
Abstract
Heart valve disease carries a substantial risk of morbidity and mortality. Outcomes are significantly improved by valve replacement, but currently available mechanical and biological replacement valves are associated with complications of their own. Mechanical valves have a high rate of thromboembolism and require lifelong anticoagulation. Biological prosthetic valves have a much shorter lifespan, and they are prone to tearing and degradation. Both types of valves lack the capacity for growth, making them particularly problematic in pediatric patients. Tissue engineering has the potential to overcome these challenges by creating a neovalve composed of native tissue that is capable of growth and remodeling. The first tissue-engineered heart valve (TEHV) was created more than 20 years ago in an ovine model, and the technology has been advanced to clinical trials in the intervening decades. Some TEHVs have had clinical success, whereas others have failed, with structural degeneration resulting in patient deaths. The etiologies of these complications are poorly understood because much of the research in this field has been performed in large animals and humans, and, therefore, there are few studies of the mechanisms of neotissue formation. This review examines the need for a TEHV to treat pediatric patients with valve disease, the history of TEHVs, and a future that would benefit from extension of the reverse translational trend in this field to include small animal studies.
Background
V
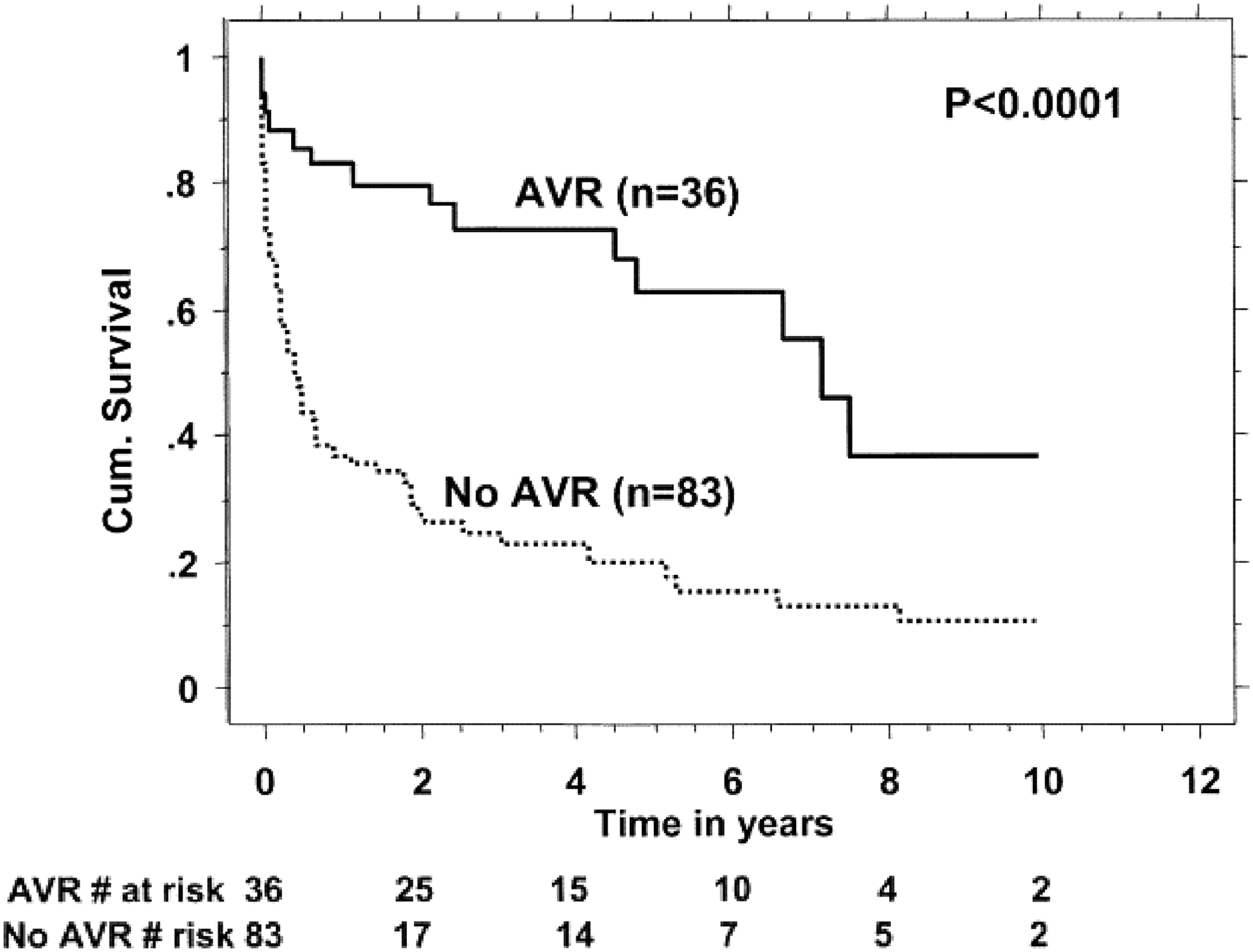
Kaplan–Meier survival curves showing the association of AVR with better survival in patients with severe aortic stenosis associated with severe pulmonary hypertension. Republished with permission from: Pai et al. 3 AVR, aortic valve replacement.
Since the first heart valve replacement was performed in 1952, the field has grown tremendously. 7 Today, ∼280,000 valve replacements are performed worldwide, 90,000 of which occur in the United States. Current replacement options can be grouped into two general categories: mechanical and biological valves. Biological valves may be subdivided into cryopreserved homografts and bioprosthetic valves. Valve replacement is split nearly equally between mechanical and biological valves. 8 The long-term survival of mechanical and biological valves is nearly identical; however, the primary failure modes are drastically different. Mechanical valves are defined by a long product life of more than 15 years, but they are plagued by thrombotic complications, requiring lifetime anticoagulation.9,10 Biological prosthetic valves are less susceptible to thromboembolism, but they are prone to mechanical failure and rupture, with excessive deterioration occurring 10–15 years postimplant.9,10 The difference in deterioration is the most pronounced in pediatric patients, where biological valves show lower long-term efficacy due to the longer required lifespan of the implant.11,12 Even with re-intervention, long-term survival remains low. The 15-year mortality rate after valve replacement is 60–80%, although only 40–60% of these deaths are secondary to valve-related complications. 13
Due to the morbidity associated with traditional mechanical and biological replacement valves, alternative approaches have been investigated. Minimally invasive transcatheter valve replacement is being performed more frequently, but these valves still lack growth capacity and the catheter deployment system has been shown to damage the valve leaflets. The ideal replacement valve would be able to grow and remodel with the patient. The field of tissue engineering, where a biodegradable or decellularized valve scaffold is implanted and replaced with native tissue, offers the potential to achieve this goal. In this review, we discuss the history of valve replacement and the current status of tissue-engineered heart valves (TEHVs).
