
Abstract
Cell therapies are an up and coming technology in orthopedic medicine that has the potential to provide regenerative treatments for musculoskeletal disease. Despite numerous cell therapies showing preclinical success for common musculoskeletal indications of disc degeneration and osteoarthritis, there have been mixed results when testing these therapies in humans during clinical trials. A theory behind the mixed success of these cell therapies is that the harsh microenvironments of the disc and knee they are entering inhibit their anabolism and survival. Therefore, there is much ongoing research looking into how to improve the survival and anabolism of cell therapies within these musculoskeletal disease environments. This includes research into improving cell function under specific microenvironmental conditions known to exist in the intervertebral disc (IVD) and knee environment such as hypoxia, low-nutrient conditions, hyperosmolarity, acidity, and inflammation. This research also includes improving differentiation of cells into desired native cell phenotypes to better enhance their survival and anabolism in the knee and IVD. This review highlights the effects of specific musculoskeletal microenvironmental challenges on cell therapies and what research is being done to overcome these challenges.
Impact statement
While there has been significant clinical interest in using cell therapies for musculoskeletal pathologies in the knee and intervertebral disc, cell therapy clinical trials have had mixed outcomes. The information presented in this review includes the environmental challenges (i.e., acidic pH, inflammation, hyperosmolarity, hypoxia, and low nutrition) that cell therapies experience in these pathological musculoskeletal environments. This review summarizes studies that describe various approaches to improving the therapeutic capability of cell therapies in these harsh environments. The result is an overview of what approaches can be targeted and/or combined to develop a more consistent cell therapy for musculoskeletal pathologies.
Introduction
Musculoskeletal diseases are a major health care concern, ranking second in years lived with disability (YLD). 1 Disability due to musculoskeletal disease is increasing and is expected to continue increasing with the rise of a sedentary and aging population. 1 The two most prevalent musculoskeletal diseases that also rank highest in YLD in this disease category include low back pain, often caused by disc degeneration (DD) of the intervertebral disc (IVD),2–6 and osteoarthritis (OA) of the knee. 1 The category of “other musculoskeletal conditions” also contributes largely to YLD within the category of musculoskeletal conditions and includes ligament injury and tendonitis. 1 Current gold standard clinical treatments for these musculoskeletal diseases are largely palliative during moderate stages and fail to regenerate tissue or retard disease progression.7–10
Due to a lack of treatment options, many patients suffering from chronic pain from musculoskeletal diseases resort to the use of pain medications, 11 which often include highly addictive opioids that have resulted in a major health crisis of abuse in the United States. The current surgical approach commonly utilized to treat end-stage knee OA and spinal DD, arthroplasty, or spinal fusion can have poor outcomes and leaves patients with foreign materials in their bodies that may require revision surgeries, especially if the procedure is performed early in life. 12
To identify novel treatment approaches aside from such invasive surgeries, there has been a rise in the number of cell therapy-based clinical trials for these musculoskeletal conditions.13,14 If cell therapies are shown to reduce pain and extend the time to subsequent intervention (such as knee arthroplasty or spinal fusion), they would present a highly desirable option for patients with these conditions. While being minimally invasive, cell therapies also have the potential to provide a multifunctional mode of action with the ability to address the complexities of OA and DD, including regenerative and anti-inflammatory effects. They also have a historically safe track record,14,15 which is especially important when navigating regulatory pathways that require extensive safety, toxicity, and tumorigenicity evaluation, ultimately coupled with direct evidence of positive clinical outcomes. 16
The gold standard cell therapy for cartilage repair has been autologous chondrocyte implantation and has existed since 1994. 17 However, due to the requirement of multiple surgeries to obtain these cells, and other commercialization challenges, market acceptance has been limited, and now, new cell therapies are being investigated for cartilage regeneration with more favorable clinical use profiles. The cells being tested in these investigations include peripheral blood stem cells, as well as adipose-, bone marrow-, and umbilical cord-derived mesenchymal stem cells.14,18 Mesenchymal and peripheral blood stem cells have been tested clinically and have shown success, but the results are still mixed and inconsistent even between different measurements in the same clinical studies. 14
For the IVD, several cell types have and are being tested, including adipose-, bone marrow-, and umbilical cord-derived mesenchymal stem cells, articular cartilage- derived chondrocytes, hematopoietic stem cells (HSCs), and IVD-derived cells.13,15 With the exception of HSCs, cell therapies investigated clinically for treatment of IVD-related pain have overall shown improvements in pain and disability measurements, but the measurements of regeneration have shown more mixed results.13,15 Interestingly, IVD-derived cells and chondrocytes fair better in outcome measurements, especially those measuring active regeneration or delay of degeneration (i.e., disc height, hydration). 13
Overall, results of clinical studies of cell therapies in both disc and cartilage demonstrate that cells native to these respective treatment environments fair better in treatment outcomes. This makes sense as these tissue environments are harsh for non-native cells due to multiple characteristics, including hypoxia, low-nutrient levels, chronic inflammation, acidity, and hypertonicity, which have negative effects on delivered cells (Fig. 1).19–22 To make cell therapies that are more consistently successful within these environments, there is a need to understand the biology and engineer these therapies in a manner that allows them to withstand these conditions better.
