
Abstract
Background and Aims:
Antibodies to tumor necrosis factor alpha (TNF-α) have been successful in treating perianal fistulae in Crohn's disease, but current modes of delivery are limited. Microspheres are currently being assessed as scaffolds for tissue engineering and drug delivery devices. The aim of this study was to produce anti-TNF-α antibody–encapsulated microspheres using thermally induced phase separation (TIPS) and to characterize their behavior.
Methods:
Anti-TNF-α antibody was encapsulated into the microspheres (100 mg infliximab/g poly[lactide-co-glycolide] w/w) using a novel technique combining a vibration encapsulator unit with a TIPS process, using either lyophilized particulate antibody or an aqueous solution of antibody. Microspheres were incubated in phosphate-buffered saline for collection of supernatant and assessment of degradation. The amount and biological activity of the encapsulated antibody released from the microspheres was assessed by enzyme-linked immunosorbent assay and its ability to neutralize recombinant human (rh)TNF-α in vitro with a cytotoxicity assay. An in vitro wound scratch assay was used to assess the effect of released antibody on fibroblast migration. Ultrastructural characteristics of the different microspheres were characterized by scanning electron microscopy.
Results:
Highly porous microspheres released anti-TNF-α antibody under zero-order kinetics and inhibited the cytotoxic activity of rhTNF-α, producing a significant increase in cell viability compared with cells treated with rhTNF-α alone. This effect was most pronounced with microspheres fabricated by blending lyophilized particulate anti-TNF-α antibody into the polymer solution, which also significantly reduced the release of lactate dehydrogenase.
Summary and Conclusions:
Anti-TNF-α antibody encapsulated into highly porous microspheres was released in a controlled manner and exhibited biological activity against TNF-α. The technique used to produce TIPS microspheres is rapid and provides high encapsulation efficiency. This technique could also be applied to other therapeutic peptides where rapid fabrication and high yields are required.
Introduction
A range of anti-TNF-α antibody therapies is now available for the treatment of CD, including adalimumab (Humira®; Abbot Laboratories, Chicago, IL), certolizumab pegol (Cimzia®; UCB Pharma S.A, Smyrna, DE), and infliximab (Remicade®; Centocor, Horsham, United Kingdom). 3 Of these, as the first to reach the market, infliximab is currently the most widely used in the treatment of CD. It is a genetically engineered chimeric monoclonal immunoglobulin G (IgG) directed against soluble and transmembrane human TNF-α.
Systemic infliximab therapy is effective in the management of fistulizing CD. 4 However, long-term maintenance therapy (as opposed to episodic therapy) may be necessary to prevent fistula relapse. 5 Nevertheless, there are drawbacks to systemic infliximab treatment. Most notable of these is the immunosuppressant effect, which predisposes the patient to severe infection, but the development of antibodies to infliximab also poses major problems. These antibodies reduce the overall bioavailability and efficacy of infliximab and are strongly correlated also with infusion reactions. 6 Antibody formation can be diminished by a deliberate policy of regular maintenance therapy compared with episodic therapy. 7 However, infusions of infliximab are expensive and inconvenient, 8 and there are concerns that its prolonged systemic use may be associated with an increased risk of lymphoma 9 as well as the persisting risks of serious infection. 10 Because of the difficulties involved with the surgical and medical treatments of perianal fistulae in CD, biomaterials are currently being viewed with interest as alternative treatment modalities. 11 One of the more recent possibilities under consideration is the use of injectable biodegradable microspheres. 12 Although microspheres have not hitherto been used in the treatment of perianal fistulae, there are several reasons to anticipate advantages from this approach. Similar to the concept of fibrin glue, an injectable microsphere network should at least theoretically conform to the dimensions of a fistulae tract, unlike preformed scaffolds, such as the Surgisis® AFP™ Fistula Plug (Cook® Biotech, West Lafayette, IN) the first medical device for perianal fistula repair composed of collagen. The shape and rigidity of the plug is not suitable for all fistulae, especially complex fistulae that may have branched tracts and multiple openings. Further, insufficient porosity prevents rapid tissue infiltration and may explain why the Surgisis AFP Fistula Plug can be extruded from fistula tracts. Cellular infiltration within the voids of a microsphere network allows fibroblast proliferation, collagen deposition, and angiogenesis. 13 Degradation of microspheres allows further space for cell migration, matrix deposition, and tissue formation. A range of materials have been successfully used to develop biodegradable microspheres such as polysaccharides, 14 biodegradable polymers (e.g., poly[lactic-co-glycolic acid] [PLGA] and poly[lactic acid]), and collagen. 15 PLGA remains a popular material for implantable devices due to its established safety tolerance in humans as well as its widespread use in medical therapeutics. 16
The aim of the current study was to investigate the encapsulation and release of anti-TNF-α antibody from porous microspheres, which could be used as a novel method for the sustained local delivery of anti-TNF-α antibody into perianal fistulae.
Materials and Methods
Fabrication of PLGA microspheres
PLGA (75:25) (Purasorb PDLG 7507 0.63 dL = g IV; Purac Biomaterials, Gorinchem, The Netherlands) was selected for the current study due to its well-characterized properties in tissue engineering applications.13,17 Neat microspheres were prepared by dissolving the polymer in dimethyl carbonate (DMC; >99.9% purity; Sigma-Aldrich, Poole, United Kingdom) under magnetic stirring to produce a polymer weight–to–solvent volume ratio of 1:24 (w/v). Microspheres encapsulating lyophilized particulate infliximab were fabricated by dispersing 100 mg of infliximab powder into 1 mL of DMC and sonicating for 15 min in an ultrasonic bath (Decon FS100B; Decon Laboratories, Sussex, England). The infliximab/DMC dispersion was added to a 1:23 (w/v) solution of PLGA in DMC to produce a final weight–to–volume ratio of 1:24. Microspheres produced from an emulsion of polymer and aqueous solution of infliximab were fabricated by dissolving 100 mg of infliximab powder into 1 mL distilled water before adding to a 1:23 (w/v) solution of PLGA in DMC to produce a final weight–to–volume ratio of 1:24. A water-in-oil emulsion was created by homogenizing the solution for 3 min at 5000 rpm using a T8 Ultra-Turrax homogenizer (Ike-Werke, Staufen, Germany).