Heart Valve Biology and Mechanics
Development and basic biology
Heart valves undergo several stages of remodeling throughout their development. Endothelial cells in the developing heart undergo endothelial-to-mesenchymal transition into the cardiac jelly to create the endocardial cushions that develop into the primitive valves. 14 Cytokines that have been implicated in this transition include transforming growth factor (TGF)-β, vascular endothelial growth factor, and bone morphogenetic protein (BMP)-2. 15 The cells that make up the endocardial cushion undergo rapid proliferation initially, but the rate dramatically decreases in the remodeling phase of valve development, and it decreases further in the mature valve in children and adults. 16 The immature valve reorganizes and synthesizes its extracellular matrix in utero and after birth, with the mature architecture not being fully present until postnatal life. 16 Adult heart valves consist of two or three leaflets, with a valve diameter around 25 mm and a leaflet thickness of ∼0.5 mm. 17
Basic histology
The valve leaflets have a detailed multi-scale hierarchical structure made of three layers. 18 The fibrosa, which is the most proximal layer with respect to blood flow, contains primarily circumferentially oriented collagen in thick bundles. 19 It provides the main mechanical strength of the leaflet and makes up the majority of the leaflet thickness.19,20 The spongiosa is the thick middle layer of the valve leaflet, and it is mostly made of randomly oriented proteoglycans and loosely arranged collagen. 21 It acts as a buffer between the top and bottom layers. 22 The glycosaminoglycans and proteoglycans in the spongiosa act to absorb the load in the valve and transfer it to the adjacent wall as well as allow shearing between the fibrosa and ventricularis, limiting the stress on the leaflets. 23 The thinnest and most distal layer with respect to blood flow, the ventricularis, is made mostly of radially oriented elastin, giving the valve its high elasticity. 22
The primary cells present in the valve leaflets are valvular interstitial cells and surface endothelial cells. The interstitial cells express characteristics of smooth muscle cells, cardiac muscle cells, and fibroblasts; however, they are phenotypically closest to smooth muscle cells and myofibroblasts. 24 The interstitial cells are present throughout the valve leaflets and are responsible for the production of glycosaminoglycans.25,26 The endothelial cells coat the surfaces of the valve and are aligned orthogonally to blood flow.27,28 Some nerve cells have also been demonstrated in valve leaflets, and they have been shown to impart some control over the mechanical properties of the valve. 29 Aortic and pulmonary valve leaflets are thin enough to be perfused from the surrounding blood and, as such, contain few blood vessels. Mitral and tricuspid leaflets, on the other hand, contain a few capillaries in their most basal portion. 21 Adult valves have minimal regenerative capacity, and, therefore, valves damaged by pathologic processes must be surgically repaired or replaced.
Biomechanics
The hierarchical organization of the valve leaflets gives them anisotropic mechanical properties. 30 The radial fibers in the leaflets are more crimped than the longitudinal fibers.31,32 Biaxial testing has shown the leaflets to be highly anisotropic, with nearly four times higher elasticity in the radial direction than in the circumferential in porcine aortic valves. 33 The elastic modulus was also shown to be 10 times higher in the circumferential than in the radial direction, with the radial direction having an initial modulus of 2–10 kPa compared with 20–100 kPa in the circumferential direction in porcine pulmonary and aortic valves, with aortic valves having a higher modulus.34,35 The total stress on the valves has been estimated at 50 kPa in diastole and 500 kPa in systole in porcine aortic valves. 36 In human aortic valves, there is a positive correlation between modulus of elasticity and collagen cross-link concentration, but not collagen content, suggesting that collagen cross-links may play a more dominant role in determining biomechanical behavior. 37
