
Abstract
Spinal cord injury (SCI) is a serious problem that primarily affects younger and middle-aged adults at its onset. To date, no effective regenerative treatment has been developed. Over the last decade, researchers have made significant advances in stem cell technology, biomaterials, nanotechnology, and immune engineering, which may be applied as regenerative therapies for the spinal cord. Although the results of clinical trials using specific cell-based therapies have proven safe, their efficacy has not yet been demonstrated. The pathophysiology of SCI is multifaceted, complex and yet to be fully understood. Thus, combinatorial therapies that simultaneously leverage multiple approaches will likely be required to achieve satisfactory outcomes. Although combinations of biomaterials with pharmacologic agents or cells have been explored, few studies have combined these modalities in a systematic way. For most strategies, clinical translation will be facilitated by the use of minimally invasive therapies, which are the focus of this review. In addition, this review discusses previously explored therapies designed to promote neuroregeneration and neuroprotection after SCI, while highlighting present challenges and future directions.
Impact Statement
To date there are no effective treatments that can regenerate the spinal cord after injury. Although there have been significant preclinical advances in bioengineering and regenerative medicine over the last decade, these have not translated into effective clinical therapies for spinal cord injury. This review focuses on minimally invasive therapies, providing extensive background as well as updates on recent technological developments and current clinical trials. This review is a comprehensive resource for researchers working towards regenerative therapies for spinal cord injury that will help guide future innovation.
Introduction
Spinal cord injury (SCI) results from direct trauma to the tissue and is associated with loss of motor, sensory, and autonomic functions caudal to the site of injury. 1 According to the World Health Organization (WHO), 2 between 250,000 and 500,000 people around the world sustain an SCI each year. In the United States alone, there are around 11,000–20,000 new cases each year. 3 However, the annual incidence of SCI varies in different countries; for example, it is 9.2 patients per million in Denmark and 40.1 per million in the United States. 4 Around the world, the incidence ranges from 3.6 to 195.4 patients per million. 5
In the United States, there are around 250,000 patients who are at present living with SCI. 3 Over a lifetime, direct costs of SCI can reach 1.1–4.6 million USD per patient. 6 Most often SCI occurs in young and middle-aged adults 7 and those with SCI are two to five times more likely to die prematurely. 2 SCI affects not only a patient's physical and psychological health but also one's family and the broader community and economy.
Due to the lack of plasticity and limited regenerative capacity of the central nervous system (CNS), recovery of neural function after SCI is rare. After injury, the spinal cord undergoes several changes on the cellular and molecular level that interfere with axonal regeneration. These complex events are poorly understood, hindering the development of treatments that can lead to complete recovery. 8 Present SCI treatment is mostly conservative relying on stabilization of the patient, prevention of complications, and physical rehabilitation.
Extensive research into regenerative strategies for SCI has been performed over the last couple of decades. Improvements in our understanding of the pathophysiology of SCI coupled with advances in cell-based therapies, biomaterials, and biomolecules have enabled us to develop new therapeutic approaches for neuroregeneration. Promising results from in vivo experiments evaluating therapies based on biomaterials, cells, or biomolecules are being continuously reported.9–13 Because of the complexity of SCI pathophysiology, the use of combinatorial therapies may be more effective and lead to better regeneration.14,15 Although various procedures can be used to administer therapy after SCI (Fig. 1), the use of minimally invasive strategies, such as injection, is needed to reduce risk of complications, including introducing additional injury, and thus spare neuronal circuitry. 16
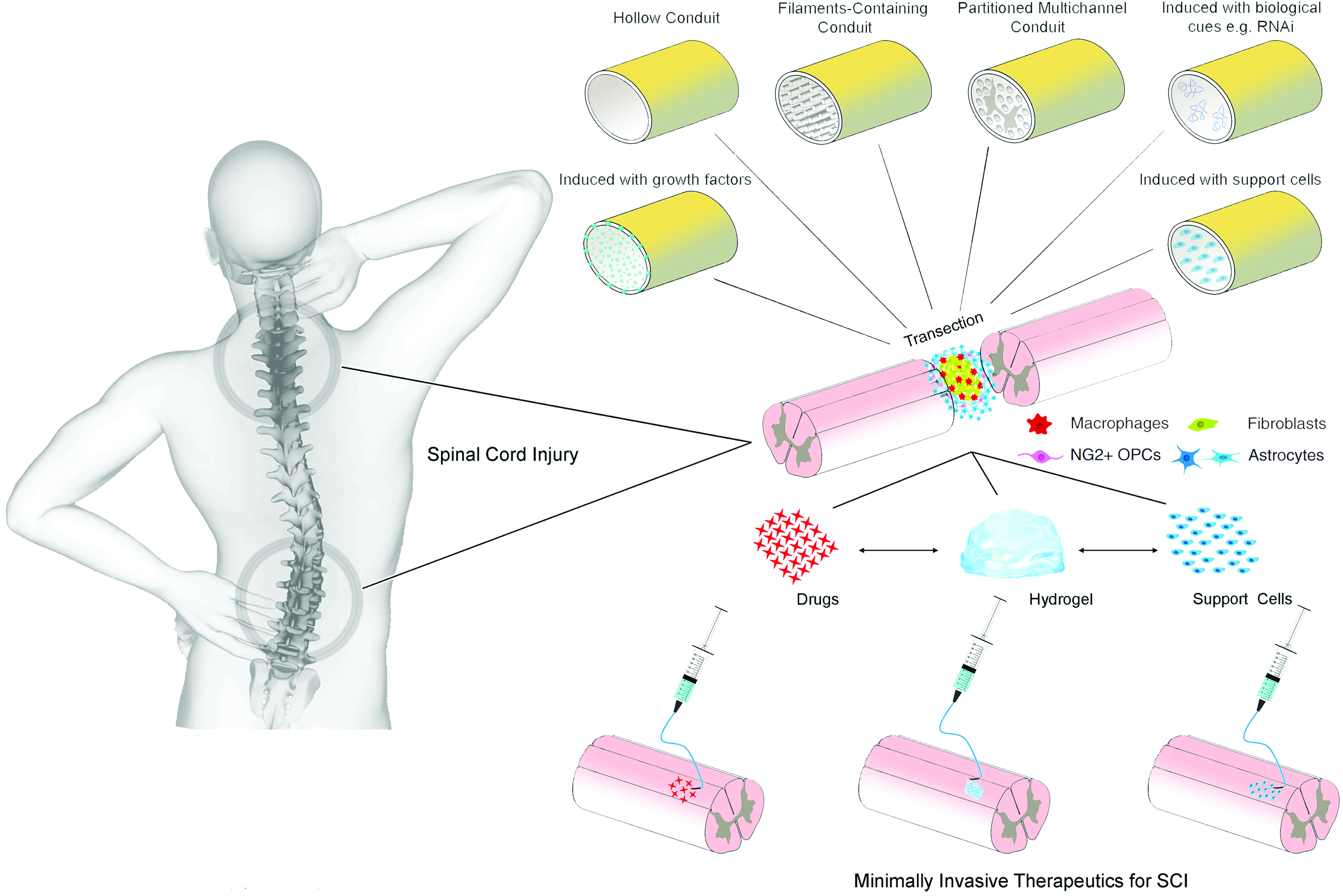
A schematic illustration showing different methods that can be used for the treatment of SCI. SCI, spinal cord injury. Adapted from Führmann et al. 182 Color images are available online.
This review focuses on minimally invasive SCI therapeutics in clinical trials,1,3,6,17 as well as those in preclinical9–13 and in vitro phases of development.18–21 In addition, major challenges are highlighted. Future successful approaches for the treatment of SCI will likely include the integration of several recent advances in various fields as combinatorial therapies in minimally invasive formats. This review summarizes accumulating knowledge, examines evidence and development, and highlights potential paths forward.
Pathophysiology
SCI is characterized by sequential primary, secondary, and chronic phases. The primary injury to the spinal cord is the result of initial trauma. The primary mechanical insult may occur from compression, shearing, laceration, stretch, distraction, hemorrhage, or vasospasm. Bone or tissue fragments from the primary injury can exacerbate swelling of the spinal cord and add to tissue damage.