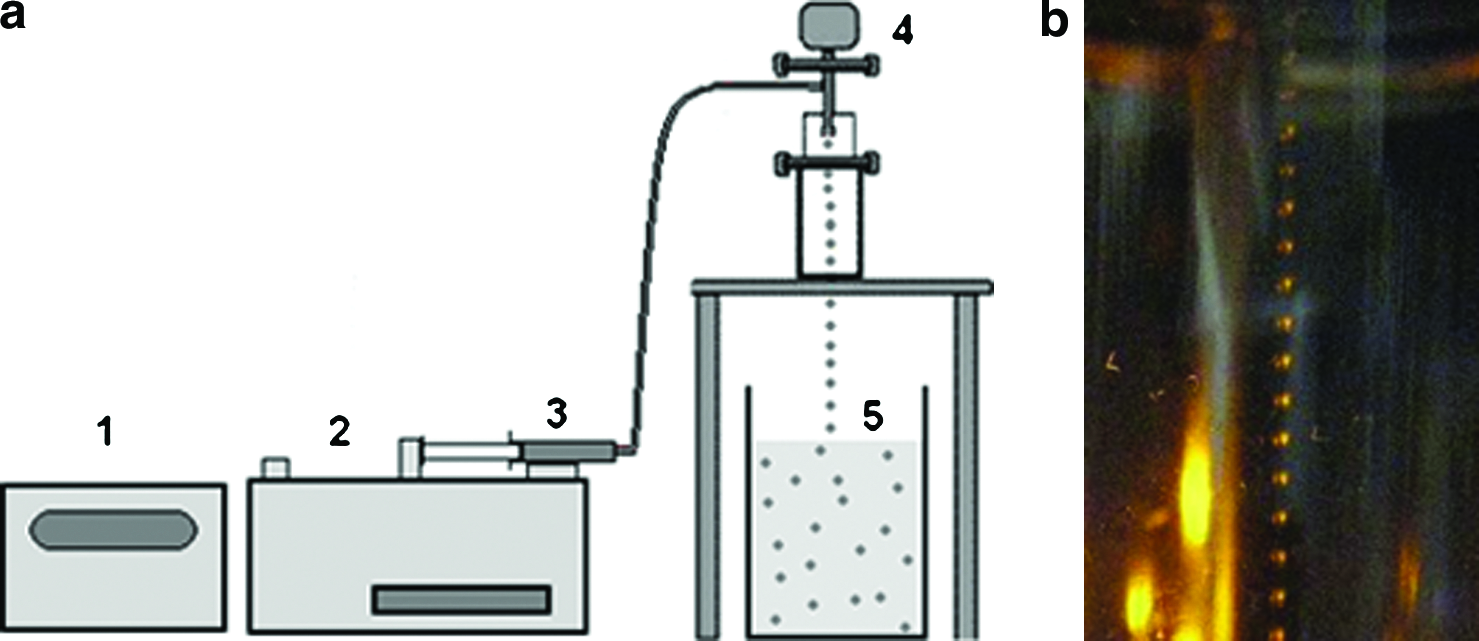
Microspheres were fabricated from the different polymer solutions using a Nisco encapsulator unit (Nisco Engineering, Zurich, Switzerland), fitted with a stainless steel sapphire-tipped nozzle with a 150 μm orifice (Fig. 1). Polymer solution was fed into the encapsulator unit by a syringe pump (Pump 11; Harvard Apparatus, Kent, United Kingdom), connected via a silicone tube, at a constant rate of 3 mL/min. A stroboscopic lamp was coupled to the vibrational frequency of the nozzle to facilitate observation of the falling droplets. The vibrational frequency of the nozzle was kept at 1.80 kHz and the amplitude of frequency 100%. A steady state of droplet formation was ensured, paying particular attention to avoid splitting of the droplet stream or coalescence of the droplets into a single stream (Fig. 1). Liquid polymer droplets were ejected into a polyethylene beaker containing 250 mL liquid nitrogen. The frozen droplets were allowed to equilibrate in the liquid nitrogen and transferred to a 50 mL Falcon™ tube (BD Biosciences, Franklin Lakes, NJ). Samples were freeze-dried using an Edwards MicroModulyo freeze dryer (Thermo Fisher Scientific, Asheville, NC) for 24 h to allow the sublimation of residual DMC solvent. The samples were sieved to produce microspheres with a size range of 150–710 μm.
(
In vitro assessment of the biological activity of the microspheres
Infliximab and neat microspheres were suspended in sterile phosphate-buffered saline (PBS; 50 mg/mL w/v) in microfuge tubes in replicates of five and incubated at 37°C and 5% CO2. Supernatants were collected after 24, 48, and 72 h incubation (stored at −80°C) and replaced with fresh PBS. The TNF-α neutralizing activity of the released antibody was determined by incubating a volume of supernatant from each type of microsphere with an equal volume of recombinant human (rh)TNF-α (2200 U/mL; R&D Systems, Oxfordshire, United Kingdom) for 90 min at 37°C. The combined rhTNF-α/supernatant solution (20 μL) was added to L929 fibroblasts (European Collection of Cell Cultures, Wiltshire, United Kingdom), seeded in a 96-well cell culture plate (Corning B.V. Life Sciences, Amsterdom, The Netherlands) at 2 × 104 cells per well in 80 μL of Dulbecco's modified Eagle's medium (DMEM) containing 2 mM glutamine, 10% fetal bovine serum (FBS), and 1 mg/mL actinomycin D. The culture was incubated for 24 h before measuring cell viability using the CellTiter 96® Aqueous Non-Radioactive Cell Proliferation Assay (Promega, Southampton, United Kingdom). The cytotoxic activity of rhTNF-α was determined using the CytoTox 96® Non-Radioactive Cytotoxicity Assay (Promega).
Encapsulation yield
The amount of infliximab encapsulated in the microspheres during fabrication was determined by dissolving 10 mg of microspheres containing particulate or emulsion infliximab in 500 μL of chloroform and adding 100 μL PBS. The solutions were vortexed and allowed to settle for 6 h. The infliximab-rich solution was collected for measurement by enzyme-linked immunosorbent assay (ELISA) of the amount of encapsulated infliximab.
