
Abstract
Surgical debridement of the dead bone and subsequent systemic antibiotic therapy is often ineffective in eliminating Staphylococcus aureus infections in osteomyelitic patients. The recurrence of S. aureus infection is mainly due to the intracellular growth of bacterial colonies within osteoblast cells that protect the organism from extracellular host defences and/or antibiotic therapy. In this study, porous gelatin–hydroxyapatite (HAP) scaffolds with various amounts of ciprofloxacin (1, 2, 5, and 10 wt%) were fabricated by freeze-drying technique and the release of the antibiotic was characterized, as was the efficacy of the released antibiotic against methicillin-sensitive and methicillin-resistant S. aureus. Furthermore, the impact of the released antibiotic on the viability and osteogenic differentiation of human adipose-derived mesenchymal stem cells (ADMSCs) cultured on the scaffolds were assessed. Finally, the efficacy of the released ciprofloxacin to enter the cells and abate intracellularly located S. aureus was evaluated. All the groups of CGHA scaffolds displayed sustained release of ciprofloxacin against S. aureus for 60 days above the minimum inhibitory concentration for the target species with zero-order kinetics and Korsmeyer–Peppas models. While comparing, the released antibiotic from CGHA5 scaffolds was found to be effective at reducing S. aureus through the study period, without detrimental effects on human ADMSC viability or osteogenic potential. When stem cells internalized with S. aureus were cultured onto the drug-loaded scaffolds, a significant reduction in the colony count of internalized bacteria was observed, resulting in the osteogenic differentiation capability of those cells. Our results clearly demonstrate that the ciprofloxacin incorporated gelatin-HAP scaffolds, which were cytocompatible and could target both intracellular and extracellular S. aureus, defining its potential to be used as local drug delivery system.
Introduction
S
Management of chronic osteomyelitis with a local antibiotic delivery system achieves therapeutic antibiotic concentration at the infected site, without generating systemic toxicity. 10 The commercially available local drug delivery matrix is polymethylmethacrylate (PMMA) with gentamicin or tobramycin, which is offered either in the cement form (Palcos and Simplex P) or in the bead form (Septopal). 11 However, the main drawback of PMMA is its nonbiodegradability that necessitates revision surgery. 12 Another disadvantage associated with PMMA is the exothermic reaction that occurs during its mixing that decreases the effectiveness of certain antibiotics. 13 In addition, the penetration of gentamicin or tobramycin through the mammalian cell membrane to target internalized S. aureus is poor. Thus, an ideal local antibiotic delivery system for chronic osteomyelitis includes an appropriate (a) biodegradable biomaterial, which can deliver antibiotics locally and simultaneously support cellular and vascular infiltration followed by bone regeneration, (b) antibiotics that can kill both extracellular and intracellular S. aureus, and (c) concentration of antibiotics that can inhibit bacteria without creating toxicity to mammalian cells.
The scaffolds like hydroxyapatite (HAP) or its composites (gelatin-HAP or collagen-HAP) have gained much interest in bone tissue engineering since it is osteoconductive and has similarity in chemical composition to native bone.14,15 There were reports showing the antibacterial efficacy of vancomycin or arbekacin sulfate-loaded dense HAP for the treatment of osteomyelitis developed through intramedullary injections of S. aureus in rat models.16,17 However, for effectual vascularization followed by bone regeneration in the chronic osteomyelitic area, the antibiotic-loaded scaffolds should have appropriate porosity, with the pore size above 100 μm. 18 It should also support the viability and osteogenic differentiation of mesenchymal stem cells (MSCs). 19
Among many antibiotics, ciprofloxacin is reported to have good penetration ability even in poorly vascularized site. 20 It has broad-spectrum antibiotic activity against sensitive and resistant-type S. aureus as well as gram-negative bacteria. Recently, Sisto et al. demonstrated the uptake of ciprofloxacin by bone marrow-derived MSCs, 21 so this antibiotic may be useful for targeting S. aureus internalized in the osteoblast or MSCs. However, a higher concentration of ciprofloxacin can inhibit osteoblast proliferation and function. 22 Thus, the concentration of ciprofloxacin released from porous biomaterials should be optimal, which can eliminate S. aureus without causing toxicity to MSCs or osteoblasts.
The present study investigated the antibacterial effect of the ciprofloxacin loaded gelatin-HAP scaffold against methicillin-sensitive S. aureus (MSSA) and methicillin-resistant S. aureus (MRSA) for a period of 8 weeks. Concurrently, viability, proliferation, and osteogenic differentiation of human adipose-derived mesenchymal stem cells (ADMSCs) cultured on these scaffolds were studied. Furthermore, MSSA and MRSA were internalized in ADMSCs and the ability of the ciprofloxacin-loaded scaffold to eliminate internalized bacteria and to recover the viability and functionality of infected cells was evaluated.
Materials and Methods
Fabrication of gelatin-HAP scaffolds with ciprofloxacin
HAP was synthesized by the aqueous precipitation method, as reported earlier. 23 Ciprofloxacin HCL (1, 2, 5, and 10% wt/vol) and gelatin Type A (10% wt/vol) were dissolved in distilled water at 40°C. HAP was then added to this mixture and stirred for 1 h with an additional sonication for 30 min (35% gelatin:65% HAP). The slurry was poured into 48 well plates and kept at −20°C for 6 h and lyophilized for 24 h. As a control, gelatin-HAP scaffolds without ciprofloxacin were prepared in the same manner. These scaffolds were cross-linked with 1% gluteraldehyde for 24 h, followed by washing with distilled water. The scaffolds with and without ciprofloxacin were named as CGHA (CGHA1 [1 wt%], CGHA2 [2 wt%], CGHA5 [5 wt%], and CGHA10 [10 wt%]) and GHA, respectively.
Characterization of scaffolds
The morphology and pore size of the scaffolds were analyzed by a scanning electron microscope (SEM) at an accelerating voltage of 15 kV (JSM-6490LA; JEOL), functional groups by Fourier transform infrared spectroscopy (FTIR) (Perkin Elmer Spectrum RX-1), and crystallinity by X-ray diffraction (PAN analytical X'Pert PRO X-ray diffractometer fitted with CuKa source).