Secondary injury follows in a progressive way, as a result of ischemia, inflammation, and development of a cytotoxic microenvironment, leading to death of functional cells and damage to the tissue microenvironment. The chronic stage of SCI is characterized by formation of astroglial and fibrous scar tissue around cystic cavitations. As a result, regeneration is thought to be inhibited, at least partially, by the extracellular matrix (ECM) and soluble factors secreted by inflammatory cells within the scar tissues (Fig. 2). 6
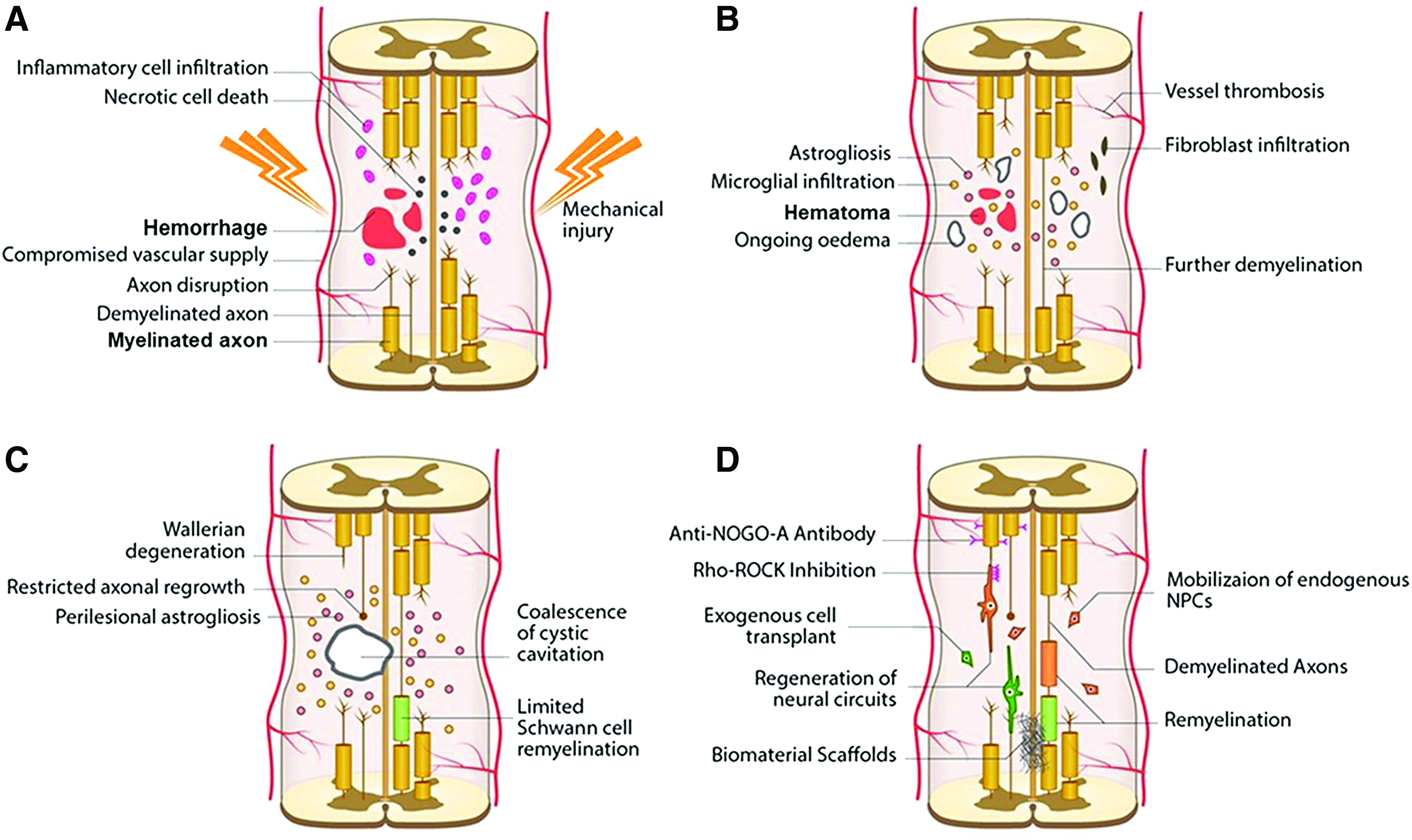
An illustration showing the development of pathophysiological changes following SCI. The acute phase takes 0–48 h and it involves hemorrhage, edema, and proapoptotic factors
Any therapeutic intervention should consider and address the dynamic pathophysiological events occurring in SCI. For example, combating measures against increased extracellular amino acids should be applied early on, in minutes, while measures against inflammatory mediators in hours and measures against myelin-associated inhibitors within weeks after injury. 22 Because inflammation continues and may persist for years, the administration of therapeutic measures should be considered to continue accordingly. 22
Given practical limitations of treating acute SCI in a clinical setting, many therapeutic interventions in development aim to target either the secondary or chronic stages of injury. For example, accumulation of myelin debris during secondary injury is associated with inhibition of regeneration. Myelin-associated proteins lead to inhibition of neurite outgrowth, thus named NOGO inhibitors, which act through NOGO receptors leading to activation of GTPase Rho A. Its effector, Rho-associated protein kinase (ROCK), leads ultimately to apoptosis, axonal collapse, and neurite retraction. 6 While a detailed discussion of the mechanisms of myelin-associated inhibition of axonal outgrowth is outside the scope of this review, we refer the reader to a review by Zhang et al. for more information. 23
There is also an accumulation of extracellular amino acids at the site of injury, whose abundance relates to severity of SCI and neurotoxicity. 22 These molecules are attractive targets for pharmacological intervention aimed at enhancing neuroprotection and neuroregeneration post-SCI and are discussed more in the following sections. During secondary injury, damage occurs on the cellular level through several mechanisms, including mitochondrial dysfunction leading to high calcium levels, increased production of oxygen free radicals, and oxidative injury. 24
In chronic injury, scar formation is a problem and its disruption is a common strategy for promoting regeneration. For example, a recent study found that the protein tyrosine phosphatase σ (PTPσ) contributes to a transition of regenerating growth cones into dystrophic bulbs through interactions with chondroitin sulfate proteoglycans (CSPGs), which are abundant in the glial scar and many forms of which have been widely reported to inhibit axonal outgrowth. 25 Experimental inhibition of PTPσ was found to promote regeneration in a rodent model of SCI by enabling axons to overcome CSPG-mediated growth inhibition and, consequently, serotonergic fiber navigation across the SCI lesion leading to some functional recovery. 25
While the CSPG-rich glial scar was previously thought to be completely inhibitory to axonal growth, more recent studies have found that some aspects of scar ECM, which is secreted by astrocytes, are permissive and may even promote regeneration. 26 Furthermore, prevention, attenuation, or ablation of chronic astrocytic scars increased lesion size and reduced axonal ingrowth. 27 Recent studies found also that the ECM secreted by protoplasmic, but not fibrous, astrocytes can promote axonal elongation when injected into the rats' spinal cord after SCI. 26 Taken together, these findings suggest that while some aspects of the astrocytic scar may be detrimental, other components may be required for regeneration.
Therapeutic Approaches
Standard treatments
The management of SCI represents a formidable challenge, and there is no treatment at present available that can effectively restore lost tissue function. Several factors are responsible for the failure of healing after SCI, including chronic local inflammation and the release of antiregenerative factors. Present treatment methods include the use of neuroprotective and neuroregenerative strategies. The first line of management for SCI patients includes resuscitation, stabilization, and critical care in specialized centers with early determination and localization of specific injuries. Stabilization may include removal of bone fragments or foreign objects, physical stabilization of the vertebral column, and spinal decompression.
Nonpharmacological methods to reduce inflammation, including hypothermia 28 and cerebrospinal fluid drainage, 29 have also been in phase I/II clinical trials with promising early results. Early surgical decompression (within 24 h), administration of anti-inflammatory drugs, and augmentation of blood pressure lead to reduced acute complications and hospital stay. 6 Timely and early intervention is important and can be achieved by using neuroprotective measures (ideally in the acute stage).
The management of SCI also includes prevention and treatment of complications, and physical rehabilitation. Without these, there is very limited recovery of neurological function. 1 Besides failure of regeneration, SCI is often complicated by other problems such as infection and pressure sores, which can be serious and ultimately lead to death, such as in the case of the actor Christopher Reeve following his SCI. 30 Development of regenerative therapies to treat neurological deficit represents an active area of research and is a rapidly growing field. 6 Improved clinical outcomes will emerge by harnessing the potential of recent advances in different fields and integrating them to create innovative therapeutic strategies.