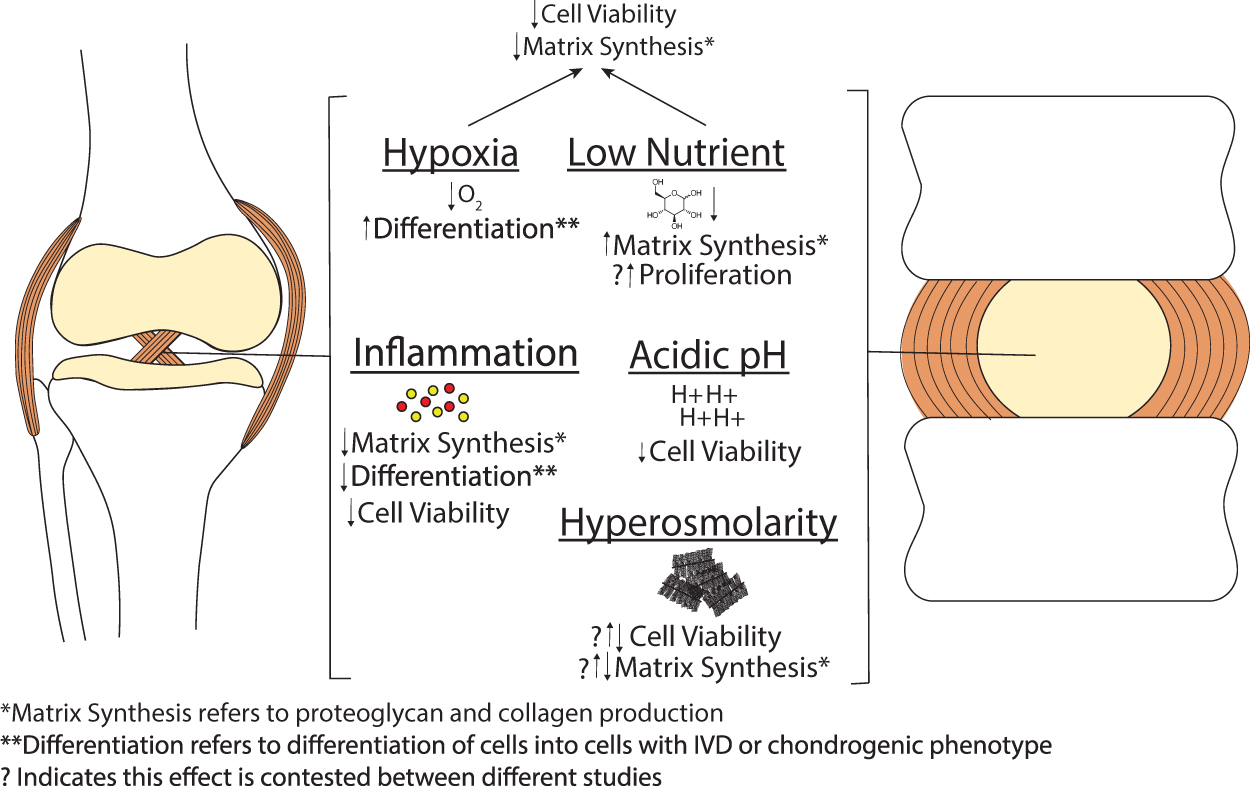
Microenvironmental factors within musculoskeletal environments of the pathological knee and intervertebral disc and how they positively or negatively affect cells delivered to these environments.
This centers around several goals that include improving differentiation and paracrine effects within musculoskeletal disease environments, and decreasing the negative response toward inflammatory cytokines. Improving differentiation and paracrine effects within these environments is useful as it allows these cells to best achieve a native cell phenotype once delivered, and could enhance their survival and regenerative effects. Decreasing the negative response toward inflammatory cytokines is another crucial aspect of improving these cell therapies as these disease environments have a chronically elevated level of inflammatory cytokines that have negative effects not only on stem cells but also on native cells delivered.20,21,23
There is ongoing research attempting to achieve these goals in numerous ways. The purpose of this review is to highlight the challenges presented by diseased musculoskeletal tissue environments toward cell therapies, and to summarize current research that is being done to enhance cell therapy regenerative effects and survival, as well as decrease negative responses toward the harsh environmental conditions presented by musculoskeletal diseases. This review is broken up into two parts, with the first focusing on specific targeting of environmental factors found in the musculoskeletal disease environment to promote cell function/survival, and the second focusing on more generalized methods for promoting cell differentiation and anabolism in musculoskeletal disease environments to enhance regenerative effects.
Mitigating Effects of Inflammation, Acidic pH, Hypoxia, Low Nutrition, and Hyperosmolarity on Cell Therapies in the Musculoskeletal Disease Environment
Inflammation
It is well known that DD and OA have a major inflammatory component and are not just degeneration caused by overuse.23,24 There are multiple inflammatory cytokines known to be involved in these pathologies such as TNF-α, IL-1α, IL-1β, IL-2, IL-4, IL-6, IL-8, IL-12, IL-17, and interferon-γ.24–32 Therefore, when cells are delivered to these environments, they are exposed to these cytokines and the negative consequences they cause. These consequences include cell signaling that can induce apoptosis, and therefore directly affect cell survival. 33
Signaling of these cytokines can also induce the expression of enzymes that degrade tissues such as matrix metalloproteinases (MMPs) or aggrecanases, which causes delivered cells to participate in degrading the tissue they are trying to regenerate.23,24 In addition, these cytokines can inhibit chondrogenic differentiation of the delivered stem cells causing the inhibition of stem cells adapting to their delivered environments. 34 With all this in mind, there is a need to prepare cells before they are delivered to these environments to allow them to tackle the obstacles presented by inflammatory cytokines.