Antibacterial study
Drug encapsulation efficiency
The gelatin-HAP matrix with ciprofloxacin (9 mm diameter×16 mm height) was powdered, immersed in 5 mL phosphate buffered saline (PBS) at pH 7.2, and centrifuged at 8000 rpm for 15 min. The absorbance of ciprofloxacin in the supernatant was determined at 275 nm using a spectrophotometer (Biotek Powerklave XS). 24 The concentration of the drug was calculated from the optical density using a calibration line plotted with known concentration of ciprofloxacin. The entrapment efficiency percentage=(amount of drug encapsulated/amount of drug added)×100.
Drug release kinetics and bacterial inhibition study
The GHA and CGHA scaffolds (sample size: 9 mm diameter×4 mm height) were immersed in PBS at 37°C for 60 days, and the concentration of ciprofloxacin in PBS was calculated at each time point (days 1, 7, 14, 21, 28, 35, 42, 50, and 60), as mentioned above. The scaffolds were used for the bacterial inhibition study against MSSA and MRSA. The log-phase cultures of S. aureus were adjusted to get a final cell density of 106 colony forming unit (CFU)/mL and were spread onto the Luria Bertani (LB) agar plate. The scaffolds were placed on those agar plates; the plates were incubated overnight at 37°C and the zones of inhibition were measured. A Whatman disc (5 mm) loaded with 0.4 μg ciprofloxacin was taken as the positive control. 25
Release kinetics modeling
The ciprofloxacin release from the scaffolds were evaluated kinetically using four different drug release models—zero-order kinetics, first-order kinetics, Higuchi model, and Korsmeyer–Peppas model, as reported earlier. 26 The goodness of fit was determined by comparing the average R 2 values generated from simple linear regression.
Viability of S. aureus on scaffolds
S. aureus (2×105 CFU) (MSSA and MRSA) were cultured on GHA and CGHA scaffolds for 4 h and analyzed for bacterial viability using confocal microscope, Alamar blue assay, and colony count. The bacterial cells were stained with calcein AM (4 mM)/ethidium bromide (2 mM) for 5 min, followed by washing with PBS, and viewed under the confocal microscope (Leica, SP5II) at an excitation and emission wavelength of 480/520, respectively. For colony count studies, the scaffolds with S. aureus after 4 h were cultured in LB broth at 37°C for 24 h. Bacterial cells were serially diluted and plated on LB agar plates to evaluate their growth as described above. Additionally, the viability of cells at 4 and 24 h was quantitated by Alamar blue assay. For this, LB broth were supplemented with Alamar blue reagent (10%) and the absorbance was measured at 570 and 600 nm (Biotek Powerklave XS). The absorbance was correlated with S. aureus cell viability using a calibration line plotted with known concentrations of bacterial cells.
Cell culture studies
The Institutional Human Ethics Committee has approved the isolation of MSCs from adipose tissue collected from patients. The human ADMSCs were isolated from different patients, pooled, and the cells in passage 2–5 (5×104 cells) were seeded on GHA and CGHA scaffolds (sample size: 9 mm diameter×4 mm height) and incubated in α-minimal essential medium (α-MEM) with 10% fetal bovine serum (FBS) at 37°C. After 24 h, the basal medium was supplemented with 10 mM β-glycerophosphate, 10−8M dexamethasone, and 0.05 mg/mL
Cell viability and proliferation
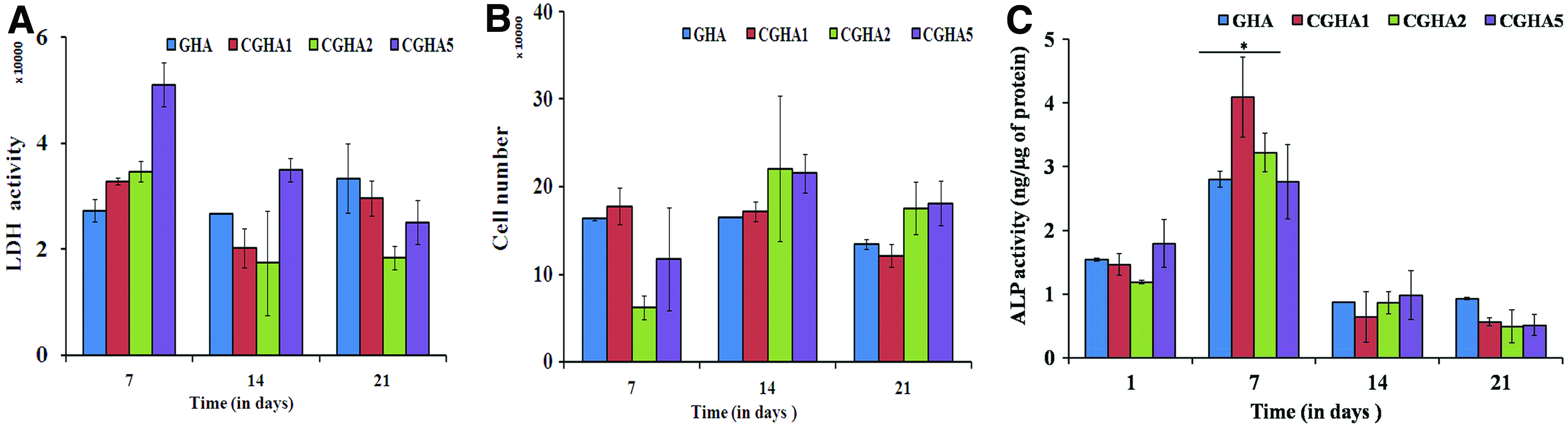
The human ADMSCs cultured on scaffolds after 4 and 24 h were stained with calcein AM and ethidium bromide as described above and evaluated for live–dead assay by confocal microscope. The same scaffolds were fixed with 1% gluteraldehyde in Sorenson's phosphate buffer, dehydrated with increasing concentration of ethanol, and visualized under SEM to determine cell adhesion. The viability and proliferation of cells cultured on the scaffolds were quantitated (on days 7, 14 and 21) through the total activity of lactate dehydrogenase (LDH) (Cytotox96 kit; Promega) and picoGreen® dsDNA quantitation assay (Invitrogen), respectively, as reported earlier. 27 The relative fluorescence units were correlated with the cell number using a calibration line constructed with known concentrations of cells.