Neuroregenerative and neuroprotective therapies
Despite active research and clinical studies, there is no effective and globally accepted standard treatment for SCI. 8 Various minimally invasive, neuroprotective, and neuroregenerative strategies using cells, biomaterials, or pharmacological agents are in various stages of preclinical research and clinical trials around the world (Table 1 and Fig. 3). Clinical trials have evaluated agents that can neutralize axonal growth inhibitors, such as the Rho-ROCK inhibitor, Cethrin/VX-210, and anti-NOGO monoclonal antibody.6,31 However, no pharmacological agent for neuroregeneration (restoration of neurological function) has been approved by the U.S. Food and Drug Administration (FDA) for treatment of SCI. 32
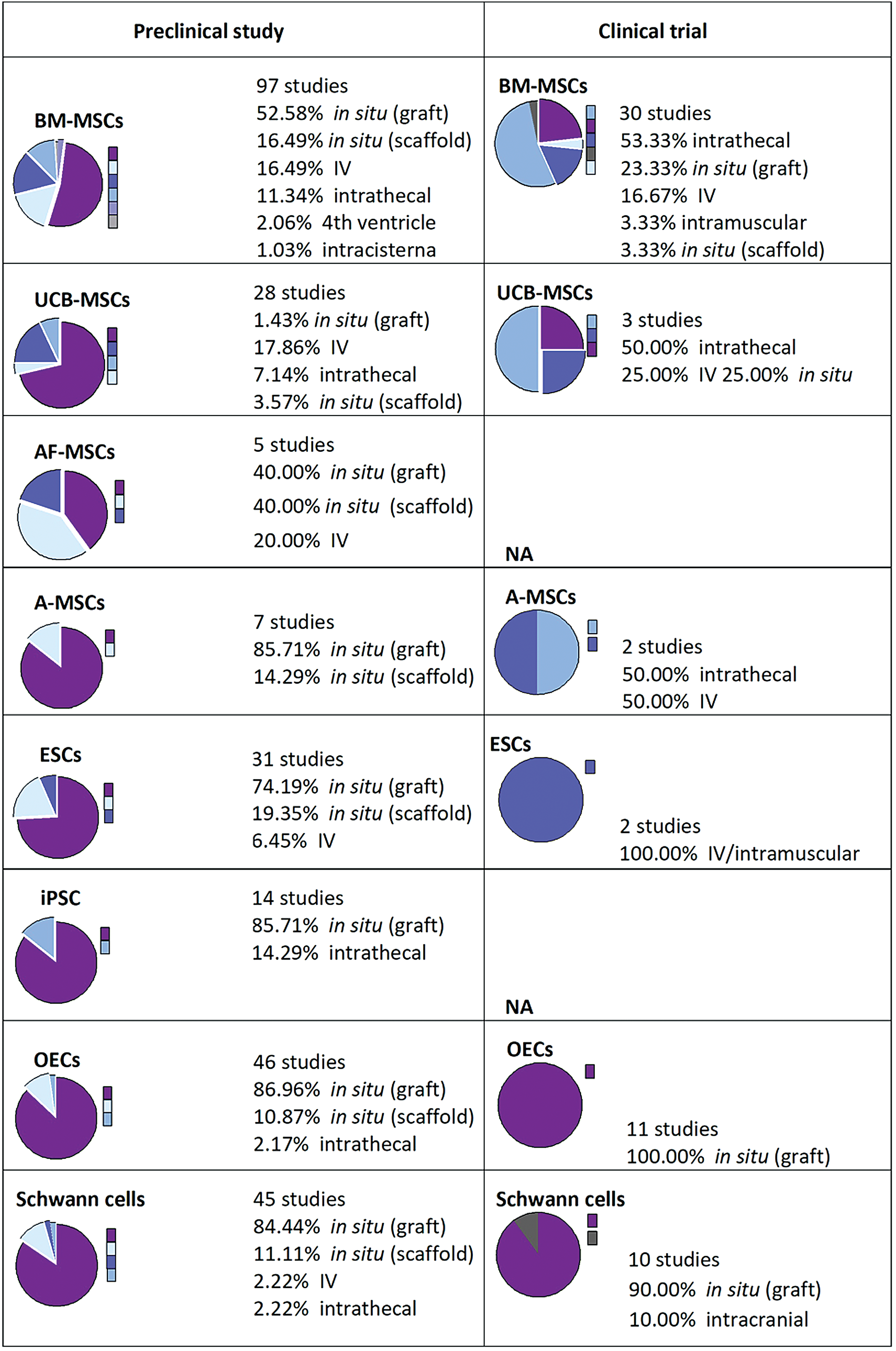
An illustration showing the global trends of clinical and preclinical studies in which cell transplantation is involved. Number of studies, type of cells (ESCs, BM-MSCs, A-MSCs, AF-MSCs, UCB-MSCs, or OECs), and routes of administration (IV, intrathecal, fourth ventricle, or intracisterna) are shown. When no data available, it was indicated as NA. AF-MSCs, amniotic fetal MSCs; A-MSCs, adipose tissue-derived mesenchymal stem cells; BM-MSCs, bone marrow-derived mesenchymal stem cells; ESCs, embryonic stem cells; IV, intravenous; OECs, olfactory ensheathing cells; UCB-MSCs, umbilical cord blood MSCs. Reproduced with permission from Vismara et al. 70 Color images are available online.
Biomaterials Studied for Treatment of Spinal Cord Injury
ECM, extracellular matrix.
Cell-based therapies may provide multiple benefits, including neuroprotection, angiogenesis, immune modulation, and tissue regeneration. Cell types evaluated have included stem cells (embryonic [ESCs], neural [NSPCs], or mesenchymal [MSCs]) and glial cells (Schwann cells, olfactory ensheathing cells [OECs], or oligodendrocyte precursor cells [OPCs]).1,6 In addition, electrical field stimulation of the injured spinal cord has been used to enhance neuronal plasticity and direct rewiring of circuitry into functional relays. 33 As in wound healing of other tissues, angiogenesis within the injured spinal cord tissue has been correlated with positive outcomes, particularly in studies delivering biomaterial, cell, or angiogenic soluble factors.13,34,35
Biomaterials have also been investigated for their inherent regenerative potential as well as for the delivery of therapeutic agents, including cells,9,16,36–44 drugs,36,45 growth factors,16,37,38,46 or genes (Fig. 4). 47 Combinations of these are also being investigated.16,36–38,48–51 Nevertheless, only one biomaterial has reached clinical trials, 52 while most remain in preclinical animal43,53–56 or in vitro stages of investigation.57,58 Even developed therapies with potential for clinical translation still require extensive testing to prove their safety and efficacy in patients. Further complicating results is the fact that there are no comprehensive studies to compare different strategies under identical conditions. Research groups can vary greatly in the choice of animal or injury model and are understandably restricted in scope. To date, none of these neuroregenerative therapies is used routinely in clinical practice.
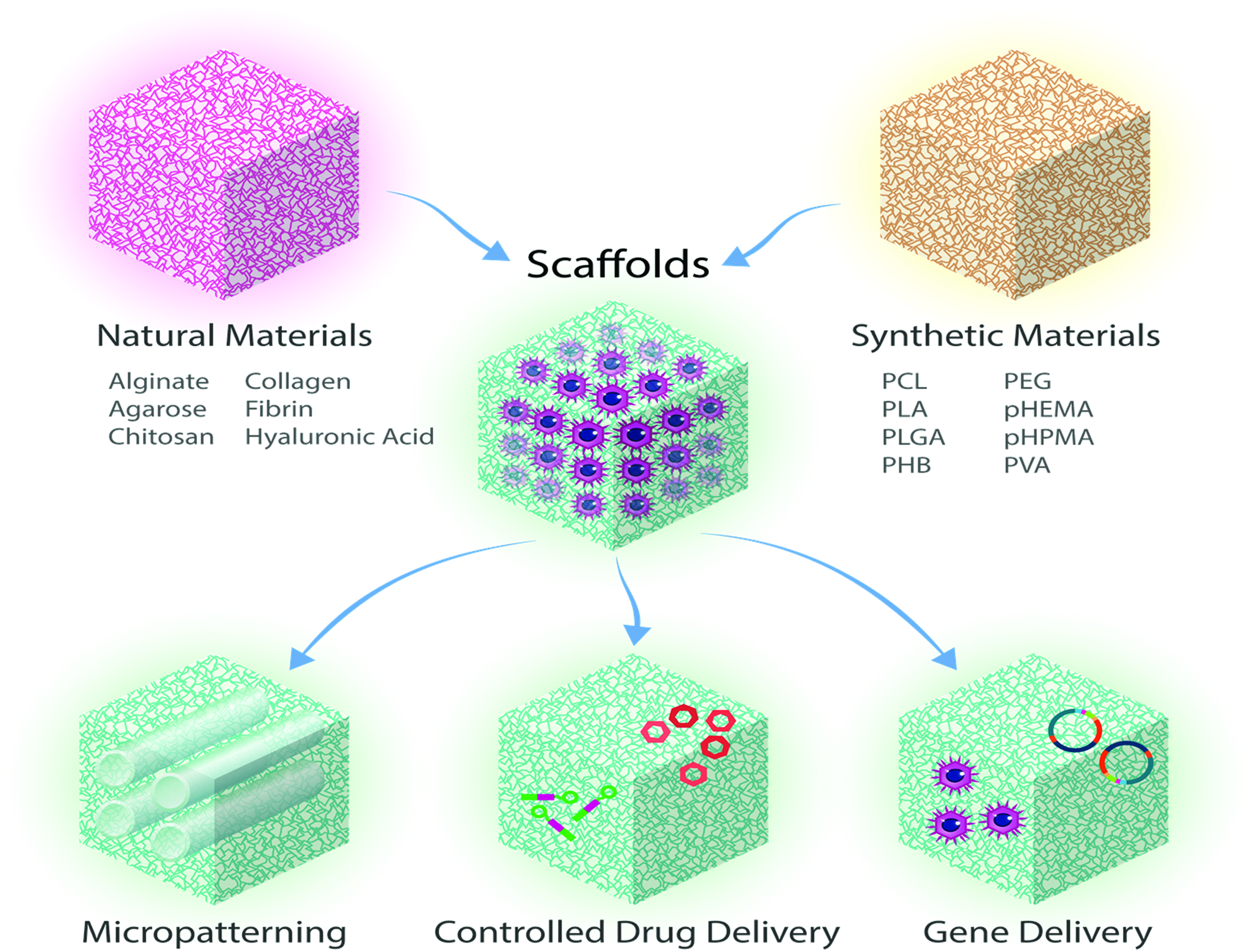
Illustration showing that scaffolds (made of synthetic or natural biomaterials) can be used for the treatment of SCI, as micropatterned devices or as matrices combined with drug delivery, or gene delivery to enable guided tissue regeneration. Adapted from Iyer et al. 201 Color images are available online.
