
Abstract
Myelomeningocele (MMC) is a common and devastating malformation. As an alternative to fetal surgical repair, tissue engineering has the potential to provide a less invasive approach for tissue coverage applicable at an earlier stage of gestation. We have previously evaluated the use of gelatin hydrogel composites composed of gelatin sponges and sheets as a platform for tissue coverage of the MMC defect in the retinoic acid induced fetal rat model of MMC. In the current study, we compare our previous composite with gelatin microspheres as a scaffold for tissue ingrowth and cellular adhesion within the amniotic fluid environment. We also examine the relative efficacy of various bioactive protein coatings on the adhesion of amniotic fluid cells to the construct within the amniotic cavity. We conclude from this study that gelatin microspheres are as effective as gelatin sponges as a scaffold for cellular ingrowth and amniotic fluid cell adhesion and that collagen type I and fibronectin coatings enhance amniotic fluid cell adhesion to the gelatin-based scaffolds. These findings support the potential for the development of a tissue-engineered injectable scaffold that could be applied by ultrasound-guided injection, much earlier and less invasively than sponge or sheet-based composites.
Introduction
Toward that goal, we are investigating tissue engineering techniques to achieve tissue coverage of the MMC defect. We have previously described the use of gelatin hydrogel composites constructed by combining a gelatin sheet and a gelatin sponge. Application of the composite to the MMC defect in the rat model of retinoic acid (RA)-induced MMC resulted in the induction of epidermal ingrowth underneath the gelatin sponges, and cellular adhesion over the gelatin sheet with associated deposition of extracellular matrix (ECM). 10 Gelatin hydrogel engineered as shaped sheets or sponges appeared to be an effective scaffold in the unique amniotic fluid-filled intrauterine environment and may be amenable to fetoscopic application. However, an injectable scaffold would be much less invasive and could potentially be applied much earlier in gestation under ultrasound guidance maximizing the preservation of neural elements. 11
The objective of this study was to evaluate whether gelatin microspheres could provide an injectable scaffold with the same properties as the previously described gelatin sponge and sheet composite supporting epidermal ingrowth and cellular adherence over the MMC defect. We also examine whether bioactive proteins present in the ECM can enhance cellular adhesion to the scaffold.
Materials and Methods
Biomaterials
Gelatin with an isoelectric point of 5.0 (Mw = 99,000 Da), prepared through alkaline processing of bovine bone, was kindly supplied by Nitta Gelatin Co. The bioactive proteins used in this study were the following: collagen type I (BD Biosciences); collagen type IV (Sigma-Aldrich); fibronectin (EMD Chemical); laminin (Invitrogen).
Preparation of gelatin sponges
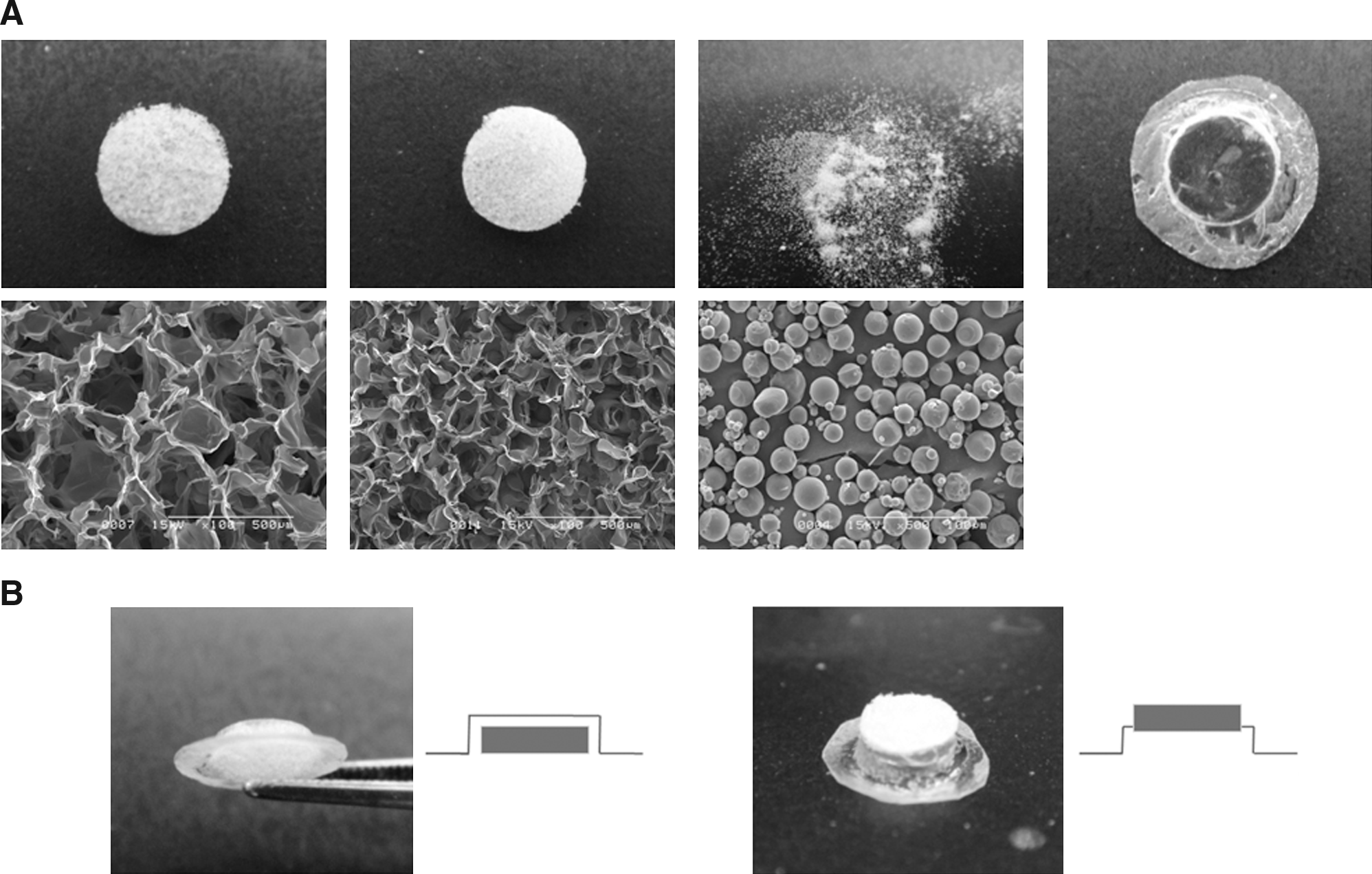
Gelatin sponges, microspheres, and sheets were prepared by dehydrothermal crosslinking of gelatin prepared as previously described.10,12–14 For the gelatin sponge preparation, a 3 or 7 w/v% gelatin aqueous solution was agitated at 5000 rpm for 3 min with a homogenizer (Auto cell master CM-2000; AS ONE Co.) at room temperature, followed by casting into a 60 × 60 cm2 polypropylene dish. The homogenized solution was frozen in liquid nitrogen for 20 s, frozen at −20°C for 12 h, and freeze-dried (TF5-85ATANN; Takara Co.). The frozen gelatin sponges were dehydrothermally crosslinked at 160°C for 12 h in a vacuum drying oven (DN-30S; Sato Vac, Inc.). The crosslinked gelatin sponges were punched out to obtain discs of 1 mm thickness and 3.5 mm diameter and sterilized with ethylene oxide gas (EOG) (EOG sterilizer SA-160; ELK Co.) (Fig. 1A).
