
Abstract
To treat coronary heart disease, coronary artery bypass grafts are used to divert blood flow around blockages in the coronary arteries. Autologous grafts are the gold standard of care, but they are characterized by their lack of availability, low quality, and high failure rates. Alternatively, tissue-engineered small-diameter vascular grafts made from synthetic or natural polymers have not demonstrated adequate results to replace autologous grafts; synthetic grafts result in a loss of patency due to thrombosis and intimal hyperplasia, whereas scaffolds from natural polymers are generally unable to support the physiological conditions. Extracellular matrix (ECM) from a variety of sources, including cell-derived, 2D, and cannular tissues, has become an increasingly useful tool for this application. The current review examines the ECM-based methods that have recently been investigated in the field and comments on their viability for clinical applications.
Impact statement
In reviewing extracellular matrix (ECM)-based small-diameter vascular grafts, we have thoroughly and concisely summarized the foundational work in the field, in addition to exploring the recent developments and approaches used. Due to the plethora of research articles for constructing vascular grafts, we dedicated this review to focus on grafts from ECM to provide a more comprehensive look at this specific technology.
Introduction and Motivation
Cardiovascular disease (CVD) is the primary cause of death globally and kills 17 million people each year. 1 CVD encompasses a range of conditions, including coronary heart disease, which is characterized by the stenosis or occlusion of blood vessels surrounding the heart. 1 Treatment for CVD includes lifestyle changes to reduce risk factors, medications, and surgeries such as coronary artery bypass grafting (CABG). 2 First utilized in the 1950s, CABGs divert blood flow around a blockage in the coronary artery by using a small-diameter vascular graft. 3 Today, there are about 400,000 CABGs performed each year in the United States, alone. 4
Autologous grafts, largely from the saphenous vein and internal mammary artery, are the current gold standard for bypasses, but they are an insufficient treatment in both the approach and the results. Autologous grafts are limited by quality and availability from the donor; ∼25% of patients requiring arterial bypass procedures do not have saphenous veins that are acceptable for implantation. 5 The isolation of autologous grafts requires a secondary surgical site and risks donor site morbidity. 6 In addition, the harvesting process and subsequent assessment of the graft before implantation can damage the vessel and lead to endothelial dysfunction, a pro-inflammatory response, and ultimately thrombosis and graft occlusion.7–9 Postoperative failure of saphenous vein grafts is largely due to technical failure or thrombosis within the first month, intimal hyperplasia within the first year, and atherosclerosis after the first year. 10 These issues result in a 10% failure rate after the first month and a 50% failure rate at 10 years.11–13 The high failure rates render this method of treatment largely inadequate, which has led to the development of non-autologous alternatives.
Tissue engineering techniques utilizing synthetic and natural polymers fall short for small-diameter (<6 mm) vascular grafts. Commercially available synthetic grafts composed of polyethylene terephthalate/Dacron and polytetrafluoroethylene/Teflon (ePTFE) function well for large-diameter vascular grafts, but they perform poorly in small-diameter applications.14–16 Generally, small synthetic grafts are characterized by a lack of an endothelium, high modulus, and low compliance, which often lead to thrombosis and intimal hyperplasia.17–21 Alternatively, natural polymers such as collagen and fibrin have been investigated for small-diameter grafts because they are biocompatible and biodegradable and promote endothelialization.22–24 Natural polymers exhibit an elastic modulus that is more comparable to native vessels, and they do not illicit a chronic inflammatory response.22,25,26 However, they possess substantially lower strengths than physiologically required and can degrade faster than the body regenerates.2,23,26–28 These types of grafts have been reviewed extensively and will not be addressed further.28–31
Another material that has been increasingly examined for vascular graft engineering endeavors is extracellular matrix (ECM). The composition of this three-dimensional fibrous network produced by cells depends on the type of tissue, but largely includes collagen, fibronectin, laminin, glycosaminoglycans (GAGs), and growth factors.32–36 This material is obtained through the decellularization of tissue, where the cellular and nuclear matters are removed through physical, chemical, and enzymatic approaches.36–38 The ECM provides both physical support and biological cues to cells that direct cell adhesion, proliferation, and differentiation.38,39 When utilized in tissue engineering scaffolds, ECM encourages constructive remodeling and favorable clinical outcomes.40,41 Specifically in vascular applications, collagen,42,43 fibrin, 44 fibronectin, 45 laminin,46,47 chondroitin sulfate, 48 and vascular endothelial growth factor (VEGF) 49 have been shown to encourage endothelialization. However, ECM components can also lead to platelet activation and thrombosis,50–52 so it is important to consider the individual components, as well as the overall composition of the ECM. In addition to its bioactivity and biocompatibility, the ECM has demonstrated mechanical properties that are comparable to those of native vessels.38,53–55 The ECM has been employed for tissue-engineered vascular grafts in three major ways: cell-derived ECM, extracted 2D tissues, and extracted cannular tissues (Fig. 1). Cell-derived grafts are those created from the culture of cells either in a cannular shape or in a monolayer. After the cells have produced ample ECM, the structures are decellularized. In addition, isolated 2D and cannular tissues can be used to develop grafts through the use of decellularization and surface modifications. Grafts can be implanted acellularly or endothelialized with autologous endothelial cells (ECs).
