
Abstract
Vascularization of bioartificial tissues can be significantly enhanced by the generation of an arteriovenous (AV) loop. Besides the surgical vascularization, the choice of the scaffold and the applied cells are indispensable cofactors. The combination of alginate dialdehyde and gelatin (ADA–GEL) and mesenchymal stem cells (MSCs) is a promising approach with regard to biocompatibility, biodegradation, as well as de novo tissue formation. In this study, we targeted the investigation of the vascularization of ADA–GEL with and in the absence of encapsulated MSCs in the AV loop model. A Teflon chamber filled with ADA–GEL microcapsules was placed in the groin of Lewis rats and an AV loop was placed into the chamber. Group A encompassed the ADA–GEL without MSCs, whereas group B contained 2 × 106 DiI-labeled MSCs/mL ADA–GEL. Four weeks postoperatively, tissue formation and vascularization were investigated by histology and microcomputed tomography. We were able to prove vascularization originating from the AV loop in both groups with statistically significant more vessels in group B containing MSCs. Moreover, encapsulated MSCs promoted biodegradation of the ADA–GEL microcapsules. In the present study, we were able to demonstrate for the first time, the successful vascularization of ADA–GEL microcapsules by means of the AV loop. Furthermore, ADA–GEL displayed a good biocompatibility and encapsulation of MSCs into ADA–GEL microcapsule-enhanced vascularization as well as biodegradation.
Introduction
T
Hydrogels are commonly used biomaterials for tissue engineering applications because they offer several interesting features. Hydrogels are characterized by a high porosity facilitating oxygen and nutrition supply. Due to their high water content, hydrogels represent a tissue like environment. 12 Furthermore, cells can be encapsulated into hydrogels protecting them from external influences upon transplantation. Although there are manifold hydrogels, such as fibrin, hyaluronic acid, or collagen, most of them seem to be unsuitable for tissue engineering applications due to a fast degradation rate or poor mechanical properties. 13 Hydrogels consisting of crosslinked alginate dialdehyde (ADA) and gelatin (GEL) display a good biocompatibility and biodegradability as well as proangiogenic characteristics.14–18
Due to their easy isolation and the ability to differentiate into multiple cell types, MSCs are a promising cell source for the generation of bioartificial tissues. 19 Moreover, MSCs display several interesting characteristics under hypoxic conditions, such as increased migration, proliferation, and reduced cell death. 20
The aim of this study was to prove the intrinsic vascularization of ADA–GEL microcapsules in the AV loop model. Furthermore, MSCs were encapsulated into ADA–GEL microcapsules to analyze the effect of MSCs on the intrinsic vascularization.
Materials and Methods
The animal experiments were approved by the Animal Care Committee of the University of Erlangen and the Government of Mittelfranken, Germany (AZ 54-2532.1-24/09, AZ 54-2532.1-9/13-2).
MSC isolation and cultivation were performed according to established protocols. Briefly, one male Lewis rat (Charles River Laboratories, Sulzfeld, Germany) was sacrificed, the femoral bones removed, the bone marrow flushed with phosphate buffered saline and fetal calf serum (Biochrom, Germany).18,21 After centrifugation, the cell pellet was resolved in Dulbecco's modified Eagle's medium (Gibco/Life Technologies, Carlsbad) containing 20% fetal bovine serum (Biochrom AG, Berlin, Germany), 1% penicillin/streptomycin (Gibco Invitrogen), and 1%
Production of ADA–GEL microcapsules
The ADA–GEL microcapsules were produced according to an established protocol. 22 Briefly, sodium alginate was oxidized to ADA with metaperiodate allowing covalent crosslinking of ADA and GEL in a 1:1 ratio. The final concentration of the ADA–GEL hydrogel amounted to 5% w/v ADA and 5% w/v GEL. For cell encapsulation 2 × 106 DiI-labeled MSCs were added per milliliter of ADA–GEL. The ADA–GEL microcapsules were generated immediately before implantation.
AV loop implantation
Eighteen male Lewis rats (Charles River Laboratories) with a body weight of 320–470 g underwent AV loop implantation. The operations were performed by one surgeon (L.F.) under general anesthesia with isoflurane (Baxter, Vienna, Austria) using an operating microscope (Carl Zeiss, Oberkochen, Germany). First, an incision was placed in the left groin and the femoral vessels were identified and prepared. The same procedure was performed on the contralateral side with the exception that the right femoral vein was gathered. One AV loop was created on the left side by interposing the vein graft from the right side between the femoral artery and vein. A Teflon chamber, with a capacity of 1 mL, was placed in the left groin, filled with the first half of the ADA–GEL microcapsules, and the AV loop was embedded on the matrix. Then the second half of the ADA–GEL microcapsules was added, the Teflon chamber sutured on the thigh musculature, and the skin closed (Fig. 1).