Osteogenic differentiation
The alkaline phosphatase (ALP) activity of cells after 1, 7, 14, and 21 days was determined based on the hydrolysis of p-nitrophenyl phosphate (Sigma) to p-nitrophenol (n=6), as reported earlier. 27 The cells lysed with 1% Triton X-100 were added with p-nitrophenyl phosphate and the absorbance was measured at 405 nm (Biotek werklave XS). A calibration line was constructed with different concentrations of ALP enzyme, which could hydrolyze p-nitrophenyl phosphate to p-nitrophenol. The ALP activity measured for each sample was normalized to total protein content.
Internalization of S. aureus in human ADMSCs
The human ADMSCs (1×105 cells) were cultured in α-MEM with 10% FBS to form a monolayer. S. aureus inoculum was added to these cells at a multiplicity of infection (MOI) of 30:1 and cultured for 2 h. 28 The cells were washed twice with PBS and provided with α-MEM supplemented with gentamicin (10 mg/mL) to remove extracellular bacteria. Green fluorescent protein (GFP) expressing S. aureus (SA113) 29 within MSCs were imaged using confocal and differential interference contrast (DIC) microscopy (Leica, SP5II) and it was quantitated by flow cytometry (BD FACS Aria II) using fluorescein isothiocyanate (FITC) filters. In addition, colony count studies were done, for which the infected MSCs were lysed using Triton X-100 and the lysates after serial dilution were cultured on the agar plate.
S. aureus internalized human ADMSCs on scaffolds
The infected human ADMSCs were cultured on GHA and CGHA5 scaffolds (sample size: 9 mm diameter×4 mm height) for 4 and 24 h and investigated for cell viability and adhesion by confocal microscopy and SEM, respectively. In addition, osteogenic differentiation of these infected MSCs on CGHA5 scaffolds was determined by ALP activity on day 7.
Colony count studies
The infected human ADMSCs cultured on the scaffolds were trypsinized and lysed using Triton X-100 after 4 and 24 h. The lysate was serially diluted, plated on LB agar plates, and incubated overnight at 37°C to evaluate bacterial colonies.
Ciprofloxacin uptake by MSCs
The infected human ADMSCs cultured on the scaffolds were trypsinized, counted with a hemocytometer, and lysed using Triton X-100 after 4 and 24 h. The ciprofloxacin concentration in the lysate was measured as described above.
Statistical analysis
Six samples were used for each parameter in all quantitative experiments. Each parameter is expressed as mean of all values±standard deviation. Student's t test was employed to assess the statistical significance of results. p-Values <0.05 were considered significant for all analysis.
Results
Physiochemical characterization