ELISA for measuring infliximab release
An ELISA was used to measure the release of infliximab into the supernatants. The assay was performed as previously described. 18 Briefly, a 96-well plate (Nunc Maxisorp™; Thermo Fisher Scientific) was sensitized by incubating 100 μL of rhTNF-α (0.75 μg/mL in 1 M carbonate-bicarbonate buffer pH 9.6) overnight at 4°C. After washing the plates with wash buffer (PBS containing 0.05% Tween 20) the plates were blocked with 200 μL of PBS containing 1% bovine serum albumin for 2 h at room temperature. The plate was re-washed four times before adding 100 μL of standards or sample and incubated for 2 h at 37°C. The plate was then washed before adding 100 μL of peroxidase-conjugated goat anti-human IgG specific for Fc fragment (Sigma-Aldrich, Poole, United Kingdom) diluted 1:10,000 in 1% bovine serum albumin in PBS and incubating for 1 h at room temperature. After washing the plate 100 μL of o-phenylenediamine dihydrochloride solution (SigmaFASTTM OPD; Sigma-Aldrich, Poole, United Kingdom) was added to the plate and incubated in the dark for 20 min. The reaction was stopped by adding 50 μL of 2 M sulfuric acid, and the plate read at 450 nm with a correction wavelength of 630 nm. Data were plotted as the cumulative release of infliximab over 72 h.
Wound scratch assay
To assess the effects of collected supernatants on cell migration, a wound scratch assay was performed. L929 cells were seeded into 24-well plates at 2 × 105 cells per well in 1 mL DMEM containing 2 mM glutamine and 10% FBS, and incubated for 48 h until confluent. Wounds were created by scratching the monolayer with a 200 μL pipette tip between markers printed on a plate sealer (Sigma-Aldrich) applied to the base of the plate (Fig. 2). The monolayers were immediately washed with PBS before adding 250 μL of DMEM containing 2 mM glutamine and 10% FBS plus 25 μL of supernatant collected from the microspheres. The wounds were photographed at × 4 objective lens magnification, using an Axiovision microscope (Carl Zeiss, Munich, Germany) with an attached Nikon E950 digital camera, immediately after wounding (time point zero, t0) and after 8 h (t1) incubation at 37°C in 5% CO2. The area of cell migration into the wound area after 8 h (calibrated to mm2) was measured with image analysis software (ImageJ 1.41o; National Institutes of Health, Bethesda, MD), using the markers on the base of the plate as reference points (Fig. 2). The experiment was performed with five replicates for each type of microsphere, with each wound providing two wound margins for analysis.
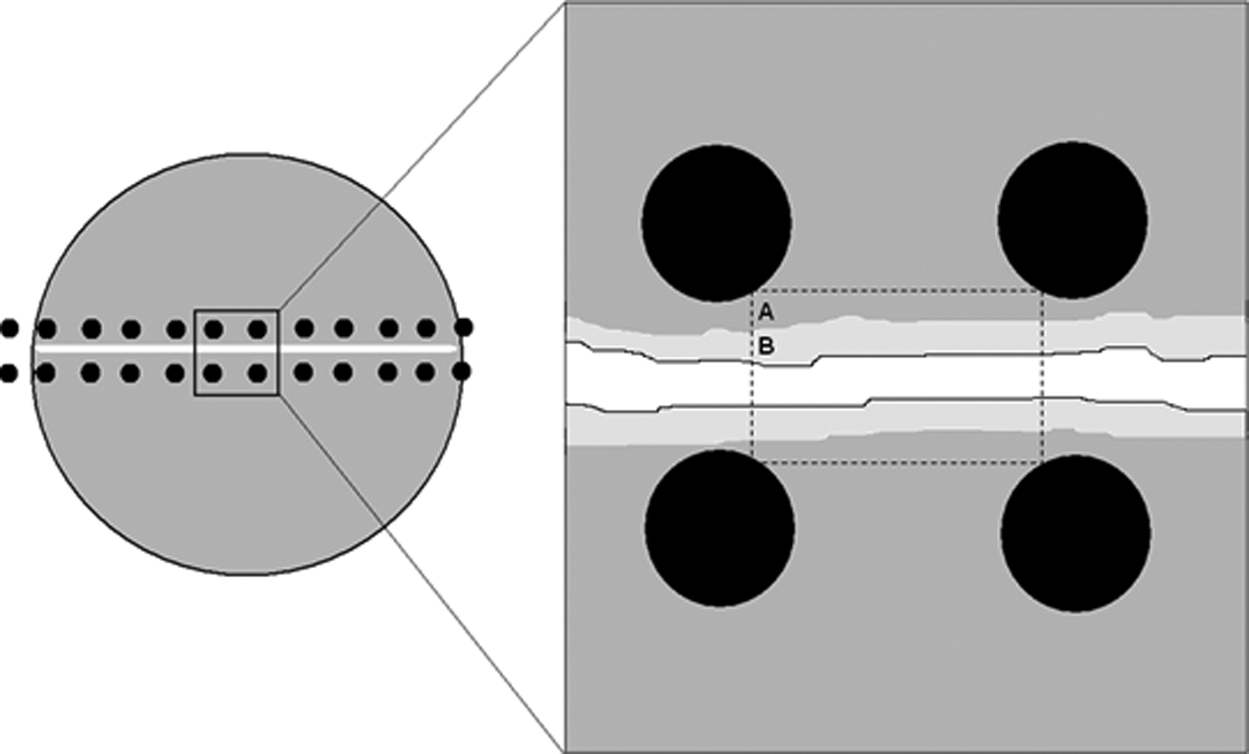
Schematic illustration of an individual well of a marked 24-well plate. The monolayer wound was made between the rows of markers that served as reference points. Image analysis of the wound area, consisting of the front of the cell line and bordered by dashed lines at t0 (A) and t1 (B) enabled measurement of the area of cell migration.
In vitro degradation of PLGA thermally induced phase separation microporous spheres
Aliquots of dry microspheres from each composition (W0) were immersed in PBS (50 mg/mL w/v) and degraded in vitro at 37°C for up to 7 weeks, in replicates of five. At weekly intervals, supernatant was collected from a sample of each type of microsphere for measurement of pH and storage at −80°C until analysis. The microspheres from these samples were dried in a vacuum oven (Gallenkamp model 8465F; Weiss Gallenkamp, Loughborough, United Kingdom) for a minimum of 2 weeks before changes to the size of the microspheres were measured from photomicrographs using image analysis software (Image-Pro Plus; Media Cybernatics, Bethesda, MD). A total of 10 microspheres were measured at each time point. Ultrastructural features of the microspheres were analyzed by scanning electron microscopy (SEM) either intact, or bisected using a double-edged razor blade. Samples were mounted onto aluminium stubs via adhesive carbon tabs and sputter coated with gold/palladium alloy for 10 min in an argon atmosphere before viewing by SEM (Jeol JSM 550LV Jeol, Tokyo, Japan, operated at 20 kV).
