
Abstract
The aim of the study is to provide an up-to-date review of studies that used preclinical animal models for the evaluation of tissue engineering treatments for spinal cord injury (SCI), which involved the use of biomaterials with or without the addition of cells or biomolecules. Electronic search of the PubMed, Web of Science, and Embase databases was performed for relevant studies published between January 2009 and December 2019. In total, 1579 articles were retrieved, of which 58 studies were included for analysis. Among the included studies, rats were the most common species used for animal models of SCI, while complete transection was the most commonly used injury pattern. Immediate intervention after injury was conducted in the majority of studies, and 8 weeks was the most common final time point of outcome assessment. A wide range of natural and synthetic biomaterials with different morphologies were used as a part of tissue engineering treatments for SCI, including scaffolds, hydrogels, and particles. Experimental parameters in studies using SCI animal models to evaluate tissue engineering treatments should be carefully considered to match the purpose of the study. Biomaterials that have functional modifications or are applied in combination with cells and biomolecules can be effective in creating a permissive environment for SCI repair in preclinical animal models.
Impact statement
This review provides an up-to-date summary of the preclinical landscape where tissue engineering treatments involving biomaterials were tested in animal models of spinal cord injury (SCI). Using studies published within the last 10 years, novel perspectives were presented on the animal species used, injury pattern, timing of intervention and outcome measurement, and biomaterials selection, as well as a summary of the individual findings of each study. This review provides unique insight into biomaterials-based tissue engineering strategies that have progressed to testing in animal models of SCI, which will help shape future research in the field and propel the clinical translation of discoveries.
Introduction
Spinal cord injury (SCI), most often caused by traffic accidents, is one of the most serious diseases of the central nervous system (CNS), leading to devastating neurological deficits and disabilities in the patient. The incidence of SCI is estimated to be between 10.4 and 83 cases per million people per year. 1 Less than 1% of SCI patients can achieve complete recovery of neurological function, with most cases resulting in partial or complete paralysis, and the cost of lifetime care for each SCI patient is in the range of 0.7–3 million USD. 2 SCI therefore imposes a significant socioeconomic burden, particularly since the majority of patients are <30 years at the time of injury. 3 The management of SCI patients is challenging, since the loss of sensory, motor, and autonomic functions distal to the point of injury often leads to multiple health problems, including recurrent kidney stones, urinary tract infection, pressure sores, and cardiac and respiratory dysfunction, 4 as well as major impacts on quality of life due to complications such as neuropathic pain, 5 spasticity, 6 heterotopic ossification, 7 and syringomyelia. 8
Current clinical approaches for treating SCI include early surgical decompression, drugs, and cell therapy. Early surgical decompression has been found to have positive effects on improving behavioral and pathological outcomes in preclinical SCI models. 9 However, it is difficult to achieve satisfactory clinical outcomes, and there is little consensus regarding the role and timing of decompression in SCI. 10 Anti-inflammatory drugs, such as a high dose of methylprednisolone, can be administered for acute SCI to reduce swelling and secondary injury. 11 However, the common methods for drug delivery such as intraperitoneal injection using a syringe or intrathecal infusion using an osmotic minipump can lead to scar formation and infection, 12 and tissue penetration by the drug is also limited by the blood–spinal cord barrier. 13 Cell therapy, such as stem cells, Schwann cells, or olfactory ensheathing cells (OECs), have been used for reducing secondary injury and boosting axonal and neuronal regeneration after SCI. Nevertheless, these therapies are associated with risks of immunological rejection, tumorigenicity, low survival rate of transplanted cells, and potential dangers in genetic manipulation of the host tissue. 14 The current clinical treatments are not ideal for the safe and effective restoration of neural function after SCI. After swelling from the injury subsides, the patient begins a long period of rehabilitation, which may allow some lost spinal function to be compensated by the remaining nerve fibers.
Tissue engineering approaches have been recently explored as new therapeutic strategies for the treatment of SCI. Tissue engineering has been used across many applications in tissue regeneration to construct biological substitutes that can replace, restore, or enhance tissue function. 15 For SCI, tissue engineering strategies such as cell delivery using a biomaterial system have been shown to preserve spared neural tissue and bridge the injury site with local tissue. 16 In this review, tissue engineering is defined as the insertion of biocompatible or functional scaffolds at the injury site that may or may not be combined with living cells, biomolecules, or other therapeutic agents. Current tissue engineering strategies aiming to achieve functional recovery in SCI are focused on reproducing the native architecture of the extracellular matrix (ECM) surrounding the injury site,17,18 and tuning the differentiation of transplanted cells to re-establish communication through new neural relay circuits. 19 The overall aim is to create a permissive environment for the interactions among cells, scaffolds, and bioactive molecules that can limit inflammation and promote the restoration of sensory and motor functions. 20
The safety and feasibility of using bioresorbable polymer scaffolds for the clinical treatment of SCI have been reported in a small number of patients.21,22 These studies have shown some evidence of functional recovery, as reflected through the results of magnetic resonance imaging, neuronal electrophysiology, and scores for sensory, motor, and autonomic neural functions. However, due to the limited sample size, it was not possible to obtain reliable, high-quality evidence from follow-up. In addition, retrieving spinal cord specimens from patients to observe pathological changes is ethically prohibited. Therefore, animal models with disease etiology that have a degree of similarity to humans are being widely used in preclinical studies to assess tissue engineering strategies for treating SCI. A holistic view of the current findings in animal models will help shape future research directions in the field and propel the clinical translation of discoveries.
The use of animal models for the preclinical assessment of tissue engineering strategies for SCI treatment has been reviewed in selected studies.4,23,24 However, the last comprehensive review on this topic was published >15 years ago. More recent reviews have not specifically focused on tissue engineering strategies, or focused on specific aspects within tissue engineering. They have also mainly focused on the effects of animal species selection and the injury pattern, but other important parameters such as the timing of intervention and outcome assessment, and experimental variables such as biomaterials selection have not been addressed. Biomaterials selection can play an important role in the outcome of SCI repair. Collagen, 25 chitosan, 26 and polyethylene glycol (PEG)27,28 are some of the most commonly chosen biomaterials, but their effects on treating SCI may differ depending on the animal species, injury pattern, timing of intervention, among other variables. In this systematic review, we provide an up-to-date analysis of studies involving animal models to assess SCI treatment using biomaterials-based tissue engineering approaches, and report on the trends observed in the selection of animal species, injury pattern, and timing of intervention and outcome assessment.