Current Heart Valve Replacement Technologies
Mechanical heart valve replacements
Although the initial mechanical heart valve design had only a single tilting valve, innovations since then have seen the use of bileaflet designs. 7 The material properties of mechanical heart valves allow them to have a very long life, typically lasting beyond 15 years postimplantation. 10 However, these properties, along with the flow mechanics of mechanical heart valves, also result in thromboembolic complications and a lack of growth potential. The risk of thromboembolism is much higher in mechanical heart valves than in biological valves, and it is higher for valves implanted in the mitral position than the aortic position and higher on the right side of the heart than the left. 38 To mitigate this risk, patients are placed on lifelong anticoagulation. 39 However, this long-term anticoagulation is not without its own added risk. The incidence of intra- and extra-cranial bleeding events in mechanical heart valve patients on anticoagulation therapy ranges from 1.2% to 2.6% per year.40,41
Mechanical heart valves are also complicated by fibrotic ingrowth and regurgitation. Mechanical valves are not capable of biodegradation and remodeling, and, as such, any fibrotic ingrowth over the life of the valve contributes to compromised valve performance. 42 Although mechanical valves are not prone to deformation and degradation like biological valves, they, in fact, have a greater degree of regurgitation during the immediate postoperative period. This regurgitation is typically not a failure, but instead is a built-in back flow of the valve, with the intent to prevent blood stasis and thrombosis. 8
Biologically derived heart valve replacements
Biological heart valves consist of fixed or decellularized human or animal valves that may be attached to a stent. The main advantage of biological valves over mechanical heart valves is their lower rate of thromboembolism.43,44 Because systemic anticoagulation is unnecessary, the lifetime risk of hemorrhage is greater than three times lower for biological valves compared with mechanical valves. 45 The risk of thrombosis is highest in the first 3 months after surgery, and it is related to the absence or subtherapeutic use of anticoagulants. 42 The risk of thrombosis is increased in stented biological valves compared with nonstented valves. 46
Bioprosthetic valves
Bioprosthetic valves are derived primarily from xenogenic material that has been chemically fixed to reduce immunogenicity and preserve the tissue. 47 They are often made from porcine heart valves or bovine pericardium. 47 These preservation techniques severely decrease the biological activity of the natural matrix. 48 Consequently, although they are made from natural extracellular matrices, biological prosthetic heart valves do not demonstrate growth potential, limiting their use in the pediatric population. 49
The primary mechanism of failure for biological prosthetic valves is degradation-related failure of the valve, which accelerates 10–15 years postimplant (Fig. 2). 13 Most valve failures occur during this time, resulting in the need for re-intervention (Fig. 3). 13 The valve degeneration is seen grossly in the form of cusp calcification, cusp tears, perforation, stretching or shortening, thickening, stiffening, and prolapse. 42 This deformation is believed to be due to chemical interactions between the aldehyde groups of phospholipids and circulating calcium ions, the immune system response to the valve, and dystrophic calcification. 42
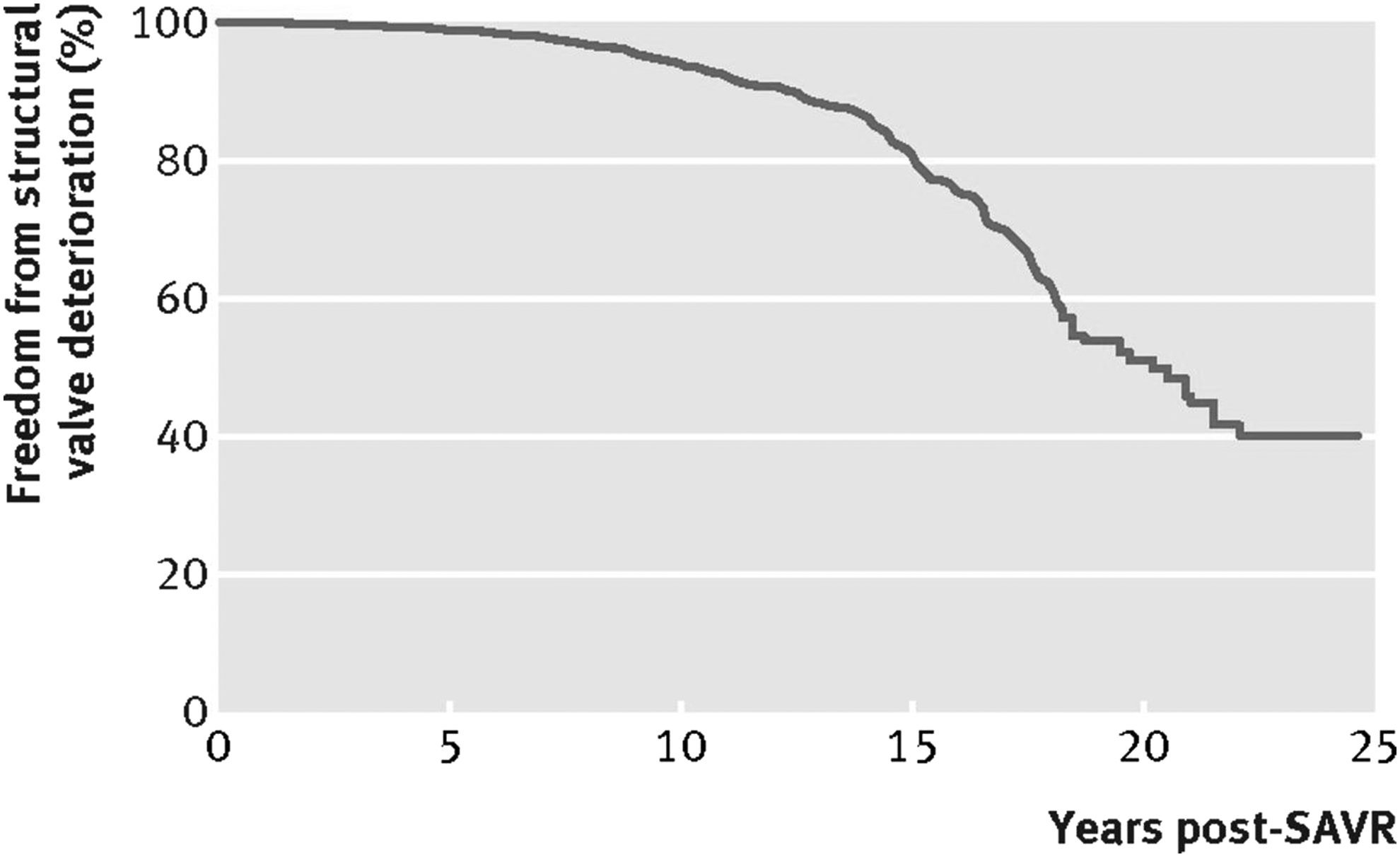
Freedom from valve deterioration after SAVR with a biological valve. The rate of deterioration accelerates 10–15 years after implantation. Republished in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license from: Foroutan et al. 143 SAVR, surgical aortic valve replacement.