Gelatin-HAP scaffolds (with and without ciprofloxacin) were fabricated by the freeze-drying method, which generated pores in the range of 100–550 μm. In the FTIR spectrum of raw ciprofloxacin HCL, the bands at 1622 and 1463.25 cm−1 represented both asymmetric and symmetric stretching vibrations of the O–C–O group of carboxylic acids, respectively. In GHA and CGHA scaffolds, HAP-specific peaks (570.23, 602.69, 1049.10 cm−1 corresponding to phosphate groups) and gelatin-specific peaks (1243.47, 1548.93, 1657.90, 2937.29 cm−1 corresponding to amide I and II bonds) were observed. Figure 1c represents the X-ray diffractogram of GHA and CGHA scaffolds in comparison to the raw ciprofloxacin HCL drug wherein all three groups showed crystallinity. The major peaks of GHA and CGHA scaffolds were at 26° and 32° (Fig. 1).
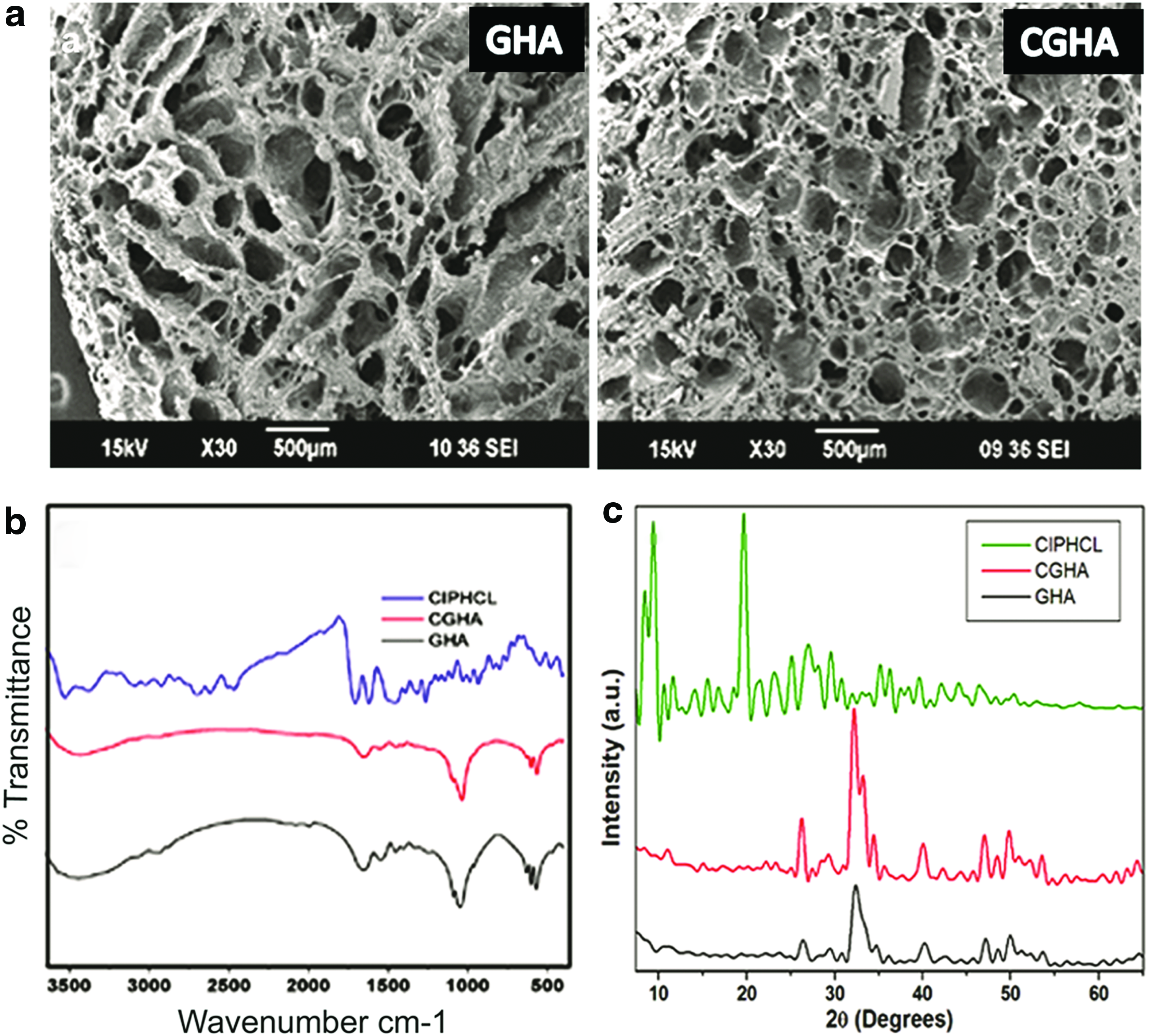
Physiochemical characterization of composite scaffolds:
Antibacterial study
Encapsulation efficiency of the ciprofloxacin drug (1, 2, 5, and 10% wt/vol) within the gelatin-HAP matrix was 93.1%, 73.9%, 58.4%, and 33.2%, respectively. Thus, the encapsulation efficiency was decreased with increase in the wt% of ciprofloxacin incorporated into the matrix. The ciprofloxacin release from scaffolds was described as average drug release rate per day (μg ciprofloxacin/mL construct/day) as well as % cumulative drug release (Fig. 2). CGHA scaffolds in all wt% showed a burst release of ciprofloxacin within 24 h, followed by sustained release for 7 weeks at levels above the minimum inhibitory concentration (MIC) against S. aureus (The MICs of ciprofloxacin against MSSA and MRSA were 0.4 and 2 μg, respectively). Among all scaffolds, CGHA10 showed the highest release (∼250±50 μg/mL/day for the initial 4 weeks and ∼150 μg/mL/day for later time points), followed by CGHA5 (∼150 μg/mL/day), which was followed by CGHA1 and CGHA2 scaffolds (∼100 μg/mL/day). The drug release kinetics was analyzed theoretically through modelings, such as zero-order, first-order, Higuchi, and Korsmeyer–Peppas. The ciprofloxacin release from the scaffolds was best fit to the zero-order and the Korsmeyer–Peppas models, irrespective of the concentration (Table 1).
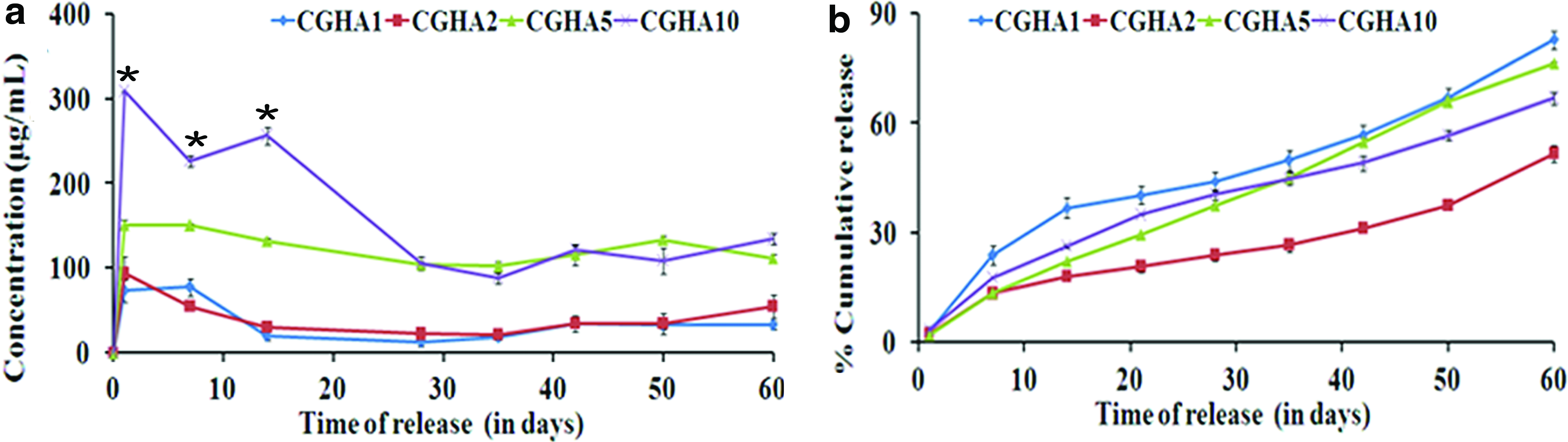
Drug release from CGHA scaffolds:
The modification of the Kirby-Bauer disc diffusion assay was done to assess the antibacterial action of ciprofloxacin released from CGHA scaffolds against MSSA and MRSA (Fig. 3). The positive control was the Whatman filter paper disc containing 0.4 μg/mL ciprofloxacin, which showed a zone of inhibition of 1.9 cm against MSSA and 1 cm against MRSA. The negative control was the GHA scaffold without drug. All CGHA scaffolds have demonstrated antibacterial efficacy against MSSA and MRSA for 60 days, except CGHA1 and CGHA2, which showed only up to 42 days against MRSA. The bioactivity of CGHA1 and CGHA2 scaffolds against MSSA and MRSA was significantly decreased on 28–42 days compared with initial time points, whereas the diameters of zones of inhibition of CGHA5 and CGHA10 scaffolds were almost alike throughout the study period. The diameter of the zone of inhibition against MRSA was significantly less when compared with MSSA, with all groups of scaffolds.