Statistical analysis
All data are expressed as mean ± SEM. Statistical analysis was performed using one-way analysis of variance with post hoc Bonferroni test, unpaired two-tailed t-test, and Pearson correlation using GraphPad Prism (GraphPad Software, San Diego, CA). A p-value of <0.05 was considered statistically significant.
Results
Polymer microspheres were successfully fabricated using a vibration encapsulator unit coupled with thermally induced phase separation (TIPS) processing. The frequency and polymer solution volumetric flow rate used generated a steady stream of liquid polymer droplets. The ultrastructure of neat microspheres, observed under SEM, revealed features typical of microspheres produced using TIPS. The surface consisted of a skin containing pores ranging from approximately 1–5 μm in diameter, frequently arranged in a chevron-like pattern (Fig. 3). Cross-sectioned microspheres showed highly ordered interconnected tubular morphologies, ranging from approximately 10 to 50 μm, with a ladder-like substructure that was orientated in a radial pattern. Microspheres containing particulate or an emulsion of infliximab appeared to have a more open porous surface compared with the neat microspheres.
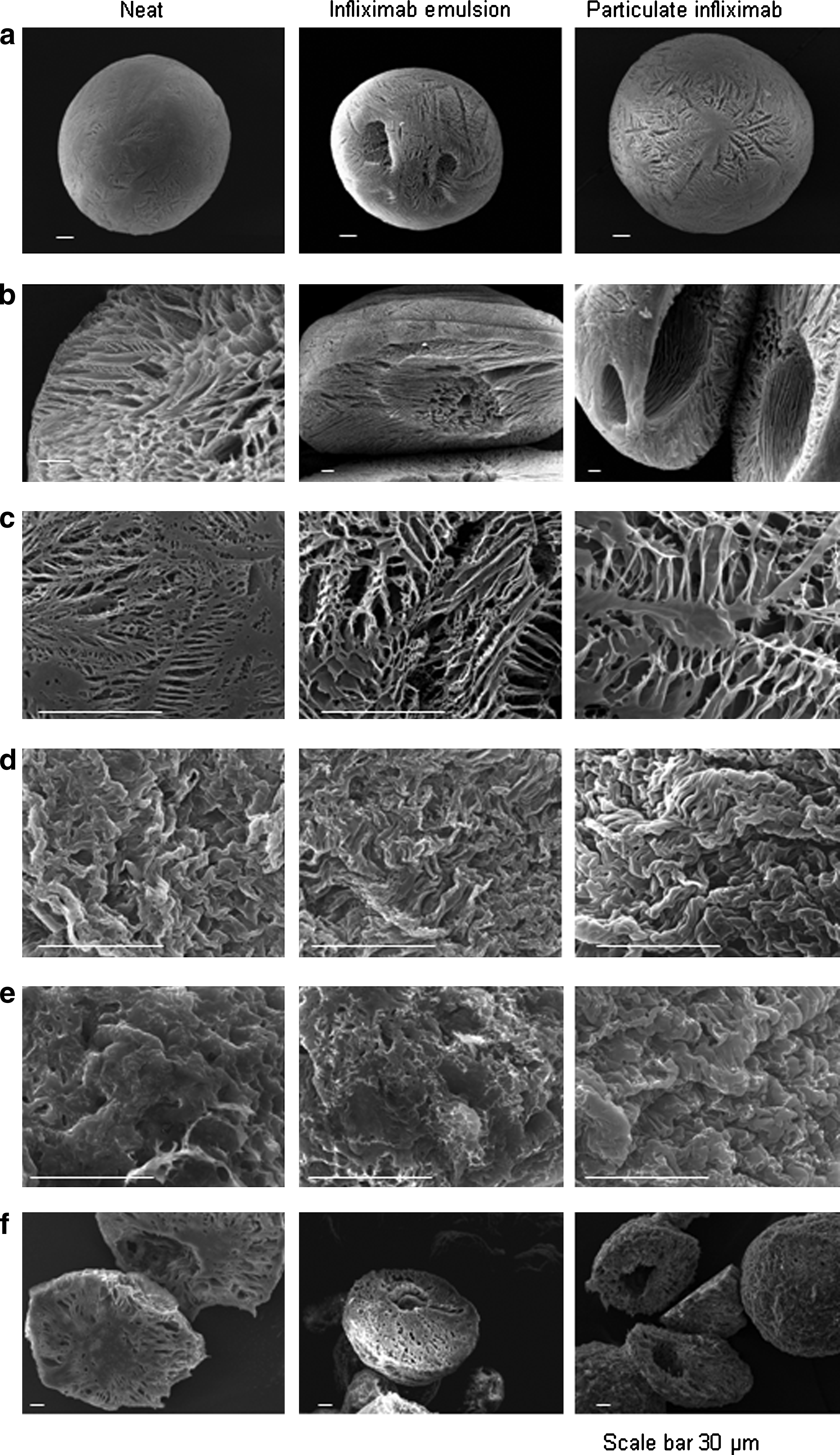
Scanning electron microscopy of neat microspheres and microspheres containing emulsion or particulate infliximab. (
Degradation of the microspheres in PBS was observed for up to 7 weeks. After incubation for 72 h in PBS, the surface of the microspheres became rugose with a less open porous structure, whereas the internal structure remained highly porous (Fig. 3). After 4 weeks of degradation the surface of the microspheres remained rugose, but the walls of the interconnecting internal tubular morphology had thickened. The surface appeared similar after 7 weeks degradation, but the internal porosity appeared to be reduced with thickened walls of the internal pores (Fig. 3). Degradation of all types of microspheres during the incubation period was confirmed by the significant reduction in size of the microspheres over the 7-week period (p < 0.001; Fig. 4).