Cell therapies: inflammation
There are several approaches that have been designed to aid stem cell therapies within the inflammatory conditions of musculoskeletal disease environments. These include the delivery of anti-inflammatory proteins/molecules with stem cells, genetic modification of stem cells, the introduction of biomaterials, and physical methods (Table 1).
Cell Therapies: Inflammation
ACLT, anterior cruciate ligament transection; ADSC, adipose-derived stem cell; BM-MSC, bone marrow mesenchymal stem cells; BMP, bone morphogenetic protein; DAD, diallyl disulfide; dECM, decellularized extracellular matrix; ECM, extracellular matrix; GAG, glycosaminoglycan; HA, hyaluronic acid; iPSC, induced pluripotent stem cell; LPS, lipopolysaccharide; LV, lentivirus; MMP, matrix metalloproteinase; NPSC, nucleus pulposus stem cell; OA, osteoarthritis; OARSI, Osteoarthritis Research Society International; PRP, platelet-rich plasma; TGF, transforming growth factor; UC-MSC, umbilical cord MSC; WJMSC, Wharton jelly MSCs; XG, xanthan gum.
Proteins are not typically delivered directly with cells as they have a short in vivo half-life, which limits their application. As a result, there were only two studies found to use proteins. One used a cocktail of proteins termed platelet-rich plasma (PRP) within a canine OA model where injections of adipose-derived stem cells (ADSCs) with or without PRP were given weekly for a month. 35 The results demonstrated improved matrix content and mechanical properties of treated tissue and decreased inflammation and cell death when PRP was codelivered with ADSCs. In addition, an in vitro study investigated the approach of preculturing stem cells with growth factor IGF-1 to enhance their anabolic activity in an OA cell culture model. 36 This approach demonstrated an ability to decrease proteolytic enzymes and RANKL expression, resulting in an overall reduction in matrix-degrading properties under inflammation.
Overall, these approaches demonstrated positive outcomes although the second described study with IGF-1 preculture may be a more clinically feasible approach, as it could be applied relatively easily during the manufacturing process of preparing stem cells for clinical treatment and does not modify the process in the clinic. Whereas studies with PRP-ADSC codelivery indicated a need for multiple injections to demonstrate positive outcomes thereby complicating the clinical treatment process.
As proteins have a short in vivo half-life and are relatively expensive to manufacture, the use of more accessible anti-inflammatory small molecules is more commonly studied. These molecules are either modulators of specific pathways37–40 or have broad anti-inflammatory effects41–49 and have demonstrated an ability to modulate inflammatory signaling in models of musculoskeletal disease environments (Table 1).
Treatment of stem cells with pathway-specific modulators, JAK and TAK1 inhibitors, 39 or PPAR-δ agonist, 37 improved chondrogenesis under treatment with OA synovial fluid. Treatment of stem cells with the JNK inhibitor decreased apoptosis under TNF-α treatment. 38 A study using an MAPK inhibitor took the approach of preculturing the stem cells with this inflammatory pathway modulator instead of treating them during differentiation. 40 This approach worked well with the MAPK inhibitor, demonstrating improved chondrogenesis under IL-1β treatment making it a useful approach in improving stem cell preparation for implantation.
General anti-inflammatory molecule treatment of stem cells under inflammatory conditions has demonstrated the improvement of differentiation, tissue formation, and inhibition of inflammation-mediated pathways. Treatment of stem cells with kartogenin, an RUNX1 transcriptional activator, in coculture with human OA explant tissue improved tissue morphology and decreased MMP-13 expression. 43 Treatment of stem cells with a number of other anti-inflammatory small molecules decreases oxidative stress (melatonin and diallyl disulfide),41,42,47 inflammatory signaling (honokiol, diallyl disulfide, and curcumin),44,47,48 apoptosis (melatonin, honokiol, and curcumin),41,42,44,48 and proteolytic enzyme expression (melatonin, honokiol, and glucosamine)41,44,49 and improves differentiation under treatment with IL-1β in vitro (melatonin, honokiol, kaempferol, diallyl disulfide, curcumin, and glucosamine).41,42,44,45,47–49
Treatment of stem cells stimulated with lipopolysaccharide in vitro with the flavonoid kaempferol demonstrates an ability to decrease apoptosis and IL-6 expression, while improving IL-10 and chondrogenic marker expression. 45 In an in vivo rat model of OA, codelivery of a polysaccharide, xanthan gum, with stem cells improved tissue morphology and decreased inflammatory cytokines within synovial fluid. 46 While these studies have demonstrated positive outcomes, they have the drawback of using molecules that still degrade relatively quickly in vivo, which make long-term benefits without repeated administration questionable. While repeated injection to the knee is not concerning aside for the hassle of repeated visits to the clinic, it is of concern for IVD therapeutics, as the simple act of injections into the IVD can potentially be harmful to tissue structure. 50
To overcome this issue of therapeutic molecule degradation in vivo resulting in a need for multiple injections, gene engineering/delivery methods are utilized to improve anti-inflammatory properties of stem cells so that delivered cells may more continually decrease the negative effects of surrounding inflammation on them.