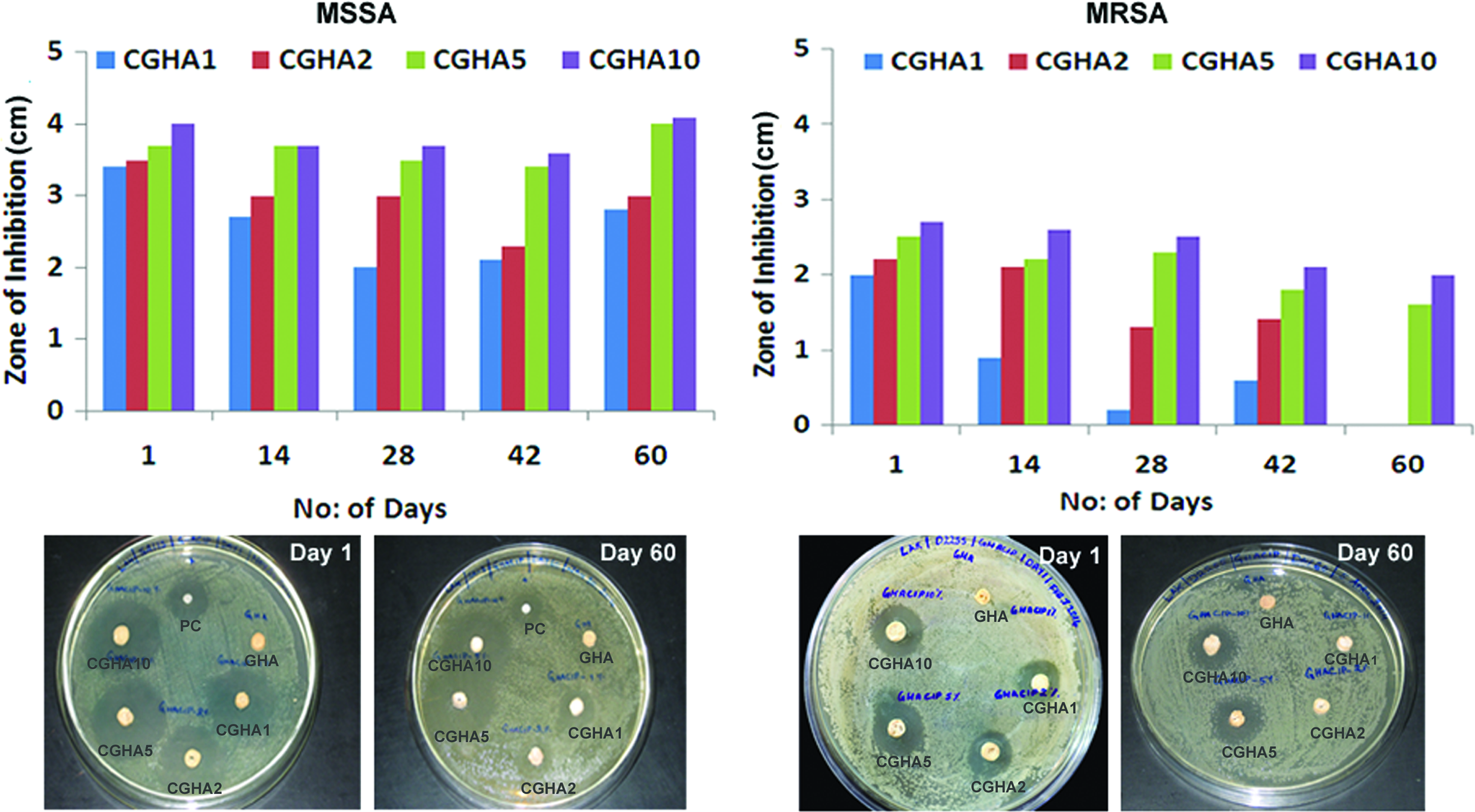
Antibacterial action of ciprofloxacin released from CGHA scaffolds against MSSA and MRSA for 60 days. PC: bare drug on Whatman filter disc, and negative control: GHA scaffold. MSSA, methicillin-sensitive S. aureus and MRSA, methicillin-resistant S. aureus; PC, positive control. Color images available online at www.liebertpub.com/tea
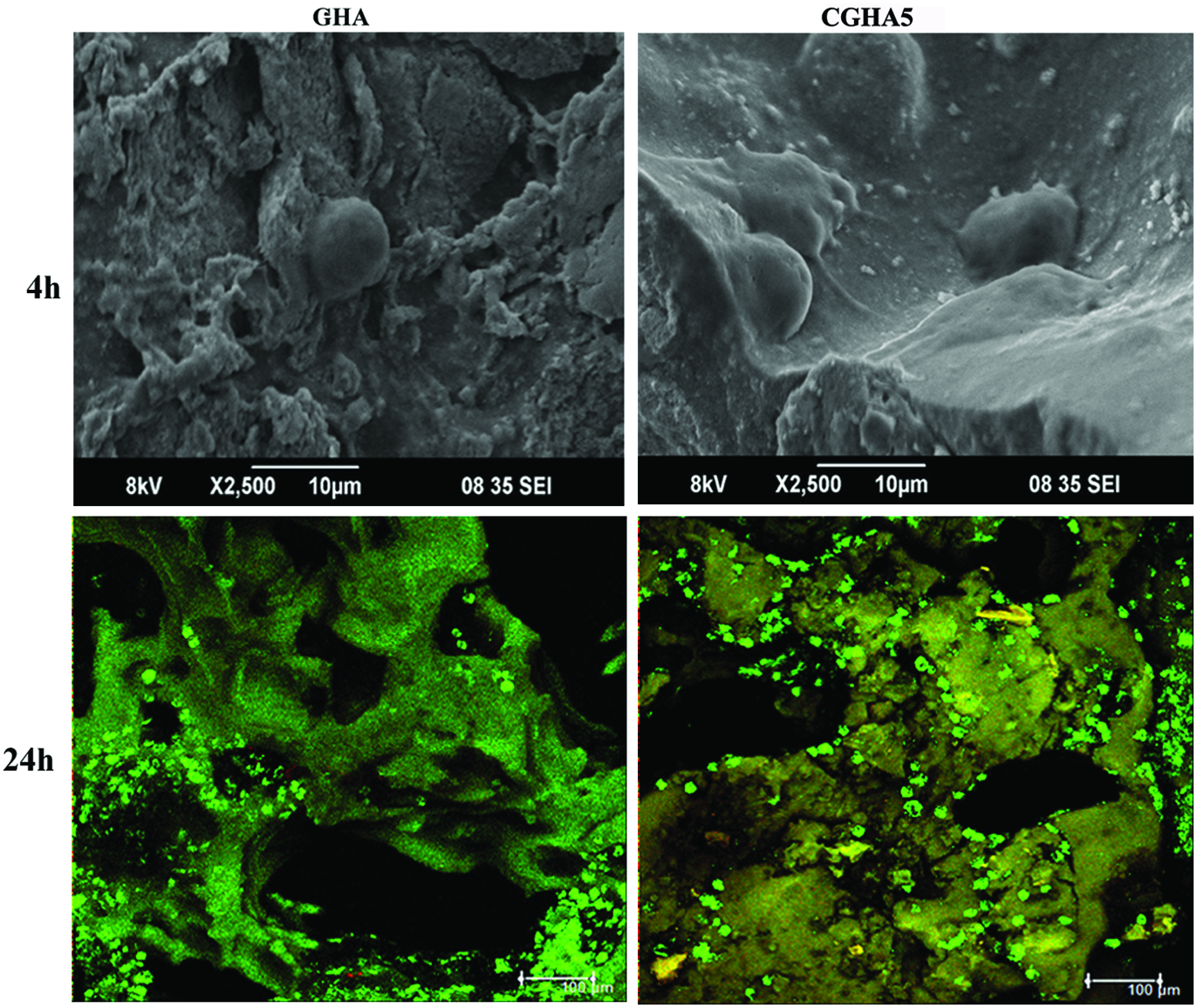
The effect of contact between S. aureus and scaffolds was evaluated by monitoring bacterial viability and adhesion on GHA and CGHA5 scaffolds at 4 h (Fig. 4). The bacterial cells were alive and more in number on GHA scaffolds, while majority of S. aureus were dead in the presence of ciprofloxacin drug on CGHA scaffold. To confirm the same, Alamar blue assay was conducted, which revealed that there was a significant decrease in bacterial viability on CGHA scaffolds (both MSSA and MRSA).