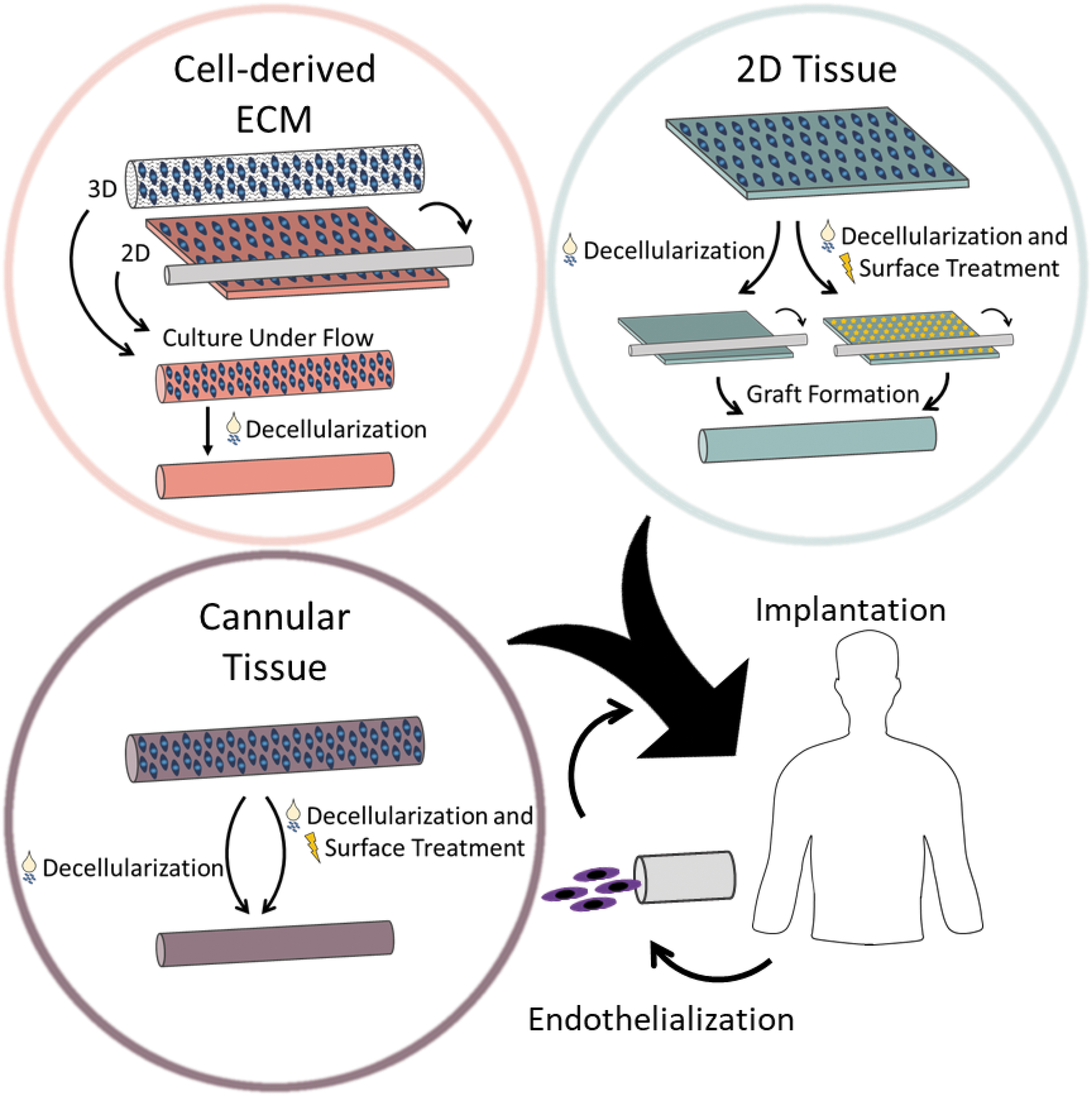
ECM-based technologies, including cell-derived ECM, 2D tissue, and cannular tissue, for small-diameter vascular graft scaffolds. Cell-derived ECM grafts are developed through weeks of cell culture before decellularization, in either a 3D or 2D geometry. The 3D geometry method employs a scaffold to support cell growth, whereas the 2D method utilizes cell sheets to wrap around a mandrel. Vascular grafts can be constructed from decellularized 2D tissue by using sutures or glue, whereas cannular tissues only need to be decellularized. ECM from 2D and cannular tissue sources frequently undergo surface treatment to improve the outcome of the graft. Vascular grafts can either be implanted directly or endothelialized with the patient's own cells before surgery. ECM, extracellular matrix.