Several studies have worked on antagonizing TNF-α and IL-1β signaling by gene delivery of IL-1RA or TNF-α antagonists Atsttrin or sTNFR1.51–56 These have been expressed under both constitutive and inducible promoters, and both have shown an ability to improve differentiation,51–53,56 decrease inflammatory signaling,51,53,55 and decrease matrix degradation52–56 under inflammation. However, inducible promoters can have the added benefit of only being activated when needed and not continue expression after tissue repair has been done. Alternatively, TNF-α and IL-1β have also been antagonized by CRISPR-based downregulation of expression of their receptors TNFR1 and IL-1R1 and shown similar positive effects.57,58 The added benefit of this method is that it is specific to regulating TNF-α and IL-1β signaling only in the modified cells, rather than all surrounding cells if desired. In addition, this preserves TNFR2 signaling, which has been shown to have protective effects itself.59,60
Other studies have also focused on increasing anti-inflammatory gene expression and/or decreasing inflammatory gene expression. In vitro, it has been demonstrated that overexpression of IL-37 by stem cells improves chondrogenic differentiation and decreases proteolytic enzyme and inflammatory cytokine expression under IL-1β- or OA-conditioned media treatment. 61 In vivo delivery of IGF-1 overexpressing and COX-2 and aggrecanase-1 silenced stem cells in a monkey OA model improved tissue morphology and decreased IL-1 and PGE2 in synovial fluid. 62
In vivo delivery of IL-10 overexpressing stem cells into a mouse OA model was not as successful, with no improvement in OA score, although there was a reduction of activated T cells. 63 Overall, these gene engineering approaches allow for a more prolonged effect of anti-inflammatory proteins on cell therapies under inflammatory conditions of the musculoskeletal disease environments. However, given that they use viral-based gene delivery, they are not without safety concerns, such as immunogenecity, insertional mutagenesis, and potential for oncogene activation.64,65 An option for overcoming this concern would be the use of nonviral gene delivery approaches. Nonviral gene delivery has historically had low delivery efficacy; however, in recent years, there have been strides made in this field that have increased the efficacy of nonviral gene delivery, 66 improving the likelihood that it may be an effective delivery option moving forward.
Other methods studied to decrease the effect of inflammation on stem cells include the use of biomaterials or physical treatments. Biomaterials utilized include a BMP-7 self-assembling peptide or hyaluronic acid with optimized molecular weight.67,68 The BMP-7 peptide was able to decrease apoptosis while improving extracellular matrix (ECM) expression under TNF-α treatment in vitro. 67 Culture of stem cells in 1.6 MDa hyaluronic acid hydrogel in the presence of immune cells increased M2 macrophage activation and IL-10 expression showing activation of an anti-inflammatory immune cell phenotype rather than an inflammatory one. 68 While neither biomaterial was studied in vivo, the results with these biomaterials demonstrate they have the potential to improve the impact of delivered cells.
In addition, these biomaterial-based approaches can be potentially combined with the cell modifying strategies explored here. Physical methods that have been studied include photobiomodulation and electromagnetic fields (EMFs).69,70 In a rat model of OA, photobiomodulation performed daily for 7 days after cell delivery resulted in improved cell survival, collagen II, TIMP, and IL-10 expression, and decreased inflammatory gene and MMP expression. 52 Testing of EMFs was done in vitro and demonstrated an ability to improve differentiation under IL-1β treatment. 53 The feasibility of these physical treatments clinically is questionable as they require continuous/daily exposure to the treatment, and their effectiveness in large tissues may be inhibited due to a need to penetrate over longer distances. Nonetheless, these could be useful for engineering tissue to be implanted rather than cell therapies.
Overall, tackling the negative effects of inflammation on cells within musculoskeletal disease environments is the most investigated of the harsh disease environment conditions. Many of these studies have shown promising findings and demonstrated that cells can be engineered for their disease environment. However, there is more work to be done as many methods, especially more long-term gene engineering/delivery-based methods, have not been tested in vivo yet. Continued work needs to be done to understand the long-term implications of these modifications in terms of efficacy and safety in vivo.
Hypoxia and low-nutrient conditions
The cartilage and IVD environment are hypoxic due to the avascular nature of the tissues with oxygen tension ranging from 1% to 5% in IVD71,72 and 1% to 10% in cartilage. 22 In addition, this avascularity results in these tissues being low-nutrient environments.22,73 Hypoxia and low-nutrient environments by themselves can have some positive effects on stem cells, as it has been demonstrated that hypoxia aids in stem cell differentiation into disc- and cartilage-like cells,73,74 and low-nutrient conditions can improve stem cell proliferation and metabolism.19,73
However, musculoskeletal disease environments have both hypoxia and low-nutrient conditions. This has negative effects on stem cells as it has been shown that hypoxia, in combination with serum deprivation or low-glucose conditions, results in stem cell death and decreased matrix production.75–78 Overall, methods looking to improve stem cell health in hypoxic and low-nutrient conditions must understand both the individual effects of these conditions and their combined effects.