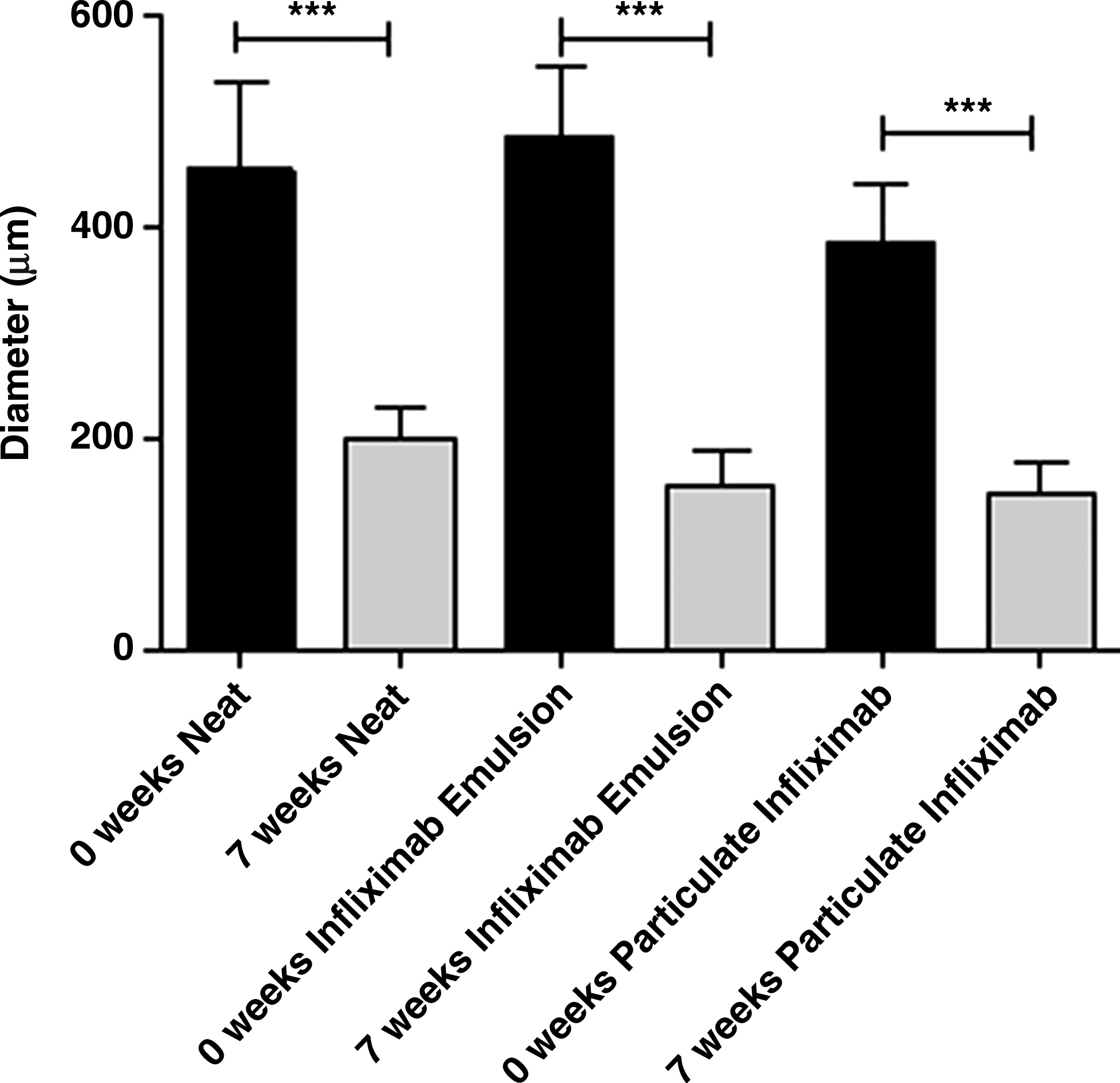
Reduction in size of microspheres after degradation in phosphate-buffered saline for 7 weeks. Data plotted are the geometric mean with 95% confidence interval (***p < 0.001).
The encapsulation yield for microspheres containing particulate infliximab was 60.38 ± 5.90% compared with 37.88 ± 14.37% for microspheres containing an emulsion of infliximab. The ability of the microspheres to release a steady amount of infliximab over a 72-h period was assessed by ELISA. Approximately 13 μg of infliximab per day was released from microspheres containing particulate infliximab with zero-order kinetics (Pearson correlation coefficient value r = 1.0; p = 0.0044) (Fig. 5). The release from microspheres containing an emulsion of infliximab was lower and less uniform compared with the microspheres containing particulate infliximab, increasing to approximately 6 μg of infliximab only at 72 h (Pearson correlation coefficient value r = 0.9699).
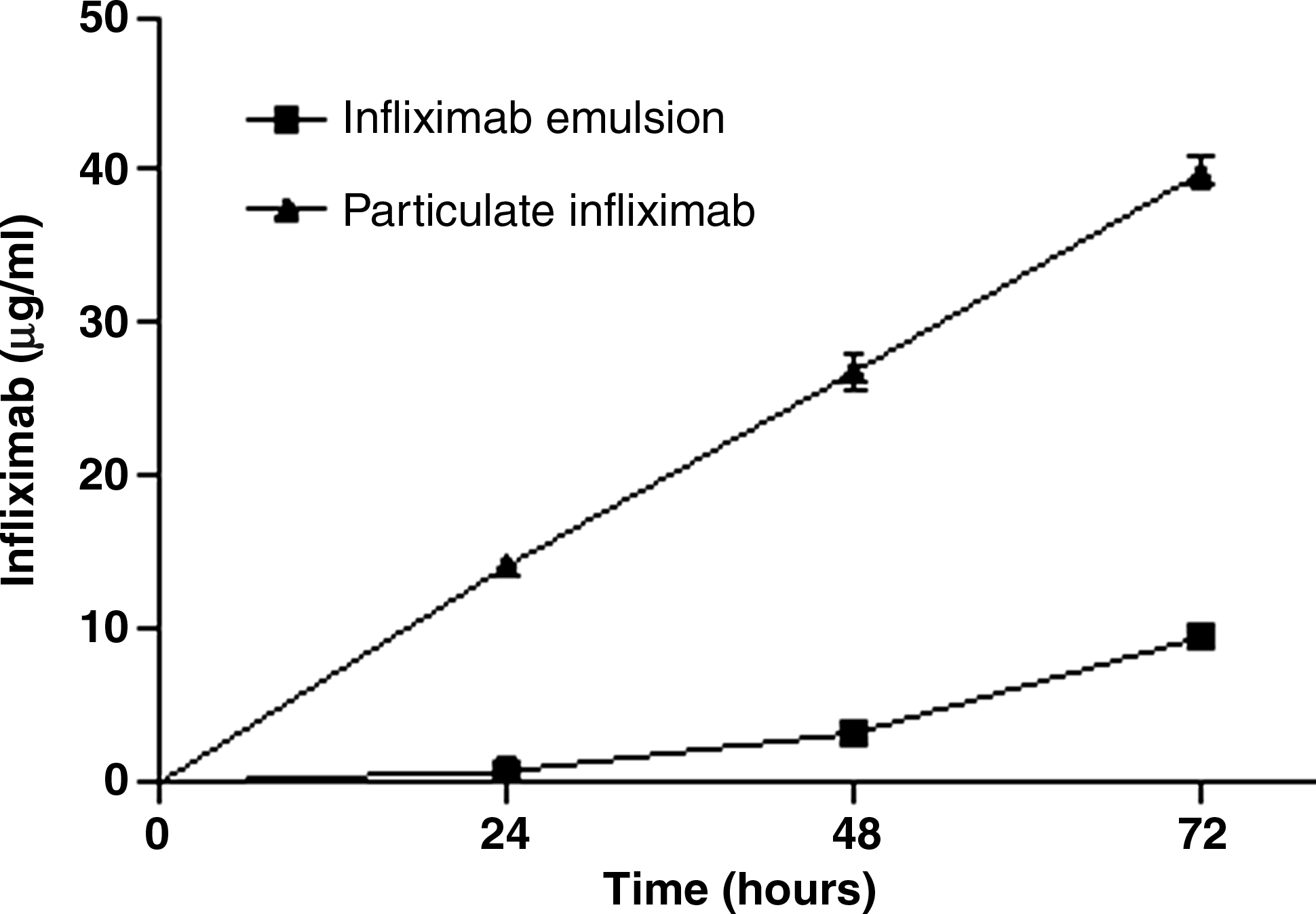
Cumulative release of infliximab from microspheres into supernatants, measured by enzyme-linked immunosorbent assay.