Arteries have a relatively simple function, to carry blood away from the heart; however, they have a complex structure that can be difficult to recapitulate. To support the high pressures, flow rates, and shear stresses, arteries have a thicker wall and smaller lumen diameter than veins. 56 The vessel wall is composed of three layers: tunica intima, tunica media, and tunica adventitia. 57 The innermost layer, the tunica intima, contains the endothelial lining, which is imperative to the prevention of platelet adhesion and thrombosis.17,35,58 When the endothelial lining is damaged, the artery is susceptible to infection, thrombosis, and intimal hyperplasia.31,56,59,60 The tunica media, the middle layer, contains both elastin and smooth muscle and largely controls the mechanical functionality of the vessel.56,61 The smooth muscle cells (SMCs) in this layer have a contractile phenotype, characterized by the presence of smooth muscle actin (SMA), calponin, smooth muscle myosin heavy chain (SM-MHC), SM22-α, and smoothelin. 62 Further, SMCs can transition between a quiescent, contractile phenotype and a proliferative, synthetic one.62,63 The outermost layer, the tunica adventitia, is predominantly composed of collagen, but it contains elastin, fibroblasts, and adipocytes.56,58 The elastin and collagen contribute to a sophisticated two-region mechanical behavior of the arterial wall.61,64 Each of these elements must be considered during the development of new approaches for constructing vascular grafts.
To create a truly viable and sustainable solution for patients, many different requirements need to be satisfied. Overall, the vascular graft must demonstrate biocompatibility, meaning it is nontoxic, nonimmunogenic, and nonthrombogenic. 65 It should be easy to remodel, complete with a confluent, quiescent, and nonactivated endothelium.28,31,65 It is vital that the vascular graft mimics the complex mechanical behavior of native arteries, including the modulus, circumferential strength, burst pressure, and suture retention strength.28,65,66 Vascular grafts must be more patient friendly, in that any human-derived elements should be isolated noninvasively. In addition, grafts should have short production times, low costs, and off-the-shelf availability to maximize their clinical impact.28,67
In this review, we explore the ECM-based approaches, namely cell-derived ECM, extracted 2D tissues, and extracted cannular tissues, used to develop small-diameter vascular grafts and summarize the recent approaches in Tables 1, 2, and 3, respectively. Further, we provide our analyses on the impact of each method and the future direction of small-diameter vascular graft research. The search terms for this review included, but were not limited to, “small diameter,” “vascular graft,” “extracellular matrix,” and “decellularized.” We focused on papers published within the past 5 years that developed small-diameter grafts for applications in CABG surgeries. Articles reporting on vascular grafts that were larger than 6 mm in diameter or utilized materials that were not ECM based, such as polymers or hydrogels, were excluded from this review.
Summary of Recent Cell-Derived Extracellular Matrix Approaches for Small-Diameter Vascular Grafts
ECM, extracellular matrix; PDMS, polydimethylsiloxane; hDF, human dermal fibroblast; PGA, polyglycolic acid; hSMC, human smooth muscle cell; hiPSC, human induced pluripotent stem cell; EC, endothelial cell.
Summary of Recent Two-Dimensional Tissues for Small-Diameter Vascular Grafts
HUVEC, human umbilical vein endothelial cell; SIS, small intestine submucosa; GA, glutaraldehyde.
Summary of Recent Cannular Tissues for Small-Diameter Vascular Grafts
bFGF, basic fibroblast growth factor; VEGF, vascular endothelial growth factor.