Materials and Methods
Literature search strategy
A comprehensive systematic search was conducted in PubMed, Web of Science, and Embase for studies published in the last 10 years (between January 1, 2009 and December 31, 2019), on using tissue engineering approaches to treat SCI that involved animal models. The following search terms were used: “spinal cord injury” AND “animal model” AND (“polymer” OR “hydrogel” OR “biomaterial” OR “scaffold” OR “tissue engineering”). Specific search strategies used for each database have been included in the Supplementary Data.
Study selection
The records of retrieved studies were imported into Endnote. After the removal of duplicate records, two reviewers independently screened all studies for inclusion in this systematic review. Any disagreement was adjudicated by a third reviewer. The inclusion criteria were as follows: (1) studies focused on the treatment of SCI; (2) studies that used a tissue engineering approach involving biomaterial(s); (3) studies that used an animal model; and (4) studies published in English. The exclusion criteria were as follows: (1) nonoriginal studies, such as reviews, editorials, and opinion pieces; (2) absence of essential information, including the injury pattern, timing of intervention and outcome assessment, and type of intervention used; (3) conference abstracts and studies where the full text was unavailable.
Data extraction
For each included study, two reviewers independently extracted all relevant information for the review: (1) study characteristics (authors, journal, year of publication); (2) study design (animal species, injury pattern, timing of intervention and outcome assessment, type of intervention used); (3) outcomes and findings.
Results
The search strategy identified 1579 potential studies. After the removal of duplicate records, 1400 studies were screened by title and abstract, through which 769 unrelated studies, 368 reviews, and 130 studies on other aspects of tissue engineering were excluded. The full text of 133 articles was screened according to the inclusion and exclusion criteria, which gave rise to 62 eligible studies. Four of these were excluded for using an uncommon injury model and presenting unclear outcomes, respectively. Finally, 58 articles were included for analysis in this systematic review. The study selection process is depicted in Figure 1, and a summary of the included studies is presented in Table 1.
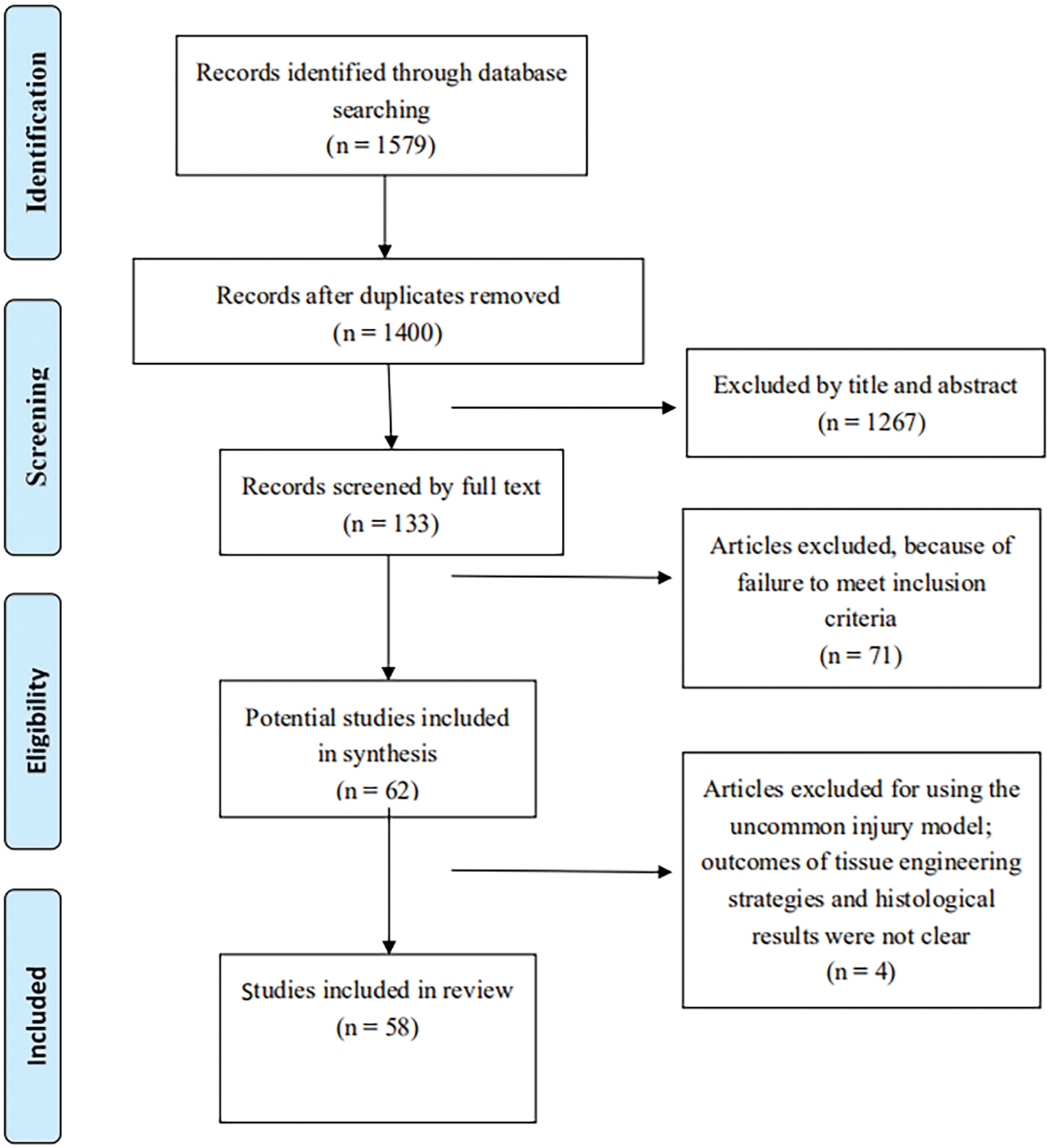
Flow diagram for the study selection process. Color images are available online.