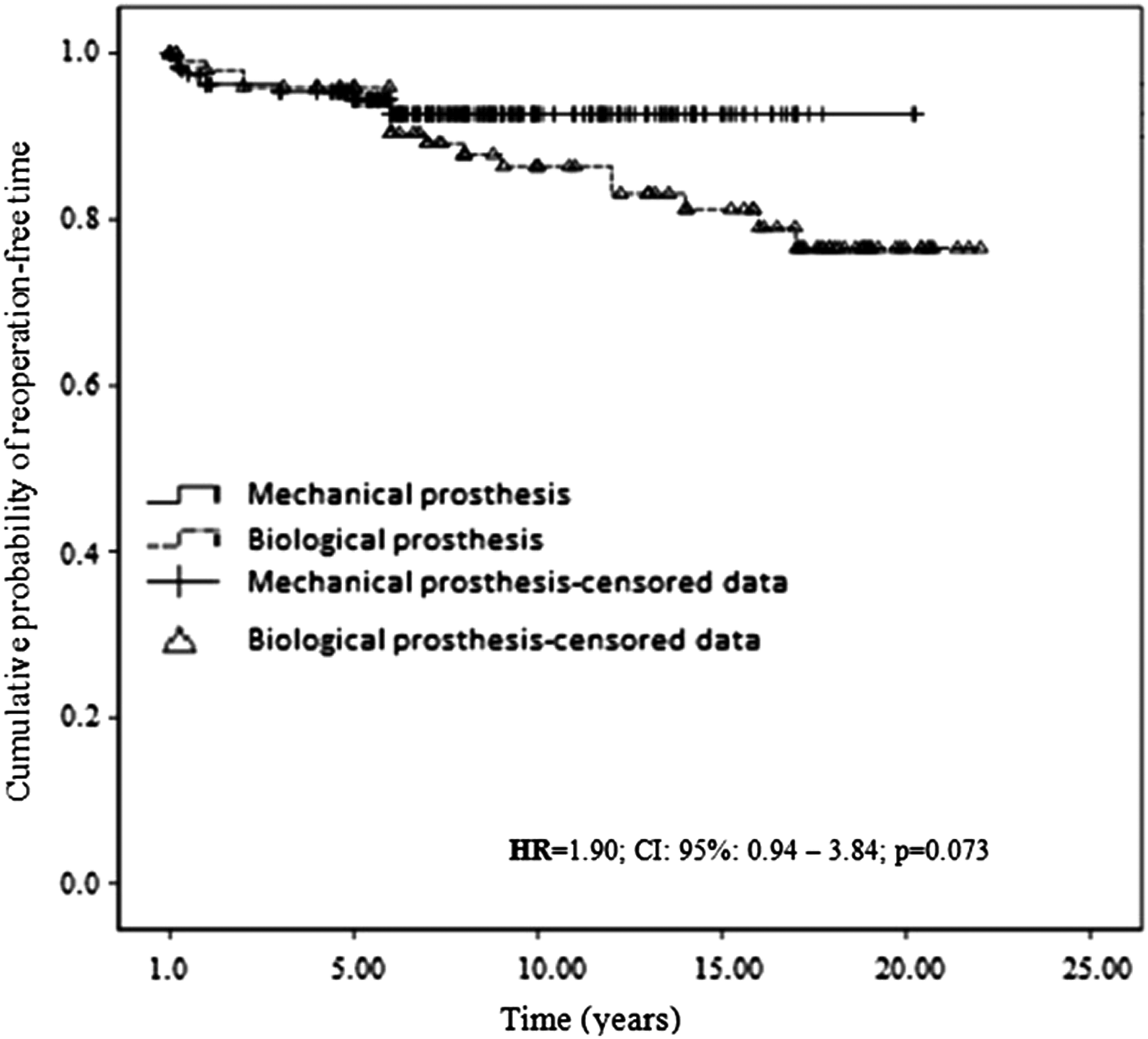
Freedom from reoperation for replacement valves. Because there is a high rate of valve deterioration after 10–15 years, there is a trend toward increased probability of reoperation in biological mitral valve replacements compared with mechanical valves. Republished in accordance with the Creative Commons Attribution License (CC BY 4.0) from: Ribeiro et al. 144
Cryopreserved homografts
Homografts are derived from human valves and cryopreserved to increase their shelf life. They have been used in congenital cardiac surgery since the 1960s, when Ross and Somerville reported the first use in a patient with tetralogy of Fallot and pulmonary atresia. 50 They have been used in many congenital cardiac lesions since then, and they are favored because of their low thrombogenicity. Cryopreserved homografts are satisfactory replacements in many cases, but they are imperfect. 51 They are prone to early calcification, and in contrast to bioprosthetic valves, they have limited availability. 52 Similar to bioprosthetic valves, they are prone to structural degeneration and the need for replacement, as long-term function of both bioprosthetic valves and homografts is poorer than for mechanical valves and autografts.52,53 Reported 5-year survivals for cryopreserved homografts range from 55% to 94%. 54 Durability is poorest in patients <2 years old.54,55
Transcatheter deployment versus open valve replacement
A recent advancement in the past 10–15 years is the development of transcatheter deployment systems for artificial valves. In this way, a replacement valve may be implanted via an endovascular approach without the need for an open surgery. This technique has shown promise in reducing the surgical risks associated with traditional replacement via sternotomy, particularly in high-risk patients with comorbidities who may not be surgical candidates. 56 The clinically available transcatheter heart valves consist of stainless steel stents with equine or bovine valves wrapped around a valvuloplasty balloon.57,58 The long-term survival is equivalent to that of surgical replacement, but transcatheter valve replacement is associated with a lower risk of stroke, acute kidney injury, and major bleeding. 59 However, it should be noted that there are still advancements to be made in this area. Transcatheter valve replacement has a higher risk of conduction abnormalities. 60 After transcatheter aortic valve replacement, mild-to-moderate perivalvular leak is seen in 47% of patients. 61 The crimping of the valve to fit it into the catheter for deployment has been associated with leaflet structural damage and calcification. 62 In addition, the use of the catheter deployment system can block the coronary ostium with the artificial valve or the native valve leaflets. 60 Transcatheter heart valve replacement techniques also enable the valves to be “upsized,” thereby enabling some accommodation for growth, although with the risk of additional endovascular procedures and complications. As the stents currently used in the delivery of transcatheter heart valves lack growth potential, the adoption of bioresorbable stents will be a necessary step in bringing this technology to pediatric patients. 63 As technology and techniques in this area continue to improve, transcatheter placement will become increasingly more relevant for pediatric patients with heart valve disease.
Tissue-Engineered Heart Valves
Tissue engineering
The ideal solution for a long-term heart valve replacement would be biodegradable, nonimmunogenic, and capable of withstanding constant shear stress. It would also mimic the tri-laminar architecture of the native valve leaflet, demonstrate growth and repair capabilities, and be fully functional at the time of implant. 10 A TEHV has the potential to meet all these criteria by forming a neovalve composed entirely of native tissue.