Cell-based therapies
Cell-based therapy may be suitable for the treatment of discrete lesions in SCI (Figs. 3 and 5) to provide the following: (1) trophic support, 59 (2) immunomodulation,60,61 (3) angiogenesis, 35 (4) and generation of new CNS cells,1,6 which may form functional relays (Fig. 6).15,16,48 In addition, paracrine factors released by administered cells may aid in the activation of resident progenitors. 62 While stem cell therapies have shown promising results in clinical trials,63,64 translation faces substantial challenges, including timing and method of administration, 1 and risks that have to be carefully evaluated, including (1) poor survival of transplanted cells,46,63 (2) migration away from the delivery site,65,66 (3) formation of ectopic stem cell colonies or tumors, 67 (4) excessive proliferation, 37 (4) differentiation into unwanted, nonregenerative cell types, 68 and (5) aberrant axonal growth leading to allodynia. 69 Controlling stem cell differentiation or production of specific regenerative factors remains as additional key objectives.70,71
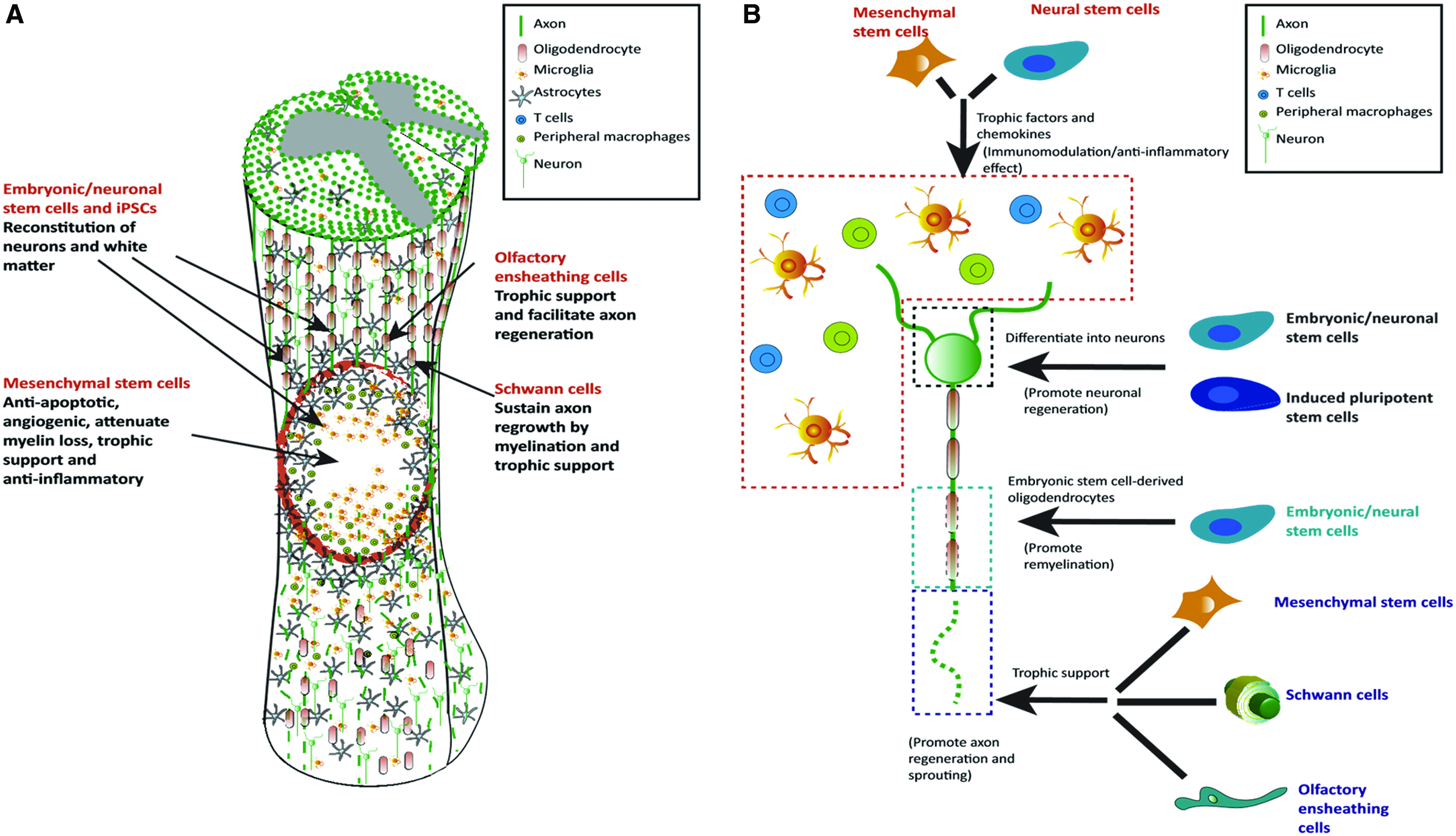
Schematic illustration showing the main cellular targets of cell therapy in SCI and how this works
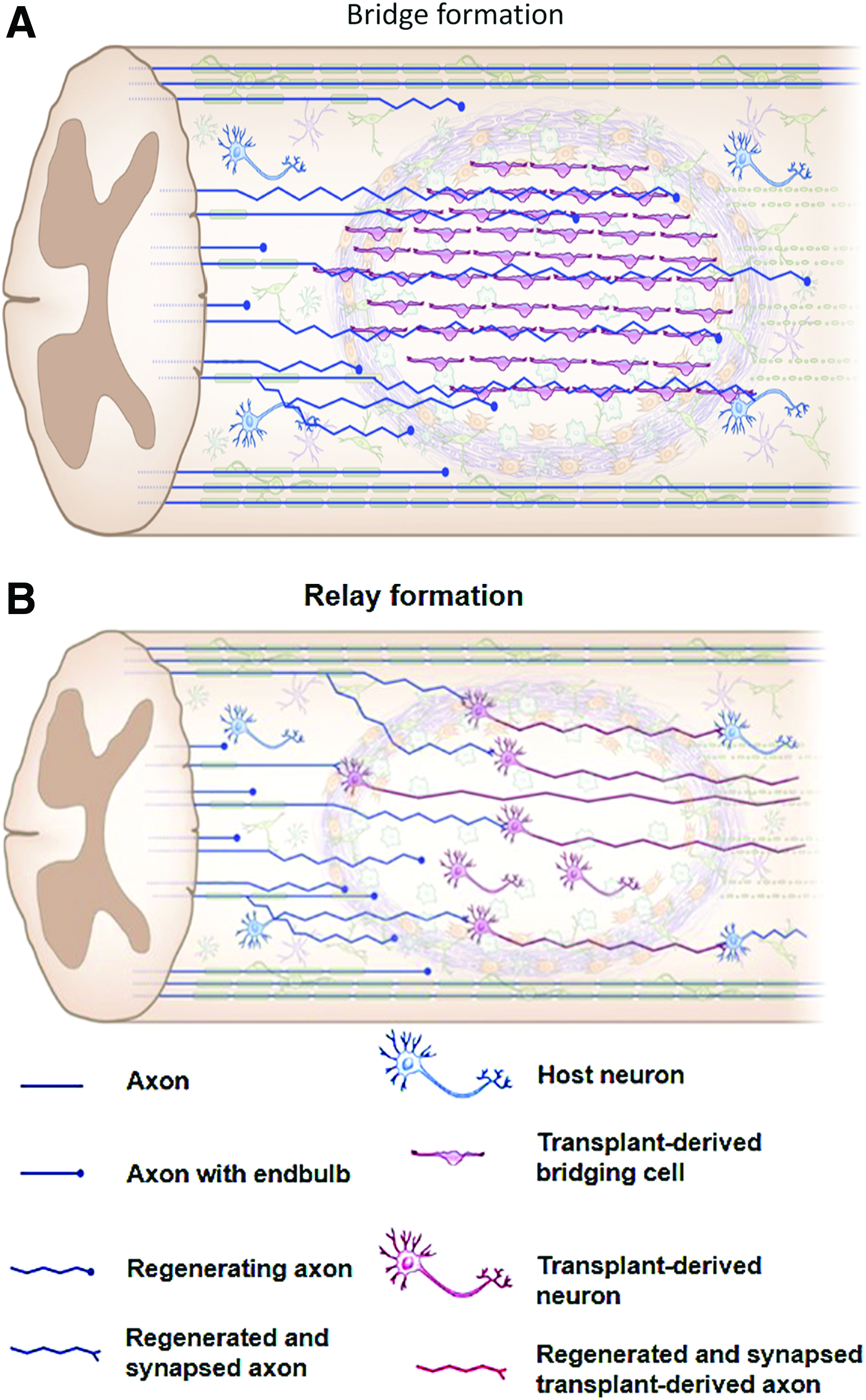
Schematic illustration showing bridge
While various cell therapies are being evaluated in clinical trials, none of these trials has progressed past phase I/IIa. 3 The absence of controls in these trials has limited their value, and the efficacy and long-term outcomes after treatment of SCI are yet to be demonstrated. 17 Financial costs of cell-based therapies are another major hurdle. Of the more successful clinical trials, one was terminated due to limited long-term effects, 72 while another was terminated for financial reasons. 73 Questions relating to the type of cells used, number, and safety remain to be addressed. 74 Stem cell therapy remains experimental and it cannot ethically be offered to patients as a proven form of treatment.