Preparation of the gelatin scaffolds. (
Preparation of gelatin microspheres
Gelatin microspheres were prepared as previously described. 15 Briefly, 20 mL of 10 wt% gelatin solution preheated at 40°C for 1 h was added drop wise into 600 mL of olive oil while stirring at 400 rpm for 10 min at 40°C to prepare a water-in-oil emulsion. The emulsion was cooled to 0°C, and stirring was continued for 30 min to complete the gelation of the gelatin in the water phase. After addition of 200 mL of acetone, the emulsion was further stirred at 200 rpm for 15 min. The resulting microspheres were washed four times with acetone, collected by centrifugation (5000 rpm, for 5 min, at 4°C), and suspended in acetone. The microspheres were put through a sieve with an aperture of 32 or 20 μm, followed by air-drying at 4°C to obtain noncrosslinked gelatin microspheres. Microspheres were then put into a vacuum drying oven at 160°C for 24 h and sterilized with EOG (Fig. 1A).
Preparation of gelatin sheets
Hat-shaped gelatin sheets were prepared for the in vivo experiments as previously described. 10 Briefly, a 5 w/v% solution of gelatin solution was poured between a bicomponent mold, with corresponding elevated and recessed areas. The filled molds were kept in a refrigerator at 4°C until the gelatin solution was completely air dried. The molded gelatin was peeled off of the cast and put into a vacuum drying oven at 160°C for 24 h for crosslinking. The resulting product was harvested by cutting around each of the sheets to form 36 individual gelatin sheets that corresponded to the shape of the MMC defect. The sheets were sterilized with EOG. When epidermal ingrowth underneath the gelatin scaffolds was examined, the gelatin sponges or microspheres were put into the concave space of the hat-shaped gelatin sheet to prepare a gelatin composite. When cell adhesion onto the gelatin scaffolds was examined, gelatin sponges or microspheres were glued on the outside of gelatin sheets with cyanoacrylate adhesive (Instant KRAZY GLUE; Krazy Glue) (Fig. 1B).
For the in vitro cell proliferation experiment, flat gelatin sheets were prepared. A 5 w/v% of gelatin solution (5 mL) was poured into a 100 × 100 cm2 polypropylene dish and kept in a refrigerator at 4°C until the gelatin solution was completely air-dried. The dried gelatin was peeled off of the cast and put into a vacuum drying oven at 160°C for 24 h for crosslinking. The crosslinked gelatin sheet was punched out to obtain 15-mm-diameter round sheets to fit a 24-well dish. The sheets were sterilized with EOG.
Coating of gelatin sheets with bioactive proteins
Aqueous solutions of collagen type I, collagen type IV, fibronectin, and laminin or phosphate-buffered saline (PBS, pH 7.4) control (1 mg/mL, 50 μL) were applied to crosslinked dry gelatin sheets and left overnight at room temperature to allow complete absorption. The gelatin sheets coated with proteins were used without PBS washing.
Estimation of in vitro degradation of gelatin scaffolds
Gelatin sponges or microspheres (10 mg) were put into 2 mL tubes with 750 μL of distilled water to allow them to swell for 12 h, and then 750 μL of 2N hydrochloric acid was added. At different time intervals, 200 μL of solution was sampled and 200 μL of fresh 1N hydrochloric acid was added. The absorbance of solution of samples was measured at a wave length of 260 nm by a UV-vis spectrophotometer (Beckman Coulter, Inc.) to estimate the amount of gelatin degraded.
In vitro cell culture on gelatin sheets coated with bioactive proteins
Rat fetal fibroblasts were used as a cell source. Briefly, after euthanasia, fetal skin was sterilely dissected from fetal rats and placed on 10 cm culture dishes (Corning, Inc.). After the skins became relatively dried and adherent to the culture dish, Dulbecco's modified Eagle's medium (Gibco) supplemented with 10% fetal bovine serum (Gemini Bio) and 1% penicillin–streptomycin (Cellgro) was added, and they were incubated in 5% carbon dioxide (CO2) at 37°C. Fibroblasts started growing on around 7–10 days after harvest and the skins were removed at 14 days. Fibroblasts were expanded in culture and collected after two passages for use. Fifteen-millimeter round gelatin sheets coated with bioactive proteins were placed in 24-well dishes and 4 × 104 fibroblasts were placed on each gelatin sheet. Four samples were prepared per each group. At serial time points gelatin sheets were sampled and the viability of adherent cells on the scaffolds was measured by the methylthiazol tetrazolium (MTT)-based colorimetric assay kit according to its instructions (Cell Proliferation Kit I; Roche; MTT labeling reagent 10 μL, solubilization solution 100 μL, 650 nm wavelength).
Animal experiments
All experimental protocols were approved by the Institutional Animal Care and Use Committee at The Children's Hospital of Philadelphia or the Committee on Animal Care and Use at Kyoto University and followed guidelines set forth in the National Institutes of Health Guide for Care and Use of Laboratory Animals.