Cell-Derived ECM
Niklason et al. have played a critical role in laying the groundwork for and progressing the cell-based ECM approach for small-diameter vascular grafts. Their work has utilized either SMCs (bovine,68,69 porcine,54,68 canine, 70 human70,71) or human mesenchymal stem cells (hMSCs) 72 to seed onto a polyglycolic acid (PGA) mesh scaffold. After 8–10 weeks of culture, these grafts demonstrated appropriate vessel wall thickness, collagen content, suture retention strength, and burst pressure.68,69 Overall, these grafts have shown good long-term patency in vivo in both baboon and canine models. 70 Further, they were utilized in clinical trials for hemodialysis access in patients with end-stage renal disease with promising patency trends: 15% primary patency, 25% primary assisted patency, and 80% secondary patency at 2 years. 71 Despite the positive results in animal studies and progression to hemodialysis access clinical trials, the PGA mesh foundation has caused several complications. Namely, the degradation and residual fragments of PGA trigger a shift in SMC phenotype from a contractile to a synthetic one with lower expression of myosin, SMA, and calponin.68,69,73,74 The shift to the synthetic phenotype is detrimental to the regulation of vessel diameter 62 and is a precursor to intimal hyperplasia 62 and atherosclerosis. 63
Various methods have been implemented to eliminate the use of the polymer scaffold. Growing monolayers of cells and wrapping these cell sheets around a removable mandrel was first introduced by L'Heureux et al.75,76 This method has been applied to nanograted polydimethylsiloxane to create aligned cell sheets of hMSCs and either human dermal fibroblasts (hDFs) 77 or human endothelial progenitor cells (hEPCs). 78 These cell sheets were rolled and cultured under flow, which resulted in a vascular graft with circumferential cell alignment.77,78 Xing et al. demonstrated the corresponding anisotropic behavior and moduli, both similar to the behavior of native arteries. 77 Further, the grafts stained positive for SMA and SM22-α, indicating contractile SMC phenotypes, and showed increased cell–cell communication. 77 Jung et al. demonstrated a functional endothelium and low, but ample burst pressure, although this assembly was largely geared toward drug testing models. 78 Another alternative method is culturing either hSMCs or hMSCs around pillars to form rings of cells and then culturing these rings together to allow the layers to fuse to one another. 79 Although the hSMCs did not retain their contractile phenotype, the hMSC-cultured grafts did, as demonstrated by the expression of SMA and SM22-α. 79 Syedain et al. developed a vascular graft from culturing hDFs in bovine fibrin gel for 5 weeks before decellularization, which resulted in grafts with burst pressure and suture retention strength comparable to human arteries. 80 Grafts implanted in baboons for 3 and 6 months demonstrated patency values of 83% and 60%, respectively, but showed evidence of thrombosis on the luminal surface at explantation. 80
The in vivo success of acellular grafts falls on the ability of the host cells to infiltrate the scaffold, which can be a challenge for patients with vascular cells of reduced remodeling capacity, a large demographic of CABG recipients. Previously addressed with autologous ECs, one new approach to circumvent the decellularization step is incorporating allogeneic human induced pluripotent stem cell (hiPSC)-derived cells. hiPSCs are an invaluable tool in the tissue engineering field, because they serve as a possible avenue to create a “universal” cell bank that does not induce an immune response and does not require decellularization.81,82 Although hMSCs have been investigated for this reason, 83 research has expanded the use of hiPSCs due to their pluripotency. hiPSCs were differentiated into SMCs and cultured on PGA mesh for a total of 8–9 weeks. 84 Although these grafts allowed blood flow and demonstrated cell infiltration in nude rats for 1 and 2 weeks, histologically the grafts appear collapsed with irregular lumens. 84 A secondary study incorporated a cyclic strain during the 8 weeks of graft culture, which increased burst pressure and suture retention strength. 82 These grafts were patent in nude rats over 30 days and expressed markers for a contractile and mature SMC phenotype, including SMA, calponin, and SM-MHC, as well as ECM markers for collagen I and elastin. 82 The ECs can also be derived from iPSCs and have been incorporated in vascular grafts. hiPSC-derived ECs were seeded on the lumen of vascular grafts fabricated from hiPSC-derived SMCs cultured on PGA mesh for a total of 3–9 weeks. 85 The walls of the grafts that underwent 6 and 9 weeks of culture were very thick, but they have visibly more SMA when compared with those at 3 weeks of culture. 85
One imperative advancement to transition cell-derived scaffolds into a clinical technology is the reduction of cell culture time, as an avenue to increase production capacity and control cost. von Bornstädt et al. assembled a vascular graft by using alternating layers of SMC and fibroblast cell sheets, reinforced with Dermabond Advanced tissue glue. 86 The grafts were perfused with human umbilical vein endothelial cells (HUVECs) for 24 h and then cultured for 2 weeks. 86 After the 2 week culture period, grafts demonstrated ample burst pressure to support physiological conditions, which increased after 8 weeks in vivo to values comparable to native rat femoral arteries. 86 A continuous endothelial lining and appropriate media and adventitia layers were confirmed, suggesting no incidence of intimal hyperplasia. 86
Impact and clinical outlook
Grafts fabricated by using the cellular method are useful because they are largely patient independent, with the exception of autologous ECs, and can be fabricated ahead of time to keep patient wait times short. Although early cell-derived grafts composed from animal cells required decellularization, recent endeavors to develop these types of grafts employ human cells and largely do not undergo decellularization. We speculate that this shift is driven by the ultimate goal of mitigating an immune response without the need for decellularization through the utilization of patient-specific cells or cells from a “universal” cell bank. However, the cell culture required to produce ample cell populations, in addition to the graft culture, is extremely time-consuming, resource-intensive, and expensive. Although substantial progress has been made in improving graft function and patency of cell-based grafts, which resulted in a clinical trial for hemodialysis access, little work has been completed to improve the feasibility of clinically implementing this technology, predominately in terms of reducing culture time. We predict that by cutting the culture period, the amount of resources required and cost will decrease, rendering cell-based vascular grafts a more practical solution. In the context of the 400,000 CABG grafts implanted each year and the millions of cells necessary for each graft, there are logistics-related obstacles to investigate to scale this technique to meet the current needs of patients. Further, due to the established effects of cell source, specifically the age and health of the donor, on cell function,87–89 we anticipate that the source will affect not only cell expansion and cell sheet culture, but also graft functionality and success. Advancing the use of allogeneic hiPSCs in these grafts may serve as an alternative to the variables associated with cell donors. Despite the difficulties associated with the application of this technique, cell-derived ECM technologies provide the unique opportunity for further investigation into the largely unexplored area of the effect of ECM composition, which can be controlled through cell type and culture time, on in vivo endothelialization.