Cell therapies: hypoxia and low-nutrient conditions
Research looking to improve stem cell survival and anabolism in the low-oxygen and low-nutrient environments of musculoskeletal tissues is limited, with only a handful of studies, and all are in vitro (Table 2). Within these studies, a variety of approaches have been taken.
Cell Therapies: Hypoxia and Low-Nutrient Conditions
One study involved preconditioning the cells before differentiation under hypoxic, low-nutrient conditions by preculturing them under hypoxic conditions with or without transforming growth factor (TGF)β3. 79 It was demonstrated that hypoxic preculture without TGFβ3 best-promoted cell survival in hypoxic, low-nutrient pellet culture. Similarly, another study performed hypoxic cell expansion before differentiation under hypoxia in a gelatin hydrogel and demonstrated improved differentiation with hypoxic expansion. 80
Two studies utilized biomaterials to improve outcomes in a hypoxic, low-nutrient environment. One compared culture in alginate versus chitosan hydrogels and demonstrated that alginate better supports cell survival and glycosaminoglycan (GAG) and collagen II deposition. 81 The other study compared alginate versus alginate/collagen hydrogels and demonstrated that alginate/collagen hydrogels better support cell survival and collagen deposition. 82
Another approach taken was preselection of clonal populations. 83 This study demonstrated that compared with heterogenic stem cell populations, certain clonal populations have improved GAG deposition and cell survival under hypoxic, low-nutrient conditions. Finally, one study performed gene delivery of antiapoptotic protein BCL-2 to stem cells by lentivirus. 84 This study indicated improved viability and higher aggrecan/collagen II indicating a more nucleus pulposus (NP) cell-like phenotype, although the experiments were done under hypoxia and not hypoxia combined with low-nutrient conditions. Therefore, it is unknown if this approach would be useful in a more clinically relevant environment.
Overall, these studies show promise in addressing the problem of cell death caused by hypoxic and low-nutrient conditions. Strategies range from a simple hypoxic preculture protocol, biomaterial selection, phenotype control through cell selection, or altering cell phenotype via gene delivery. The preconditioning methodology is relatively simple to apply as it is an adjustment to culture conditions rather than implantation conditions. This is in contrast to biomaterial use that requires additional design of how to incorporate the material into cell implantation strategy, and gene engineering with viral delivery that adds additional safety concerns.64,65
Nonetheless, it is still of interest to further test all of these methodologies as the previously described studies are preliminary in vitro work and no in vivo studies have been performed to further demonstrate their efficacy. If further studies demonstrate the extension of the longevity of cells in vivo, the clinical benefit of cell therapies may be improved with these methods even if there are hurdles to their clinical application.
Acidity
A factor considered one of the biggest hurdles to cell survival in these musculoskeletal environments is acidity. These environments are acidic due to the anaerobic glycolysis occurring within these avascular tissues, which builds up lactic acid. Within healthy cartilage or disc tissue, the pH falls within a neutral range of 6.9–7.2.85,86 When these tissues become degenerated and damaged, the pH drops, especially in the IVD, to values as low as 6.2.87,88 This has shown to be problematic for the survival of stem cells, in experiments where they were cultured within acidic environments mimicking diseased IVD tissue.89,90
Native cells of the IVD and cartilage are naturally able to better tolerate these acidic conditions and this is believed to be due to their expression of specific acid-sensing ion channels (ASICs).73,91 It is known that ASIC1a is proapoptotic under acidic conditions and that ASIC3 promotes survival under acidic conditions.92,93 MSCs and IVD vary in their expression of ASICs, with MSCs having a higher ratio of ASIC1a to ASIC3, and therefore, the specific ASIC signature of IVD cells could be what gives them better ability to survive in acidic environments.94,95 ASIC3 and ASIC1a are also known to play similar roles in the degeneration and protection of cartilage. 91 While methods to address the cell's response to acidic environments are critical for developing effective cell-based therapies, limited work has been conducted in this space.
Cell therapies: acidic environment
Only two studies were found to have investigated methods of improving stem cell survival under acidic conditions, and both are in vitro (Table 3). One study investigated the use of the diuretic amiloride and demonstrated that it can decrease apoptosis, while increasing proliferation and chondrogenic marker expression at pH values as low at 6.2 in NP-derived stem cells. 96 The other study compared stem cells from two different sources, NP tissue and bone marrow. 97 This comparison demonstrated that NP stem cells had better viability, proliferation, and anabolic gene expression under acidic conditions.
Cell Therapies: Acidic Environment
ADMSC, adipose tissue-derived mesenchymal stem cell; NP, nucleus pulposus.