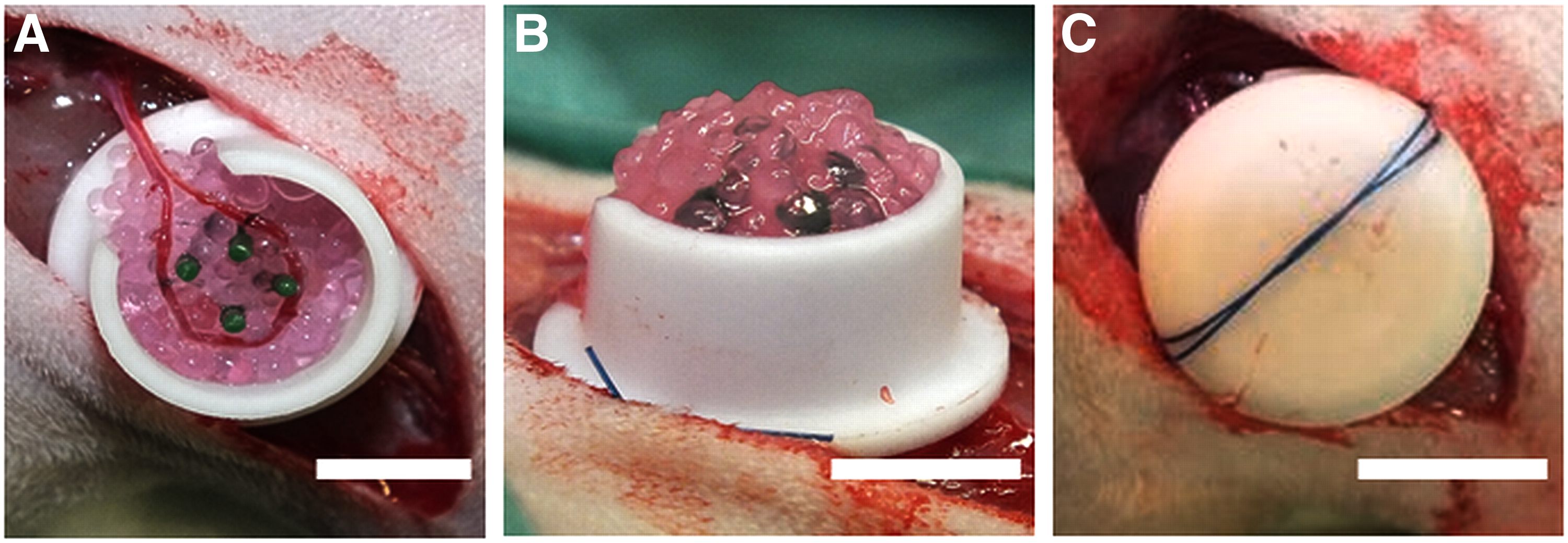
Implantation of the AV loop in the left groin of Lewis rats (scale bar ≙5 mm). First, the Teflon chamber was half filled with the ADA–GEL microcapsules. Thereafter, the AV loop was placed and the second half of the ADA–GEL microcapsules added
Group A (n = 8) encompassed the ADA–GEL microcapsules without cells, whereas group B (n = 10) comprised the ADA–GEL microcapsules with 2 × 106 DiI-labeled MSCs. After the surgical procedure, the animals received enoxaparin adapted to the body weight (10 mg/kg) for 2 days. Four weeks postoperatively, the constructs were explanted and microcomputed tomography (μCT) scans as well as histological analyses performed.
Explantation procedure
Microfil® perfusion (Flow Tech, Inc., Carver) was performed 4 weeks after AV loop implantation to visualize vascularization of the constructs. Briefly, a median laparotomy was performed, the descending aorta cannulated, and the inferior caval vein cut. After flushing the vascular system with Ringer heparin (100 IU/mL) solution, 20 mL Microfil MV-122 solution with 0.6 mL curing agent was applied intravenously. Then, the descending aorta and inferior caval vein were ligated and the specimen placed at 4°C overnight. Afterward, the constructs were explanted, embedded in formalin, and μCT scans as well as histology performed.
μCT analysis
Each extracted AV loop was examined on a Skyscan 1172 μCT (Skyscan, Kontich, Belgium) fitted to an 11 megapixel detector. The X-ray tube operated at 80 kV and 100 μA using an additional Al 0.5 mm filter to cutoff low-energy X-rays (most <40 kV). Each loop was scanned with a rotation step = 0.4° over 360°, an exposure time = 445 ms per slice and a random movement = 10 at a resolution of 8.00 μm per pixel. Reconstruction of the raw data sinograms was done with the tomographic software N Recon Client and Server 1.6.9 with GPU support (Skyscan). Segmentation was done using the software Amira 5.6 (FEI, Berlin, Germany) applying a global threshold to the three-dimensional image stack creating a label image field. To extract the vessel network and defining the network segments an auto skeletonization algorithm subroutine was applied. A local Euclidian distance map is generated by structure thinning and separating into segments. Based on this distance map, the segment diameter is determined by gradual expansion until the vessel outline is reached. Based on the segment data (length, diameter, volume) over several AV loops, a cumulated vessel diameter distribution with a certain histogram size is calculated.
Histological staining
After μCT analysis, the constructs were embedded in paraffin. Thereafter, we performed 3 μm cross sections, exact at the same level and perpendicular to the longitudinal axis of the AV loop. Besides Hematoxylin and Eosin and Masson's Trichrome staining, 4′,6-diamidino-2-phenylindole (DAPI) staining was carried out following standard protocols.
ED1 immunostaining was performed to identify macrophages. Briefly, the slides were treated with a blocking solution using the ZytoChem-Plus AP Polymer-Kit (Zytomed Systems GmbH, Berlin, Germany). Thereafter, the slides were incubated with an anti-ED1 primary antibody (Serotec) in a 1:300 dilution overnight. After a washing step, a second alkaline phosphatase-labeled anti-mouse antibody (AP-Polymer) was added and Fast Red TR/Naphthol AS (Sigma) substrate applied. Counterstaining was performed with hemalaun. To visualize the structure of the newly formed vessels, endothelial cells were stained with biotinylated isolectin B4 from Bandeiraea simplicifolia (Sigma) and smooth muscle cells were detected with an alpha smooth muscle actin (α-SMA) antibody (Dako GmbH) as previously described. 6 To detect hypoxic cells we performed hypoxia-inducible factor 1α (HIF-1α) staining. According to Yuan et al. a cooking step at 121°C was performed for antigen retrieval. 23 Immunostaining was carried out corresponding to the manufacturer's protocol. After the blocking procedure, using the ZytoChem-Plus AP Polymer-Kit (Zytomed Systems GmbH), the slides were incubated with a primary monoclonal mouse HIF-1α antibody (Novus Biologicals, Littleton) in a 1:10,000 dilution overnight. Afterward, a second alkaline phosphatase-labeled anti-mouse antibody (AP-Polymer) and the Fast Red TR/Naphthol AS (Sigma) substrate were added.
Microphotographs were obtained using an Olympus IX81 microscope (Olympus, Hamburg, Germany) and digital camera under 40 and 100-fold magnification. Afterward, the microphotographs (only 40-fold magnification) of each individual cross-section were merged into a high-resolution overview image with cellSens Dimension V1.5 software (Olympus). For the detection of DiI-labeled MSCs, we performed fluorescence images with a Leitz DMRBE microscope (Leica Microsystems, Wetzlar, Germany) and a Leica DFC420 camera under 100-fold magnification. To analyze the spatial assignment of the DiI-labeled MSCs, we performed overlays with DAPI staining. DiI-labeled MSCs and cells positive for HIF-1α were automatically counted with ImageJ (NIH, Bethesda, MD).
