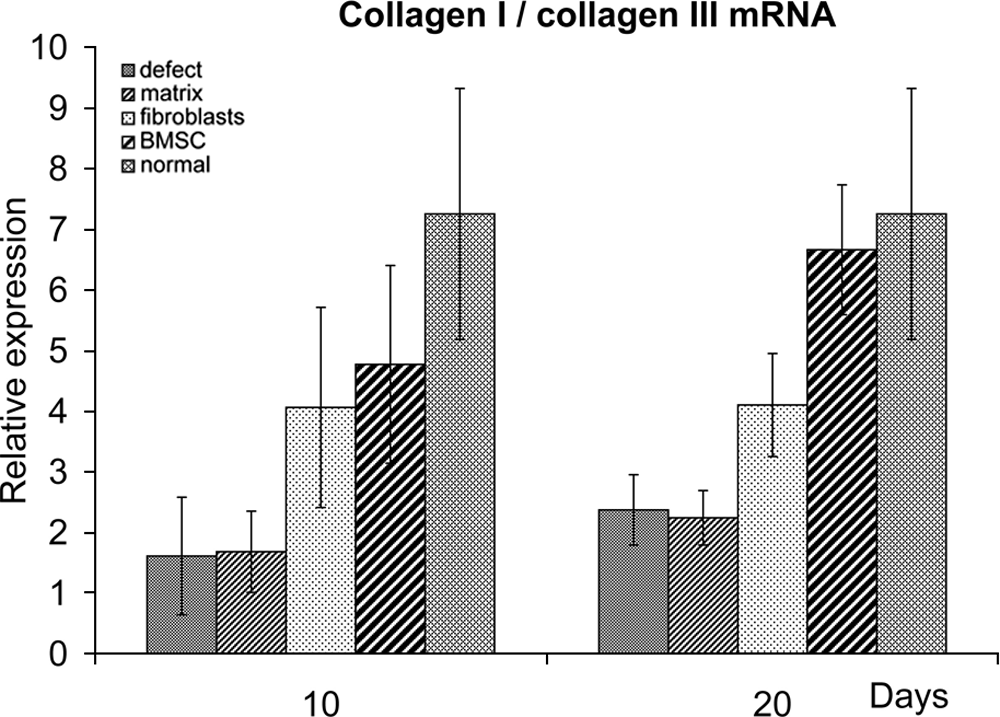
Ratio of relative mRNA expression of collagen I/collagen III in standardized defects of the central portion of rat patellar tendons ± standard deviation. Significant differences on day 10: defect–normal (p = 0.002) and matrix–normal (p = 0.002). Significant differences on day 20: defect–BMSC (p = 0.002), defect–normal (p = 0.001), matrix–BMSC (p = 0.002), matrix–normal (p = 0.001), and fibroblast–normal (p = 0.027).
Analysis of the fibronectin mRNA expression revealed similar levels in all groups on days 10 and 20. Slightly higher values were found at both time points in the fibroblast group, without reaching significant levels (data not shown).
Biomechanical analysis
On postoperative day 10, the ultimate stress was 5.86, 4.96, and 4.19 times lower in the defect, matrix, and fibroblast groups, respectively, compared to normal tendon tissue (p < 0.001 for all). In the BMSC group, ultimate stress differed from normal tissue by a factor of 2.68 (p < 0.001). On postoperative day 20, the ultimate stress increased in all groups. The ultimate stress for the BMSC group was 2.00-fold higher than the defect group (p = 0.088) and 2.19-fold higher than the matrix group (p = 0.057). Ultimate stress of normal tendons was still significantly higher than the defect, matrix, fibroblast, and the BMSC groups (p < 0.001 for all). In the BMSC group the ultimate stress on average was 51.5% of the normal tendons (Fig. 8).