These studies demonstrate that it is possible to alter cell response to low pH environments and that certain cell types have improved native capacity to handle these environments. Future work will need to investigate these outcomes in vivo and understand what is driving these changes so they can be better harnessed for cell therapy. It is also of interest to test whether adjustment of cells, ASIC expression signature, could allow cells derived from non-IVD tissue to survive in acidic environments as this was not tested in either of the described studies but has been indicated as an important factor in basic research.91,94,95 Furthermore, knowledge of cell adaption to acidic environments is still currently limited, as shown by the limited number of studies, and thus, more basic research is needed to further elucidate survival mechanisms under acidity to optimize approaches of improving cell survival and anabolism in these environments.
Hypertonicity
IVD and cartilage are hyperosmotic tissues, mainly due to the high concentration of proteoglycans in these tissues.98,99 These conditions have been shown to have negative effects on stem cell viability and adaptation. It has been shown that the survival and matrix production of stem cells are inhibited by hyperosmotic environments mimicking these tissues.89,90 In terms of adaptation, it has been shown that these conditions can also negatively affect chondrogenesis of these stem cells. 89 Interestingly, there have been contrasting results demonstrating improved chondrogenesis under hyperosmotic conditions in specific contexts.100–102 This indicates osmolarity is a complex environmental factor whose effects rely on coexisting environmental factors. Nonetheless, the direct effects of hyperosmolarity on the viability of stem cells are negative, indicating a need to address this issue for improving cell therapies.
To our knowledge, there are no studies directly investigating the problem of hypertonicity. Rather, studies have focused more on improving differentiation of stem cells into more native-like cells under pathological musculoskeletal conditions so that the issue of hypertonicity is tackled in tandem with other microenvironmental challenges in musculoskeletal disease environments. These studies are discussed in the following section.
Regulating Cell Differentiation and Regenerative Effects in Musculoskeletal Disease Environments
As a way to tackle all of the challenges listed above, there is a significant body of work investigating how to improve the induction of differentiation of cells into native phenotypes within musculoskeletal disease environments. This is a useful technique because, as previously mentioned, the cell therapies that typically work best are those using cells with native or close to native phenotypes.13,103 Therefore, several methods have been investigated for their ability to promote differentiation in musculoskeletal disease environments. These approaches include preconditioning protocols, gene delivery of differentiation-inducing factors, and biomaterials, as discussed below.
Preconditioning
Preconditioning protocols aim to provide a feasible protocol for cell preparation before implantation that enhances their differentiation and regenerative capability within harsher in vivo environments. There are several studies in this area that have tested different preconditioning protocols, both in vitro and in vivo (Table 4). Two studies were in vitro with one investigating preculture with TGFβ3104 and the other investigating high- versus low-glucose media for cell expansion. 105 Preculture with TGFβ3 improved cell proliferation and collagen II and aggrecan expression in NP-like conditions (low glucose, 485 osmolality, 6.8 pH). Low glucose during expansion improves chondrogenic marker expression and GAG content during chondrogenic pellet cultures. The remainder of the studies identified are conducted in vivo and are in both DD and OA animal models.
Preconditioning Approaches for Promoting Differentiation in Osteoarthritis and Disc Degeneration Model Environments
ICRS, International Cartilage Regeneration and Joint Preservation Society; MRI, magnetic resonance imaging.
For the disc, two studies investigated the use of hypoxic preculture before cell implantation and demonstrated decreased loss of disc height, improved matrix protein expression, and improved cell survival.106,107 One study investigated mechanical loading in a hydrogel system with TGFβ1 present before cell implantation and demonstrated improved GAG deposition and SOX9 and collagen II expression. 108 In addition, selection of cells highly expressing TGFβ1 and TGFβ2 receptors before implantation demonstrated improved tissue morphology while increasing anabolic gene expression. 109 There has also been a preclinical study using preconditioned cells from the NP of human IVD tissue, called discogenic cells, with promising outcomes.110,111 These are cells extracted from NP tissue and expanded in a proprietary cocktail of supplements before insertion into degenerative IVD tissue. Preclinical studies demonstrated the ability of discogenic cells to significantly partially restore lost disc height and improve morphology compared with vehicle or sham controls while demonstrating these cells are safe too. These positive outcomes have led to a phase I/II clinical trial using these discogenic cells combined with a hyaluronic acid carrier for treatment of specific cases of lumbar DD (clinicaltrials.gov study identifier NCT03347708).
For OA models, two studies investigated preculture with growth factors before implantation, one using TGFβ1 and the other using TGFβ3 and BMP-6.112,113 Both demonstrated improved morphological/histological scores, and the one with TGFβ1 preculture demonstrated improved chondrogenic marker expression and cell survival. One study interestingly investigated preculture with inflammatory cytokines TNF-α and IFN-γ and demonstrated improved histopathology score and ECM expression, as well as decreased inflammatory cytokine expression. 114 The use of vitamin E preculture demonstrated improved cell survival, matrix content, and histological score. 115
Overall, there have been a variety of preconditioning approaches investigated with promising results. With strategies ranging from growth factor/cytokine treatment to cell selection to mechanical loading in preculture, there are many new exciting methods to be further tested preclinically and clinically to find the best options for each target treatment. In general, all of these approaches provide potentially feasible methods for improving cell therapies for treating DD or OA, but when it narrows down to what is clinically used, it will amount to which preconditioning processes are easiest to incorporate into manufacturing. In summary, preconditioning is currently the most progressed approach for improving in vivo therapeutic effects of delivered cell therapies for musculoskeletal disease, with one methodology (discogenic cells) already in clinical trials.