MMC defects in fetal rats were created based on the protocol described previously.10,11 Briefly, time-dated Sprague-Dawley rats (Charles River Laboratories or Shimizu Laboratory Supplies Co.) were used for this study. After a brief exposure to isoflurane (Abbott Lab), pregnant rats were fed 50 mg/kg of all-trans RA (Sigma-Aldrich) dissolved in olive oil (10 mg/mL) at embryonic day 10 (E10).
Organ culture of fetal rat MMC
RA-exposed Sprague-Dawley dams were euthanized by CO2 inhalation followed by cervical dislocation at E22. The fetuses with MMC were harvested, and the MMC lesion and surrounding tissues were dissected. The gelatin scaffolds were applied over the MMC and fixed with a cyanoacrylate adhesive between the scaffold edge and surrounding skin. The MMC explants were cultured in six-well plates with Dulbecco's modified Eagle's medium supplemented with 10% fetal bovine serum and 1% penicillin–streptomycin with 5% CO2 at 37°C for 7 days. There were four experimental groups: Group A—the MMC covered with gelatin sponge prepared from 3 w/v% gelatin solution and 12 h dehydrothermal crosslinking; Group B—the MMC covered with the gelatin sponge prepared from 7 w/v% gelatin solution and 12 h dehydrothermal crosslinking; Group C—the MMC covered with gelatin microspheres prepared from 10 w/v% gelatin solution and 24 h dehydrothermal crosslinking; Group D—the MMC covered with the gelatin sheet prepared from 5 w/v% gelatin solution as a control.
Surgical procedure
RA-exposed Sprague-Dawley dams were anesthetized at E18 with inhaled isoflurane. The uterine horns were exposed through a maternal midline laparotomy. The uterine wall and amniotic membrane were sutured with a 6-0 polypropylene purse string suture (PDS-II; ETHICON). The back of each fetus was exposed through a small hysterotomy created within the purse string and a gelatin sheet or composite was applied over the MMC area. The edge of the gelatin sheet was spot glued with a cyanoacrylate adhesive for better adhesion. After the gelatin was securely fixed, the fetus was returned into the uterus. The amniotic fluid was replaced with sterile normal saline and the hysterotomy was closed with the purse-string suture. The uterus was returned to the abdomen and the incision closed in two layers with a 4-0 Vicryl running suture (ETHICON). Four fetuses with MMC per dam were manipulated. Dams were euthanized by CO2 inhalation followed by cervical dislocation at E22 and the fetuses were harvested by cesarean section. Analysis was dependent upon the experimental groups. Groups A, C, and D had constructs applied as described for the in vitro MMC organ culture above and underwent analysis for epidermal ingrowth and cellular adhesion. MMCs that were covered with gelatin sheets coated with bioactive proteins (collagen type I, collagen type IV, fibronectin, laminin, and PBS control) were assessed for cellular adhesion alone.
Histological analysis
Cultured MMC explants and operated whole fetuses were fixed in 10% neutral buffered formalin (Sigma-Aldrich) and decalcified using Immunocal (Decal chemical corp.) for 7–10 days. After histoprocessing, they were embedded in paraffin wax and sectioned at 4 μm thickness. Sections were dewaxed, serially rehydrated, and stained with eosin and hematoxylin. Sections assigned for immunohistochemistry were air-dried overnight in a 50°C incubator, deparaffinized, and rehydrated in distilled water. To block endogenous peroxidase, slides were incubated for 30 min with 3% hydrogen peroxide solution (Sigma-Aldrich). The sections were then immersed in antigen unmasking solution (pH 6.0; Vector Laboratories) and microwaved (Ted Pella) for 4 min on high power, cooled at room temperature for 30 min, washed in distilled water, and transferred to PBS containing 0.1% Triton X-100. The following primary antibodies were used: antivimentin (Invitrogen; prediluted); anti-panCytokeratin (Abcam, Cambridge, MA; 1:100); antidesmin (Invitrogen; prediluted); antismooth muscle actin (DAKO; 1:100); anti-CD31 (BD Biosciences; 1:25).
Primary antibodies were diluted using ready-to-use Antibody diluent (DakoCytomation Denmark A/S), and applied over the slides and then incubated over night at 4°C. On the following day, the sections were washed three times with PBS containing 0.1% Triton X-100 and then incubated with horseradish peroxidase (HRP) polymer conjugate broad spectrum (DAB) (SuperPicture™, ZYMED Laboratories, Inc.) for 30 min at room temperature. Finally, the sections were washed one time with PBS containing Triton X-100, observed using Peroxidase Substrate Kit (DAB, Vector Laboratories, Inc.), counterstained with hematoxylin, dehydrated, and mounted using Permount (Fisher Scientific). If necessary, the images were merged into a single image, using an Apple Macintosh computer (Mackintosh) with Adobe Photoshop Elements 2.0 (Adobe).
Assessment of epidermal ingrowth
As a measure of role of gelatin scaffolds in cell growth, the distance between the original keratinized epidermis and the edge of epidermis at the site of applied gelatin scaffolds was measured to assess the epidermal ingrowth underneath the scaffolds using a Windows XP computer (Microsoft Co.) with Axio Vision 4.5 (Carl Zeiss MicroImaging, Inc.).
Evaluation of cellular adhesion on gelatin scaffolds
To evaluate cell adhesion on the gelatin scaffolds, measurement of viability of adherent cells was performed. Just after euthanasia, adherent gelatin scaffolds were removed from fetal body. The edge of gelatin sheet was removed to eliminate the contamination of glued fetal body tissue. The trimmed gelatin scaffold was placed in a 48-well culture dish and cellular viability was measured using the MTT-based colorimetric assay kit according to the kit instructions (Cell Proliferation Kit I; MTT labeling reagent 20 μL, solubilization solution 200 μL, 650 nm wavelength).