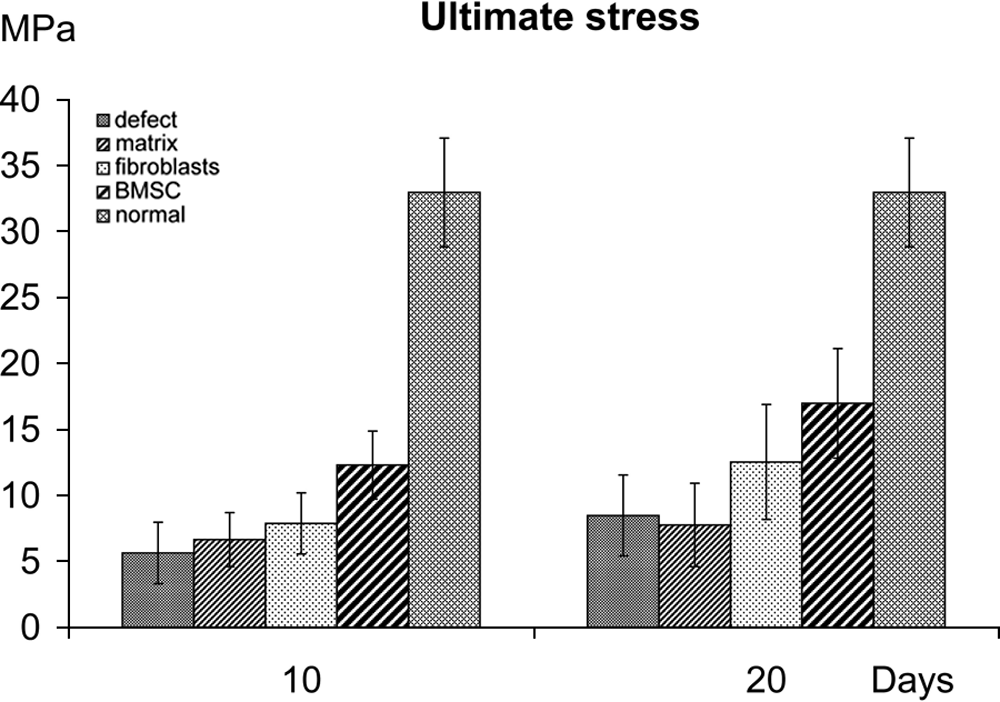
Ultimate stress of standardized defects of the central portion of rat patellar tendons ± standard deviation. Significant differences on day 10: defect–normal (p < 0.001), matrix–normal (p < 0.001), fibroblast–normal (p < 0.001), and BMSC–normal (p < 0.001). Significant differences on day 20: defect–normal (p < 0.001), matrix–normal (p < 0.001), fibroblast–normal (p < 0.001), and BMSC–normal (p = 0.001).
Young's modulus measured 57.2 ± 26.1 MPa in the defect group 10 days postoperatively, corresponding to 19.7% of the value of normal tendons, whereas in the BMSC group this was 106.7 ± 37.6 MPa, corresponding to 36.7% of the normal tendon. On day 10, the differences compared to normal tendons were highly significant in all groups. Twenty days after surgery, an increase of Young's modulus was observed in all groups. Whereas in the defect group Young's modulus measured 76.3 ± 29.3 MPa, which was similar to the matrix group (79.6 ± 23.2 MPa), and the modulus in the fibroblast group and BMSC group raised to 108.2 ± 26.8 MPa and 186.3 ± 31.4 MPa, respectively. Compared to the defect group and matrix group, the modulus in the BMSC group differed by a factor of 2.44 and 2.34 (p = 0.007 and p = 0.009). However, the modulus was 37.3% of the average value calculated for the normal tendon tissue in the fibroblast group (p < 0.001) and 64.2% in the BMSC group (p = 0.011) (Fig. 9).
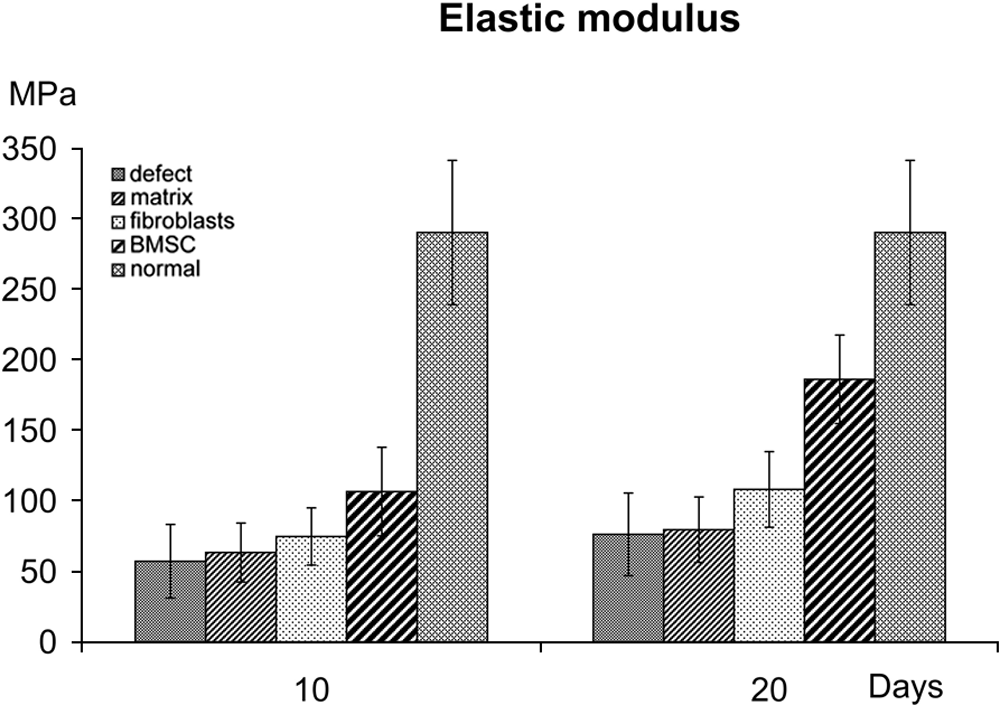
Young's modulus of standardized defects of the central portion of rat patellar tendons ± standard deviation. Significant differences on day 10: defect–normal (p < 0.001), matrix–normal (p < 0.001), fibroblast–normal (p < 0.001), and BMSC–normal (p < 0.001). Significant differences on day 20: defect–BMSC (p = 0.007), defect–normal (p < 0.001), matrix–BMSC (p = 0.009), matrix–normal (p < 0.001), fibroblast–normal (p < 0.001), and BMSC–normal (p = 0.011).