Summary of Included Studies on Testing Tissue Engineering Strategies in Animal Models of Spinal Cord Injury
aFGF, acidic fibroblast growth factor; BDNF, brain-derived neurotrophic factor; bFGF, basic fibroblast growth factor; BMHP1, bone marrow homing peptide; BMSC, bone marrow stromal cells; ChABC, chondroitinase ABC; CNTF, ciliary neurotrophic factor; DTX, docetaxel; EGF, epidermal growth factor; EGFR, epidermal growth factor receptor; EnSC, endometrial-derived stromal cells; ESNPC, embryonic stem cell-derived neural progenitor cell; FHPS, fragmented physical hydrogel suspension; HA, hyaluronic acid; HEMA-MOETACL, hydroxyl ethyl methacrylate [2-(methacryloyloxy)ethyl] trimethylammonium chloride; HP, heparin-poloxamer; IKVAV-PA, IKVAV-functionalized peptide amphiphile; iPSC, induced pluripotent stem cell; MSC, mesenchymal stem cell; NPC, neural progenitor cells; NSC, neural stem cell; NT-3, neurotrophin-3; OEC, olfactory ensheathing cell; PDGF, platelet-derived growth factor; PEG, polyethylene glycol; PLGA, poly (lactic-co-glycolic acid); PLL, poly-L-lysine; PNIPAAm, poly(N-isopropylacrylamide); PGS, poly(glycerol sebacate).
Animal species
SCI animal models for evaluating tissue engineering treatments included rat (77.4%), mouse (6.5%), dog (7.8%), nonhuman primate (3.2%), pig (1.9%), and other rodents (guinea pig and rabbit, 3.2%). Rodents were the most common species used. Larger animals such as dogs and pigs, and nonhuman primates, which have the greatest resemblance to humans, are gradually being adopted in preclinical experiments of SCI treatment. The advantages and disadvantages of each species are shown in Figure 2.
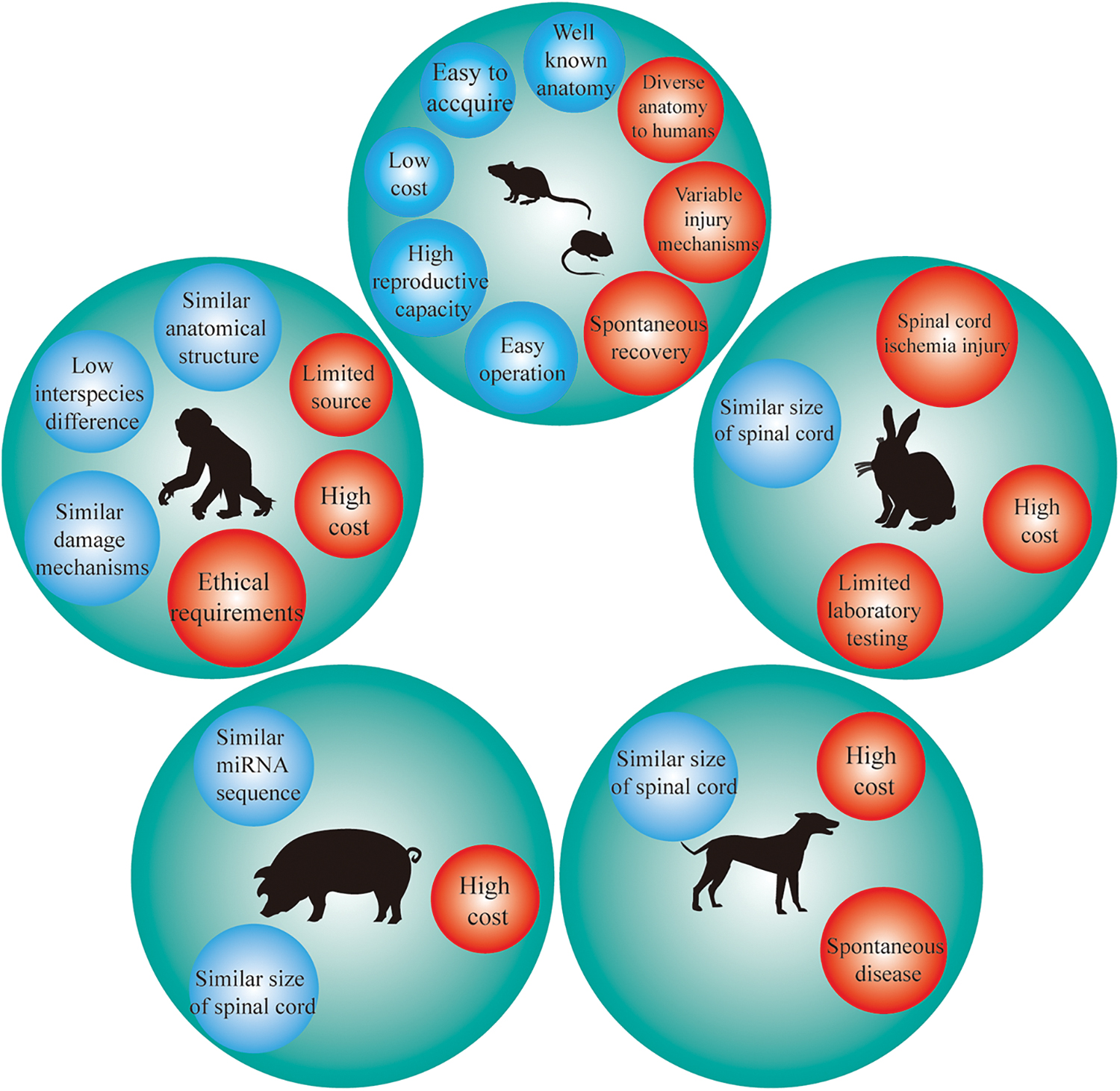
Advantages (blue) and disadvantages (red) of common SCI animal models used to evaluate tissue engineering treatments. SCI, spinal cord injury. Color images are available online.
Injury pattern
Transection and contusion (or compression) injuries were induced in SCI animal models used to evaluate tissue engineering treatments, as shown in Figure 3. For transection models, the biomaterial can be transplanted directly into the injury site, while contusion models have an intact dural structure and the biomaterial can be injected to fill the gaps. The most common injury pattern was complete transection (42.4%), followed by hemisection (33.9%). Contusion models (23.7%) were often used to test soluble or microparticle scaffolds.