Adhesion and viability of S. aureus on GHA and CGHA5 scaffolds:
In vitro cell culture studies
The concentration of ciprofloxacin released from CGHA10 scaffolds was very high (300 μg/mL for first 4 weeks), so this group was avoided for cell culture studies. Both CGHA (CGHA1, CGHA2, and CGHA5) and GHA scaffolds allowed adhesion, proliferation, and osteogenic differentiation of human ADMSCs. The cells readily attached and spread on both scaffolds (Fig. 5) and these cells were viable up to 21 days (Fig. 6A). Picogreen assay demonstrated that the cells were maintaining a steady-state phase, that is, there was no increase in cell number from day 7 to 21 on all the scaffolds, except CGHA2 wherein the cell number was enhanced on days 14 and 21 when compared to day 7 (Fig. 6B). The ALP activity (μg/mg bovine serum albumin protein) was less on day 1, followed by an increase in activity on day 7, which was again followed by a decrease in activity on days 14 and 21. Thus, the highest activity was on day 7 (Fig. 6C). There was no significant difference in the response of cells cultured on CGHA scaffolds in comparison to GHA scaffolds.
Adhesion and viability of human ADMSCs on GHA and CGHA5 scaffolds. Top panels: scanning electron micrographs; lower panels: confocal micrographs. Scale bar, 100 μm. ADMSCs, adipose-derived mesenchymal stem cells. Color images available online at www.liebertpub.com/tea
Response of human ADMSCs on GHA and CGHA scaffolds:
S. aureus internalized ADMSCs on scaffolds
Our final objective was to perceive the effect of ciprofloxacin on S. aureus (both MSSA and MRSA) internalized within MSCs. The occurrence of GFP-expressing S. aureus within the cytoplasm of MSCs was imaged by confocal and DIC microscopy after 4 h (Fig. 7a–c). Flow cytometry revealed that the percentage of internalization was around 80%. Additionally, the viable bacterial colonies inside human ADMSCs were distinguished by colony count (Fig. 7d–f).
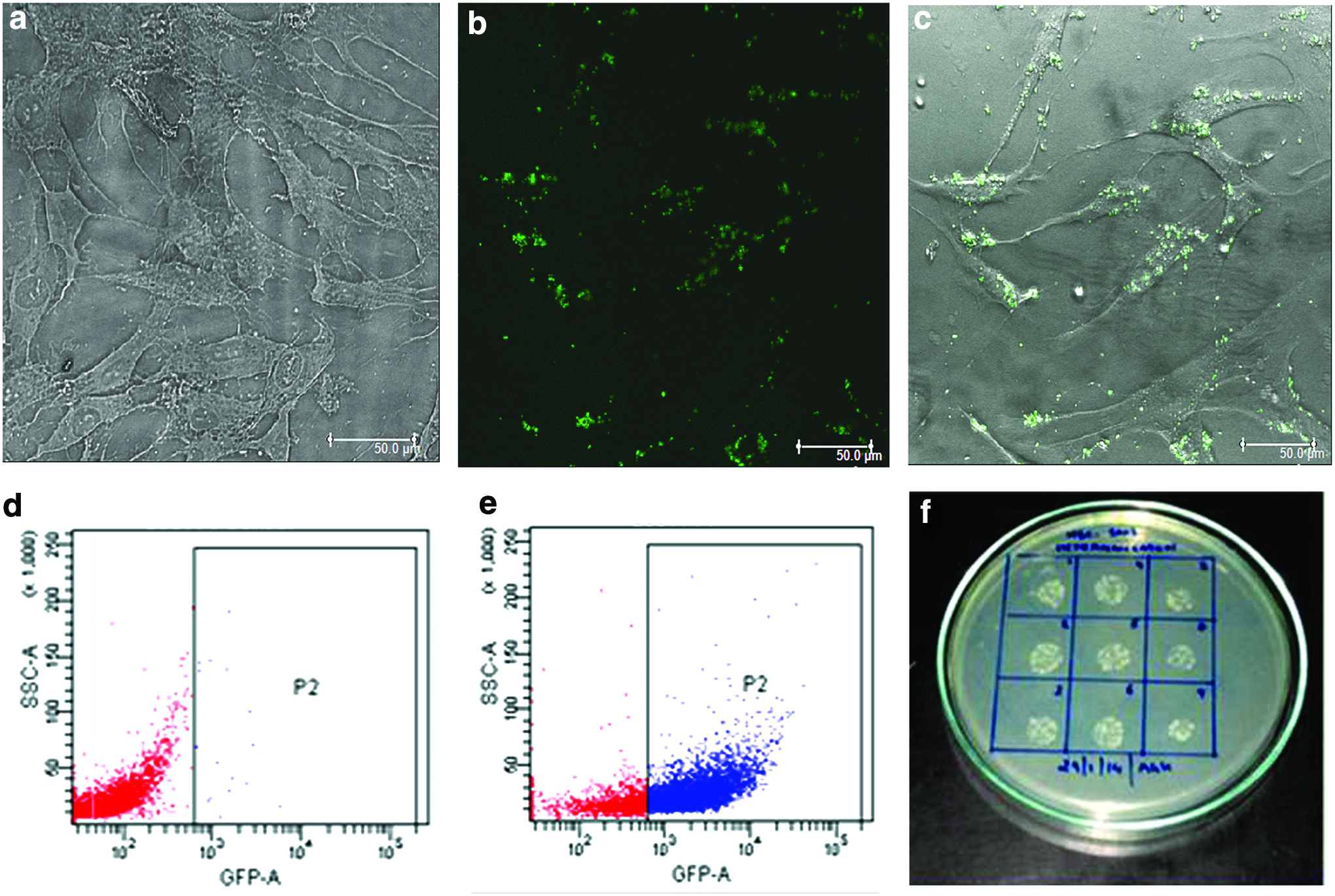
Internalization of S. aureus within human ADMSCs:
Human ADMSCs internalized with S. aureus (MSSA and MRSA, separately) were cultured on GHA and CGHA5 scaffolds and analyzed for live–dead assay as well as ALP activity. The morphology and viability of human ADMSCs were affected after internalization of S. aureus. At 4 h, the human cells were viable and retained their spindle-shaped morphology on CGHA scaffolds, yet the cells were rounded in appearance on GHA scaffolds. At 24 h, the human cells were completely dead on GHA scaffolds, which were then occupied by bacterial cells, resulting in turbidity of the cell culture medium. Interestingly, the human cells on CGHA5 scaffolds retained their viability and the cell culture medium was clear at 24 h. In addition, these cells were able to differentiate into osteogenic lineage on day 7. However, the ALP activity was significantly less when compared to the ALP activity of normal human ADMSCs (cells without infection) induced in osteogenic lineage (Fig. 8A).