Statistical data analysis
SPSS (Version 18: SPSS, Inc.) was used for statistical analysis. Data were first analyzed for normality of distribution using a Shapiro-Wilk test. For non-normally distributed data, differences between groups were determined using a Kruskal-Walls test, and Mann-Whitney post hoc tests to identify differences between individual mean values. Normally distributed data were analyzed using a one-way analysis of variance. When variance of data was homogeneous, as determined by Levenes test, post hoc analysis was performed using the least significant difference test. When variance of data was inhomogeneous, the Tamhane post hoc test was used to identify significant differences between individual means. Statistical significance was accepted at p < 0.05. All data are expressed as means ± the standard deviation.
Results
Preparation and characterization of gelatin scaffolds
Table 1 summarizes the preparation methods utilized and characterization of each gelatin scaffold. In an attempt to standardize our scaffolds so that the primary variable would be scaffold shape, we tested the in vitro degradation of each scaffold to confirm similar degradation characteristics in 1N hydrochloric acid assay. Figure 2 demonstrates the time course of in vitro gelatin scaffold degradation. The kinetics of degradation to complete dissolution varied slightly between scaffolds but all were completely dissolved in 12 h, irrespective of the crosslinking conditions and scaffold shape.
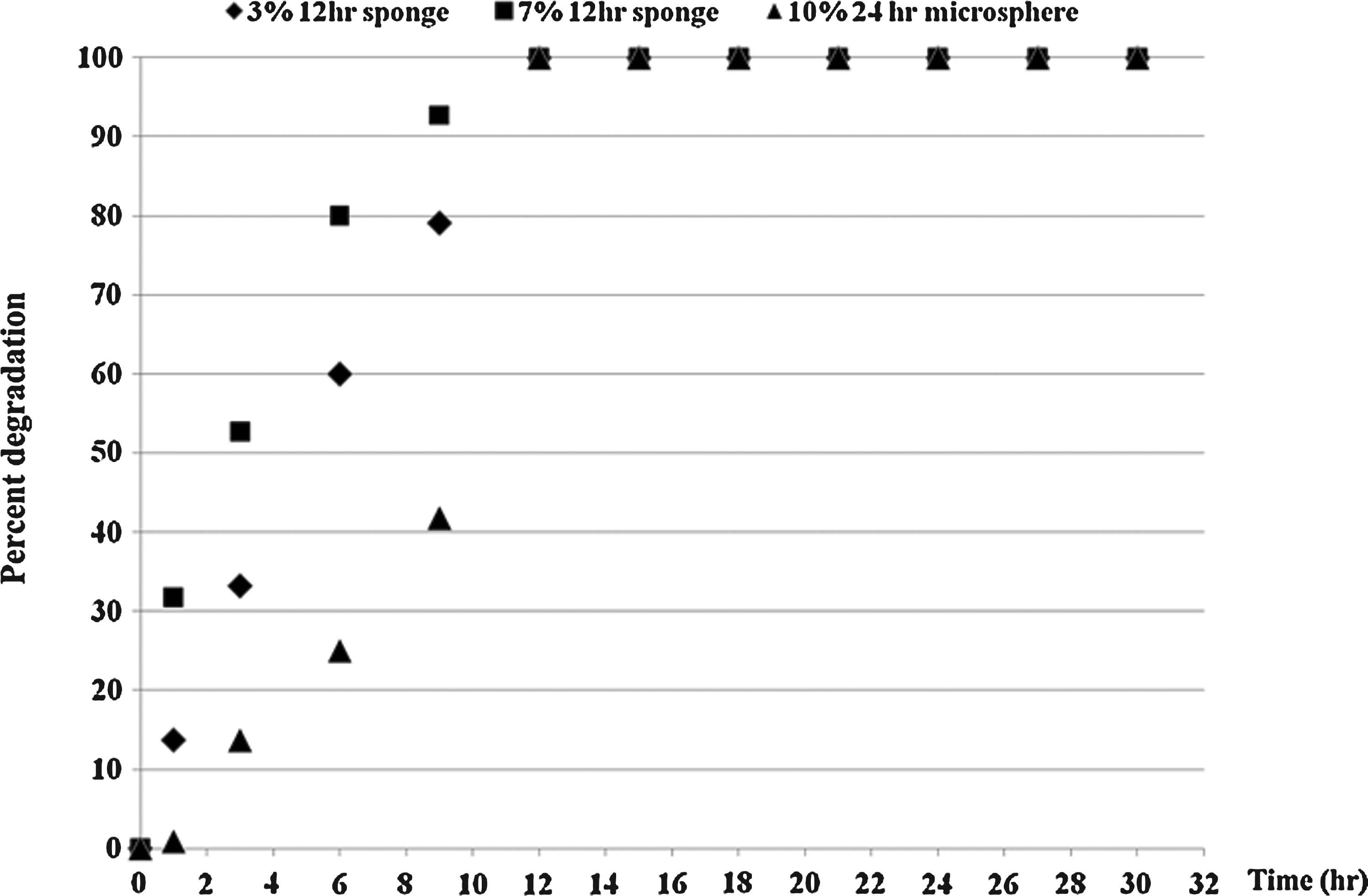
In vitro degradation profile of gelatin scaffolds. In vitro time profiles of gelatin scaffold degradation. (♦) The gelatin sponges prepared at 3 w/v% gelatin. (▪) The gelatin sponges prepared at 7 w/v% gelatin. (▴) The microspheres prepared at 10 w/v% gelatin. The sponges and microspheres underwent dehydrothermal crosslinking for 12 and 24 h, respectively.
Details of preparation of gelatin scaffolds of each group and their morphologic characteristics.
CL, cross-linked.
Epidermal ingrowth in organ culture
Figure 3A shows cross-sectional images of gelatin scaffolds on MMC after 7 days of in vitro organ culture. Figure 3B demonstrates the epidermal ingrowth underneath the scaffolds. Compared with the gelatin sheet control (Group D; 22.22 ± 20.90 μm), significantly increased epidermal ingrowth was observed in the two sponge groups (Group A and B; p < 0.05). The sponge with larger pore size (Group A) (73.06 ± 32.91 μm) showed greater epidermal ingrowth than the sponge with the smaller pore size (Group B) (53.89 ± 12.12 μm) (p < 0.05). The extent of epidermal ingrowth for Group C (microsphere) (53.98 ± 24.62 μm) was similar to that of Group B, but much greater than that of Group D (sheet) (p < 0.05).