Tissue engineering rests on three essential pillars: (1) the scaffold, which ultimately degrades and is replaced by extracellular matrix, (2) cells (either seeded in vitro or mobilized in vivo), and (3) signals (humoral and mechanical). The three factors are interdependent and are all required for the formation of organized neotissue. Various combinations of the components have been intermixed in an attempt to create an optimal neovalve. 64
The scaffold provides a three-dimensional structure onto which neotissue can grow. Cells may also be capable of modeling the scaffold depending on the material and processing techniques used. Two types of scaffold may be used: (1) decellularized extracellular matrix or (2) biodegradable synthetic materials. Decellularized tissue sources include allogeneic, xenogenic, or in vitro engineered tissues that contain an intact extracellular matrix. 65 Decellularization can be achieved by a combination of physical agitation, chemical surfactant removal, and enzymatic digestion, which disrupt cells and remove most of the cellular antigenic components. However, the decellularization process can also degrade matrix components, which results in a loss of extracellular matrix integrity. 66 The resultant tissue deterioration can lead to degenerative structural graft failure. 66 A main concern for porcine-derived materials is the presence of residual cells, DNA, and alpha-Gal epitope after the decellularization process. 67 In a study comparing decellularized with traditional allografts, no functional or pathological differences were observed, but in this study the decellularized allografts were analyzed at a much shorter follow-up time than the traditional allografts. 68 Additional drawbacks of decellularized scaffolds include an inability to modify the matrix content and architecture and rapid degradation on implantation relative to mechanical valves.
Alternatively, naturally occurring or synthetic polymers can be used to form scaffolds. The ideal scaffold allows for a microenvironment that promotes cell adhesion and differentiation and permits deposition of extracellular matrix. Natural materials include collagen, gelatin, hyaluronate, glycosaminoglycan, chitosan, alginate, silk, fibrin, dextran, and Matrigel.
69
Synthetic polymers include polyglycolic acid (PGA), polylactic acid, polylactic-co-glycolic acid, poly-
Scaffolds may be seeded with stem cells such as bone marrow-derived mononuclear cells. These cells have seen a shift in understanding in recent years. The original hypothesis was that they differentiated into the neotissue, but more recent work has shown that seeded cells disappear within the first week of implantation. Nevertheless, their presence makes a drastic difference in the inflammatory response to the implantation, as well as in the neotissue and clinical outcomes. 70 SCID/Beige mice were used to evaluate the effect of each portion of the immune system on graft remodeling, and they demonstrated the critical role of the innate immune system and macrophages in neotissue development. 71
Regardless of the type of scaffold or presence of seeded cells, the goal remains the same: to permit cellular deposition and then degrade, thereafter providing an autologous structure for ongoing TEHV growth. The ideal TEHV would approximate the composition of a native valve, with a luminal endothelial cell layer and centrally located interstitial cells. Although the search for the ideal TEHV has resulted in a vast array of material and cell combinations in vitro, an exhaustive list of these combinations is beyond the scope of this review, and we will focus primarily on those studies that have progressed to animal and human studies.
Previous Studies of TEHVs
Overall, studies of TEHVs have focused on large animals and humans (Table 1). The earliest studies of TEHVs were performed in large animals. The first TEHV was in the form of individual leaflets made of a PGA fiber matrix seeded with autologous endothelial cells and fibroblasts, and it was implanted as a pulmonary valve replacement in an ovine model. 72 These single leaflets showed remodeling within 7 days, with no regurgitation or stenosis present at 2 months. 73 After this work, whole heart valves were created with the more pliable elastomer polyhydroxyalkanoate. 74 Early work used stiff materials for their durability, but they were complicated by stenosis. 75 Later designs opted for more pliable materials, which were shown to last 17 weeks in vivo with ingrowth and remodeling, but only when seeded with cells; valves without seeded cells did not exhibit full ingrowth of cells or as much remodeling. 75
Native pulmonary valve was not replaced.
RVOT, right ventricular outflow tract; PVR, pulmonary valve replacement; PGA, polyglycolic acid; PGLA, poly (glycolic acid/lactic acid); PLA, polylactic acid; PHO, polyhydroxyl butyrate; P4HB, poly-4-hydroxybutyric acid; AVR, aortic valve replacement; PC-BU, bis-urea-modified polycarbonate; PV, pulmonary valve; PA, pulmonary artery; SMC, smooth muscle cell.
Dohmen et al. 76 utilized endothelial cell seeding on decellularized porcine valves in sheep. After demonstrating that at 3 months the valve leaflets were not calcified, showed no fibrous tissue overgrowth, and were endothelialized, a small clinical study with six patients using a similar decellularization and seeding technique with pulmonary valve allografts was performed. These valves showed similar positive results at 3 months. 76
A myriad of material and cell source combinations have been used in ovine models with varying success. PGA and PLGA seeded with myofibroblasts demonstrated rapid remodeling over 2 weeks, with limited stenosis or regurgitation. 73 Polyhydroxyl butyrate (PHO) seeded with vascular endothelial cells showed rapid deposition of collagen to levels higher than the native tissue over 17 weeks. 75 The rapid deposition of collagen in these grafts points to the activation and early infiltration of native cells, as endothelial cells are not strong producers of collagen. PGA/poly-4-hydroxybutyric acid (P4HB) seeded with myofibroblasts demonstrated complete degradation of polymer within 8 weeks, and mechanical properties similar to native valves by 20 weeks. 77 PHO seeded with endothelial cells had no postoperative thrombosis, compared with a high incidence of thrombosis in unseeded valves. In addition, they demonstrated progressive remodeling over at least 6 months, with mild but nonprogressive valvular regurgitation. 78 An electrospun polycarbonate bis-urea on a polyether ether ketone ring seeded with a fibrin gel in a sheep pulmonary valve study was functional at 12 months, with layered collagen deposition and polymer degradation. 79 Additional materials that have been attempted include porcine small intestinal submucosa, fibrinogen, and decellularized pulmonary and aortic valves.80–82