Automatic quantification of the vascularization
We used a custom-made program written in MATLAB for the automatic quantification of the vascularization as previously described. 6 Briefly, “negative experts” (such as cell nuclei or the sample background) and “positive experts” (vessels) were defined and the images of the histological cross-sections were transformed into RGB color space. Thereafter, the pixels were classified into the abovementioned experts and the parameters “total number of vessels” as well as “cross-section area” calculated by the program.
Statistical analysis
Statistical analysis was performed with GraphPad Prism 7.00 (GraphPad Software, San Diego, CA). Unpaired student's t-test was used and p-values ≤0.05 were considered statistically significant. Data are shown as mean arbitrary units ± standard deviation.
Results
Surgical outcome and macroscopic appearance
In group A all animals survived. One animal died postoperatively in group B. Two specimens from group B had to be excluded from analysis due to construct dislocation or insufficient Microfil perfusion. The animals tolerated the chambers well and no further complications were observed.
Histological analysis
Microphotographs of histological cross-sections revealed no complete degradation of the constructs after 4 weeks. Constructs containing encapsulated MSCs displayed a statistically significant smaller construct area compared with ADA–GEL microcapsules without MSCs (1.15 ± 0.256× 107 μm2 vs. 1.46 ± 0.366 × 107 μm2) (Fig. 2). Furthermore, ADA–GEL microcapsules containing MSCs displayed a rather irregular surface compared with the cell-free ADA–GEL microcapsules. Except fibrovascular tissue between the ADA–GEL microcapsules, we were not able to prove newly formed bone tissue in the constructs (Figs. 3 and 4). ED1 staining was carried out to label macrophages as a surrogate parameter for immunoreaction. Although ED1-positive cells were present, with predominance in the newly formed fibrovascular tissue between the microcapsules, no multinuclear giant cells were detected in both groups. Furthermore, we were not able to prove an impact of encapsulated MSCs on immunoreaction (Fig. 5). DiI-staining of MSCs before implantation displayed the presence of MSCs in the constructs after 4 weeks, with most of the MSCs in the central parts of the ADA–GEL microcapsules. DiI-positive cells were quantified with ImageJ demonstrating that most of the MSCs were located in peripheral parts of the constructs. Besides DiI-positive MSCs, we proved the presence of nucleated cells in the ADA–GEL microcapsules with DAPI staining (Fig. 6).
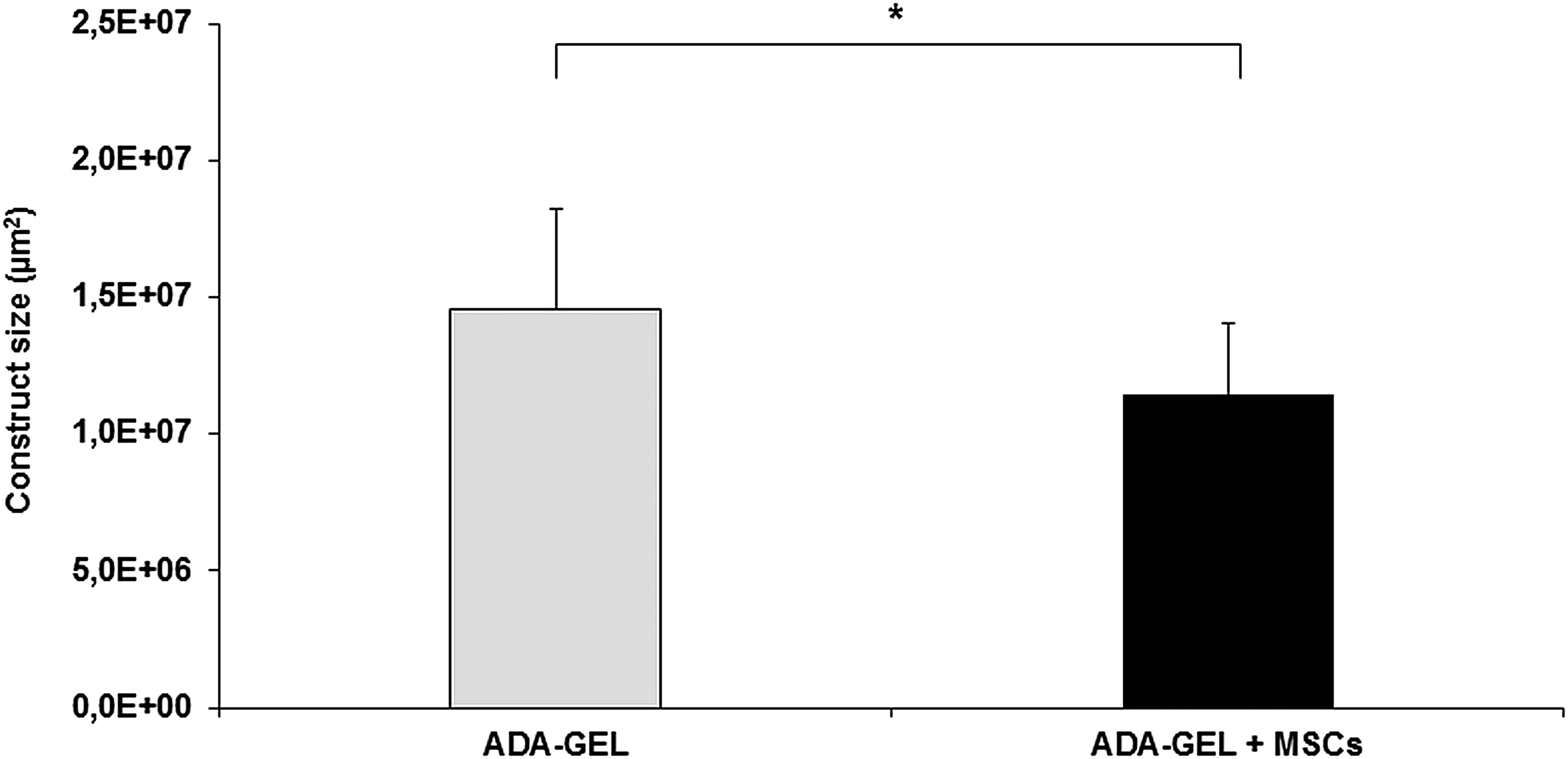
Determination of the construct area revealed significant smaller constructs in group B containing MSCs. Statistically significant differences between the different groups are indicated for *p < 0.05. MSC, mesenchymal stem cell.