Epidermal ingrowth under the gelatin scaffolds after 7 days of in vitro organ culture. (): significant difference versus Group A: p < 0.05 (#): significant difference versus Group B: p < 0.05 (O): significant difference versus Group C: p < 0.05. MMC, myelomeningocele. Color images available online at www.liebertonline.com/tea.
Epidermal ingrowth in vivo after fetal surgery
Figure 4A shows cross-sectional images of gelatin scaffolds covering the MMC defect 4 days after application by open fetal surgery as well as an image of a nontreated MMC defect. Advancement and morphological changes of the epidermal edge were observed in all experimental groups, compared to nontreated MMC. Figure 4B shows a graph quantifying the degree of epidermal ingrowth underneath the scaffolds. Epidermal ingrowth extended 71.22 ± 19.91 μm underneath the sponges (Group A) and 66.38 ± 19.79 μm under the microspheres (Group C), which was significantly greater than that of the gelatin sheets (Group D) (8.96 ± 10.96 μm) (p < 0.05). There was no significant difference between Group A and Group C.
Epidermal ingrowth under the gelatin scaffolds 4 days after MMC coverage by fetal surgery. (): significant difference between the groups: p < 0.05. Color images available online at www.liebertonline.com/tea.
Cell adhesion to the outside of the gelatin scaffold in vivo
Figure 5A shows cross-sectional images of cell adhesion with associated ECM coating the outside of the gelatin scaffolds 4 days after application of the gelatin scaffolds to the MMC defect in vivo. The total number of adherent cells as evaluated by the MTT cellular proliferation assay is shown in Figure 5B. Significantly increased cell adhesion was observed in the sponge and microsphere groups (Group A; 84.54 ± 50.47 × 103 and Group C; 84.93 ± 16.41 × 103) compared to the gelatin sheet control (Group D; 34.43 ± 14.66 × 103, p < 0.05).
Cell adhesion with ECM deposition along the outside of the gelatin scaffolds 4 days after application by fetal surgery. (): significant difference between the groups: p < 0.05. ECM, extracellular matrix. Color images available online at www.liebertonline.com/tea.
Cell adhesion and proliferation on gelatin sheets coated with bioactive proteins in vitro cell culture
The proliferation of cells adherent to gelatin sheets coated with the various bioactive proteins in in vitro cell culture is shown in Figure 6. Cells became confluent around day 12 and then regressed in the collagen type I, collagen type IV, and fibronectin groups. Among the different bioactive proteins the number of cells at confluence was greater in the collagen I and fibronectin groups than collagen IV. In contrast, cells grew very slowly in the laminin and PBS groups and did not reach confluence by day 15.
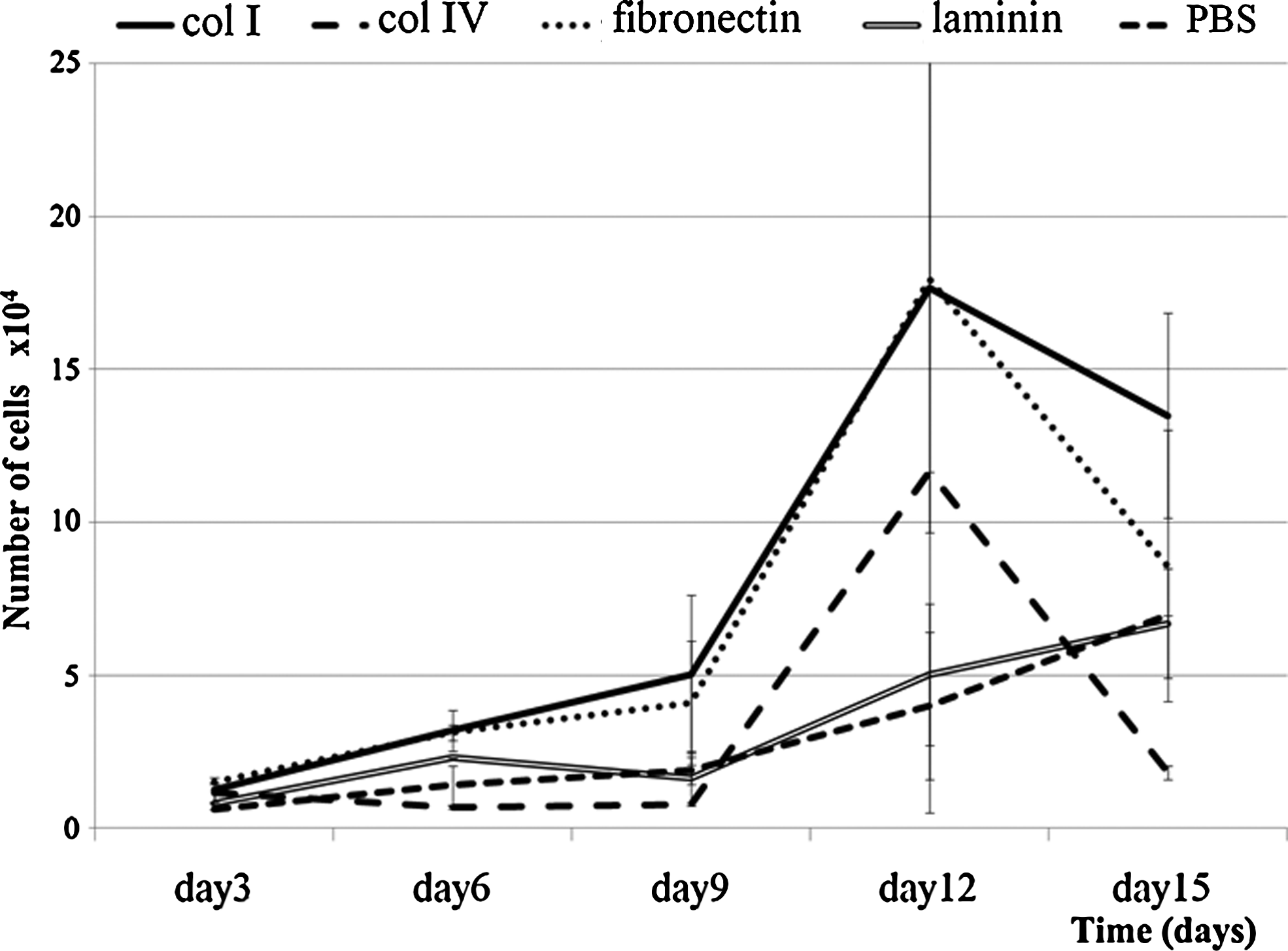
Cell adhesion and proliferation on gelatin sheets coated with various bioactive proteins after up to 15 days of in vitro cell culture. Graph of the proliferation of cells adherent to gelatin sheets coated with bioactive proteins at serial time points of in vitro cell culture evaluated by methylthiazol tetrazolium cellular proliferation assay.