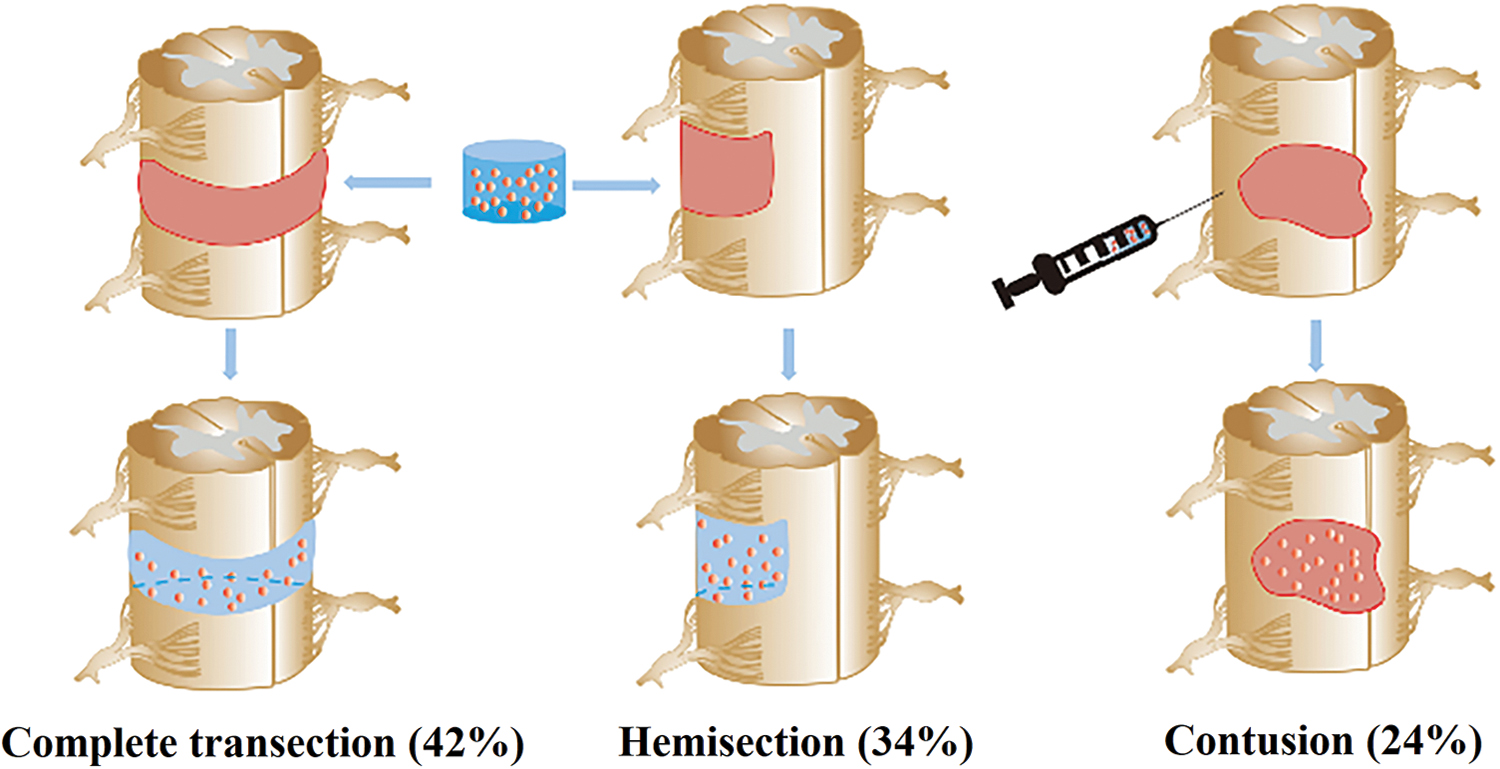
Common injury patterns in SCI animal models used to evaluate tissue engineering treatments. Color images are available online.
Timing of intervention and outcome assessment
For the timing of intervention (Fig. 4A), the biomaterial was immediately implanted into the host after SCI in the majority of studies (74.1%). Implantation at 1–2 weeks after injury (19.1%), together with other shorter times of intervention, was adopted in the remaining studies. For the timing of outcome assessment (Fig. 4B), 8 weeks was most commonly chosen as the final time point, followed by comparable numbers of studies that chose 4 and 12 weeks. In addition, studies involving small (Fig. 4C) and large (Fig. 4D) animals differed in the most common final time point chosen for outcome assessment. The majority of small animal studies were terminated at 8 weeks, while longer time points were generally chosen for large animal studies.