Hematoxylin and Eosin staining with 40 [

Masson Trichrome staining with 40 [

ED1 staining demonstrating the presence of macrophages (red cells) with no multinuclear giant cells. Images were made under 40 [
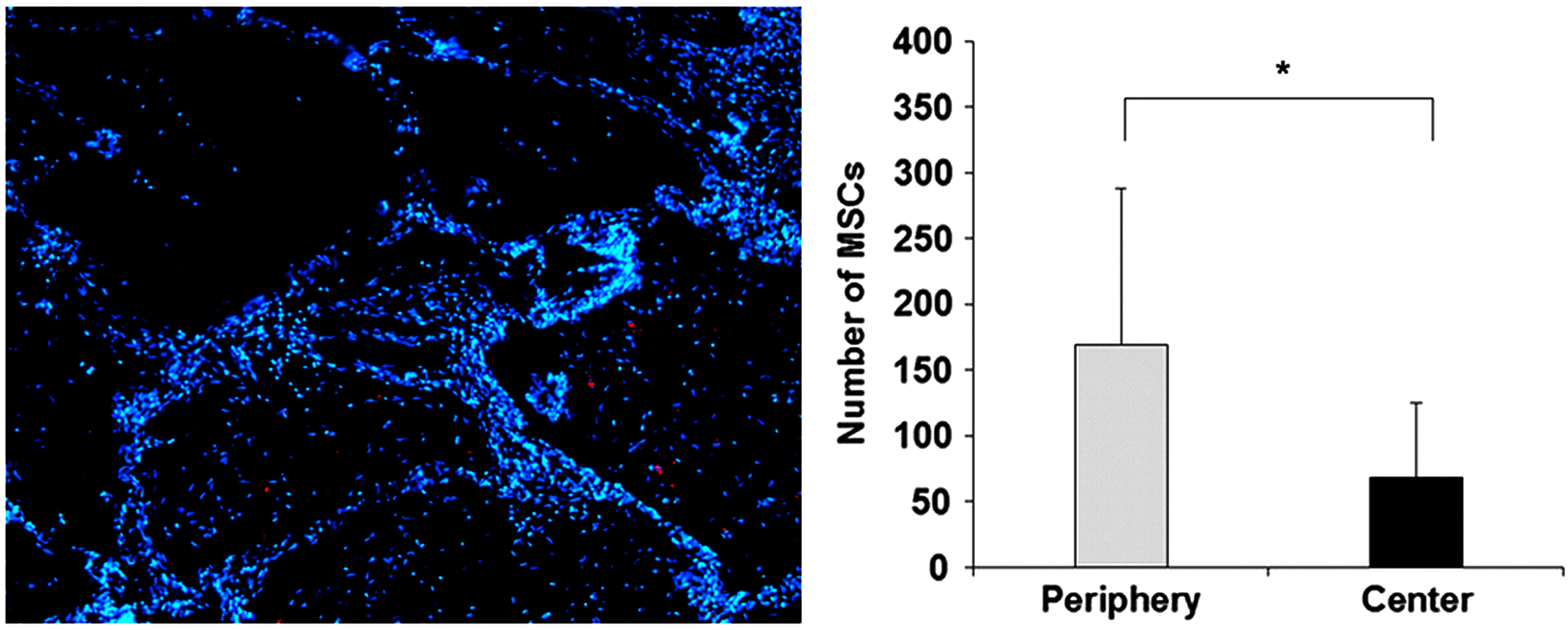
DiI and 4′,6-diamidino-2-phenylindole staining revealing the presence of MSCs 4 weeks after implantation with most MSCs located in the peripheral part of the construct. Statistically significant differences are indicated for *p < 0.05. Color images available online at www.liebertpub.com/tea
Histological evaluation of the vascularization revealed a patency rate of 62.5% in group A (n = 8 specimen) and 71% in group B (n = 7 specimen) with five patent AV loops per group. Newly formed fibrovascular tissue was located between the ADA–GEL microcapsules with predominance around the AV loops (Figs. 3 and 4). We were not able to prove the presence of vascular structures in the microcapsules. The lumen of the newly formed vessels was filled with black Microfil. The total number of vessels per cross-section was statistically significantly higher in group B encompassing MSCs (174 ± 105 vessels vs. 31 ± 24 vessels). Also, the average vessel area per cross-section was statistically significantly larger in the ADA–GEL group containing MSCs (97859 ± 83581 μm2 vs. 13418 ± 11219 μm2) (Fig. 7).