Fresh decellularized allografts have shown clinical improvement over their crosslinked and cryopreserved counterparts. 83 The primary decellularized heart valve on the market for clinical use is the CryoValve SynerGraft, a decellularized cryopreserved heart valve available from pig and human sources.84,85 In an early case series of porcine-derived grafts, three of four children died, one due to valve rupture on postoperative day 7 and the others with severely degenerated valves 6 weeks and 1 year after implantation. 85 The valves elicited a strong inflammatory response that led to structural failure. In human-derived grafts, elevated valve gradients are common and unpredictable. 84 In a 2005 study, SynerGraft decellularized allografts (“CryoValves”) were shown to have equal survival and freedom from reintervention to standard cryopreserved allografts, with an added benefit of having a lower degree of regurgitation and lower gradients. 86 In a multicenter retrospective review including 163 patients status post SynerGraft implantation, there was no difference in 5- and 10-year survival among patients who received a SynerGraft valve or a standard cryopreserved valve. Freedom from conduit dysfunction at 10 years was significantly better in the SynerGraft group (83% vs. 58%, p < 0.001), and freedom from conduit reintervention was significantly higher in the SynerGraft group. 87 Freedom from moderate-to-severe insufficiency was significantly improved in SynerGraft valves, and there was no difference in stenosis between SynerGraft and standard cryopreserved valves. 88 A comparison of decellularized cryopreserved allografts to traditional cryopreserved allografts by Burch et al. showed that although there were no differences in the degree of insufficiency, the decellularized allografts had a minor improvement in gradient over their traditional counterpart. 89 However, Burch et al. also noted that the decellularized allografts had one-tenth of the shelf life and cost substantially more than traditional cryopreserved allografts. 89
TEHVs have been used clinically as pulmonary valve replacements alone or as part of the Ross procedure, in which a patient's pulmonary valve is used to replace the aortic valve. 90 Two pediatric patients implanted with fresh decellularized cadaveric pulmonary valves showed no adverse events at 3.5 years, and the valve leaflets demonstrated growth and remodeling.81,83 In a Ross procedure study of 45 patients using pericardial heart valves in polytetraflouroethylene (PTFE) conduits, no patients required valve replacement at 15–86 months follow-up, and no significant stenosis or regurgitation occurred. 91 Ozaki et al. utilized autologous pericardium as a material for aortic valve reconstruction in adult patients. One of 108 patients required a reoperation for endocarditis. There were no complications among the other 107 patients at a mean follow-up of 34.2 months. 92
Brown et al. 93 performed a study of 117 non-Ross patients who received an allograft right ventricular outflow tract conduit. The freedom from failure was 60% at 5 years and 43% at 15 years, with freedom from dysfunction at 40% and 23% at 5 and 15 years, respectively. The performance of the allografts was markedly worse in infants, and younger age, smaller allograft size, and presence of truncus arteriosus were identified as risk factors for graft dysfunction and failure. 93
In a clinical trial conducted by Dohmen et al., 94 23 patients underwent Ross procedures with TEHVs (Fig. 4). The valves used in this study were cryopreserved pulmonary valve allografts that were decellularized and seeded with autologous vascular endothelial cells. One patient died 3 months postoperatively secondary to an arrhythmia, and one patient underwent valve replacement for an increased maximum flow velocity and narrowing at the distal anastomosis. One patient had postoperative atrioventricular block grade III. Otherwise, there were no complications at a mean follow-up of 46 months. 94 At a 10-year follow-up of a subset of 11 patients, no patients had developed thromboembolic complications or endocarditis, and no mortalities occurred. The patient with atrioventricular block required a pacemaker implantation. No calcification was seen for a maximum of 10 years postimplant. 95
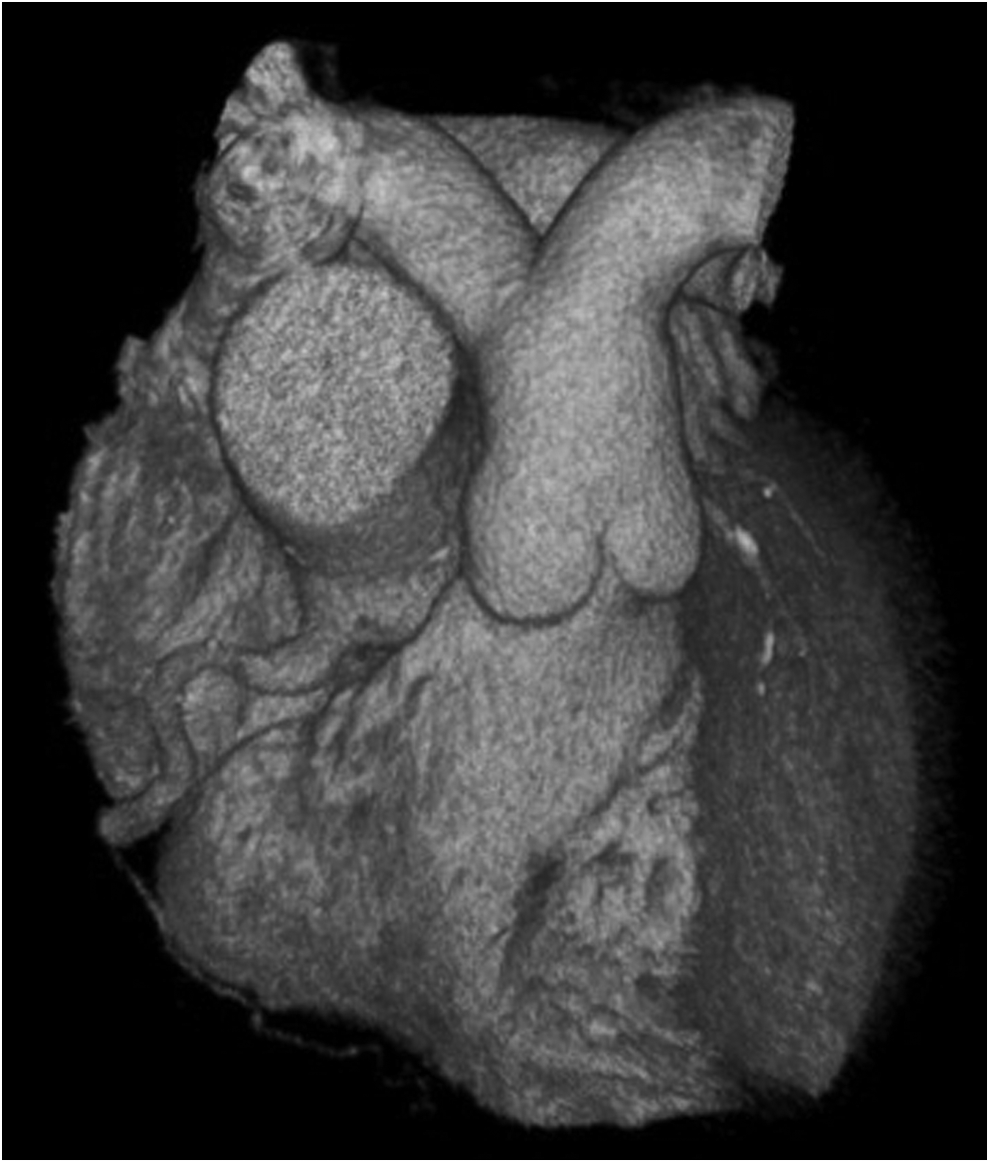
Three-dimensional computed tomography reconstruction of a tissue-engineered pulmonary valve 10 years after implantation. There is no evidence of calcification or valve degeneration. Republished with permission from: Dohmen et al. 95
In a study by da Costa et al., 96 41 patients received decellularized aortic roots as aortic valve replacements. The mean postoperative gradient was 7 mmHg, and regurgitation was rated as none or trivial in all but one patient. Only mild calcifications were observed by computed tomography over 4 years. In the one patient who was explanted at 18 months, mild intimal hyperplasia was noted, with very little repopulation of the graft material. 96
Ruzmetov et al. demonstrated that in children and adults younger than 40 years of age receiving aortic root replacements, autografts and cryopreserved allografts had similar 5- and 15-year survival and freedom from overall reintervention, but autograft patients had significantly greater freedom from explantation. 97
Early studies with Matrix P and Matrix P Plus in right ventricular outflow tract reconstruction, using TEHVs made from decellularized porcine pulmonary valves, demonstrated 87% freedom from intervention at 1 and 3 years postoperatively. 98 However, further studies showed a freedom from failure and dysfunction rates of 60% and 77% at 2 years and <20% freedom from failure at 3 years, with the most common cause for failure being conduit stenosis. Histological samples of explanted valves revealed poor cell growth into the scaffold and an abundance of inflammatory giant cells. Age <1 year at implant was associated with poorer outcome. 99 Further studies showed that the grafts elicited a strong foreign body reaction of innate and adaptive immune cells, as well as a low neovascularization and high fibrotic deposition. These studies also showed that the grafts may have been incompletely decellularized, increasing their immunogenicity. 100