Despite these limitations, clinical and preclinical studies evaluating effects of transplanting several different cell types, including NSPCs, MSCs, Schwann cells, OPCs, and OECs, have shown promising results to date.1,6,17 NSPCs have been derived from human fetal spinal cord,63,75 human fetal brain,44,72,76 or pluripotent or ESCs 64 and can differentiate into the glial and neuronal cells, which normally make up the spinal cord. MSCs, including those derived from adipose tissue (A-MSCs), 77 umbilical cord blood, 78 and Wharton's jelly, 79 human OPCs derived from human ESC (hESC) lines, 64 and human NSPCs derived from fetal spinal cord tissues 63 have been investigated in clinical trials.
While not in clinical trials, there has also been recent interest in using human dental pulp cells (hDPCs) because they contain neural crest-derived ecto-MSCs. These cells were found to be more effective than bone marrow-derived MSCs in inducing functional recovery in rodents following SCI. 80 Another promising cell source yet to be used in clinical trials is the human inducible pluripotent stem cell (iPSC), which may help overcome issues with immune rejection of allogenic transplants.
These types of cells vary greatly in their tissue source and processing methods, often making it difficult to directly compare results obtained from different studies. For example, there is strong evidence that NSPCs or OPCs derived from hESCs using different protocols or obtained from varying sources may have different regenerative capacities. 46 For example, some preclinical studies reported robust results with the use of NSPCs, and it was found that axonal regeneration can be obtained even with the use of NSPCs obtained from a different species, for example, with the use of human NSCs in immunodeficient rats. 16 In contrast, other reports indicated that CNS-derived stem cells were not efficient in the treatment of cervical spine contusion injury in mice and may even have negative effects. 46
Recently, questions regarding the translation of preclinical data describing cell therapies to the clinic have been raised.46,81,82 It was found that there are differences in therapeutic effects between cell lots, such as that observed with the cell lots used for research and those of clinical grade of an NSPC product (human central nervous system stem cell [HuCNS-SC]) cell in preclinical studies by Anderson et al. 46 Although the use of a research-grade cell lot was successful in rat and mouse thoracic SCI models, transplantation of the corresponding clinical-grade cell lot into a cervical SCI mouse model provided no benefits. Moreover, some data suggested negative effects. 46
One possible reason for the difference is the heterogenicity of the fetal tissue from which these cells were derived. Donor genetic makeup, the location from which cells were taken, and the developmental stage at which the cells were isolated may all vary. In addition, protocols and reagents used to maintain and differentiate therapeutic cells may all lead to differences among study outcomes. 81 These difficulties may have contributed to the termination of clinical trials using HuCNS-SC transplantation for the treatment of SCI, which were terminated based on business decisions unrelated to any safety concerns.72,83 Differences between research-grade and clinical-grade cells will undoubtedly be a critical factor in the translational capacity of stem cell therapies.
Timing of the administration of cell-based therapy after SCI is very important. Early delivery after an acute injury may not be appropriate because the hyperinflammatory environment may lead to death of transplanted cells. On the contrary, delayed administration may result in no neuroregenerative effects because of the loss of cell plasticity at the site of injury and extensive scar and cyst formation. 74 Studies have suggested that cell transplantation during the subacute stage is more effective than that during acute or chronic stages. 1 Hence, in most previous studies, cells were administered during the subacute stage. 84 It was also found from a clinical study that cell application within the therapeutic window of 3–4 weeks post-SCI will have an important role in clinical settings to balance the feasibility of transplantation with optimal therapeutic efficacy. 85
Soluble bioactive molecule-based therapies
Soluble bioactive molecules, such as growth factors and drugs, have been explored as SCI therapies for their neuroprotective, neuroregenerative, angiogenic, and immunomodulatory effects. As discussed in detail later in this review, biomolecules are often delivered in combination with biomaterials.16,86,87 The use of carriers 88 such as hydrogels, and nanoparticles (NPs) can improve therapeutic drug delivery and efficacy. 89 Promising neuroprotective therapies for use in the acute stage of SCI that are being investigated for translation to the clinic include the use of various pharmacological agents such as riluzole, 90 magnesium, 91 minocycline, 92 hepatocyte growth factor (HGF), 93 and granulocyte-colony stimulating factor (G-CSF).6,94
In preclinical studies, improved axonal sprouting has been demonstrated in experimental SCI in rats to which antibodies against NOGO were delivered by cells placed into the parietal cortex. 95 Inhibition of phosphatase and tensin homologue (PTEN), a downstream target of NOGO-RhoA-ROCK in the sensorimotor cortex, has also been shown to promote corticospinal tract regeneration in rodents.96,97 Another recent study reported that the administration of connective tissue growth factor (CTGF) in zebrafish, after SCI leads to healing of SCI in these fish within weeks. 98 Recently, pregabalin, an established drug treatment for several neurological disorders, was also found to block the axonal regeneration inhibitor in mice, 99 and it is worth exploring its use further in SCI studies.
Biomolecules modulating the immune response are also candidates for SCI treatment. For example, blocking of the interleukin-7 (IL-7) receptor favors the generation of M2 phenotype macrophages and thus improves functional recovery after experimental SCI in mice. 100 Delivery of IL-4 and IL-10 chemokines to promote macrophages to adopt an M2-like phenotype has also been shown to improve recovery after SCI in a mouse model.101,102 The use of fractalkine, a chemokine that preferentially recruits reparative monocytes, was found to dramatically increase the regeneration of experimental nerve defects in rats 103 and thus may have benefits if used as a treatment for SCI.
Factors released by stem cells may also be useful in the treatment of SCI. 70 Intrathecal injection of conditioned medium of MSCs into experimental SCI in rats was found to increase axonal regeneration and improve locomotor recovery 1–4 weeks after the treatment. 59 Stem cell-conditioned media contain several potentially regenerative factors, including insulin-like growth factor 1 (IGF-1), vascular endothelial growth factor (VEGF), transforming growth factor β1 (TGF-β1), and HGF. It has been reported that the use of such media are more effective than using individual factors or their combinations in enhancing the survival of neurons and growth of neurites. 104
Factors secreted by stem cells can also have an important role in regulating immune cell phenotypes, that is, immunomodulatory action. Such secreted factors may influence neutrophils, macrophages, dendritic cells, NK cells, T cells, and B cells. 71 Furthermore, stem cell-derived exosomes can be used to modulate the recruitment and function of macrophages. 105 It is important to have a deep understanding of stem cell-derived exosomes, and their effect, to enable the development of novel therapeutic methods. 71 The use of these media or exosomes provides many future possibilities for their application in minimally invasive therapy of SCI.
Therapeutic biomolecules can also be used to stimulate resident NSPCs, various types of which are present throughout the spinal cord. 106 It has been suggested that ependymal progenitor cells, present in the central canal of the spinal cord, may enable regeneration in some animals even after severe injury. 107 Furthermore, ependymal progenitor cells in the glial scar can be beneficial. They can limit secondary injury by maintaining tissue integrity and releasing bioactive factors that promote neuronal survival.108,109 Thus, manipulation of the local ependymal stem cell niche 107 or mobilization of other resident progenitors 106 to stimulate self-repair through these cells may be a useful approach. 110 For example, delivery of factors known to promote oligodendrocyte-lineage differentiation during development in a mouse model of acute SCI, including sonic hedgehog, platelet-derived growth factor-AA (PDGF-AA), and noggin, has been reported to increase the numbers of myelinated, regenerating axons and functional outcomes.111,112
It is worth highlighting some recent outcomes of clinical trials investigating the use of antiregeneration inhibitors (Rho-ROCK inhibitors 113 and G-CSF 114 ) for the treatment of SCI. Rho-ROCK inhibitors are thought to have neuroprotective and neuroregenerative effects. 115 In a phase I/IIa clinical trial that involved 48 patients who had acute and complete cervical (C4-T1) or thoracic (T2-T12) SCI, the application of Rho inhibitor to the epidural space in a fibrin glue resulted in no increased adverse effects. Improvement in long-term motor function was best seen in cervical SCI patients who had the drug administered during 7.8–146 h after injury. 115
Despite these promising results, a phase IIb trial for treatment of acute SCI with Cethrin/VX-120 was halted in late 2018 due to lack of efficacy. 116 G-CSF is also being investigated for the treatment of SCI. 114 Two phase I/IIa trials94,117 and a small-scale double-blind, randomized clinical trial 118 have reported improved outcomes. However, future clinical trials that are larger in scale and randomized will be required to demonstrate the efficacy of the treatment with G-CSF.