The sensitivity of L929 cells to rhTNF-α-mediated cytotoxicity was demonstrated via the positive control samples that received rhTNF-α alone, resulting in a significant reduction in cell viability (82.53 ± 0.32%; p < 0.001) and increase in release of lactate dehydrogenase (LDH) (192.2 ± 5.17%; p < 0.001) (Fig. 6). The addition of supernatants collected from neat control microspheres did not significantly inhibit the cytotoxic activity of rhTNF-α. Supernatants collected at all time points from microspheres loaded with particulate infliximab produced a significant increase in cell viability compared with cells treated with rhTNF-α alone (p < 0.001). A significant increase in cell viability was only observed with supernatant collected at 72 h from the microspheres containing an emulsion of infliximab (p < 0.05). The release of LDH was significantly reduced by supernatants collected from microspheres containing particulate infliximab at 24 h (p < 0.001) and 72 h (p < 0.05) compared with cells treated with rhTNF-α alone. No significant reduction in LDH release was observed with supernatant collected from the microspheres containing an emulsion of infliximab or neat microspheres.
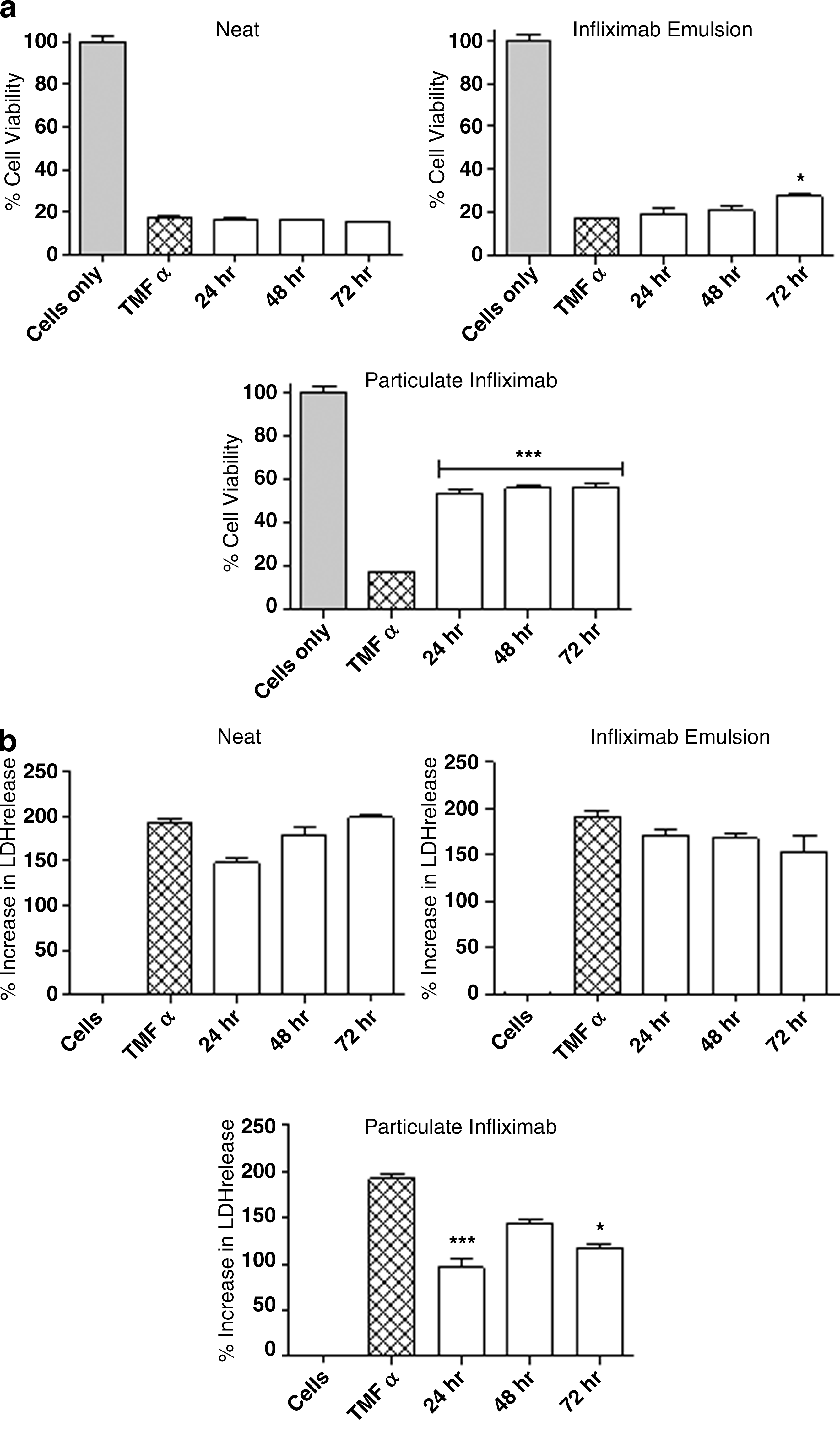
(
The migration of L929 cells into wounded area of the monolayer was increased by supernatants collected from the microspheres containing particulate and emulsion infliximab at 24 h compared with neat microspheres, but this was not significantly different (neat microspheres, 0.23 ± 0.112 mm2; emulsion infliximab microspheres, 0.49 ± 0.05 mm2 [p = 0.0591]; particulate infliximab microspheres, 0.50 ± 0.06 mm2 [p = 0.0635]) (Fig. 7). An increase was also observed with supernatants collected from microspheres containing particulate infliximab at 72 h compared with neat microspheres, but this was also not significantly different (neat microspheres, 0.58 ± 0.07 mm2; particulate infliximab microspheres, 0.66 ± 0.08 mm2 [p = 0.4699]).