Cellular adhesion to gelatin sheets coated with bioactive proteins in vivo
Figure 7 shows the number of cells adherent to gelatin sheets coated with different bioactive peptides in vivo after application by fetal surgery. Collagen I (10.54 ± 4.65 × 104) and fibronectin coating (7.32 ± 1.61 × 104) resulted in a significantly higher number of adherent cells than the other bioactive proteins (collagen IV; 5.05 ± 1.38 × 104, laminin; 3.27 ± 0.58 × 104, and PBS; 2.63 ± 0.85 × 104, p < 0.05). There were no significant differences between the collagen I and fibronectin groups or between the collagen IV, laminin, and PBS groups.
Cell adhesion on gelatin sheets coated with various bioactive proteins in vivo 4 days after application by fetal surgery. Bar chart of the number of cells adherent to gelatin sheets coated with different bioactive proteins assessed 4 days after application of gelatin sheets in vivo. (): significant difference versus collagen type I: p < 0.05 (#): significant difference versus fibronectin: p < 0.05.
Histological evaluation of adhered cells to the gelatin sheet coated with bioactive proteins
Figure 8 shows histology of the cells and ECM coating the outside of the gelatin sheets. Cells and ECM were observed as either multiple layers or a thick single layer. Many cells stained positively for smooth muscle actin and some cells stained positively for pancytokeratin and vimentin. There were no cells expressing desmin or CD31. These findings were seen in all groups irrespective of the bioactive protein coatings.
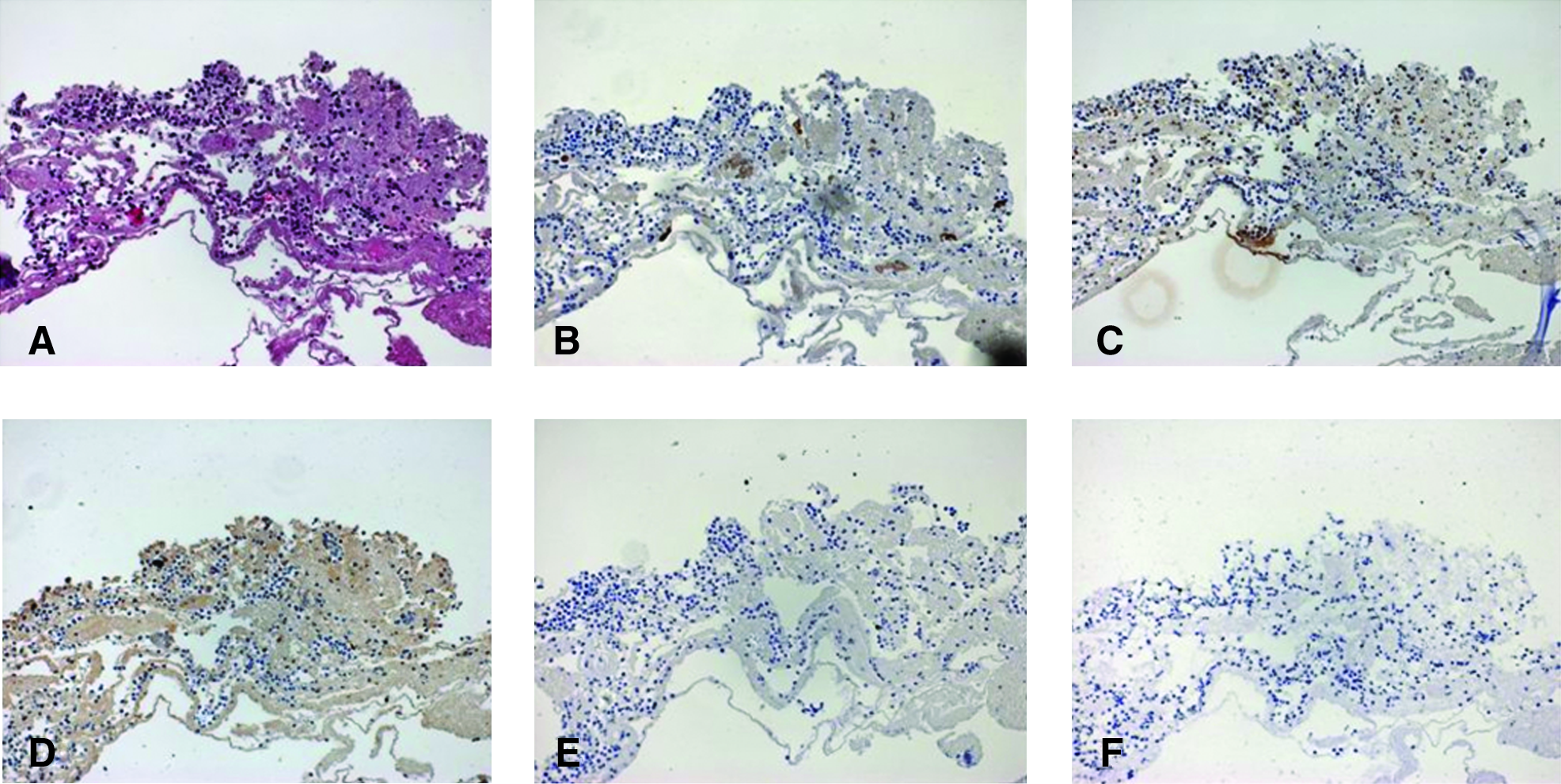
Immunohistochemical analysis of the adherent cell layer to gelatin sheets coated with various bioactive proteins 4 days after application by fetal surgery Representative sections of the adherent cell layer and associated ECM on the outside of the gelatin sheets. The staining did not differ between types of bioactive proteins, and all images are from sheets coated with collagen type I. Magnification: ×20. Immunohistochemical staining for (
Discussion
The primary requirement for a tissue engineering solution to prenatal coverage of MMC is the generation of a mechanically stable, amniotic fluid impermeable tissue layer over the MMC to protect the exposed neural elements from chemical and physical injury. The application of tissue engineering in the intrauterine environment presents unique obstacles and opportunities. The fetus has unique regenerative capacity with a higher frequency of stem cells in all tissues and higher cell proliferation rates, as evidenced by the remarkable ability of the early gestational fetus to heal wounds without scar formation. 16 Thus, an attractive approach is to utilize scaffolds and bioactive molecules to stimulate endogenous fetal stem cells to regenerate a tissue layer over the MMC similar to the approach used for regeneration of skin defects or corneal wound healing.17,18 In our previous study, a natural biodegradable biomaterial, gelatin hydrogel, was selected as the tissue engineering scaffold for fetal MMC due to the advantages of cytocompatibility, easy formulation into various shapes, the ability to control degradation, and its properties for protein release.12,19,20 We demonstrated that gelatin sponges could support cellular and epidermal ingrowth by endogenous cells with the associated production of ECM even in the amniotic fluid environment. Neovascularization was also observed within the sponges, particularly with bFGF incorporation, supporting the potential for generation of sustainable tissue coverage and the ability of the scaffold to release exogenous growth factors in the intrauterine environment. 10 These findings were in good accordance with previously reported wound healing studies utilizing gelatin hydrogel.14,18,21–23 If the MMC defect can be covered by neo-epidermal or other types of tissue derived from ingrowth of native cells, it would likely provide the necessary protection against amniotic fluid exposure. In this in vivo study, the calculated percent of closure by epithelial ingrowth of the MMC defects was 25.03 ± 10.49% in the sponge group (Group A) and 22.31 ± 9.34% in the microsphere group (Group C) compared to only 2.69 ± 6.93% in Group D (sheets) at the time of harvest (4 days after scaffold application). We beleive that this is promising; however, a large animal model will be necessary to obtain longer term data and to assess whether complete coverage is achieved. Future results may be improved by incorporating growth factors into the scaffolds to accelerate epidermal or other types of cellular ingrowth.