While the majority of previous clinical studies have delivered potentially therapeutic agents either intravenously or orally, intrathecal delivery may provide better access to the injury and better approximates the design of many preclinical experimental studies with positive results. Thus, despite its more invasive nature, it has been argued that this route of administration will have better clinical success. 119 A recent phase I clinical trial reported the safety and tolerability of intrathecal infusion of the human anti-NOGO antibody ATI355 in patients after acute SCI. 31 In addition, a phase I/II clinical trial in which the HGF was intrathecally injected at the lumbar level in patients with cervical SCI was completed in 2018 in Japan, and results are expected in the near future. 119
Biomaterial-based therapies
So far, no biomaterial-based regenerative therapy of SCI is in routine clinical practice. However, a biomaterial technology, the Neuro-Spinal Scaffold, has recently reached clinical trials.52,120,121 Biomaterials used for the treatment of SCI can be in the form of conduits,101,112,122 sheets, 123 scaffolds,121,124 fibers, 125 particles, or hydrogels (Table 1).126–130 Biomaterials are used to mechanically stabilize the injury site and provide an environment for interactions with host cells, physically fill SCI-associated cavities, reconstituting ECM, and bridging the injury to guide axonal growth across the gap.70,101,112,121,131–135 To guide axonal regeneration, several biomaterial architectures have been investigated, including channels,86,136–138 fibers, 139 scaffolds, and magnetic microgels. 58
Biomaterials for the treatment of SCI can also be used for the delivery of therapeutic agents and cells (Fig. 4).6,132 In addition, they can support cell survival of delivered cells in situ,44,50 as discussed later in this review, and recruit migrating endogenous cells, such as Schwann cells 121 and stem cells,111,112,140 that can support regeneration. To avoid additional complexities associated with the use of cells, the use of acellular biomaterials for supporting spinal cord regeneration and remodeling after injury has been important to investigate.121,136,141,142
It is preferable that biomaterials be biodegradable and injectable for delivery through minimally invasive means. 70 In the acute phase of SCI, the use of a hydrogel is preferred as it may be used to seal the dura and release anti-inflammatory drugs. At later stages the use of fibers and conduits may be better for achieving guided neural regeneration. 132 However, it would be ideal to design a system that could be implanted acutely and remain for months to both guide regeneration and prevent chronic inflammation.
To achieve appropriate tissue repair, the implanted biomaterial should degrade as the host tissue regenerates. While biomaterials such as poly(lactide-co-glycolide) (PLGA) degrade hydrolytically,142,143 naturally derived materials such as fibrin are degraded by cell-produced enzymes15,48 and thus may have better potential for coupling degradation to native matrix formation, which is a challenging objective. Hybrids of synthetic and natural biomaterials can combine desirable properties of both types of materials. For example, synthetic biomaterials with controlled properties and tailored degradation profiles can be functionalized with peptides, which are susceptible to degradation by cell-produced enzymes,138,144 or provide sites for cell adhesion.121,125
Several different types of scaffolds have been investigated for the treatment of SCI. A scaffold made of a block copolymer of PLGA and poly-
Results from preclinical studies, where these PLGA-PLL devices known as “Neuro-Spinal Scaffold” were implanted into a thoracic-level contusion in rats and minipigs after internal decompression was performed, reported reduced inflammation and lesion cavitation volumes and increased tissue sparing and deposition of new, endogenous laminin-rich tissue. 121 However, no functional benefits were observed. The Neuro-Spinal Scaffold has recently been evaluated in small-scale clinical trials for treatment of thoracic-level SCI and has shown promising results.52,120
While porous polymeric scaffolds, such as those based on PLGA, have shown promise, hydrogel materials can be fabricated to better match hydration and mechanical properties of native spinal cord tissue, both of which are thought to reduce inflammation and scarring. In addition, hydrogels can be readily formulated to be injected and formed in situ in the spinal cord. In addition, microgels can be used for the delivery of cells,146,147 drugs, and/or biomolecules,70,89,148 and they can be interesting formulations to use in regenerative therapy of the spinal cord. For detailed reviews of hydrogels as minimally invasive therapies for spinal cord repair, the authors refer the readers to Perale et al., 127 Macaya and Spector, 126 Pakulska et al. 148 and Khaing et al. 149
The use of polyethylene glycol (PEG), an FDA-approved biomaterial used for many applications, is considered promising for the treatment of SCI because it can support stem cell growth, migration, proliferation, and differentiation. PEG hydrogels can also help to reduce local glial scar invasion, and promote and guide axonal regeneration.138,150 While PEG is essentially biologically inert, hydrogels containing bioactive polymers provide the opportunity to more directly affect cells in the spinal cord, and thus, the repair process. In particular, polymers derived from the native ECM, including hyaluronic acid (HA),26,44,50,151–155 fibrin,37,42,48 and laminin,125,156,157 have shown success in preclinical studies.
In contrast to including individual ECM components, cell-secreted ECM compositions have also been shown to aide in regeneration.43,125,158 Alternatively, spinal cord tissue, decellularized to preserve not only the ECM composition but also the structure, has been found to enhance axonal regeneration in the spinal cord of rats. 159
A number of studies have found that provision of a physical structure to guide regenerating axons along the longitudinal axis to their targets in the form of conduits or channels enhances functional recovery after SCI. For example, collagen-based neural conduits were functionalized with the neurotrophin-3 (NT-3) gene and used for the treatment of completely transected spinal cord in rats. 47 Increased NT-3 levels seen in surrounding tissues and axonal regeneration, observed 1 month postoperatively, were significantly higher than in controls.
PLGA scaffolds with multiple guidance channels implanted in mice were found to be sufficient for promoting corticospinal tract axonal regeneration into the channels, through the injury site, and out of the conduits, where they have the opportunity to connect with synaptic targets caudal to the lesion. 160 In this study, the extent of axonal regeneration was found to correlate with functional recovery. Hydrogels made from multiple base materials and containing guidance channels have been reported to promote regeneration in animal models of SCI.9,138,161,162 A recent report by Koffler et al. described the use of a microscale continuous projection printing method to create hydrogel scaffolds with guidance architectures that conform to contusion lesions in unique animals. 161
While conduits and channels provide macroscale guidance structures, nanofibers that mimic the nanostructure of the native ECM have been developed for regenerative biomaterials and studied in vitro and in vivo.163,164 Nanofibers have been shown to guide the orientation of regenerating neurites parallel to their orientation. 165 In addition, the use of electrospun nanofibers has been associated with ESC differentiation toward neural lineages. 166 Recently, it was found that peptide nanofibers containing long laminin motif can influence neurogenesis both in vitro and in vivo. 157 Synthetic poly(ɛ-caprolactone) (PCL) nanofibers were also investigated and found to successfully create electrically active human three-dimensional (3D) neuronal networks with synapses using brain neural progenitors. 167
Engineered NPs have been explored for their use for the regeneration of the spinal cord. For example, PLGA NPs were used for local delivery of flavopiridol (a cyclin-dependent kinase inhibitor that inhibits astrocyte growth and inflammatory agent synthesis), and they resulted in recovery following SCI in rats. 168 Using a biological ligand, gold NPs were bonded to neurons for optical excitation and they exhibited potential benefits over optogenetics. 169 Pulsed infrared light and plasmonic gold nanorods were also used to enhance infrared neural stimulation by increasing neural responsivity. 170
Intravenously injected NPs made of ferulic acid-modified glycol chitosan were shown to be effective in achieving functional restoration after SCI in rats. 171 Moreover, magnetic NPs coupled to HA-based hydrogels can be used to modulate the activation of mechanosensitive ion channels in dorsal root ganglia neurons as it was demonstrated in vitro. 20 Nanofibers can be combined with therapeutic agents and NPs 164 to enhance their function. For example, gold NPs were incorporated into electrospun PCL/gelatin nanofiber-based scaffolds. Neuronal cells were subsequently seeded onto these scaffolds and resulted in axonal elongation forming 3D networks in vitro. 18 In another example, zero valent zinc NPs included in a PCL matrix using electrospinning were found to promote neuroglial cell proliferation in vitro. 19
In addition, electroconductive (e.g., graphene) or magnetic (e.g., iron oxide NPs) elements can be incorporated into scaffolds. The use of electroconductive materials and applied electromagnetic fields may help to influence cell migration, adhesion, proliferation, and differentiation.
172
For example, magnetic NPs can be used to guide neurite growth
173
and enable the control of cell organization and differentiation (Fig. 7).