Gene-engineered stem cells
Another approach investigated to improve differentiation in vivo, is gene delivery of differentiation-inducing factors into stem cells before delivery (Table 5). This is done as a method to have growth factors provide more useful long-term effects on in vivo differentiation. In addition, having stem cells express these factors is also useful for stimulating anabolic effects on surrounding cells.
Gene Delivery Approaches for Promoting Differentiation in Osteoarthritis and Disc Degeneration Model Environments
Gene delivery of multiple growth factors has been done, including traditional growth factors such as TGFβ and bone morphogenetic proteins (BMPs) and also other lesser known factors. Although TGFβ is a potent in vitro differentiation factor, the use of TGFβ growth factor expressing stem cells is limited to one study, as it is known that the differentiation inducing capacity of TGFβ is inhibited by the inflammatory cytokines present in musculoskeletal disease environments.34,116 This study investigated in vivo delivery of TGFβ1 and TGFβ3 in a rat OA model and demonstrated some morphological improvements. 116
Delivery of a variety of BMPs has been performed as specific types of BMPs have been shown to be chondrogenic. 117 In models of OA, both BMP-9 and BMP-4 expressing stem cells have been delivered in vivo with positive effects on cartilage morphology.118–120 Delivery of BMP-4 expressing cells was done in both mice and rat models of OA and was codelivered with cells expressing a VEGF inhibitor sFlt1.119,120 This was because it has been demonstrated that angiogenesis can inhibit chondrogenesis, and indeed, it was demonstrated that codelivery of sFlt1 expressing cells provided the best results. Delivery of BMP-7 expressing cells has been performed for DD models as BMP-7 exerts chondrogenic effects and is known to stimulate anabolic effects in disc cells too.121,122 These studies demonstrated improved morphology and tissue content measured months after delivery in rodent and rabbit DD models, indicating potential longer term effects with this approach.121,122
Other lesser known factors have also been utilized that induce desired musculoskeletal phenotypes. Overexpression of NELL-1 has been utilized to improve repair of osteochondral defects as NELL-1 is known to induce stem cells down an osteochondral lineage. 123 Overexpression of GDF-5 has been investigated for use in ex vivo disc repair in degeneration-induced bovine disc as GDF-5 is known to induce a more NP-like phenotype in stem cells. 124 Overexpression of Wnt11 has been performed to induce a chondrogenic phenotype in stem cells as it is known to stimulate collagen II accumulation. 125 The use of these types of factors helps better assure native phenotypes. As we learn more about the developmental biology of these tissues, these factors and others may become more commonplace in differentiation protocols as well as potential protocols for cell therapy engineering/preculture.
Aside from the use of differentiation signaling growth factors, some studies have induced differentiation through overexpression of SOX transcription factors in stem cells, which are known to be heavily involved in chondrogenesis.126,127 Although SOX9 is known as the main chondrogenic transcription factor, in vivo delivery of cells has involved cells overexpressing both SOX9 and SOX6, as SOX6 enhances SOX9 activity. 128 One of the two studies, referenced in Table 5, uses ANGPTL4 shRNA along with SOX6 and SOX9 overexpression, as ANGPT4 has been shown to be higher in OA chondrocytes and induces MMP expression within them and stem cells. 127 Therefore, this approach may be more powerful as it is also counteracting negative genes associated with OA.
In summary, gene engineering stem cells have provided methods that allow cells to endogenously produce differentiation enhancing proteins or reduce differentiation inhibiting ones. With flexibility of which genes to regulate expression, especially with CRISPR gene regulation tools that allow for endogenous gene activation and repression,129,130 there is a high potential for what can be achieved with this technique. Although there are safety considerations to consider, especially as genes are typically virally introduced, as shown in Table 5. Nonetheless, there are several clinical trials using ex vivo virally gene-engineered cells for other indications.131,132 Thus, this yields the possibility for the use of these gene-engineered stem cells for musculoskeletal indications clinically. In addition, there is ongoing research into providing more efficient nonviral gene delivery approaches that potentially have higher safety profiles. 66
Overall, no matter which gene engineering approach is taken, to continue moving gene-engineered cell therapies forward, there needs to be preclinical and clinical work focusing on safety outcome measurements to ensure that not only can these treatments be more efficient but also that they are safe.
Biomaterial-based differentiation
Biomaterials have long been a focus of promoting and maintaining cell phenotype. These biomaterial-based approaches can enhance in vivo differentiation by creating a stable microenvironment to support differentiation and cell survival. To focus this section on biomaterial-driven differentiation, no studies including the addition of growth factors are discussed here. There are three main categories of biomaterials utilized to induce differentiation, synthetic, natural, and mixed biomaterials (Table 6).
Biomaterial-Based Approaches for Promoting Differentiation in Osteoarthritis and Disc Degeneration Model Environments
Synthetic materials are relatively easy to manufacture with greater reproducibility than natural biomaterials. All studies referenced use synthetic materials, and use polymer-based biomaterials to successfully improve differentiation and therefore regeneration within in vitro degenerative disc culture models, and a rabbit OA model.133–137 Although all are polymers, important differences between them are their mechanical properties, with each material tailored to their specific application in the disc or the knee. Importantly, mechanical properties, including matrix elasticity itself, have demonstrated to provide a strong signaling cue for cell differentiation, 138 and therefore, the mechanical properties of biomaterials used are of primary consideration in promoting cell survival and function in diseased musculoskeletal environments.