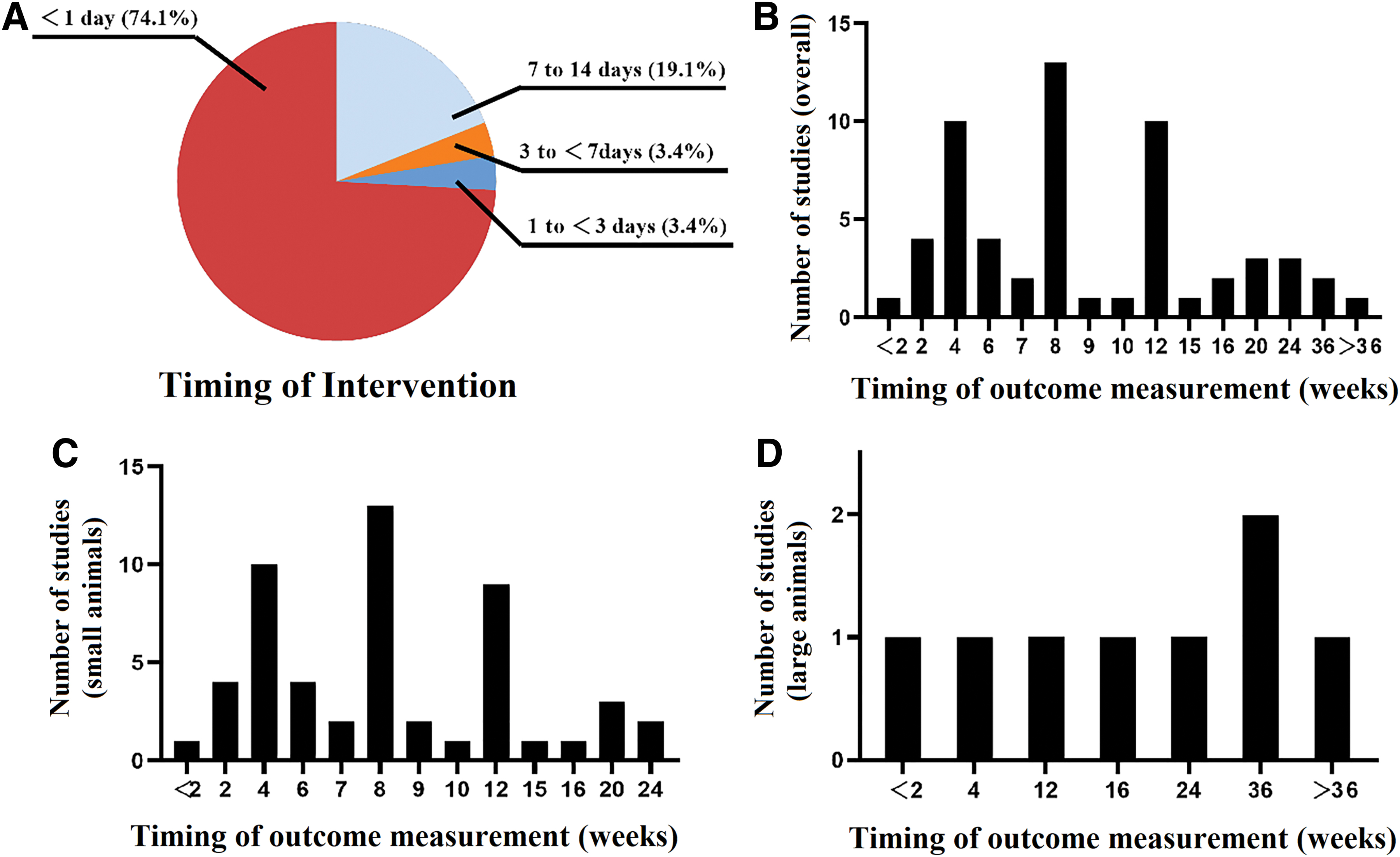
The timing of
Biomaterials selection
A wide range of biomaterials were used as a part of tissue engineering approaches to treat SCI in animal models, including both natural and synthetic polymers. The studies could be broadly classified by the composition of the biomaterials-based intervention: biomaterials alone, biomaterials with cells, biomaterials with drugs, or biomaterials with a combination of additional factors (Table 1). Collagen and chitosan were the most commonly used natural biomaterials, while poly lactic-co-glycolic acid (PLGA) and PEG were the most commonly used synthetic materials. In most studies, the biomaterials were either implanted into the injury site as scaffolds or hydrogels, or injected in the form of particles, solutions, or hydrogels. The majority of studies loaded cells and/or bioactive molecules into the biomaterial(s) before implantation.
Discussion
The complicated pathophysiology of SCI poses significant barriers to functional recovery, and the pace of advances in therapeutic interventions has been slow for many years. Rapid progress in tissue engineering over the last two decades has opened up the potential for new therapeutic strategies, which have already demonstrated some promising results in animal models of SCI. From the included studies, it is apparent that tissue engineering strategies consisting of a biomaterial coupled with the delivery of permissive cell types and growth factors could promote repair in SCI. Nevertheless, full recovery has been rarely achieved in animal models, and the treatment effects may be related to a variety of factors in the study design. Our review of studies published over the last 10 years, on the assessment of tissue engineering strategies to treat SCI in animal models, has indicated that the rat is the most commonly used species, and complete spinal cord transection is the most commonly adopted injury pattern. The tissue engineering construct is usually implanted immediately after injury, and 8 weeks is the most frequently used final time point for outcome assessment. A wide variety of natural and synthetic polymers have been used in the form of scaffolds, hydrogels, or other forms for implantation. Gaining an understanding of the preclinical landscape for treating SCI using tissue engineering is important in the planning of future studies, and for ultimately translating the application of these therapeutic strategies to humans.
Selection of animal species
Our study showed that rats were the most commonly used species for evaluating tissue engineering treatments of SCI. Rats have the beneficial characteristics of low cost, abundance source, ease of care and operation, well-understood anatomy, and ability to test a range of injury patterns. Most types of SCI encountered in humans can be replicated in adult rats, and several established behavioral tests are available to assess the loss and recovery of sensory and motor functions.29,30 Pathological changes in rats due to SCI have partial similarity to humans. For instance, the early formation of fibrotic tissue at the core of the lesion site in rats and humans is typically associated with a breach of the three meninges, allowing fibroblasts to invade the injury site. 31 Rats also often develop large cystic cavities at the site of injury, a pathological feature that is seen in human SCI. 24 Some methods of SCI treatment analogous to human therapy are well established in rats, such as neuroprotective drugs and autologous cell transplantation. For example, the efficacy of riluzole in functional recovery and inhibition of damage extension, 32 and the effect of autologous OEC transplantation in increasing axonal growth across the injury site and promoting recovery of neural circuits 33 have been confirmed in rat SCI models. However, whether the results of tissue engineering treatments in rats can be extrapolated to human SCI still needs further exploration, 34 for several reasons. First, the efficacy of interventions in rats is overpredicted by their high rate of spontaneous recovery, 35 which is rarely seen in humans. Second, the design of the tissue engineering construct, including the size, elasticity, and morphology of the biomaterial implant, depends greatly on the structure of the spinal cord, 36 which is vastly different between rats and humans. Third, the evaluation of functional recovery may be influenced by the different functions of key spinal tracts between rats and humans. For instance, the corticospinal tract is thought to be critical for fine motor control in humans and nonhuman primates, but less so in rats. 37
It is important to assess the substantial risk of moving tissue engineering treatments to human clinical trials from rodents without testing in an intermediate large animal model, such as dog, pig, or nonhuman primate. The spinal cord anatomy and physiology of these larger animals have a greater degree of similarity to humans compared with rodents, particularly in the position and function of the spinal tracts. 35 The spinal circuitry of nonhuman primates has a high degree of similarity to humans, and the activation of motor-related circuitry depends more on supraspinal input than in nonprimates. 37 Other animal models may provide species-specific benefits compared with rats, such as an adequate arterial blood supply to the spinal cord in rabbits, 38 and similar mRNA sequence in pigs compared with humans. 39 Large animal models of SCI may therefore allow a more physiologically relevant evaluation of outcomes but are limited by higher cost and more stringent ethical requirements, particularly for large vertebrates and nonhuman primates. We believe that the use of large animals in SCI research should only be considered when models in less developed species are inadequate for addressing important mechanistic or translational questions.