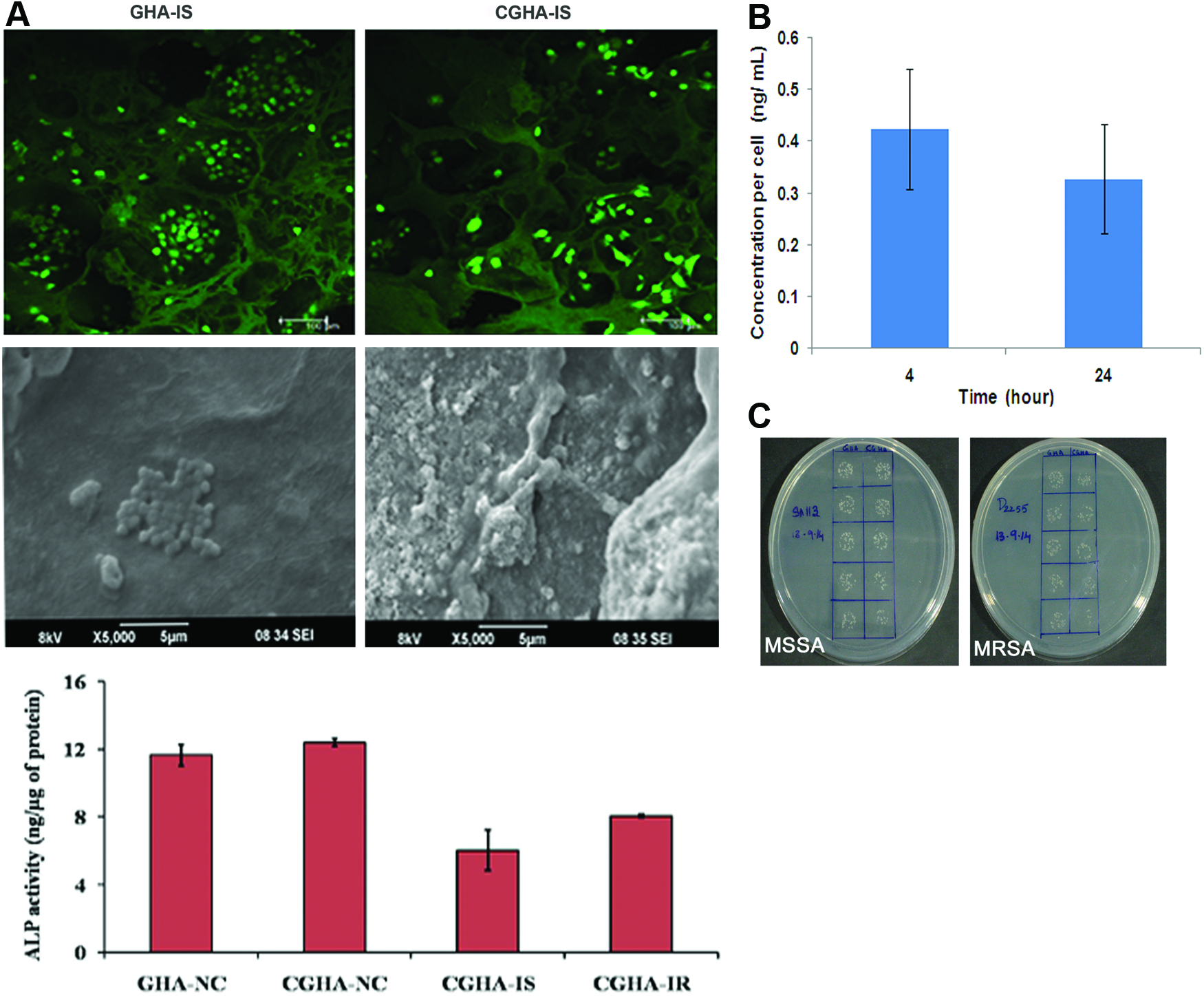
The spectrophotometric analysis of cell lysate has shown that around 400±100 pg of ciprofloxacin could enter into each human ADMSCs. This intracellular concentration of drug was capable of significantly reducing the number of viable bacterial cells (both MSSA and MRSA) within human cells (Fig. 8B).
Discussion
The current treatment protocols for chronic osteomyelitis include prolonged parenteral antimicrobial therapy and surgical debridement of dead bone. 30 Still, patients have recurrent attacks of osteomyelitis, which is probably due to the internalization of S. aureus within bone cells that protect the organism from extracellular host defenses and/or antibiotic therapy. 31 To eliminate bacteria internalized in the osteoblasts, it is necessary to increase the intracellular concentration of antibiotics. Therefore, in this study, a local drug delivery system of gelatin-HAP and ciprofloxacin was developed and its proficiency to target extracellular S. aureus as well as internalized S. aureus within MSCs (both MSSA and MRSA) was investigated. In addition, the compatibility of the ciprofloxacin loaded scaffold toward viability, proliferation, and osteogenic differentiation of normal human ADMSCs was evaluated.