Discussion
Injured tendon and ligament tissue undergo a complex repair process. However, the material properties of healed tendon and ligament, especially when treated nonoperatively, can at maximum approach one-half of the uninjured tissue.17,18,20,30 This relates to the impaired ultrastructure of the repair tissue and the changed morphology of the macromolecules. Namely, the collagen fibers are less organized and suboptimally crosslinked,17,20 and have a relative increase in the number of small diameter collagen III and decrease of larger collagen I fibrils resulting in decreased mean collagen fibril diameter and relative area covered by collagen fibrils.16,31,32 Although tissue engineering has brought promising possibilities for enhancement of long bone and cartilage defects,1,2 the clinical application of tissue engineering for ligament and tendon repair still remains in its infancy.
To the best of the author's knowledge, no studies have analyzed collagen fibril diameter and relative area covered by collagen fibrils in animal studies of tissue engineering approaches in ligament and tendon healing so far. In a gentherapeutic approach with antisense decorin, collagen fibril diameter increased in rabbit medial collateral ligaments by 37% after 4 weeks. 32 In the author's study, collagen fibril diameter increased by 54% 20 days after treatment with BMSC in fibrin matrix compared to the untreated defect group. Collagen fibril diameters in BMSC treated and uninjured patellar tendon tissues were comparable. These findings correlate with the molecular biological findings. Collagen I was associated with larger fibrils than collagen III, 33 and in the BMSC group, significantly higher levels of collagen I mRNA and higher quotient of collagen I/collagen III were noted compared to the defect group and matrix group 20 days after surgery.
Whereas no molecular biological investigations of tendons or ligaments of in vivo tissue engineering approaches have been published, several studies have reported about histological and immunohistological results of tissue-engineered ligaments or tendons.17–19,34,35 Most studies revealed more mature tissue formation after application of matrices with BMSC. Ouyang et al. filled an Achilles tendon defect of rabbits with allogenic BMSC and a matrix of PLGA and fibrin glue. Immunohistological studies revealed an increase of positive staining for collagen I and collagen III on day 14 postoperatively. 36 Two recent studies used pluripotent cells in fibrin matrix for the treatment of collagenase-induced tendinitis. Crovace et al. treated collagenase-induced tendinitis in an equine model with a mixture of bone marrow mononucleated cells and fibrin glue, and noted increased type I and decreased type III collagen synthesis in comparison to treatment with fibrin glue or saline only. The results of bone marrow mononucleated cells were similar to those of cultured BMSC. 37
One main concern of BMSC transplantation is ectopic tissue differentiation into bone, which was described in a study by Dressler et al., investigating constructs of collagen gel and BMSC in a patellar tendon defects. 38 Ectopic tissue differentiation was not detected in histological sections of our study. One explanation can be different cell culture conditions.3,5,14,24 Another explanation might be that Dressler et al. created bony defects in the adjacent bones with an oscillating saw, so that scattered bone tissue might have induced bone formation. Dressler et al. themselves discussed whether marked contraction of the collagen gel in vitro before implantation might have influenced tissue differentiation. 38
Improvement of structural properties by tissue engineering approaches can be caused by increased tissue diameter. Therefore, exact analysis of tissue diameter is essential; however, it is demanding in small animals. In our study, noncontact laser analysis was used to determine cross-sectional soft tissue areas, which is highly accurate and avoids the influence of confounding variables. Some of the inaccuracies of the conventional cross-sectional area analysis such as the influence of irregular tendon diameter and unpredictable tissue deformation during measurements are eliminated. 6 A significant increase of Young's modulus was detected in the BMSC group in relation to the defect group and matrix group. Ultimate stress increased by a factor 2.0 and 2.2 compared to the defect group and matrix group, respectively. Despite this trend, the data were not statistically significant with the chosen number of samples. Although material properties were not recovered in the BMSC group, ultimate stress and Young's modulus measured 51.5% and 64.2% 20 days after surgery, compared to normal tendon tissue.