Selection of injury pattern
Transection (complete or partial) is the most commonly adopted injury pattern in animal models of SCI to test the effects of tissue engineering treatments, even though the pathology of this model is far from human SCI and causes higher complications and mortality rate compared with other models. 40 This is in large part due to the convenience of this model in providing space for easy implantation of biomaterials and evidence of repair. Complete transection results in no sparing of axons or neural tissue in the lesion site, which is useful for demonstrating genuine axonal regeneration 41 and neuroplasticity 42 when evaluating the effects of exogenous interventions. However, completely severed spinal cord stumps may form new circuits, particularly in animals where there is a high ability for spontaneous healing, leading to difficulties in evaluating the true efficacy of implanted biomaterials. 43 For instance, self-regenerative neural circuits formed at the stumps after complete transection may play a functional role in initial locomotor improvement, independent of the biomaterial. 44 Complete transection is also associated with a risk of retraction of the rostral and caudal stumps, which may cause unexpected damage if no other treatments were used to bridge the gap. 45 As an alternative, partial transection or hemisection can be used to evaluate tissue engineering implants. These injury patterns lead to less severe functional deficits compared with complete transection, and can help avoid excessive animal loss. 46 Nevertheless, secondary injury may be associated with hemisection, which has detrimental effects on the contralateral spinal cord around the surgery site, such as the appearance of postoperative edema and severance of midline blood vessels.
Contusion or compression, while being the least commonly used injury pattern in SCI animal models, allows for minimally invasive implantation and is useful for injecting biomaterials in the form of particles or solutions.47–49 The main advantage of this injury model is that the integrity of the spinal dura mater is preserved, avoiding the need for bigger surgical incision. 46 This leads to a low fatality rate, low cost, and easy handling. However, the precision of contusion injury is difficult to maintain, 50 and the presence of uninjured nerve fibers and axons in the injury site may allow compensatory proliferation and establishment of new neural connections, making it difficult to accurately evaluate neural regeneration. 51
Selection of timing of intervention
In a clinical setting, the progression of SCI should ideally be controlled during the acute or subacute phase of injury. 52 However, immediate or early intervention is difficult, and largely depends on the availability of medical services, patient condition, and complexity of complications. Nevertheless, we found that the majority of studies testing tissue engineering treatments in SCI animal models implanted the biomaterial immediately after spinal operation. While this is not necessarily reflective of the clinical reality, immediate intervention has the advantage of minimizing differences in individual responses to injury, particularly for small animals. A small number of studies conducted intervention within a few hours or days after injury, which may better mimic the clinical situation, but also introduces additional risks as a second injury is performed soon after the first one.53,54 During acute injury, the trauma site is dominated by inflammation and cell necrosis. Previous studies in murine models indicated that homologous neural grafts and dissociated cell grafts survive poorly in acute lesion sites.55,56 A biomaterial implant is beneficial in offering immediate protection to grafted cells and nutrients from inflammatory mediators and reactive oxygen species during acute injury. For instance, neural stem cells transplanted within a scaffold were found to survive in all grafted animals in a rat complete transection model, and completely filled the scaffold channels 1 month after injury. 28 However, cells transplanted without a scaffold showed poor survival and invariably failed to fill the gaps at the injury site.
A substantial portion of studies have evaluated the effects of delayed intervention during the subacute phase of injury (1–2 weeks after the initial injury). From a clinical standpoint, the pathology of the lesion has stabilized to some extent at this stage, and the lesion site may have a more permissive environment for supporting regeneration. In a rat model, delaying hydrogel implantation to 1 week after SCI led to greater anatomical improvements than immediate implantation, as evidenced by a greater decrease in cavity volume. 57 Other studies in rats suggested that SCI might be better stabilized at 2 weeks after injury, based on the injury size and glial scar formation. 58 The transplantation of fetal spinal cord tissue with neurotrophins also improved axonal growth and functional recovery to a greater extent at 2 weeks compared with when applied acutely. 59 The benefits associated with delayed intervention in tissue engineering studies are possibly due to avoiding the impact of environmental fluctuations and influx of inflammatory cells in the acute phase, which are thought to negatively affect the bioactivity of implanted biomaterials. 58
Selection of timing of outcome assessment
The timing of outcome assessment for different animal models of SCI needs to be adjusted according to their time course of pathological changes and potential for spontaneous recovery. The majority of included studies used 8 weeks as the final time point, which was largely tailored for the rat model. Studies conducted using larger SCI models such as dogs and nonhuman primates reported proportionally longer observation times typically extending beyond 12 weeks. For the rat model, histopathological changes typically stabilize and plateau at 8 weeks after injury, 60 and the size of the lesion epicenter also remains constant during this time. 61 In addition, 8 weeks usually allows the test group to show significant increases in the repair of neural circuits, density of fibrous tissues, and infiltration of host cells compared with the control.12,62 It is also a suitable time point for assessing behavioral improvements,42,63 where motor function has been reported to increase gradually in rats within 8 weeks, after which functional scores tend to stabilize. 64
The need to have longer observation times for large animal models of SCI is related to the increasing complexity of their CNS compared with small animals, and the greater similarity of their neural circuitry as well as injury and repair processes is compared with humans. The vertebrate motor system has undergone pronounced evolutionary changes that have resulted in significant variations between rodents and nonhuman primates. 37 One example is the motor cortex and the corticospinal tract as its descending output, which are highly similar between humans and nonhuman primates but less so in rodents. In higher vertebrates including humans, which have a complex and sophisticated CNS, it becomes more difficult to recover neural function after injury compared with smaller animals. For this reason, the time frame for recovery in large animal models of SCI is generally longer than that in rodents. Some large animal models of SCI have been used as parallel groups alongside human patients to verify their clinical relevance. For example, a canine model of complete SCI at 3 months after injury was thought to be comparable with American Spinal Injury Association (ASIA)-A patients (complete loss of motor and sensory function) at 12 months, and dogs with some retention of motor function were thought to be fit models for intervention efficacy in human ASIA-C patients (incomplete loss of function below the lesion). 65 A study that tested a combination of materials and stem cell therapy saw significant improvements in motor function in a canine complete SCI model at 3 months postsurgery, and it was speculated that a similar recovery pattern might be applicable to humans. 41 When choosing an SCI model to test for the clinical relevance of interventions, the timing of outcome assessment should be considered together with the animal species.