Two-Dimensional Tissue
Porcine small intestine submucosa (SIS) is a commonly used 2D tissue scaffold and it was first employed by Badylak et al. in its native state as a large-diameter vascular graft. 90 Although early SIS grafts had low patency results that were comparable to autologous saphenous vein grafts, they demonstrated appropriate mechanical properties similar to those of native vessels in terms of burst pressure, elastic modulus, and compliance.91–93 The HUVECs cultured on decellularized SIS demonstrated higher proliferation and appeared more evenly spread with a cobblestone morphology, when compared with the ePTFE and Dacron alternatives. 44 Although these characteristics are indicative of better endothelialization, an important mechanism in preventing platelet adhesion, 17 both native and decellularized SIS grafts are prone to thrombosis.91,94
Endothelialization of the lumen and a variety of surface treatments, including the immobilization of heparin and growth factors, have been employed to prevent thrombosis and improve the patency of SIS grafts. The culture of ECs for 1 week on the lumen of a SIS graft, glued with fibrinogen and thrombin, preserved the graft patency ex vivo. 95 In a follow-up study, these grafts were treated with fibrin and SMCs before endothelialization and implanted into sheep for 3 months. 96 Over this time, grafts with and without SMCs were similar in their diameters, flow rates, and homogenously endothelialized lumens that were free from clotting, intimal hyperplasia, and loss of patency. 96 Although cell infiltration occurred quicker in SMC grafts, by 3 months the cell densities were comparable. 96 The SMC grafts had significantly more collagen, which suggests a higher maturation of cells and higher macrophage invasion. 96 Han et al. used plasma treatment to immobilize heparin on the surface of decellularized SIS before it was sutured into a vascular graft and implanted into adult dogs for 6 weeks. 94 The heparin treatment was vital to the patency of the grafts; all 10 treated grafts were patent and showed an endothelial lining without any signs of thrombosis, whereas scaffolds without heparin quickly occluded due to thrombi. 94 Similarly, both heparin and VEGF were immobilized on laminated SIS tubes before implantation in female sheep for 1 week, 1 month, and 3 months. 93 Eleven of the 12 grafts demonstrated patency without any thrombosis and developed a confluent endothelium within 1 month with SMC infiltration at 3 months. 93
In addition to SIS, surface modifications have been utilized in an assortment of 2D tissues, including bovine Achilles tendon and Hypophthalmichthys molitrix-derived swim bladders. Thin layers of decellularized bovine Achilles tendon were layered around a Teflon mandrel and soaked in an elastin and glutaraldehyde (GA)-containing solution. 97 The control group with GA treatment-only had a similar modulus to native arteries, whereas the addition of elastin lowered the modulus of the material. 97 Further, these grafts had lower than necessary burst pressure values. 97 The in vitro cell culture of SMCs and ECs showed that they aligned with the collagen fibers and demonstrated appropriate morphologies: spindle-shaped and cobblestone, respectively. 97 Liu et al. utilized Hypophthalmichthys molitrix-derived swim bladders, a unique source of collagen I-rich ECM, for applications in small-diameter vascular grafts. 98 After the swim bladder was isolated and decellularized, both unfixed and GA-fixed tissues showed reduced calcification with no visible pro-inflammatory M1 macrophages in a subcutaneous study in Wistar rats. 98 Then, both treated and untreated swim bladder was rolled and secured with tissue adhesive to create vascular grafts. 98 Grafts were implanted in rats for 4 weeks, with the GA-treated grafts demonstrating improved patency over the non-treated grafts, likely due to the increased strength and stiffness with GA treatment. 98 In addition, the grafts exhibited an established endothelium without any sign of intimal hyperplasia. 98
One alternative to surface treatment is to develop grafts with materials that naturally resist thrombosis. Human amniotic membrane (hAM) discourages platelet adhesion and activation. 99 Amensag et al. used decellularized hAM and thrombin glue to form a six-layered graft that supported the culture of SMCs, which ultimately increased the elastic modulus and GAG content, but decreased the physiological modulus. 100 All three acellular grafts displayed significant remodeling and remained patent after 4 weeks in New Zealand white rabbits, although there was thrombus formation in one graft. 100 Alternatively, bovine pericardium, a nonthrombogenic source of ECM, 101 is frequently used clinically as a vascular patch, 102 but it has only recently been employed for small-diameter vascular grafts. 103 Vascular grafts composed of decellularized bovine pericardium, coupled with poly(propylene fumarate), demonstrated a modulus similar to native vessels, with ample burst pressure and suture retention strength to support physiological pressures. 103 Although both grafts remained patent for 2 weeks in Lewis nude rats without any indication of thrombosis, the new ECM present may be indicative of the onset of intimal hyperplasia. 103