Another unique opportunity presented by the intrauterine environment is the presence of multi- or pluripotent stem cells within the amniotic fluid.24–28 Thus, a second attractive approach would be to develop methods to promote the adherence of these cells to either the MMC itself, or a tissue-engineered scaffold covering the MMC, so that they might contribute to the generation of a tissue layer. In fact, the finding of cell adhesion with ECM deposition along the outside of the gelatin composite was observed in our study. This is a phenomenon that was not mentioned in other studies of tissue engineering for fetal MMC.29–32 The cells adherent to the gelatin scaffolds seemed to derive from amniocytes in our study, not from endogenous fetal cells. They were composed of both epithelial and nonepithelial cells, which were different from the cells that migrated into the sponges from the fetal tissues that were composed of only nonepithelial cells. In addition, the cell surface markers of the adherent cells were very similar to that of the amniotic fluid cells reported by others,27,28 especially mesenchymal stromal cells. Finally, when exogenous cells were injected into amniotic fluid, we observed similar adherence to the gelatin sheet of the composite (data not shown). The appearance of the adherent cells and associated ECM varied widely between experiments. A heterogeneous ECM with sparse cells covering gelatin scaffold were seen on some MMCs, whereas multiple dense cell layers could be observed over the gelatin scaffold in other samples. This is not surprising because of the brief duration of our in vivo experiments and the variation in composition of amniotic fluid cells. However, these cells seem to have potential as a cell source for tissue coverage over the MMC, but further studies in a large animal model that would allow a longer duration of observation are needed. In addition, there may be strategies to enhance the adherence and growth of amniotic fluid cells or to add exogenous cells that might selectively target the MMC sac.
The optimal scaffold material would provide endogenous cells and amniotic fluid-derived cells with a local environment that promotes adhesion, proliferation, and differentiation. 22 Biomaterial scaffolds providing a modifiable platform to optimize these events have a variety of designs, including 33 sheets,34,35 sponges, 36 tubes, 37 and nano/micro carriers. 38 From a clinical perspective the design of the scaffold greatly influences the mode and potential timing of prenatal application. The use of sheet or sponge scaffolds dictates surgical placement by either open fetal surgery or fetoscopic technique, both of which are technically feasible only at later gestational ages (after 18–20 weeks of gestation). However, a scaffold that could be injected under ultrasound guidance onto the MMC defect would allow treatment at a much earlier stage of development, potentially as early as the MMC can be diagnosed (14–15 weeks gestation). We have considered several injectable scaffold designs, including particles, spheres, in situ forming materials, in situ crosslinkable systems, thermogelling systems, and self-assembling systems.33,38 Among these choices, microspheres that have been widely used as a drug delivery systems33,38 were chosen for ease of manufacture and because we could make gelatin hydrogel microspheres for direct comparison with our previously tested composite scaffolds for support of cell growth and proliferation as well as amniotic fluid cell adherence.
Ideally, microspheres as a scaffold material could be tested by injection into amniotic cavity. However, at this point, we have no technology that allows adherence of the microspheres to the MMC and prevents dissolution of the microspheres in the amniotic fluid. Before addressing this obstacle, we wished to establish proof in principle that gelatin hydrogel microsphere-based scaffold design could support cell ingrowth and adherence as well as our previous sheet and sponge composite scaffolds. 10 A gelatin composite was constructed with a hat-shaped gelatin sheet and either a sponge or microspheres insert. The hat-shaped gelatin sheet conforms to the MMC lesion and holds the microspheres in place over the MMC preventing their dispersion. In this study, to examine the effect of the scaffold on epidermal ingrowth underneath the scaffold, the sponges or microspheres were placed underneath the gelatin sheet against the MMC defect. To examine amniotic fluid cellular adhesion, the sponges or microspheres were glued to the outside of the gelatin sheets.