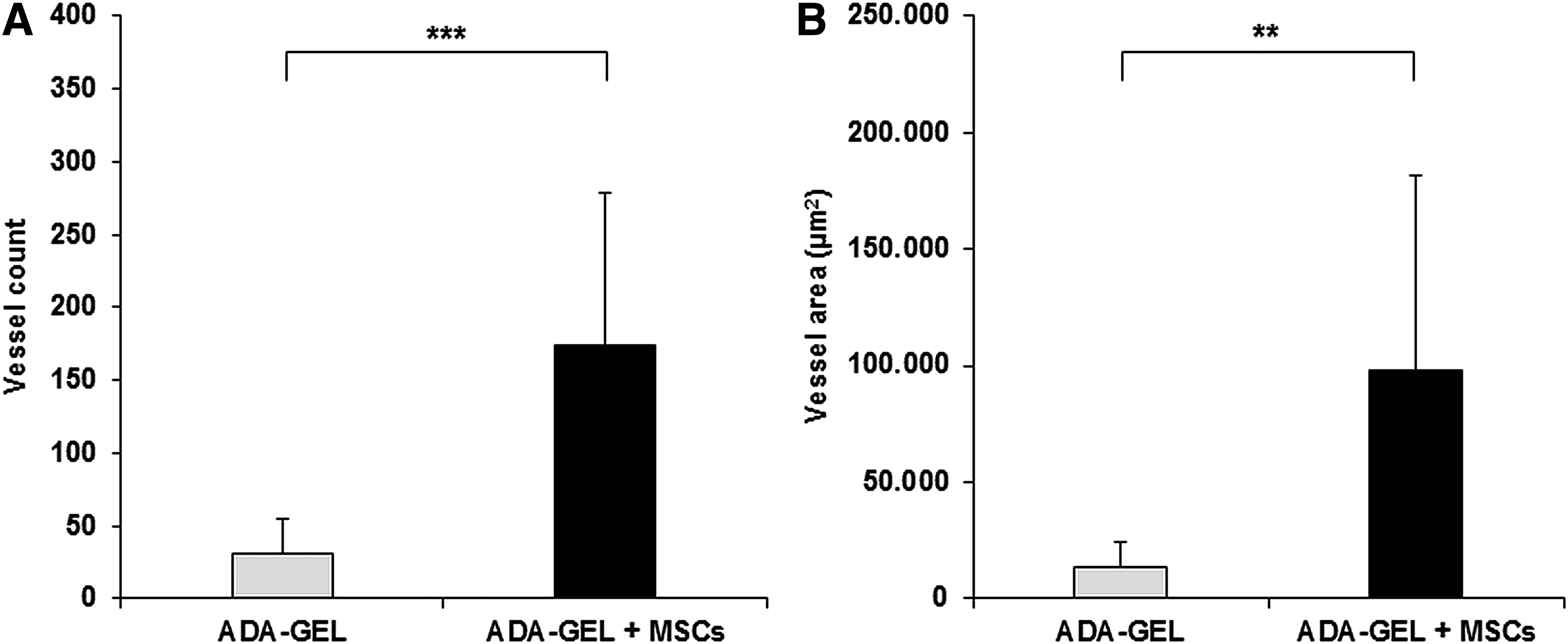
Automatic quantification of the vascularization. Encapsulating MSCs into ADA–GEL microcapsules statistically increased the vessel number
Comparing the mean vessel size between both groups we detected larger vessels in the ADA–GEL group containing MSCs without statistically significant differences (486 ±379 μm2 vs. 630.4 ± 509.7 μm2). Lectin staining revealed endothelial cells within the inner surface of the neovessels. Moreover, the newly formed vessels comprised smooth muscle cells within the vessel wall proved by α-SMA staining. The Microfil was located intravascularly and was not distributed in the connective tissue, as a sign of the integrity of the newly formed vascular network (Figs. 8 and 9).
Immunohistological lectin staining demonstrating the presence of endothelial cells (brown-colored vessels). Images were made under 40 [

Immunohistological α-SMA staining demonstrating the presence of smooth muscle cells inside the vessel walls cells (red-colored vessels). Images were made under 40 [
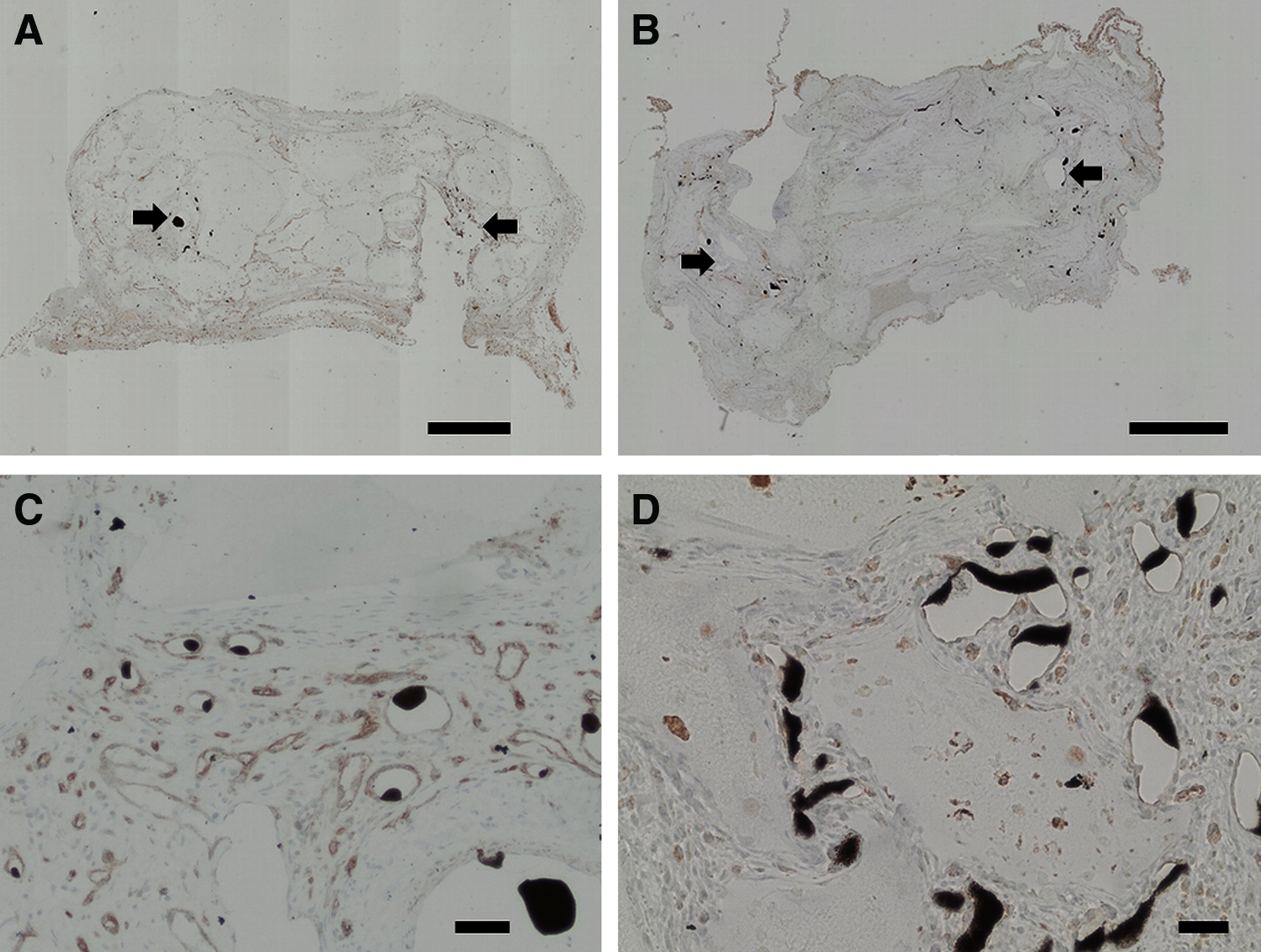
In both groups, we were able to detect cells producing HIF-1α in the fibrovascular tissue between the ADA–GEL microcapsules (Fig. 10). Interestingly, cells producing HIF-1α were located in the peripheral as well in the central parts of the constructs with no predominance. Although there was a trend with more HIF-1α-positive cells in the ADA–GEL group without MSCs, no statistically significant difference between both experimental groups was evident (Fig. 11).