174
It was found that when polypyrrole-coated poly (
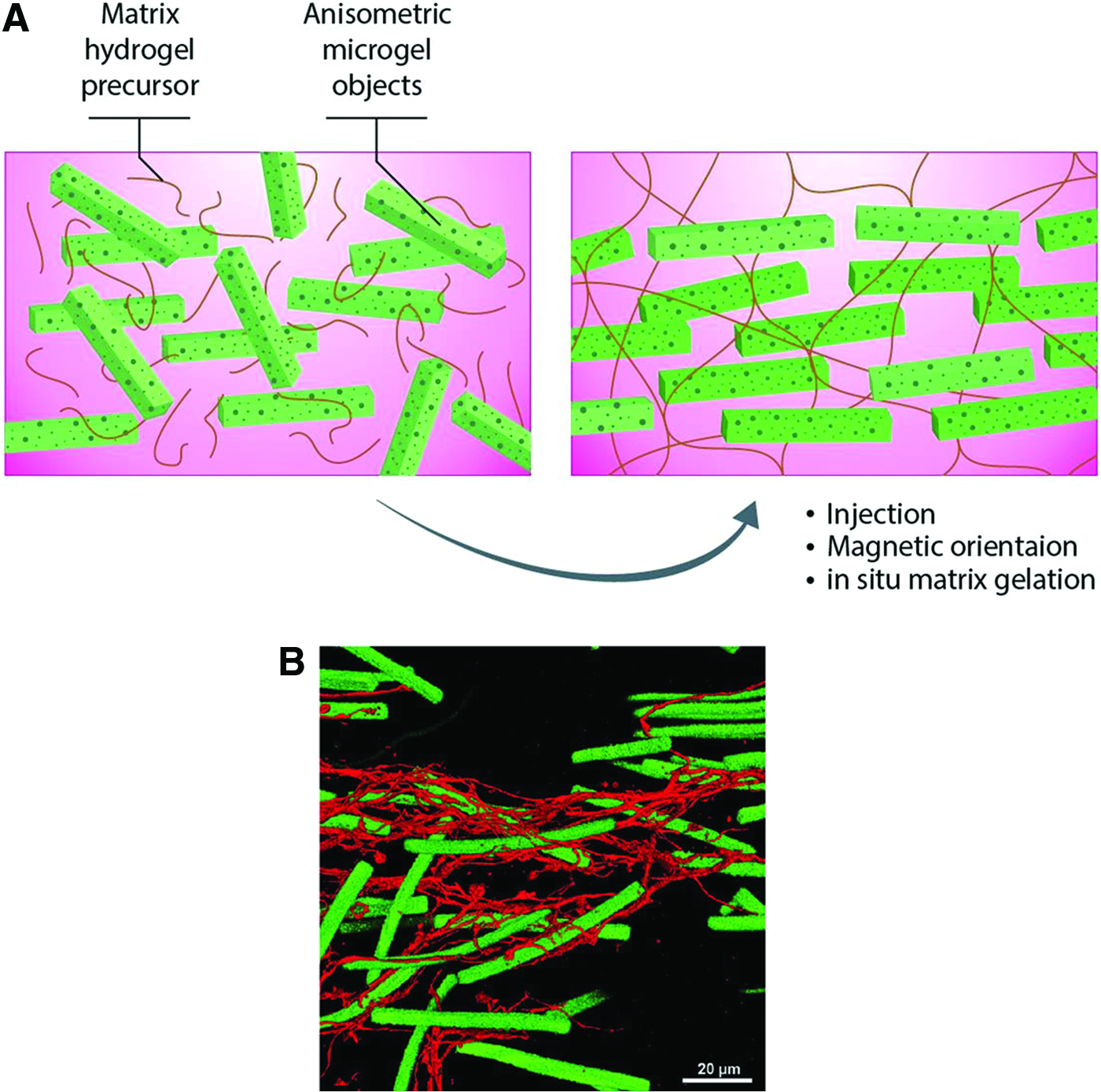
The use of magnetic rods in fibrin hydrogel to help guide regeneration that can be aligned upon exposure to magnetic field.
Combined with electrical stimulation, conductive carbon nanofiber-based scaffolds were found to enhance the regenerative function of NSPCs. 177 Moreover, core-shell-structured, piezoelectric polyvinylidene fluoride (PVDF) nanofibers that were chemically wrapped by graphene oxide lamellae showed a desirable out-of-plane piezoelectric constant higher than that of the conventional pure PVDF nanofibers. 178 To produce graphene-containing silk, a recent method reported feeding of graphene to silk-producing worms to create silk with new properties, 179 adding to the available fabrication methods.
The concept of biomaterials that can be injected and form a defined guidance architecture in situ is attractive; nevertheless, development of such biomaterials has posed a formidable challenge. Promising strategies to overcome this challenge include the use of scaffolds that are based on self-assembling fibers56,95,124,180 or that are embedded with magnetically responsive microgels. 58 In an interesting study, poly(ethylene oxide-stat-propylene oxide) gels containing supermagnetic iron oxide nanorods were used to help the orientation of nerve extension parallel to the rods that were aligned by using an external magnetic field.58,181 This offers a great opportunity to develop minimally invasive and regenerative therapies for SCI.
Combinatorial therapeutic approaches
Because of the complex nature of pathophysiological changes that occur following SCI, combinatorial approaches that address different aspects of the problem are expected to be more effective. In such an approach, biomaterials may be combined with cells and soluble molecules and administered locally to an injury. It is evident that biomaterials can provide sustained drug delivery, enhance survival, growth, host tissue integration, and even differentiation of delivered cells (Fig. 4). 182 Attention should be paid to proper biomaterial selection, tailored drug release, source and processing of therapeutic cells, and timing of intervention. Despite recent advances in these therapeutics, there is still a likely long way to go to achieve a therapy that can lead to significant recovery after SCI. 183
Biomaterials and soluble biomolecules
In one approach for the treatment of SCI, biomaterials and bioactive molecules can be combined (Table 1). There are many examples of procedures using soluble molecule delivery, for example, growth factors,86,87,184,185 drugs, 115 or other therapeutic agents,54,186–189 for the treatment of SCI. Combining biomaterials with diffusible factors, and even gene therapies, can maximize therapeutic effects by targeting more than one aspect involved in SCI.
Biomaterials can also maintain appropriate local therapeutic concentrations at or near the injury site over longer periods of time than bolus injection and hence better support regeneration.
70
For example, hydrogels fabricated from a hydrolytically degradable macromer [poly(
Biomaterials and cells
The use of biomaterials to deliver cells after SCI has been reported by several studies to improve treatment efficacy (Table 1). 190 Biomaterials may physically protect loaded cells from the hostile environment of SCI, retain administered cells near the injury site, and provide an adhesive matrix for cells and other cues to improve their survival.43,191 By minimizing the loss of delivered cells, the number of cells required for achieving a therapeutic effect can also be reduced. 43 Promising results with the use of different biomaterial/cell combinations have been observed in experimental SCI models. These include neurotrophic factor expression, 13 improved postimplantation cell survival,11,16,44,50,138 neuronal differentiation, 10 and directed axonal regeneration. 9
Although various forms of biomaterials can be used, hydrogels represent an attractive form as they can be easily used as minimally invasive therapies. A study by Kadoya et al. demonstrated some potential advantages of delivering therapeutic cells via methods that are minimally invasive, specifically those that maintain an intact dura. 16 The study observed formation of ectopic stem cell colonies in rats that were administered a cell-laden fibrin matrix, which also contained a cocktail of growth factors, after opening the dura. However, no ectopic colonies were observed in closed dura delivery, where no growth factor cocktail was used. 16 In addition, injection delivery of cells within hydrogel can help to reduce cell death induced by mechanical stresses. 192
Several combinations of biomaterials with cells have previously reported varying outcomes of axonal regeneration and functional recovery in experimental models of SCI (Table 1). These have included HA hydrogels with NSPCs, 44 self-assembling peptides with NSPCs, 12 PEG hydrogels with human iPSC-derived NSPCs, 10 polyurethane-based gel with MSCs, 193 and Matrigel with Schwann cells. 194 A fibronectin-mimetic, peptide-grafted gellan gum hydrogel was combined with A-MSCs and OECs and evaluated for the treatment of experimental SCI in rats. It was found that hydrogel encapsulation of both A-MSCs and OECs led to increased axonal regeneration and significant improvement in motor function. 195 Delivery of OECs via PQLA/PLGA scaffolds improved cell survival and proregenerative efficacy in the rat SCI model. 13 Delivery of mouse E14 spinal progenitors, loaded onto multichannel PLGA bridges providing a guidance architecture, showed marked improvement of axonal and functional regeneration in a mouse model of thoracic SCI. 196 However, another study found that collagen microfibers combined with neural progenitor cells from an alternative source failed to form a bridge across the injury site, or recovery of the motor function in a mouse SCI model. 39
It has been proposed that the combination of human MSCs and biomimetic hydrogels could modulate the immune cell microenvironment in SCI, leading to increased proregenerative M2 macrophage population. 43 The use of an MSC-seeded alginate hydrogel was found to promote linear axonal regeneration in an experimental rat C5 hemisection SCI model. 9
In a separate study, MSCs combined with a collagen sponge were found to facilitate neurite elongation in a rat model of SCI. 197 In another study, injectable scaffolds made of self-assembling peptide nanofibers containing bone marrow homing, bioactive peptide motifs were described. When combined with human endometrium-derived stromal cells (hEnSCs), these materials were explored for the treatment of experimental chronic SCI in rats. The nanofibers were found to support neural differentiation of hEnSCs. In addition, higher axonal regeneration and myelination were also demonstrated. 181 MSCs are thought to promote neuronal regeneration through neurotrophic protection and immunomodulation. 60
Cells and soluble biomolecules
Although there are some studies that have combined cells or growth factors with biomaterials for SCI treatment,16,36–38 relatively few have used combinations of cells and growth factors alone. In some studies, cells themselves were applied as delivery vehicles for specific factors. For example, FGF2 was used to prime hDPCs that were subsequently injected into a complete transection model of SCI in rats. Some axonal regeneration and locomotor recovery were observed. 198 In vitro, astrocytes were transfected to overexpress nerve growth factor (NGF) and encapsulated into a collagen scaffold. They were then added to rat dorsal root ganglion culture and found to significantly enhance axonal growth. 21 Cells were conjugated with adjuvant drug-loaded NPs and were found to enable pseudoautocrine stimulation of transplanted cells. 199 Finally, ESC-derived OPCs were combined with the ciliary neurotrophic factor (CNTF) and used to treat experimental SCI in rats leading to significant improvement in hind limb locomotor function. 200
Biomaterials, soluble biomolecules, and cells
Combining biomaterials, stem cells, and biomolecules represents a critical 201 and promising 14 approach that may improve recovery after SCI. 36 Exciting recent work has demonstrated that delivery of human NSPCs within a simple fibrin matrix containing a growth factor cocktail after SCI supports extensive engraftment with host neuronal circuits leading to functional recovery in both rodent 15 and nonhuman primate models. 48 Another recent study used a combinatorial therapy comprising a scaffold containing Schwann cells modified to overexpress NT-3 and adult stem cells modified to overexpress the NT-3 receptor TrkC. 202 In each of these studies, results suggest that NSPCs can integrate with the host tissue and act as neuronal relays across SCI leading to functional gains.