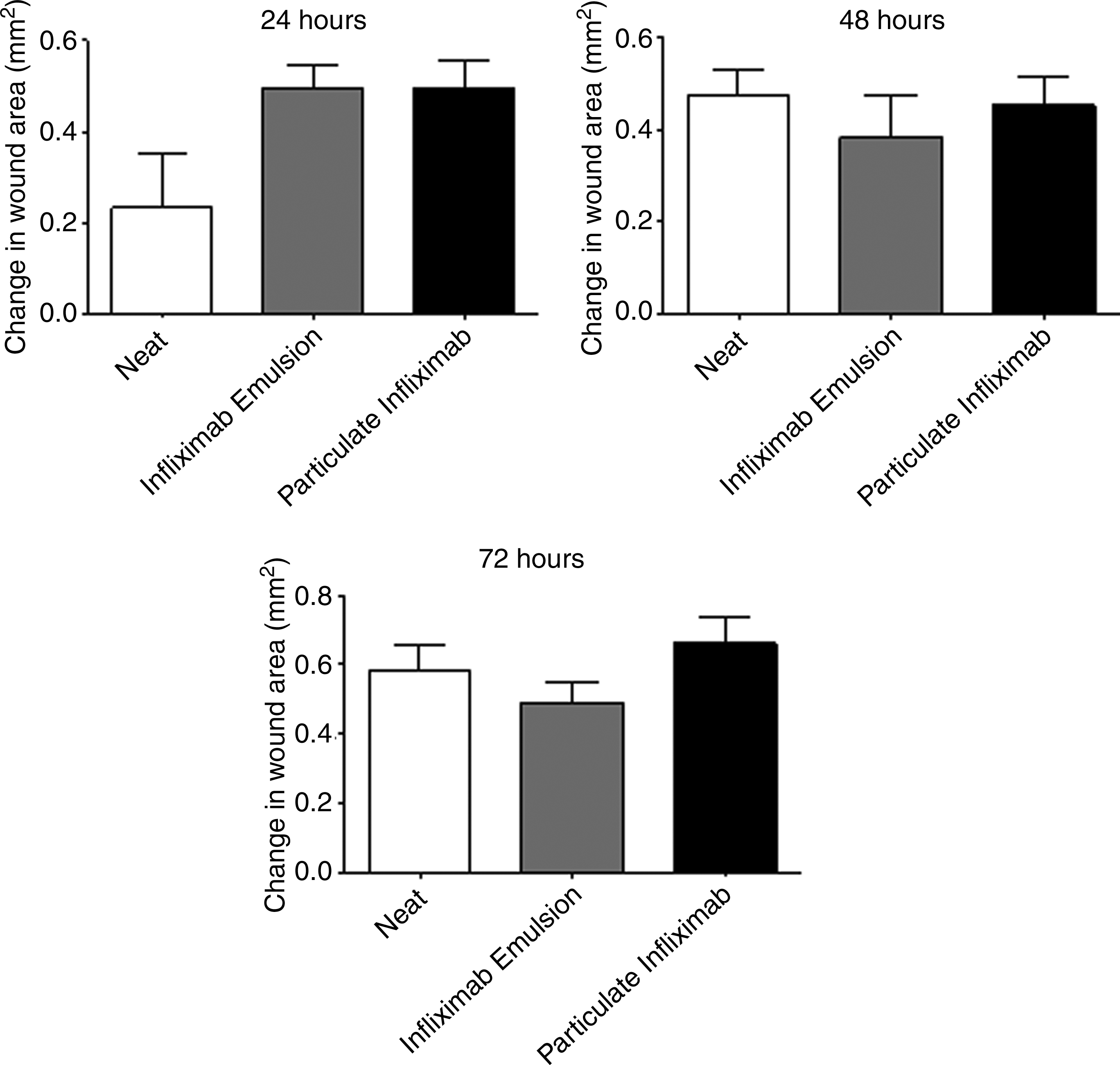
Effect of supernatants collected from microspheres at different time points on cell migration into the wound area.
Discussion
Therapeutic agents capable of modulating tissue healing can be encapsulated within microspheres for local release. Of particular importance are proteins and peptides, the delivery of which is often compromised by their short in vivo half-lives and a consequent need for frequent administration. Controlled and sustained release of encapsulated proteins is possible, even over days to months, while protection of the unreleased fraction from inactivation and physiological clearance is afforded by encapsulation in the nondegraded microsphere. Various therapeutic proteins and peptides have been successfully encapsulated within PLGA microspheres, including hormones, 19 growth factors, 20 and IgGs. 21 To date, the encapsulation of anti-TNF-α antibodies into microspheres had not been investigated.