Natural materials provide enhanced potential to induce differentiation, as they contain signaling cues that drive biological function in the process of differentiation. Two studies in IVD used the prominent ECM protein type I collagen. One study using type I collagen microspheres to encapsulate cells demonstrated the benefit of reduced osteophyte formation, an important problem to consider with cell therapies. 139 The other study utilized atelocollagen and demonstrated improved tissue composition, although no comparison was made to a control treatment that included stem cells. 138 To provide a scaffold closer to native tissue, one study in the disc utilized a crosslinked type II collagen and chondroitin sulfate composite biomaterial, which is appropriate as the disc is rich in type II collagen and GAGs. 140 This study did demonstrate improvement in tissue composition and structure compared with stem cells without biomaterial in a rat needle puncture model.
Other studies referenced utilize decellularized ECM, which provides and maintains several signaling cues beneficial to cell differentiation, function, and survival. Two studies listed utilized decellularized ECM synthesized by target tissue cells in the laboratory,141,142 while one study utilized decellularized tissue from human cartilage. 143 Overall, natural materials have the highly beneficial property of best mimicking the native tissue, but as they are biologically derived, their properties are harder to control, and they are more expensive to manufacture. Therefore, factors of efficacy along with manufacturing difficulty must be considered when deciding whether to go with a natural or synthetic biomaterial for application in cell therapies.
While natural and synthetic materials have their own described specific benefits, they may not always have the desired properties on their own, but can be combined to produce such desired properties. One study did this using hyaluronan-poly(N-isopropylacrylamide) to support disc-like differentiation. 144 This material is designed to be a hydrogel that contains a chief component of the disc, hyaluronan, and is also thermoreversible so it is injectable. This study did examine the effects of preculturing in this hydrogel with GDF-5 containing media before implanting the cells into a bovine IVD explant culture. It was demonstrated that results were slightly better without the preconditioning protocol indicating it can be delivered immediately after mixing with cells and have desired effects, yet there is still much work to do with this material as it has not been tested in vivo.
Overall, a variety of approaches utilizing biomaterials are being tested to provide methods of enhancing differentiation without the need for added growth factors to improve the chances of in vivo differentiation and survival. As can be noted, most references in this field are within the last 5 years. Thus, there is still much work to be done in comparing them and incorporating them with other methods discussed in this review.
Conclusions
While several cell therapies for OA and DD are being evaluated in the clinic with some success,13,14,18 more work is needed to understand the effects of diseased musculoskeletal environments on the cells and to identify methods to mitigate deleterious outcomes. Presented in this review are examples of research focusing on improving stem cell survival and anabolism in musculoskeletal disease environments to enhance their effects and longevity.
While the studies described were separate for OA and DD, it can be noted that a majority of the findings in these studies have the potential to be applicable to both pathologies, as inflammation, pH, low nutrition, and hypoxia are present in both conditions.19–22 The exceptions fall in some studies utilizing various methods to induce stem cell differentiation as the desired ECM production profile of cells differs between IVD and knee. 145 Therefore, differentiation inducing protocols found to be beneficial may not be appropriate for both OA and DD cell therapy, and applicability should be evalulated on a case by case basis.
In addition, the approaches discussed specifically modulate inflammation, pH, low-nutrition, and hypoxia outcomes or improve differentiation and anabolism under musculoskeletal disease conditions individually. However, it is important to note that the cells are generally exposed to all these environmental cues simultaneously. Modeling such complex environments in vitro is challenging, and animal models do not exactly mimic the human conditions, especially for DD, 146 therefore making testing of candidate cell therapies challenging and efficacy nebulous before clinical evaluation.
Furthermore, clinical evaluation tools, which include self-reported assessments, may be variable. 147 In addition, radiographic evaluations performed on a range of different machines, including X-ray and magnetic resonance imaging (MRI), are not without limitations, which hinder their ability to detect meaningful changes in disc structure. For example, X-ray can only detect disc height and not changes in hydration, 148 and while MRI can detect changes in hydration, its dynamic range is limited. 149 As a result, clinical evaluation tools must evolve to allow for visualization of clinical changes that are statistically different from control to more properly assess efficacy of cell therapies.
Nonetheless, moving forward, it will be advantageous to understand how each of these microenvironmental cues in the IVD and knee interact with one another, and if they can all be mitigated simultaneously to identify better cell therapy candidates for musculoskeletal diseases. There are many interesting approaches discussed here that may be used singularly or together as the field builds on its understanding of the effects of each microenvironmental cue. For example, it would be interesting to combine discussed biomaterial approaches with gene engineering approaches. There are many potential strategies to explore, and the field continues to investigate them in vitro and in vivo as they move these approaches closer toward clinical application.
Footnotes
Disclosure Statement
R.D.B. and N.F. have no competing financial interests. L.S. is an employee and stock option holder of DiscGenics.
Funding Information
No funding was received for this study.