In a nonhuman primate model, PGA mesh was integrated on a nitinol frame, seeded with fibroblasts to create a matrix, and finally decellularized. The neovalves demonstrated mild-to-moderate regurgitation at 8 weeks, and faster recellularization than currently available decellularized TEHVs. 101 In a growing ovine pulmonary valve model, a TEHV was made by seeding dermal fibroblasts in a fibrin gel to allow for matrix deposition, followed by decellularization. 102 The valves demonstrated growth and remodeling, but all sheep developed increasing valvular insufficiency as the valve diameter increased during growth and the leaflet lengths decreased during remodeling. 102 Although many polymer-based strategies have shown efficacy in large animal models, to date no polymer-based TEVG systems have advanced to clinical trials.
A transcatheter approach has been used in a fetal ovine model as a pulmonary valve replacement with a PGA nonwoven mat coated with P4HB on a nitinol stent and coated with amniotic fluid cells. 103 Although the valves were successfully implanted in four sheep, and showed evidence of rapid remodeling, three of the four fetuses died within 5 days, and the valve leaflets showed severe radial shrinkage. 103
The bench-to-bedside-to-bench pattern in TEHVs shows the initial success and excitement associated with early results, followed by the need to return to the laboratory to make improvements in the process. This trend differs from many other medical fields in that it does not include the small animal studies typically performed before large animal and human research. In addition, the studies that have been conducted focus extensively on outcomes, with little information known or researched about the mechanisms of tissue remodeling and the immune response to the implant. Although the findings of animal research do not always translate directly to human subjects, the information gained through animals is invaluable in gaining insights into the mechanisms of biology, preventing human patients from being subjected to untested research, and leading to appropriate research questions for human studies.
Regeneration and Repair Mechanisms of TEHV Replacements
For an implanted heart valve to remain functional throughout a patient's life, particularly during the rapid growth that defines childhood and adolescence, the valve must be able to grow and remodel similarly to host tissue. Although TEHVs have shown varying success in this capacity, the mechanisms by which neotissue forms require further study. Much of the work in mechanisms of cardiovascular tissue engineering has been done by using murine models of tissue-engineered vascular grafts. The lack of molecular and cellular mechanistic in vivo studies in TEHVs stems at least partially from the lack of effective small animal models, which permit a degree of experimental control that is not possible in large animals.
In four juvenile sheep implanted with decellularized porcine valves as pulmonary valve replacements, the valve diameter increased from 17 to 27 mm in concert with a doubling of weight by 9 months postimplantation. The valves demonstrated a monolayer of endothelial cells, fibroblast ingrowth, and collagen production. 104
Many polymers have been evaluated in the laboratory for their use as tissue engineering substrates, and the microscale properties of the graft have been evaluated for their effect on neotissue formation. 30 Of particular note are recent findings that microstructure morphology differences have a stronger effect on the in vivo and in vitro response than the specific polymer type used. 105 Particularly, reducing fiber size was shown to reduce activation of contacting blood products. 105 Aligned electrospun fibers increase the migration speed of breast cancer cells in vivo and influence the orientation of newly deposited collagen.106,107 In a rat aortic graft model, aligned fibers showed significantly higher patency and less thrombus formation than a graft with a smooth topography, despite similar cellular adhesion rates to both graft types. 108 Electrospun and expanded PTFE was shown to promote more smooth muscle cell growth than a flat PTFE surface, and the electrospun PTFE showed a significantly lower number of adhered platelets. 109 Pore size has been shown to affect cell migration, with pore sizes larger than the cells increasing migration, and pore sizes significantly smaller than the cells instead promoting cells to stay and deposit matrix over the surface pores of the graft. 107 Studies evaluating the effect of surface topography on platelet activation have found that smooth surfaces activate far more platelets than micropatterned rough surfaces, with a probable mechanism being that smooth surfaces lead to a slower boundary layer velocity, increasing platelet-wall collisions. 110 Degradation rate must be finely tuned to the rate of neotissue deposition; a scaffold that degrades too quickly will lead to early mechanical failure, whereas a scaffold that degrades too slowly may lead to stiffening and inadequate neotissue formation. 30 The mismatch of the mechanical properties, particularly compliance, has been implicated in a number of studies as a risk factor for poor outcomes. 111 Interestingly, the adjacent vasculature has also been shown to undergo significant remodeling, becoming stiffer and less compliant to more closely match the properties of the graft.112,113
Sheep aortic roots and decellularized pig aortic roots were used as right ventricular outflow tract replacements in a sheep model. The allograft sheep implants demonstrated significant calcification over 6 weeks, whereas the decellularized xenograft showed minimal to no calcification. The decellularized roots demonstrated a central acellular area surrounded by α-smooth muscle actin-positive smooth muscle cells, with a layer of von Willebrand factor-positive cells on the luminal surface. The decellularized xenografts also demonstrated blood vessels within the adventitia of the aortic root. A sharp demarcation line between the acellular and recellularized portions of the xenografts was made up of macrophages. The cellularized allografts were also infiltrated with T cells. 114