A separate study incorporated NT-3 within silk fibroin coatings on poly(ɛ-caprolactone)-block-poly(
Beyond growth factors, a hydrogel delivery platform based on SH3 affinity has been used to deliver chondroitinase ABC in combination with human iPSCs, resulting in better survival of both host and transplanted cells. 51 Liu et al. have described an approach where alginate biomaterials with longitudinally aligned channels to provide guidance were seeded with Schwann cells and implanted into cervical lesions in rats. 49 Adenovirus encoding BDNF was delivered caudally to the lesion to encourage axons to regenerate along the rostral/caudal axis and allow axons to exit biomaterial implants and re-enter the caudal spinal cord.
Other therapeutic approaches
Because of the complexity of the healing process of the spinal cord after SCI, taking advantage of non tissue engineering approaches may further support restoration of function. For example, small-scale clinical studies have demonstrated that the use of epidural electrical stimulation, in particular in conjunction with dynamic, task-specific training, can restore voluntary, coordinated motor activity in previously paralyzed individuals following SCI.204–207 It is envisioned that combining proregenerative drugs, biomolecules, and/or cells with electrical stimulation and/or rehabilitative training will lead to better results. This type of approach would be expected to create a proregenerative environment supportive of axonal growth and plasticity, which would then be guided to form and maintain relays for different bodily functions via direct neuromuscular stimulation. 33 For example, Chen et al. found that treatment of rats with anti-NOGO-A antibodies after incomplete thoracic SCI followed by treadmill locomotive training improved motor recovery. 208
Challenges and Future Perspectives
Many obstacles to the development of successful treatments for SCI remain, including reproducibility of the therapeutic paradigm (in particular with combinatorial or multimodal therapies), variations in the location and severity of SCI across patients, and clinical variability and recognizing the appropriate timing for treatment intervention, remain to be addressed. Cell-based therapies will face challenges concerning both preclinical processing and clinical administration, such as identifying the optimal number of cells for transplantation that balances efficacy and safety, improving survival of transplanted cells, and directing cell differentiation and functional integration with the host circuitry.
Important challenges also include issues related to interspecies variation and preclinical experimental models. For example, while rat SCI is more pathologically similar to the human case than mouse SCI, 209 mice have been used more frequently in preclinical studies. Even the use of rat models is not ideal as these have fundamental differences from humans, and thus, results cannot always be translated to humans. For example, the efficacy of successful cell therapy observed in animal studies has not been reproduced in human clinical trials. 17 In addition, while cervical SCI is the most common injury in human patients, it has been less often investigated in preclinical studies. 70 Instead, many preclinical studies have used lumbar and thoracic models that are technically easier to perform. 210 Therefore, more clinically representative models should be considered and developed in the future.
Given these considerations, preclinical results should be interpreted cautiously. For example, axonal regeneration does not always mean functional recovery. Efforts should be made to identify specific populations of axons responsible for functional recovery. The reversible neuronal silencing technique is a possible method for this purpose. 211 However, regeneration of large numbers of axons, which can exit spinal cord lesions caudally, remains a significant challenge. 17 There are also differences between animals and humans in biological cues, and hence, the extrapolation of results can be difficult.
Although there have been several reports of cell-based therapies for the treatment of SCI, including clinical trials, treatment efficacy is yet to be demonstrated in phase I-II trials. 3 Recently, questions regarding the translation of preclinical data to the clinic have been raised.46,81,82 It is difficult to define potency in cell products and current good manufacturing practice (cGMP) requires testing for the markers that are essential to identify desired cells and contaminants and as indicators of potency. In addition, the FDA does not require a definitive potency assay for early clinical studies. While this policy may serve to speed up translation of some therapies, it leaves room for variations in final products leading to a risk of failure in clinical trials. 81 Thus, researchers must balance the need for extensive product characterization with that for helping patients sooner. It should be noted that no preclinical model is ideal, and thus, the ultimate testing for efficacy lies in the human clinical setting. 212
In the future, the use of iPSC-derived cells may help to avoid hurdles associated with possible immune rejection of allogenic cells. They may also mitigate the need to address issues with variability across lots, as each batch of therapeutic cells would be tailored for each patient. However, iPSCs will require thorough investigation into the safety of their clinical use, as possible genetic and epigenetic abnormalities may occur during their induction and tumorigenicity after their transplantation. 84 Tools, including the use of clustered regularly interspaced short palindromic repeats (CRISPR)-mediated gene editing, have helped to identify key players involved in the cell response to injury, and may aid in developing methods to enhance the ability of stem cell-based therapies to restore function after SCI. 213
Real-time, in vivo imaging, data communication and control can be integrated in future therapeutic strategies.214,215 For example, the next wave of innovations would likely include smart, multifunctional materials that can sense, respond, actuate, and report with remote control.215–217 The use of dynamically bioresponsive materials216,217 for developing a new generation of therapeutic constructs may also be useful. 218 Such materials can be designed to provide graded, temporally and spatially controlled release of various agents, 219 and even stimuli-responsive behavior than can be triggered by external or internal means. Biomaterials may also have electroconductive elements and electroresponsive properties. In addition, including in situ organizable structures (e.g., with the use of magnetic rods 58 ) may promote organized guidance of regenerating axons/neurites. For example, the incorporation of superparamagnetic iron oxide NPs would help targetability under the influence of external magnetic field. This type of approach has the potential to yield new nonsurgical treatment options for SCI. 220
Organ-on-a-chip technologies have been developed and used to build various models for studying normal physiology and pathological conditions.221–223 Such models may be used in the future to study the various stages of pathophysiology of SCI, and to develop and test new therapeutics. Organ-on-a-chip models can be more representative to native tissues than conventional two-dimensional cell culture and can possibly recapitulate human cell behavior better than animal studies.223–225 It would be a great advantage to have SCI-on-a-chip models that may help to overcome some of the present challenges, especially those related to the development of effective therapy for a difficult condition.
Commercialization of newly developed therapeutics will depend on the feasibility of scaling up for mass cGMP production, demonstration of clinical safety and efficacy, and obtaining regulatory approvals. When developing therapies integrating diverse technologies (e.g., devices, drugs, and cells), regulatory approval presents additional challenges, such as how these combination therapies affect the body differently than might be expected for each component alone. Thus, new combination products will require extensive preclinical characterization. Targeting more specific SCI pathologies when designing trials, and the use of new imaging technologies and biomarkers 6 also promise to improve evaluation of outcomes.
There is a need to build upon already obtained clinical results to refine therapies and, in particular, cell-based therapies that are relatively new and for which the optimal potency, cell types, and dosing for therapeutic benefits are crucial to characterize. In addition, successful clinical translation will require development of safe methods for cell transplantation. Complications and risks related to the use of stem cells, such as the formation of ectopic colonies, need to be carefully assessed and resolved. More studies are needed to optimize minimally invasive delivery methods that may lead to reduced risk of cell migration. 16
Moreover, a multidisciplinary approach involving clinicians, researchers, pharmacologists, materials scientists, and bioengineers will be indispensable to achieve successful treatment of patients with SCI, a very challenging, yet important, clinical goal. Development of a global consensus and standardization for cell-based therapies should be encouraged to curb the misuse of these interventions as curative means and maximize the ability of scientific studies to advance innovative treatments for SCI. 74
Conclusions
SCI is a devastating condition with a complex pathophysiology for which no present therapies can restore lost neurological functions. The last decade has produced increasingly intensive research that has led to the development of a few cell-based therapies that have proceeded to clinical trials. Unfortunately, despite successes in preclinical animal studies, efficacy has not been reproduced in humans. To date, the most successful results have been obtained using a combinatorial therapy that used biomaterials, cells, and soluble molecules. It is anticipated that addition of electrical stimulation of the spinal cord to these therapies will achieve a better outcome. At present, functional recovery after SCI is a long process that may take years and it is unlikely that a full recovery will ever be achieved. The development of minimally invasive approaches is desired to reduce complications and avoid additional injury to the spinal cord. Nevertheless, several barriers remain to be overcome through a multidisciplinary approach and consensus based on integrated evidence and recruitment of advances made in different fields of science and technology.
Footnotes
Acknowledgment
Thanks to Mohammed Xohdy for help with drawing figures.
Funding Information
The authors also acknowledge funding from the National Institutes of Health (EB021857, AR066193, AR057837, CA214411, HL137193, EB024403, EB023052, EB022403, and EB021857), Air Force Office of Sponsored Research under award No. FA9550-15-1-0273, and a National Science Foundation Career Award (S.K.S., 1653730).
Disclosure Statement
The authors acknowledge that they have no competing interests.