With a similar structure as a coronary artery, sheets of decellularized porcine aorta have also been utilized as small-diameter vascular grafts. However, human arteries are stiffer than porcine aortas and other porcine arteries.104–106 Wu et al. circumvented the mechanical mismatch across the two species by covering the porcine aorta graft with electrospun polyurethane. 106 The polyurethane increased stiffness of the graft and supported the in vitro 2D cell culture of HUVECs and normal hDFs (NHDFs) for 2 weeks. 106 In a study by Negishi et al., sheets of porcine aorta were decellularized by using high hydrostatic pressure since traditional detergent-based methods of decellularization, including SDS and Triton X-100, did not work. 107 The decellularized tissue was fastened into a cylindrical shape with either fibrin glue or sutures and although both methods supported physiological pressures in vitro, the sutured grafts leaked in vivo. 107 Glued grafts implanted into Wistar rats for 3 weeks remained patent with some endothelial-like cells present on the intima layer, but ultimately they showed low cell infiltration likely due to the higher elastin content. 107
Impact and clinical outlook
Vascular grafts from 2D tissues can be readily constructed after decellularization, essentially without any patient wait times. Acellular grafts that do not contain any autologous cells must rely solely on the recipient for cell infiltration and remodeling, which may be troublesome for patients whose cells have limited regenerative capability and exacerbated by the unexplored effects of ECM composition on endothelialization for 2D ECM sources. Although pre-seeding patient-specific cells or iPSC-derived cells on the grafts may preserve patency and encourage remodeling, we believe that it limits the off-the-shelf availability of such grafts. To develop a clinically relevant small-diameter vascular graft from 2D tissue, it is crucial for the graft to match the properties of human arteries and support endothelialization.28,65,66 Therefore, we infer that the selected ECM should mimic the mechanics, structure, composition, and hemocompability of human coronary arteries, as opposed to the cell-based method earlier, in which these properties can largely be controlled through the types of cells used and the length of cell culture. Further, the incorporation of surface modifications to decrease the incidence of thrombosis, although a possible avenue forward, necessitates an additional step to treat the surface, which contributes to the complexity of the graft and can impact mechanical properties. Consequently, we propose that the effects of each processing step be carefully explored.
Cannular Tissue
The majority of recent investigations into small-diameter vascular grafts originating from cannular tissues utilize either human- or animal-derived arteries or veins. Since the geometry of the vessel and the layer of SMCs can make thorough decellularization more difficult, harsher decellularization methods may be required. Thus, the effects of decellularization protocols on ECM integrity must be addressed, as previously summarized.108–110 Simsa et al. found that regardless of the dynamics of the detergent application, porcine vena cava samples could be successfully decellularized without any cytotoxicity to HUVECs and displayed comparable values for mechanical properties, as well as elastin and GAG content. 111 However, scanning electron microscopy analysis revealed the presence of remnant cell debris on the static samples and local tears and a flattened luminal surface in grafts decellularized at the highest perfusion velocity, which could be detrimental to in vivo endothelialization. 111 Simsa et al. concluded that the agitation and low velocity perfusion methods of decellularization had the best overall outcomes. 111 Meanwhile, Böer et al. compared a “conventional” decellularization protocol against an “intensified” one, where the “intensified” version included a mandrel to prevent tissue collapse, three times more volume of decellularization buffers, and an additional 32 h in the SDS solution, compared with the “conventional” method. 112 Both protocols produced similar results, with no significant difference in fibroblast cell viability, endothelialization, burst pressure, or collagen content, although the intensified protocol produced a scaffold with significantly less sulfated glycosaminoglycan (sGAG) content. 112 When compared with native equine carotid arteries, both protocols demonstrated a similar reduction in compliance. 112 To compensate for the reported loss of mechanical properties during decellularization, polymers have been used as coatings. For example, polycaprolactone (PCL) was electrospun on decellularized rat aorta to improve ultimate tensile strength, suture retention strength, and burst pressure. 113 Similarly, the coating of poly(ethylmethacrylate-co-diethylaminoethylacrylate) (also known as 8g7) restored the mechanical properties of decellularized porcine carotid arteries to native values. 114
Comparable to SIS grafts, grafts from decellularized porcine vessels are largely unsuccessful without some type of surface treatment, whether it is pre-implantation EC-seeding or a luminal coating. Ma et al. dynamically seeded decellularized porcine aortas with autologous canine ECs and validated their patency at 1, 3, and 6 months without any signs of thrombosis in vivo. 115 Similarly, the autologous endothelialization of porcine carotid arteries helped to prevent graft failure and encouraged cell recruitment and proliferation of SMCs in pigs over 6 weeks, compared with the unseeded grafts that were characterized by significant clotting, a thick media layer, and an influx of inflammatory cells. 116 Li et al. demonstrated the in vitro efficacy of differentiating hMSC into ECs and SMCs with a contractile phenotype, as a means to overcome insufficient cell recruitment on decellularized porcine carotid artery scaffolds.117,118 Another method to promote endothelialization is the coating of the luminal surface with biopolymers. The 8g7 has been shown to reduce platelet adhesion, while promoting EC attachment and proliferation. 119 The 8g7-coated porcine carotid arteries displayed both a significant increase in the number of attached ECs and a more homogeneous and interconnected endothelial layer. 114 In addition, the fixation of heparin on grafts, largely achieved with the crosslinking agents N-(3-dimethylaminopropyl)-N’-ethyl carbodiimide hydrochloride (EDC) and N-hydroxysuccinimide (NHS), has improved graft success.66,120,121 Specifically, heparin immobilized on the surface of decellularized porcine carotid arteries showed a four-fold extension of the active partial thrombin time, indicative of an enhancement in anti-thrombogenic properties of the treated grafts. 120