Sheep and pig pulmonary valves were decellularized and implanted as pulmonary valve replacements in sheep. At 4 weeks, the arterial side of the grafts was shown to be severely inflamed, with additional vegetations on the ventricularis present at 12 weeks. Decellularized xenograft valves were severely calcified throughout the conduit, whereas decellularized allograft valves showed calcification only near the hinge regions of the valves and suture lines. Allogenic valves were acellular throughout the 12-week study, whereas xenograft valves were infiltrated with T cells, leading to proteoglycan deposition, collagen degradation, and leaflet thickening. These changes were not associated with a rise in TGF-β. 115
Dohmen et al. 116 implanted endothelial cell seeded and unseeded decellularized valves in the right ventricular outflow tract of juvenile sheep. There was no regurgitation or calcification in either group. Fibroblasts were seen to infiltrate both valve groups, and the unseeded grafts obtained a monolayer of endothelial cells by 6 months. These results suggest that seeding of endothelial cells may not be necessary for decellularized allograft scaffolds. 116
In a study of children receiving CryoLife's decellularized SynerGraft or CryoLife's traditional cryopreserved allograft, the cellularized allograft resulted in increased major histocompatibility complex class 1 and class 2 alloantibody titers at 1, 3, and 12 months postimplantation; however, this was not associated with any valve functional defects or clinical outcomes. 117 A similar clinical study using the AutoTissue Ltd decellularization process showed similar findings, with most patients receiving decellularized allografts remaining seronegative for the alloantibodies. 118
Macrophages, in particular, have been shown to play a key role in the remodeling process and neotissue formation, with M1 macrophages correlating with the degree of stenosis and M2 macrophages promoting a more favorable response. 119 Similar results have been shown in other organ systems as well. In a spinal cord injury model, injections of mesenchymal stem cells were shown to upregulate M2 and downregulate M1 levels, which supported remodeling over scar formation. 120 It is worth noting that the traditional paradigm of M1 proinflammatory macrophages and M2 anti-inflammatory macrophages has become contentious in recent years, with a more fluid continuum of activation between the two states becoming more widely accepted.121–123 In a study comparing decellularized aortic roots with autograft implants in the right ventricular outflow tract in sheep, the decellularized autografts were found to have a higher proportion of M2 macrophages that were CD68-, OPN-, and IL-10-positive. The two groups showed similar low levels of inflammatory infiltration. 124
Endothelialization of valve grafts has also been shown to be critical. Early in vivo experiments showed that, although grafts could be endothelialized in vitro, they may not be capable of being endothelialized in vivo.85,125 In a clinical study of expanded PTFE femoral-popliteal bypass grafts, grafts that were endothelialized showed a significantly higher 9-year patency rate compared with unseeded grafts (65% vs. 16%). 126
Fibroblasts are also important cells in the remodeling of valve grafts because of their ability to secrete extracellular matrix. In vivo experiments of P4HB valves seeded with endothelial cells in a lamb model showed the presence of fibroblast-like cells and subsequent collagen deposition within 2 weeks of implantation, with a changing phenotype and levels of matrix proteins over subsequent weeks. 127 Early clinical experience with SynerGraft decellularized porcine grafts showed that they did not experience ingrowth of any endothelial or fibroblast cells even at 1-year postimplant, and these grafts experienced fibrous hyperplasia, calcification, and rapid failure. 85
Overall, control of the foreign body response to the graft has shown to be quite influential in neotissue development, and it is likely crucial in the advancement of tissue engineering technologies. 128 Although the work done in tissue-engineered vessel grafts is exciting, it is unknown to what extent the results are applicable to TEHVs. A functional small animal model will be critical to evaluate the true mechanisms and time course for valve remodeling in vivo.
Conclusions and Future Directions
Current heart valve replacements are becoming less invasive to implant, but they still lack the capacity for growth and require long-term anticoagulation. TEHVs have the potential to overcome these challenges, but they currently have their own complications. A lack of understanding of the mechanisms driving neotissue formation in TEHVs remains a barrier to optimal TEHV design and clinical utilization. Recently developed murine models may meet this need, paving the way for a deeper understanding of TEHV technology.
Recently, a murine model for pulmonary valve transplantation has been developed to better study the mechanisms of tissue development and host responses to TEHV implantation.129,130 In this method, a pulmonary valve replacement is anastomosed to the right ventricular outflow tract of a donor heart, which is then implanted heterotopically with anastomoses to the abdominal aorta and inferior vena cava of a recipient mouse. 129 With minor variations in implantation technique, the model can be used in either low- or high-pressure configurations to further analyze the replacement valves. 131 The largest benefit of this technique is that it can be combined with the myriad of genetic modifications that exist for mice, including Cre-Lox and CRISPR technologies.132,133 These systems may allow for a detailed mechanistic evaluation of the role of specific cell types and signaling cascades that lead to the remodeling of TEHVs for both positive and negative outcomes. Of additional benefit is the fact that mice are much cheaper to purchase and care for, and they also have quick breeding times and growth rates. This allows for a much higher throughput system for the evaluation of hypotheses related to TEHV designs. Some may consider mice to be a step backward from large animals, but in the case of TEHVs, we believe that they represent an avenue to advance the field forward and move this promising technology closer to clinical utilization.
Footnotes
Acknowledgments
The project described was supported by NIH HL128847, NIH HL128602, NIH HL098228, NIH T32GM075787 (K.M.B.), and Award Number Grant TL1TR001069 (J.D.D.) from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health.
Disclosure Statement
C.K.B. receives grant support from Gunze Limited. For all other authors, no competing financial interests exist.