Musahl et al. augmented a defect of the medial collateral ligament of the knee with an acellular, xenogenic graft. After 12 weeks, ultimate stress was 54% and Young's modulus 54% higher than untreated defects. Compared to uninjured ligaments, ultimate stress was 21% and Young's modulus 30% of normal tendon tissue. 30 Rabbit patellar tendon defects, filled with biomechanically stimulated constructs of collagen gel and BMSC, increased maximum stress and Young's modulus by 54% and 80% at 26 weeks postoperatively. However, compared to healthy tendon tissue, ultimate stress was 28% and Young's modulus 27%. 17 In an Achilles tendon defect model of dogs, biomechanically stimulated constructs of collagen gel and BMSC increased maximum stress by 37% and Young's modulus by 34% 12 weeks postoperatively. 34 Ouyang et al. seeded PLGA matrices with allogenic BMSC and fibrin glue, which were implanted into an Achilles tendon defect of rabbits. Twelve weeks postoperatively, Young's modulus was 63% of uninjured tendons, whereas matrices without cells revealed a Young's modulus of 53%. 36 In conclusion, the results of our study compare favorably to the results after augmentation of ligament defects with acellularized porcine tissue and biomechanically stimulated collagen–BMSC constructs, and BMSC-seeded PLGA matrices.17,30,34,36
The method by which BMSC achieve their biological stimulation of the repair process in connective tissue is not well known. It is possible that local growth factors produced as a result of injury lead to differentiation of BMSC into fibroblasts. Although there was a tendency that injection of mature fibroblasts in fibrin glue improved the repair process, the BMSC group achieved superior results in terms of molecular biological markers and in terms of Young's modulus after 20 days. Hence, it is likely that BMSC play a more important role than purely acting as a source for repair cells. For example, these cells are demonstrated to respond to external mechanical forces by increasing their biological throughput of collagen I, collagen III, and tenascin-C mRNA. 14
The current study is not without limitations. First, BMSC were derived from six different donors (23–52 years). To minimize variability of the surgical procedure, all animals were operated by a single surgeon. Since the number of BMSC declines dramatically with aging of the cells, 38 only BMSC of the third passage were used in all 96 animals. For logistical reasons, not all animals could be operated in a short period of time by a single surgeon with BMSC of the third passage from one donor. However, all BMSC had been derived from bone marrow aspirates from the iliac crest of adult healthy human donors with isolated vertebral fractures. Patients with any other diseases or injuries were excluded from the study. Second, the authors used human cells in immunodeficient animals. Viability of human cells in immunodeficient rats had been demonstrated in studies by Grinnemo et al. and Kawamoto et al.22,23 Human BMSC remain viable and proliferate in human fibrin glue in vivo and in vitro.10,12 Further, human BMSC are easy to harvest by puncture of the iliac crest. In contrast, autologous rat bone marrow aspiration and isolation cultivation can be challenging.
Some aspects deserve further investigation. It is unknown whether regeneration of tendon was due to differentiation of human BMSC into fibroblasts in the defects, or it is simply due to the paracrine effects of BMSC. Further, it remains unclear if cells of recipient origin migrate to the defect sites in the BMSC group, and if so, how these cells interact with human BMSC. Another interesting aspect of tendon and ligament healing is analysis of three-dimensional ultrastructure of tendon and ligament fibers. Within one collagen fiber, the fibrils are orientated not only longitudinally but also transversely and horizontally, since they are exposed not only to longitudinal but also to transversal and rotational forces. The current study focused on the axial ultrastructural findings with analysis of more than 30000 collagen fibril diameters. Evaluation of complex three-dimensional ultrastructure of healing tendons and ligaments is beyond the scope of these investigations, but is of interest in future studies.
This study revealed several important findings. First, this study provides a comprehensive analysis of an in vivo study of tissue engineering of tendons. Human-derived BMSC in liquid fibrin matrix enhanced molecular biological, ultrastructural, and biomechanical parameters of tendon healing. Another important finding of this study was that BMSC were more effective than mature fibroblasts in the biological stimulation of repair tissue. In conclusion, injection of BMSC in liquid fibrin matrix seems to be a promising approach to improve the complex process of tendon healing.
Footnotes
Disclosure
No benefit in any form has been or will be received from commercial parties related directly or indirectly to the subject of this article.