The pore size and porosity of scaffolds are important criteria that affect cellular and vascular infiltration and further bone regeneration. 32 The scaffolds with smaller pores favor chondrogenesis, whereas constructs with larger pores endorse the differentiation of MSCs into osteoblast lineage.33,34 Herein, porous GHA and CGHA scaffolds with pore sizes in the range of 100–550 μm were fabricated by the conventional freeze-drying method. The incorporation of ciprofloxacin into the gelatin-HAP matrix did not alter the pore size and the porous architecture of the scaffolds. There was noncovalent interaction between amino groups of gelatin and carboxyl groups of ciprofloxacin, 35 resulting in better dispersion of ciprofloxacin in the gelatin-HAP matrix. This was verified from the reduction in the intensity of amide and carboxyl-specific peaks of CGHA scaffolds compared to GHA scaffolds. However, the encapsulation efficiency of the CGHA scaffolds was found to decrease with the increasing wt% of ciprofloxacin. This can be attributed to the lesser availability of amide groups (NH2) in gelatin for interaction with carboxyl groups (−COO) of ciprofloxacin as the concentration of drug increased.
Chronic osteomyelitis has been treated traditionally for a period of 4–6 weeks and an ideal local delivery system should provide a sustained release of antibiotics against S. aureus (10–20 times above MIC) for this period. 36 CGHA scaffolds in all wt% released ciprofloxacin, which was well above the MIC against S. aureus. Still, the bioactivity of CGHA1 and CGHA2 scaffolds against MSSA and MRSA was significantly decreased from 4th week compared to initial time points. Thus, CGHA5 scaffolds performed better both in terms of drug release profile and bioactivity when compared to all other scaffolds. It is also important to recognize the percentage of drug remaining in the scaffolds or cumulative antibiotic release, which otherwise may generate antibiotic-resistant strains as in the case of PMMA (PMMA enables only 10% of the loaded drug to diffuse through the polymer). 7 In our study, around 60–80% ciprofloxacin was cumulatively released from each scaffold within 60 days.
There are several empirical models available for simulating drug release from biodegradable scaffolds. 26 The zero-order kinetics states that the rate of drug release is directly proportional to time, whereas the first-order kinetics shows that the rate of drug release is directly proportional to the amount of drug remaining in the system. In the Higuchi model, the release of drug is governed by simple diffusion, and the Korsmeyer–Peppas model describes the release of a drug from a polymeric system. Depending on its value, the release process can be driven by Fickian diffusion (n=0.5), polymeric matrix erosion, or the combination of both mechanisms. 26 In our study, ciprofloxacin release from the scaffolds was best fit to the zero-order and the Korsmeyer–Peppas models, irrespective of the concentration (Table 1). Therefore, the rate of drug release was proportional to time and it occurred by simple diffusion through the pores of the gelatin polymer.37,38
Ciprofloxacin at a higher dose had a detrimental effect on osteoblast functions and may delay bone healing. 9 Thus, the main challenge was to maintain the concentration above MIC for antibacterial activity, without creating toxicity to stem cells or osteoblasts. The concentration of the drug released from the scaffolds was optimal, so there was no significant difference in the proliferation, viability, and ALP activity of the cells cultured on CGHA scaffolds in comparison to GHA scaffolds. ALP is a noncollagenous protein expressed during the early point of osteogenic differentiation. 39
Our final objective was to perceive the effect of ciprofloxacin on S. aureus (both MSSA and MRSA) internalized within MSCs. For this, S. aureus was internalized at an MOI of 30:1, as reported earlier. 40 Gentamicin was used for washing extracellular bacteria since its ability to penetrate through the eukaryotic cell membrane is poor and it cannot kill S. aureus within MSCs. 40 When human ADMSCs were internalized with MSSA and MRSA separately and cultured on CGHA5 scaffolds, the cells were viable after 24 h and able to differentiate into osteogenic lineage on day 7. This suggests the ability of ciprofloxacin to penetrate through the cell membrane and eliminate bacteria inside the cells. In addition, the intracellular concentration of the drug was capable of significantly reducing the number of viable bacterial cells within human cells (Fig. 8B). The intracellular concentration of ciprofloxacin obtained in our study was well above a previous report, which showed only 0.7 pg of ciprofloxacin within normal bone marrow-derived MSCs.
There are many reports that have demonstrated the persistence of S. aureus within osteoblast cells for a long period, compounding bone loss. 41 However, the MSSA and MRSA strains used in our study have damaged host cells after 4 h and could not persevere inside the cell for long periods. However, our experimental data suggest that this local delivery system can be used to target against internalized S. aureus capable of living inside osteoblasts. Further research is required with different strains of bacteria to fully exploit the potential of the ciprofloxacin loaded gelatin-HAP scaffold for osteomyelitic treatment.
Conclusion
We have developed a porous, gelatin-HAP scaffold loaded with four different concentrations of ciprofloxacin drug (1,2,5 and 10 wt%). All the scaffolds displayed sustained release of ciprofloxacin against MSSA and MRSA for 60 days. The drug release profile was fit to zero-order and Korsmeyer–Peppas models. When compared, the gelatin-HAP matrix with 5 wt% ciprofloxacin has shown appreciable performance in terms of drug release profile as well as bioactivity against MSSA and MRSA for 60 days. Ciprofloxacin could penetrate into human ADMSCs and significantly reduce the number of viable bacterial cells, resulting in the osteogenic differentiation capability of infected cells. At the same time, the scaffolds displayed no adverse effects on normal human ADMSCs.
Footnotes
Acknowledgments
The research was funded by the Science and Engineering Research Board, Department of Science and Technology, Government of India (DST fast track project) (Project No. SR/FT/LS-65/2012). Lakshmi got her M.Tech. fellowship from DST, India. The authors acknowledge Mr. Sajin P. Ravi, Mr. Sarath, and Dr. Sreerekha for technical help and Dr. R. Jayakumar for providing the ciprofloxacin drug.
Disclosure Statement
No competing financial interests exist.