Heparin surface treatment is a common approach to help reduce the occurrence of thrombosis in vascular grafts composed from cannular ECM. Decellularized rat aortas covered in electrospun PCL and treated with heparin showed less platelet adhesion and activation than decellularized-only grafts. 113 Similarly, rat aortas submerged in poly(1,8 octanediol citrate) solution and crosslinked before heparin immobilization showed the lowest levels of both platelet adhesion and thrombus formation, while supporting HUVEC adherence and growth in vitro. 122 However, Jiang et al. reported a substantial increase in the elastic modulus of rat aortas when treated with the EDC/NHS method of heparin immobilization. 66 Alternatively, grafts heparinized with the “click” method showed a formed endothelial layer, the lowest amount of intimal hyperplasia, and a reduced inflammatory response without a change in mechanical behavior. 66 Despite the differences in properties that originated from the processing techniques, both types of grafts remained patent for 4 weeks in vivo. 66 In a follow-up study pursuing the “click” method of treatment, all grafts were patent, but exhibited reduced blood flow, calcification, mineralization, and minimal cell infiltration into the walls. 123 Zhou et al. demonstrated that heparin-coated rat aortas, also treated with SDF-1α, reduced platelet adhesion and supported the attachment, activity, and migration of bone marrow stem cells in vitro and of ECs and EPCs in vivo. 124
Other types of surface treatments have been developed that not only suppress platelet adhesion and thrombosis, but also encourage endothelialization. The addition of VEGF 145 and basic fibroblast growth factor in heparinized rabbit aortas led to a substantially higher patency rate of 90% at 18 months, compared with the 10% patency of heparin-only grafts. 121 Decellularized rat aortas coated with a VEGF-conjugated hydrogel (HG-VEGF) also significantly increased the development of a functional endothelium over 8 weeks; however, there was also an increase in the occurrence of intimal hyperplasia. 125 Mahara et al. treated decellularized ostrich carotid arteries with two synthetic integrin α4β1 ligand peptides (REDV): POG7G3REDV and OPG7G3REDV. 126 POG7G3REDV-modified grafts showed significant improvements in HUVEC adherence and EPC recruitment in vitro, whereas five of the six implanted grafts remained patent throughout the 3 week period, with no signs of thrombosis. 126 Kristofik et al. cultured dermal fibroblasts from thrombospondin-2 knockout (TSP2 KO) mice on the lumens of decellularized rat aortas to encourage deposition of their naturally antithrombotic ECM.127,128 In a rat model over 4 weeks, the TSP2 KO ECM-modified grafts showed decreased platelet activation, along with increased cell recruitment and patency. 128
The use of human blood vessels poses significant advantages over other tissue sources, because the structural and biochemical properties of these grafts largely mimic the target arteries. Therefore, these grafts potentially require minimal alterations beyond decellularization, which has led to investigations of their usefulness as small-diameter vascular grafts. Decellularization protocols of human vessels impact the ECM in a variety of ways, including decreasing wall thickness 129 and mechanical strength,130–132 whereas collagen fibers 130 and burst pressure 133 are preserved. Porzionato et al. showed that decellularized arteries and veins from human hands implanted into a rabbit model remained functional, with no signs of thrombosis or inflammatory rejection. 129 The vein grafts showed endothelialization of the luminal surface and sufficient cell recruitment throughout the remaining layers, whereas the arterial grafts had only partial cell infiltration at 2 weeks, likely due to the thicker vessel wall. 129 However, longer in vivo studies paint a different picture. There was positive cell infiltration of ECs and SMCs in decellularized internal mammary arteries implanted into rabbit femoral arteries after 3 years, 134 whereas saphenous veins endothelialized with the autologous ECs showed 80% patency at 6 months and 50% patency from 9 to 32 months in humans. 135