Immunohistological HIF-1α staining. Images were made under 40 [
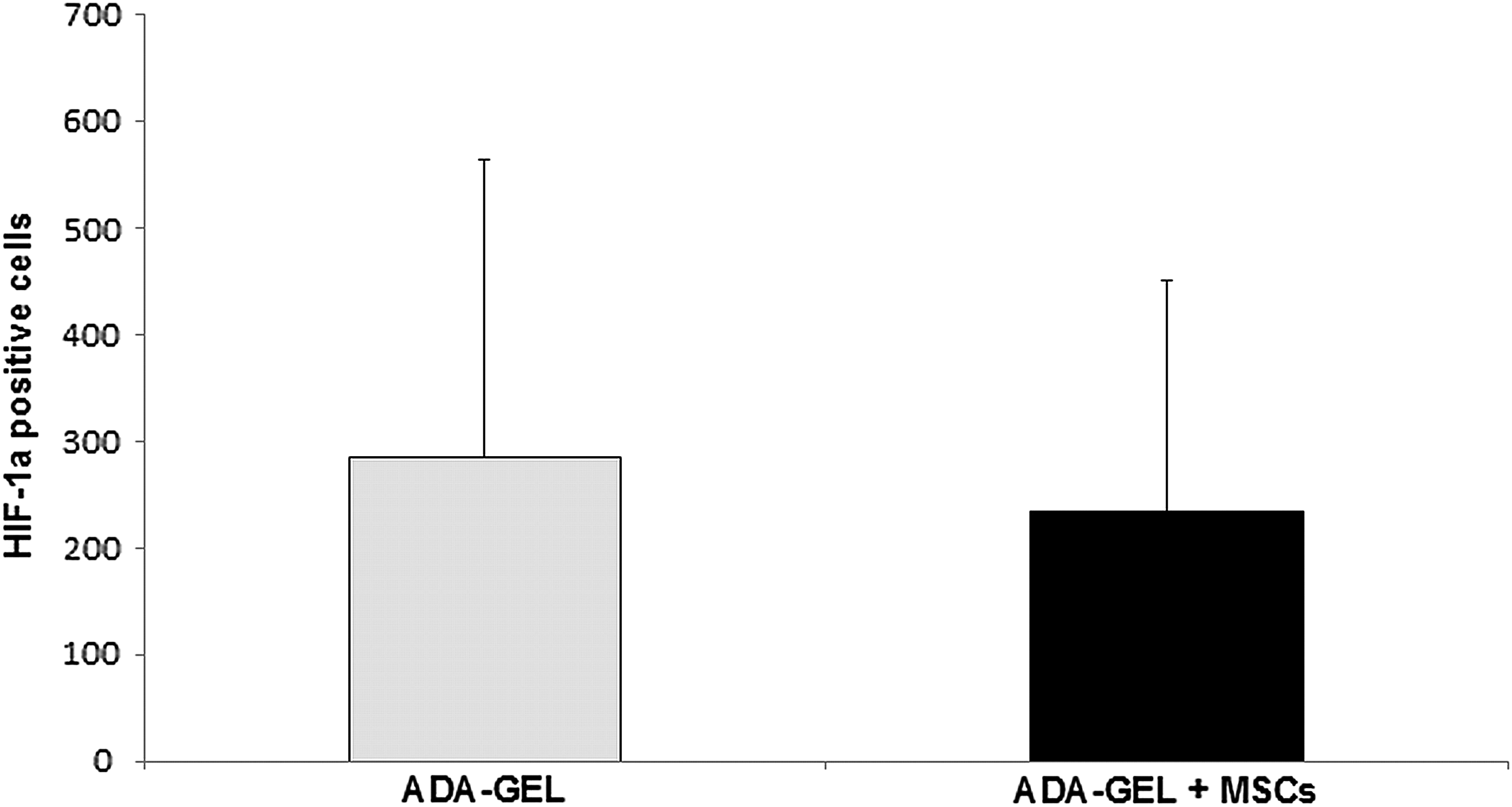
Quantification of cells positive for HIF-1α. The ADA–GEL group containing MSCs displayed fewer cells producing HIF-1α without statistically significant difference.
μCT analysis
From both groups all constructs underwent μCT analysis. Concordant to the results from the histological analysis five from eight constructs were patent in group A and five from seven constructs were patent in group B. As demonstrated in two representative μCT reconstructions, the vascularized area in constructs containing MSCs was larger (Fig. 12A, B). Considering the cumulative vessel length, group B also displayed a significant larger cumulative vessel length compared to group A (31886 ± 8524.5 μm vs. 20842.6 ± 8062.7 μm; p ≤ 0.05) (Fig. 12C). Considering the vessel radius and the corresponding cumulative vessel length, we could prove that most vessels of the newly formed vascular network displayed a radius between 75 and 275 μm.