Porous PLGA microspheres are ideal for drug delivery because the amount of polymer per microsphere is reduced compared with solid microspheres of an equal size and degradation occurs via erosion through water hydrolysis of ester bonds. Several different preparation methods have been employed to fabricate microspheres, of which emulsion solvent diffusion techniques (e.g., the oil-in-water technique) have been most frequently used. TIPS processing has been extensively employed to prepare porous PLGA monoliths for tissue engineering purposes.22,23 Recently, it has been applied to the fabrication of porous PLGA spheres. 24 Compared with emulsion solvent diffusion techniques, the TIPS process for fabricating spheres has the advantage of avoiding the long-term exposure of proteins to oil/water interfaces, which can lead to leaching and protein denaturing; it also yields high encapsulation efficiencies. 25 Other methods for producing porous microspheres, such as rapid solvent removal by introducing a temperature gradient, 26 gas foaming, 27 double emulsification (W/O/W), 28 and solution-induced phase separation, 29 are relatively more complicated and time consuming compared with the TIPS method. These methods may also require prolonged exposure to an aqueous continuous phase during solvent extraction, leading to poor encapsulation efficiency. Microspheres assessed in the current study were produced using a modified, semiautomated TIPS process utilizing a Nisco encapsulator unit. Drug encapsulation using this method is rapid, with exposure of the drug to nonfrozen solvent lasting only minutes. Previous studies preparing TIPS spheres by manually dropping the polymer solution into liquid nitrogen have produced relatively large spheres, which are too large for injectable delivery.13,24 The present study utilized a Nisco encapsulator unit to semiautomate the process to fabricate bulk quantities of smaller microspheres. The principle behind the encapsulator unit is based on Rayleigh's theory that a laminar jet of liquid will break apart into droplets of equal size if a vibration is superimposed on it. Previous studies have used the Nisco encapsulator unit to generate alginate beads within a narrow particle size distribution. 30 Sieving of the microspheres was required in the present study because polymer solution drying at the nozzle orifice or infliximab particles in the polymer solution created occasional blockages at the nozzle tip resulting in split jets of smaller droplets or coalesced larger droplets. These problems are resolvable with further modification of the fabrication process, but for the purpose of the current study, which was to demonstrate the encapsulation and release of biologically active infliximab, microspheres were sieved to a size range of 150–710 μm.
SEM revealed that the microspheres were highly porous. Slightly greater porosity was observed with the microspheres containing infliximab. In contrast to this, Maquet et al. have reported that the inclusion of glass particles resulted in decreased porosity in TIPS PLGA foams, although this effect is possibly due to a higher w/w ratio of particulates: PLGA than used in the present study. 31
Porous microspheres have several advantages over solid microspheres. They will degrade in a more predictable fashion since, unlike solid microspheres, acidic degradation products are able to escape easily via pores, preventing build up and autocatalytic effects that would accelerate degradation. 32 Their porosity also enables them to function as a scaffold, facilitating the infiltration of cells within microspheres and assisting in tissue healing. 13 The surface morphology of the microspheres in the current study became rugose at earlier degradation time points compared with previous studies investigating PLGA TIPS microporous spheres, where a smooth surface with pores arranged in a chevron-like pattern was still visible after 9 weeks of degradation. 13 A similar reduction in size was observed for all types of microsphere during the degradation period, but this was greater than the size reduction seen in previous studies with microporous spheres. 13 The reason for these differences is likely to be the lower polymer-to-solvent ratio used in the current study, resulting in a more open porous structure compared with the previous study. This would allow more liquid to infiltrate the microspheres, facilitating their shrinkage and leading to stresses along the aligned pores radiating from the center of the spheres. Plasticization due to the presence of liquid between the polymer chains would also increase their shrinkage in the short term, similar to that suggested for microporous PLGA spheres. 13
One of the challenges of protein encapsulation in microspheres is preventing damage to proteins as a consequence of the fabrication process. In a previous study, nearly 80% of IgG antibody was denatured following a double-emulsion solvent diffusion process. 21 The present study aimed to demonstrate qualitatively the release of biologically active anti-TNF-α antibodies from microspheres. An in vitro rhTNF-α neutralization assay was used to determine whether infliximab released from the microspheres was able to prevent rhTNF-α-induced cytotoxicity. Supernatants collected from microspheres containing either emulsion or particulate infliximab led to a significant decrease in rhTNF-α-induced cytotoxicity, but the effect was more pronounced and consistent over time with microspheres containing particulate infliximab. This might be attributed to the much higher encapsulation yield achieved with microspheres containing particulate infliximab compared with the emulsion infliximab microspheres. The biological activity was also reflected by the amount of infliximab measured in the supernatant by ELISA. Zero-order release was observed with supernatants collected from the particulate microspheres, whereas the release from emulsion microspheres was low but began to increase at 72 h, coinciding with the significant increase in cell viability compared with cells treated with rhTNF-α alone at this time point.
Defects in fibrinogenesis are thought to contribute to the development of perianal fistulae in CD. 4 Fibroblasts are essential for the production of extracellular matrix, and their migration into wounds is an essential component of the healing process. In vitro wound scratch assays provide a good indication of cell migration in vivo. 33 The assay in the current study was used to assess the effects of supernatants collected from microspheres on the migration of L929 fibroblasts into a model wound. Supernatants collected at 24 h from both types of microspheres containing infliximab produced an increase in cell migration into the wound area compared with neat microspheres. Supernatant collected from particulate infliximab microspheres at 72 h produced a similar effect, but this was not significant for either time point. Anti-TNF-α antibody released from the microspheres might account for the increased cell migration seen with the infliximab microspheres. Similar effects have been reported by Di Sabatino et al., who have shown that infliximab increased myofibroblast migration in a wound scratch assay in a dose-dependant fashion. 34 This effect could accelerate tissue infiltration into the scaffold structure provided by microspheres delivered into the fistula tract. Further work in this area is required to optimize and harness this additional beneficial property of infliximab, which could offer a supplementary mechanism to facilitate tissue infiltration and healing of the fistula tract.
Conclusion
The current study presents a novel method for fabricating porous medicated microspheres aimed at providing localized delivery of anti-TNF-α antibodies to perianal fistulae. Bulk quantities of porous microspheres were successfully fabricated using a modified TIPS process, which demonstrated zero-order release of biologically active anti-TNF-α antibody. On the basis of the findings from the current study, microspheres containing particulate infliximab appear to possess better properties than emulsion infliximab microspheres, especially since the ability to deliver infliximab via a zero-order mechanism will be crucial to ensure that a steady amount of antibody is released from the microspheres into the fistula tract over time, thus reducing potential peak–trough fluctuations associated with systemic delivery. These results indicate that microspheres loaded with anti-TNF-α antibody could provide a novel therapeutic strategy for treating fistulae in CD patients where they would function as a biologically active scaffold filler material. The novel microsphere processing technique described is likely to be applicable to a variety of other microsphere-based treatments involving therapeutic peptides.
Footnotes
Acknowledgments
The authors appreciate the technical support of Nicolaos Mathioudakis (Biomaterials and Tissue Engineering Group) and Nicky Mordan (SEM) at the Eastman Dental Institute, University College London, London. The work conducted in this study was supported by a grant from the European Crohn's and Colitis Organization. This work was undertaken at University College London Hospitals (UCLH)/University College London (UCL), who received a proportion of funding from the Department of Health's National Institute for Health Research (NIHR) Biomedical Research Centres funding scheme.
Disclosure Statement
No competing financial interests exist.