In this study, we wished to compare the effects of scaffold form, that is, sponge, microsphere, and sheet, as directly as possible. Gelatin scaffold is a biodegradable material and its degradation kinetics are determined by many factors, such as the type of gelatin hydrogel, isoelectric point, gelatin concentration, scaffold shape, and the method and strength of crosslinking. We reasoned that an appropriate standardization of these parameters to allow direct comparison of the effects of shape alone would be to select scaffolds of different shapes with similar degradation profiles. We selected a period of in vitro degradation (12 h in 1 N HCL) that in previous studies correlated with an in vivo degradation period of over 4 days,12,19,20 allowing preservation of the morphology of the construct over the duration of our study.
In addition, we utilized two models to compare the scaffolds, an in vitro organ culture system39,40 and our in vivo fetal surgery model. For in vitro organ culture we determined that the epidermal ingrowth was no different whether MMC defects from E20, E21, or E22 fetuses were used. Since the skin and neural tissues of fetuses at less than E22 were very fragile and difficult to manipulate, we used E22 defects for our experimental studies. We also determined that significant differences were noted between our scaffolds at 3 and 7 days of organ culture but not at 10 and 14 days in our pilot studies. We therefore used 7 days as our experimental endpoint. Finally, while the in vitro organ culture appeared similar to the in vivo model with respect to epidermal ingrowth, we did not detect the cellular migration of native tissue into the sponges and angiogenesis seen in the in vivo studies 10 ; therefore, the in vitro organ culture system was only used for evaluation of epidermal ingrowth.
We hypothesized that the gap space between microspheres would mimic the porosity of sponges with respect to support of cellular and epidermal ingrowth. Therefore, in this study, gelatin microspheres (14.83 ± 3.16 μm in diameter dry and 47.98 ± 22.22 μm in diameter in water) were compared with gelatin sponge constructs with large pores (200.22 ± 33.31 μm dry and 226.78 ± 35.04 μm in water) or gelatin sponges with small pores (152.48 ± 33.79 μm dry and 189.34 ± 26.87 μm in water) and gelatin sheets without any pore structure in vitro. The larger pore sponge proved superior in vitro, so it was selected for the in vivo studies. Theoretically, the calculated effective surface area among 10 v/w% microspheres, 3 v/w% sponges (big pores), and 7 v/w% sponges (small pores) are remarkably similar (1.78 × 106 μmm2, 1.78 × 106 μmm2, 1.78 × 106 μmm2 per 1.00 × 106 μmm2), and much higher than sheets (1.00 × 106 μmm2). Also, the scaffolds chosen for this study appeared to remain as expected histologically. Thus, we feel that the differences noted in this study are primarily the result of the different structural characteristics of the scaffolds. Our results demonstrate that gelatin sponges and microspheres were similar in their ability to support epidermal ingrowth and cell adhesion, and that both were significantly better than gelatin sheets alone. These results are consistent with previous studies demonstrating that greater surface area and porosity of a scaffold support cell adhesion and proliferation, and that the approximate pore size of our 3 v/w% sponge is optimal for tissue ingrowth.41,42 Microgeometric properties of the sponge and microsphere surfaces also explain the difference as roughened surfaces tend to promote greater cell adhesion and growth than smooth surfaces. 43
In general, artificial ECM constructs have been synthesized from either naturally occurring molecular polymers or synthetic polymers. Cell adhesion on scaffolds can potentially be enhanced by combining ECM-derived peptides such as Arg-Gly-Asp in fibronectin, Gly-Pro-Hyp in collagen type I, (α1)2-α2 in collagen type IV, and Tyr-lle-Gly-Ser-Arg and lle-Lys-Val-Ala-Val in laminin. All of these ECM-derived proteins have been widely used to improve scaffold cell adhesion, migration, proliferation, and ECM synthesis 44 with the primary goal of increasing similarity of the scaffold to native tissue.45–47 In this study, ECM-derived proteins were applied to gelatin sheets, not to gelatin microspheres, to observe the direct effect of ECM-derived proteins on gelatin scaffolds with the presumption that the same effect should be observed on all gelatin hydrogel-based scaffolds. In our study, the amniotic cells that adhered to gelatin scaffolds were composed of mixture of epithelial cells and nonepithelial cells that did not express myogenic or endothelial markers. These cells were the same in all experimental groups irrespective of the type of coating bioactive proteins. However, more cell adhesion was seen in groups coated with collagen type 1 and fibronectin, which is in agreement with other studies.48–50 This makes sense because collagen type 1 and fibronectin are major ECM constituents in epithelial tissues.
A major limitation of this study is relatively short gestation of rat model and nonsurvivability of the pups. This prevents any long-term assessment of whether or not durable tissue coverage is achieved. Nevertheless, the present study is encouraging and demonstrated gelatin microspheres could support cellular adhesion and epidermal proliferation and that they were equivalent to a sponge scaffold in all respects. This supports our hypothesis that gelatin microspheres might be a suitable starting material for development of an injectable scaffold that would facilitate a truly minimally invasive approach for coverage of fetal MMC. In further studies we hope to develop techniques to promote adherence of microspheres to each other and to the MMC defect to allow injection into the amniotic fluid over the MMC defect without dispersion. These techniques may involve positive-negative charge interactions, specific molecular binding to ligands on the MMC sac and/or the microspheres, and/or the use of hydrophobic adhesives. Also, these results suggest that utilization of collagen type I and fibronectin coating would increase cellular adhesion to the scaffold in the fetal amniotic fluid environment, accelerating coverage of the MMC defect. We speculate that growth factors could be incorporated into the gelatin microspheres to further support cell growth and proliferation to optimize this approach. 33 Although further material and technological development is needed, the present data strongly support the future potential of a less invasive tissue engineering approach for prenatal coverage of MMC.
Footnotes
Acknowledgments
The authors are indebted to Masaya Yamamoto, Ph.D., Yu Kimura, Ph.D., Kentaro Hayashi, M.Eng., from Kyoto University, and Hiroshi Koyama, M.D., Ph.D., from CHOP for teaching M.W., the methodology for making the gelatin products, and their excellent technical assistance.
Disclosure Statement
No competing financial interests exist.