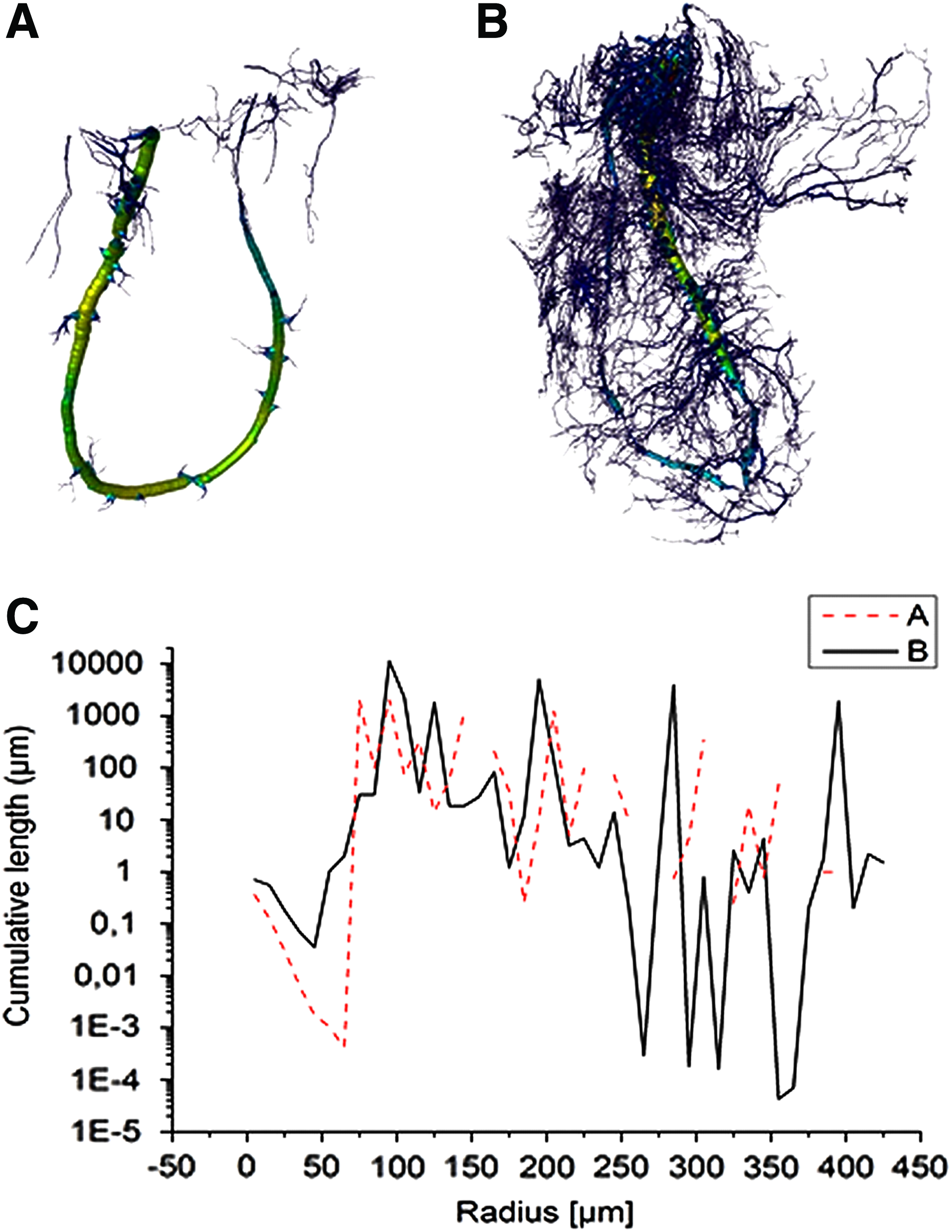
Microcomputed tomography reconstruction of cell-free
Discussion
Despite medical advance, the reconstruction of large-volume tissue defects is a current problem due to donor-site morbidity and tissue availability. For this purpose engineering of bioartificial tissues has gained much interest in the field of regenerative medicine.
However, the transplantation of tissue-engineered constructs into a host organism is critically limited by insufficient nutrient and oxygen supply in the early postimplantation phase. To overcome this problem, tissue-engineered constructs were combined with endothelial cells24,25 or angiogenic growth factors, such as VEGF 26 to accelerate the formation of a vascular network and to reduce consecutive cell death of transplanted cells.
The so-called prefabrication is another approach to axially vascularize bioartificial tissues by means of an AV loop, as first described by Erol and Sira. 3 In this context we proved vascularization of various biomaterials, such as fibrin gel, HA/β-TCP, or 45S5 bioactive glass by means of the AV loop.5,6,8 Our studies also demonstrate that the first 2 weeks have to be regarded as the critical time period for transplanted cells due to insufficient nutrient and oxygen supply. Interestingly, growth factor supplementation could not promote earlier vascularization originating from the AV loop. 11
Besides the improvement of vascularization, the choice of the appropriate biomaterial as well as the cell type, are indispensable for tissue engineering applications. In this context hydrogels may represent an ideal biomaterial as a carrier substrate for cell transplantation because their high porosity facilitates oxygen and nutrition supply. Moreover, cells can be encapsulated into a tissue-like environment and thereby protected from external mechanical influences. 12 On the contrary to alginate, used as a common wound dressing, ADA–GEL has no clinical application so far. 27 But, in the context of tissue engineering and cell encapsulation, alginate is a widely used hydrogel. Based on the pertinent literature, alginate and GEL display a good biocompatibility in vivo with positive effects on angiogenesis or bone formation.16,28,29 On the other hand pure alginate displays a dense hydrogel structure, low biodegradability, high stiffness, and lacks cell adhesion molecules restricting cellular growth and migration. 30 In previous studies Boccaccini and colleagues 31 established a promising hydrogel with oxidized alginate (ADA), which was covalently crosslinked with GEL, the so-called ADA–GEL. Compared with alginate or modified alginate with RDG-motives ADA–GEL displays a better cytocompatibility and biodegradation. In this regard, MG-63 cells, fibroblasts, MSCs and adipose derived stem cells (ADSCs) were successfully encapsulated into ADA–GEL microcapsules showing excellent cellular growth, viability, and migration.18,30–32 Moreover, it has been shown that ADA–GEL supports VEGF release, cell survival, as well as metabolic activity compared with other hydrogels. 31 Furthermore, a combination of ADA–GEL with bioactive glass, such as 45S5, was successfully tested in vitro indicating excellent cytocompatible material properties. 18
Due to their easy isolation from the bone marrow with a tolerable donor-site morbidity and the potential to differentiate into multiple cell types, including adipocytes, osteoblasts, or endothelial cells, MSCs represent a promising cell source for tissue engineering applications.19,33–35
Based on these findings, we seeded MSCs onto ADA–GEL films and could prove good cytocompatibility in vitro as indicated by cell viability and proliferation. Moreover, we could demonstrate incipient angiogenesis as well as a low immunoreaction of subcutaneous implanted ADA–GEL microcapsules after 4 weeks. 18 As the next consequent step, we performed intrinsic vascularization of ADA–GEL microcapsules with or without MSCs by means of the AV loop. We have successfully demonstrated intrinsic vascularization of constructs containing ADA–GEL microcapsules after 4 weeks.