It is worth noting that the included studies typically used a series of time points for behavioral and histological assessments, although we only included the final time point in our analysis. Behavioral assessments were usually performed weekly or at even shorter time periods, while the time points of histological assessments were carefully selected to cover the major phases of change after SCI (acute, subacute, and chronic). In rodents, the transition between acute and subacute phases often occurs within a few hours to 1 day postinjury (DPI), while 7 DPI is considered the point of transition to the chronic phase. In one study, a lesion core of dense fibrotic tissue was observed to form at 7 DPI, which maintained a constant morphology and showed no major changes after this time. 61 The transition between phases in SCI can also be identified through sequential phenotypic changes in astrocytes (naïve, reactive, and scar forming) at corresponding time points. 66
Selection of biomaterials
A wide range of biomaterials have been applied as a part of tissue engineering treatments in SCI animal models. The choice of biomaterial was influenced by the animal species and injury pattern in the majority of studies, which could impose limitations on the morphology of the biomaterial. For instance, scaffolds with pores, channels, or bundles of fibers were often used for transection injuries, while particles and solutions were typically used for contusion injuries. Hydrogels were used for all injury types. Although none of the studies specifically compared the effects of different scaffold morphologies, it is expected that these would impart some effects on repair outcomes, for instance between collagen bundles 67 and linear ordered scaffolds, 68 and between PLGA nanoparticles 53 and channeled scaffolds. 69
Synthetic polymers including PLGA and PEG were frequently chosen for SCI, which have the advantages of allowing versatile surface modification, mechanical tuning, and chemical functionalization. All of these properties are useful in producing constructs that can protect transplanted cells from intrinsic secondary injury in SCI, while promoting their attachment, proliferation, and differentiation. 70 Synthetic polymers can also be modified with ECM components, such as collagen, laminin, or synthetic peptides, which can help generate a permissive microenvironment for recovery. 18 Some synthetic materials, such as peptide amphiphile hydrogels, can undergo self-assembly, and are useful for binding and releasing growth factors and other bioactive substances.71,72 Natural polymers such as collagen, chitosan, alginate, and hyaluronic acid have structures that mimic native ECM, which can help maintain the normal function of host cells without introducing cytotoxic effects. 70 They often contain sites for cell adhesion and can intrinsically promote cellular infiltration. However, due to their natural origin, batch-to-batch variation is an issue for these materials, and their applications in SCI repair may be further limited by weak mechanical properties and a high degradation rate in vivo.
It should be mentioned that the focus of the included studies was on comparing the effects of loading cells, biomolecules, and/or bioactive motifs in the biomaterials to unmodified or partially modified biomaterials. Systematic studies using well-established SCI animal models will need to be performed in the future to compare the effects of different biomaterial morphologies or compositions to advance tissue engineering solutions toward applications in the clinical treatment of SCI. A few selected biomaterials that have proceeded beyond preclinical testing to being used in clinical trials for treating complete SCI patients are presented in Table 2.
Biomaterials That Have Been Tested in Clinical Trials for Spinal Cord Injury Repair
SCI, spinal cord injury.
The most common form of treating clinical cases of SCI using biomaterials is to remove the damaged spinal cord and replace it with the biomaterial, with or without the combination of cells. The biomaterials selected for testing in clinical studies to date have been confirmed to have low antigenicity, suitable mechanical strength, and biodegradability, as well as significant therapeutic effects in SCI animal models. A scaffold that has currently undergone the most testing in clinical studies is NeuroRegen, a collagen scaffold made from bovine aponeurosis. This scaffold has an ordered collagen filament structure to provide nerve guidance, as well as sufficient space for cell adhesion and growth without causing significant immune responses. 73 When combined with cells, either autologous bone marrow mononuclear cells (BMMCs) or allogeneic mesenchymal stem cells, the NeuroRegen scaffold achieved a significant recovery effect in patients with acute or chronic SCI.21,74 In two acute SCI patients, sensory functions began to recover at 2 months postsurgery, and one patient showed the ability to raise their lower legs against gravity when sitting on a wheelchair at 6 months. 74 In five chronic SCI patients, the erection reflex was improved in two cases at 2 months postsurgery, and the recovery of somatosensory-evoked potentials was detected in the lower limbs of two cases at 6 months. 21 Although these positive results have only been demonstrated in a very limited number of patients, the use of biomaterials to achieve clinical repair of SCI shows significant promise. It is anticipated that the testing of new biomaterials using physiologically relevant animal models of SCI will expedite the process of clinical translation.
Animal models of SCI can help achieve rigorous evaluation of biomaterials before they are considered for use in clinical treatment. Although a wide range of biomaterials are being developed with improved physical and chemical properties for SCI repair, many issues can surface during preclinical testing relating to the complexity of preparation, ease of handling, biocompatibility, biodegradability, and ability to integrate with the host tissue. For instance, some biomaterials may be nonbiodegradable, while others may lack good biocompatibility to neuronal cells or induce an immune response after implantation. 75 While scaffolds with an oriented inner structure may be beneficial for guiding axonal regrowth, these scaffolds are typically stiffer and may not integrate well with the host spinal cord, sometimes requiring a surgical opening to be made, which increases the invasiveness of the implantation process. 46 On the contrary, injectable scaffolds are soft and can conform to the injury site to integrate with host tissue, but cannot be used to achieve targeted neural growth. 72 A balanced consideration of such factors, based on the information derived from testing in preclinical SCI models, is essential for advancing new biomaterials to clinical studies.