Placental arteries and umbilical cord vessels are unique alternatives to traditional human vessels for small-diameter vascular grafts. However, placental arteries from the chorion are extremely susceptible to damage during the decellularization process, lending to a decrease in GAG content and elastic modulus, in addition to the destruction of the basement membrane.131,132 The exposure of collagen fibers during the decellularization process necessitated the use of heparin surface treatment on placental arteries by Schneider et al. 132 After 4 weeks post-implantation, these grafts were free from occlusions and the mechanical properties were comparable to native tissue due to the influx of recipient cells. 132 The human umbilical vein has demonstrated the deterioration of many components in the ECM, including collagen, elastin, fibronectin, and laminin, as well as a decrease in cell adhesion, as a result of a variety of decellularization techniques. 136 Alternatively, in decellularized and vitrified human umbilical arteries (hUA), collagen and elastin appear to be preserved with comparable sGAGs and hydroxyproline content and without any cytotoxic impact to hMSCs. 137 After 30 days in a porcine model, the ECM structures of hUA grafts mimicked those of native porcine carotids, but they lacked an organized endothelium and were prone to thrombosis. 137 One method to improve the outcome of hUAs is with human leukocyte antigen (HLA)-matching, which has been investigated by Mallis et al. through recellularizing grafts of an HLA genotype with hMSCs of a differing HLA genotype. 138 After 3 weeks, the repopulated grafts adopted the HLA profile of the seeded hMSCs and showed no remnants of the previous HLA genotype. 138 Since the presence of residual antigens, specifically HLA, is linked to an immune response and eventual graft rejection, the ability to match the HLA genotype of the graft to the patient is imperative to the longevity of graft survival.
Impact and clinical outlook
Vascular grafts can be developed with decellularized cannular tissues from an assortment of animal sources without the need for glues or sutures. However, this technology largely focuses on arteries and veins, which provides a more limited range of tissue properties and compositions when compared with the 2D sources described earlier. Many of the decellularization techniques employed, specifically harsher techniques to target the media layer of vessels, impact graft composition and strength. Since there is such an abundance of diverse decellularization methods, it would be beneficial to compare the mechanics of different types of animal ECM for the same protocols. Although tissue remodeling may lead to the recovery of the mechanical properties, cell infiltration occurs at a much slower rate in humans than in animals. Thus, the grafts may remain susceptible to failure until regeneration occurs. Before this technology can move forward clinically, we feel that it is important to investigate the impact of decellularization techniques on human cell infiltration and remodeling, as well as the effect of the resulting ECM composition on endothelialization. In addition, a loss in strength after decellularization for a given tissue typically indicates damage incurred by the ECM. However, in some cases, these changes cause the tissue to behave more similarly to human arteries, which should be considered as well. In addition to the changes in mechanical properties, harsher decellularization methods expose collagen and lead to pro-thrombotic surfaces, which necessitates the use of surface modification. As previously mentioned, surface treatment will require supplemental processing, which can alter the ECM, but they are generally simpler adaptions than the use of cell culture when considering translation to clinical use.
Conclusions
With the incidence of CVD continuing to rise and the high failure rates of autologous grafts, it is imperative to develop an alternative to autologous vessels for small-diameter vascular graft applications. We have investigated and evaluated vascular grafts composed of cell-derived ECM, 2D tissue, and cannular tissue, focusing largely on mechanical properties, infiltration of host cells, and overall patency in vivo, as well as the feasibility of translating each of the three technologies to clinical use. Cell-based approaches require lengthy cell culture periods, but they enhance control over the graft properties when compared with 2D and cannular tissue grafts. Further, autologous endothelialization has been an important tool in preventing thrombosis and, ultimately, preserving patency in many types of grafts. However, due to the large number of grafts needed, it seems improbable that a cell-only approach is the best method forward. Two-dimensional tissues require the use of sutures or glue to form the cylindrical shape, but they provide a wider array of structures and properties than cannular tissues, which are typically arteries or veins. Further, cannular materials require more abrasive decellularization methods than cell-based ECM and 2D tissue, which damage the ECM, impair the mechanical behavior, and expose thrombosis-inducing constituents of the tissues. Both 2D and cannular grafts frequently involve a secondary treatment post-decellularization to improve in vivo success. Grafts composed of 2D or cannular ECM with a surface modification, or less likely, luminal ECs, seem to be the most feasible approaches to translate to patients. However, the effects of decellularization should be further characterized. In addition, to drive this technology toward clinical implementation, critical areas to investigate, independent of graft type, include developing a practical storage process to ensure off-the-shelf availability, examining the effects of storage on the success of the vascular graft, and constructing a human model for more relevant in vitro studies with human cells. Since all three of these technologies rely on patient cells for graft remodeling, it is imperative to explore new methods to improve host cell infiltration, as well as the impact of ECM composition on endothelialization.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the NIBIB/NIH Center for Engineering Complex Tissues (Award No. P41EB023833) and the National Science Foundation CBET (Award No. 5246870).