Focusing on vascularization, our findings demonstrate that ADA–GEL displays a less dense vascular network compared with fibrin as a hydrogel matrix. In a previous study, Teflon chambers were filled with fibrin, and intrinsic vascularization was induced by means of an AV loop. After 4 weeks, statistically significant more vessels were present in the fibrin group compared with ADA–GEL (106.88 ± 24.99 vs. 31 ± 24; p = 0.001). 11 In another study, Teflon chambers were filled with fibrin as well as a porous HA/β-TCP matrix (TricOs®) and intrinsic vascularization was induced with the AV loop. 36 After 4 weeks, 42 ± 19 newly formed vessels were detected per cross-section without statistical significance compared with the ADA–GEL group (31 ± 24; p = 0.44).
Although we observed the formation of fibrovascular tissue between the ADA–GEL microcapsules we were not able to prove the presence of newly formed vessels inside the ADA–GEL microcapsules in both groups. In this regard, the generation of smaller ADA–GEL microcapsules, with a more advantageous surface-area-to-volume ratio, might enhance the biodegradation and thereby the vessel ingrowth into the ADA–GEL microcapsules.
Furthermore, we observed that encapsulation of MSCs into ADA–GEL microcapsules enhanced vascularization originating from the AV loop. Compared with constructs containing a composite matrix of fibrin and TricOs, we were able to prove statistically significantly more vessels after 4 weeks (174 ± 105 vs. 42 ± 19, p = 0.02). 36 Moreover, there is a tendency toward more vessels in the ADA–GEL group containing MSCs compared with constructs using fibrin as a matrix (174 ± 105 vs. 106.88 ± 24.99; p = 0.2). 11
In another study, osteogenic-induced MSCs and/or bone morphogenetic protein (BMP)-2 were incorporated into a fibrin/TricOs matrix and intrinsic vascularization was induced by means of the AV loop. 6 After 6 weeks, statistically significantly more vessels were evident in the matrix containing MSCs. It is alluring to speculate that incorporating MSCs might induce a stronger vascularization than BMP-2.
Our findings are in accordance with the pertinent literature indicating that MSCs promote vascularization, especially under hypoxic conditions.35,37,38 Kinnaird et al. demonstrated that MSCs produce angiogenic cytokines, such as VEGF and bFGF, under hypoxic conditions and thereby enhance vascularization. 39 It is well known that the proangiogenic transcription factor HIF-1α is a key regulator for the production of VEGF. In both experimental groups, we were able to prove cells positive for HIF-1α. Interestingly, the majority of the transplanted DiI-labeled MSCs was detected in the peripheral and presumed hypoxic parts of the constructs with predominance in the central parts of the ADA–GEL microcapsules. Taking into consideration that MSCs migrate into hypoxic tissues regulated through HIF-1α40,41 and ADA–GEL can promote VEGF secretion of encapsulated cells, 31 it is alluring to speculate that both mechanisms might enhance vascularization.
Biocompatibility and biodegradation are important material properties for tissue engineering applications. Although MSCs are described as immunomodulatory cells, we could not observe an impact of MSCs on immunoreaction. 42 A possible explanation for this finding might be the good biocompatibility of ADA–GEL without triggering a severe immunoreaction.
Regarding biodegradation, there should be an inverse correlation between biomaterial degradation and neotissue formation. 43 We proved a larger construct area of constructs containing ADA–GEL compared with fibrin gel after 4 weeks indicating a slower degradation rate of ADA–GEL (1.46 × 107 μm2 vs. 5 × 106 μm2). 10 Furthermore, the degradation of ADA–GEL could be significantly enhanced by encapsulating MSCs. This phenomenon could be explained by the fact that MSCs express MT1-MMP. 37 MT1-MMP is a matrix metalloproteinase involved in the degradation of the extracellular matrix and in angiogenesis as well.44–46 Considering the fact that ADA displays a slow degradation rate, other ratios of ADA and GEL might enhance the degradation of ADA–GEL microcapsules. In a previous in vitro study, Sarker et al. could demonstrate that an increasing GEL content in ADA–GEL hydrogels correlated with a higher cell proliferation, viability, and hydrogel degradation. 47 Also the generation of smaller ADA–GEL microcapsules with a better surface-area-to-volume ratio might enhance the degradation of the ADA–GEL microcapsules as well as the nutrition of encapsulated cells.
Our study demonstrated that encapsulation of MSCs stimulated the formation of a vascular network originating from the AV loop. Although MSCs are widely used in bone tissue engineering applications we could not detect the formation of newly formed bone tissue. Moshaverinia et al. subcutaneously implanted encapsulated MSC-alginate microbeads into the dorsum of mice and demonstrated ectopic bone formation 8 weeks postimplantation. 48
In a former study, we induced osteogenic differentiation of MSCs before transplantation into a titanium chamber containing a β-TCP/HA matrix. Intrinsic vascularization was performed by the generation of an AV loop and after 6 weeks the formation of bone tissue could be observed. Moreover, the addition of BMP-2 stimulated the bone formation in this study. 6 The results of our ADA–GEL study led to the presumption that a longer observation period than 4 weeks, osteogenic differentiation of MSCs before implantation, and/or the addition of BMP-2 might induce bone formation. Furthermore, a modification of the ADA–GEL microcapsules could induce the osteogenic differentiation of MSCs. In this context Wang et al. combined hydrogels consisting of alginate and GEL with bioactive glass and proved enhanced proliferation as well as mineralization of SaOS-2 cells. 49
Conclusion
In the current study, vascularization of constructs containing ADA–GEL microcapsules was successfully achieved by the generation of an AV loop. Encapsulating MSCs into ADA–GEL microcapsules improved vascularization and biodegradation. In conclusion, constructs of axial vascularized constructs consisting of ADA–GEL and encapsulated MSCs represent a promising approach for the generation of bioartificial tissues.
Footnotes
Acknowledgments
This study was funded by the “Emerging Fields Initiative” (TOPbiomat) and the ELAN-Fonds (14-08-22-1-Steiner) of the University of Erlangen-Nürnberg. The authors gratefully acknowledge the DFG (SFB TRR 225) for support. We thank Prof. Greil and Mr. Reinhardt for kindly producing the Teflon chambers. The present work is part of L.L's doctoral thesis for obtaining the degree “Dr. med.” The authors cordially thank Alexander Haydl for proof reading the article.
Disclosure Statement
No competing financial interests exist.