Perspectives and outlook
A satisfactory treatment of SCI to this day remains a significant challenge, with most cases resulting in irreversible damage to neurological functions. Although a small number of tissue engineering strategies involving biomaterials have been tested in clinical trials for SCI repair, these have failed to achieve the desired prognosis despite early improvements. For example, the implantation of NeuroRegen scaffolds together with autologous BMMCs was found to recover or improve sensory and autonomic nervous function in some SCI patients, such as defecation sensation, physiological erection, sweating, and superficial or deep sensations. 76 However, no motor function recovery was observed in this 3-year clinical study. A good explanation is still lacking for these findings. The difficulty of producing long-term improvements using tissue engineering or other strategies is possibly related to the complex progression of SCI after the initial injury. SCI proceeds according to a sustained injury cascade, which can be divided into several phases: acute (<48 h), subacute (48 h to 14 days), intermediate (14 days to 6 months), and chronic (>6 months). 77 During the acute phase, injury processes including cell death, blood vessel injury, expression of proinflammatory cytokines, and infiltration of inflammatory cells can trigger secondary injury. 78 This leads to the subacute phase, where ischemia and excitotoxicity result in ongoing necrosis of neurons and glia, as well as the release of excessive harmful factors that contribute to a loss of ionic homeostasis. 79 Finally, cystic cavitation and glial scar formation occur when the injury has entered the intermediate–chronic phase. It is due to this cascade of dynamic changes extending to several months after SCI that an inhibitory microenvironment is formed at the injury site or even systemically, creating significant difficulties for repair processes by limiting nerve regeneration. The rational use of animal models can help overcome the hurdles of studying SCI progression in humans and evaluating the efficacy of possible treatment strategies, for several reasons. First, animal models provide a convenient and repeatable means of observing and studying injury processes in SCI under artificially designed and controlled experimental conditions. Second, the ideal animal model can mimic human SCI anatomically and functionally, which can help researchers understand the pathophysiology of SCI and be used for preclinical validation of new therapies. For instance, large animal models such as dogs and nonhuman primates have an injury response similar to that observed in human SCI.37,65 Third, animal models allow further investigations into the mechanisms of healing after SCI treatment, which cannot be performed in humans. Using spinal cord specimens harvested from animals that have undergone SCI treatment, a range of outcomes can be evaluated, including the morphology of tissue, expression of inflammatory factors, and condition of nerve fiber regeneration.
There are some limitations in our analysis. First, we were not able to perform a meta-analysis on the included studies. The purpose of our study was to observe the selection of animal species, injury model, timing of intervention and outcome measurement, and biomaterials in preclinical studies of SCI involving biomaterials-based tissue engineering treatments. Among the included studies, there lacked a systematic reporting process for these selection parameters, leading to huge variations in study design and significant difficulties in performing quality assessment of studies. The quality of preclinical studies could be improved by well-designed author submission checklists and analogous journal initiatives, 80 such as the Stroke journal's Basic Science Checklist. 81 However, such checklists are currently field specific, and similar standards are not established in preclinical studies of SCI. It would hence be challenging to conduct an accurate meta-analysis for the included studies due to greatly variable sample numbers and surgical methods. Another significant challenge arises from the nonstandardized evaluation of “effective” repair in SCI animal models. For example, some studies used histological staining to observe the morphology of the spinal cord or neurons as the primary outcome, such as hematoxylin and eosin, Nissl, and Luxol fast blue staining.63,72 Meanwhile, other studies have used functional outcome measures, such as the Basso–Beattie–Bresnahan locomotor rating scale and swimming test. 75 Still others have chosen neuroelectrophysiology 67 or imaging examination 82 to observe spinal cord recovery in animals. These substantial variations limit the ability to conduct meta-analyses, since evaluation and interpretation of the results from animal studies of SCI need to be made in the context of the types of tests performed and relevance of the model to human pathophysiology. To enable more comprehensive analyses to be performed in the future, such as Bayesian meta-analysis, 83 the quality of preclinical SCI studies needs to be improved by standardizing the consideration of study design elements, such as randomization, blinding, sample size estimation, and sex bias.
Second, among the included studies on SCI repair in animal models, neural regeneration has been used as a primary indicator for outcomes measurement. However, other important factors may contribute to injury repair that have not been explicitly evaluated in these studies. For instance, white matter injury is a potential cause of function loss after SCI. 84 Some studies suggest that white matter recovery is closely correlated with functional restoration of paralyzed hind limbs, and may hold the key to motor recovery. 85 Interestingly, some studies have shown locomotor recovery in rodents despite not having any corticospinal fibers pass through the lesion area, 14 implying that other tracts may have played an important role. Indeed, it has been confirmed by electrophysiological evaluation that 10–25% of rubrospinal tracts were linked to the rat model, 67 which may provide additional mechanisms for locomotor recovery. Future studies may provide a better understanding of the role of white matter in the regulation and recovery of motor function in SCI by studying some of the less accessible tracts in animal models, such as the rubrospinal tract.
Conclusion
This review provides an up-to-date summary of the application of animal models in evaluating tissue engineering strategies for treating SCI. The animal species and injury pattern, as well as timing of intervention and outcome assessment, are all important parts of the experimental protocol for gaining a practical understanding of the effects of tissue engineering treatment. To maintain translational relevance, biomaterials selection should be carefully considered to be applicable both to the animal model and for future human use. Until more advanced screening technologies can be developed, preclinical animal models remain an essential step in the testing of tissue engineering products intended for the clinical treatment of SCI.
Footnotes
Authorship Confirmation Statement
All named authors have made substantial contributions to the conception of the review, and drafting and/or revising it critically for important intellectual content. They have approved the final version of the article, and agree to be accountable for all aspects of the submitted work.
Disclosure Statement
The authors have no competing interests to declare.
Funding Information
This study was supported by the National Natural Science Foundation of China (81802204), China Postdoctoral Science Foundation (2020M671453), Natural Science Foundation of Shanxi Province (201801D221117), Shanxi Medical University Second Affiliated Hospital Doctor's Funds (2017-105), Program for the Outstanding Innovative Teams of Higher Learning Institutions of Shanxi (2019L0410), and the Australian National Health and Medical Research Council (GNT1120249).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.