
Abstract
We present a method for producing a cell–scaffold hybrid construct at the bedside. The construct is composed of plastic-compressed collagen together with a poly(ɛ-caprolactone) (PCL)-knitted mesh that yields an integrated, natural–synthetic scaffold. This construct was evaluated by seeding of minced bladder mucosa, followed by proliferation in vitro. High mechanical strength in combination with a biological environment suitable for tissue growth was achieved through the creation of a hybrid construct that showed an increased tensile strength (17.9±2.6 MPa) when compared to plastic-compressed collagen (0.6±0.12 MPa). Intimate contact between the collagen and the PCL fabric was required to ensure integrity without delamination of the construct. This contact was achieved by surface alkaline hydrolysis of the PCL, followed by adsorption of poly(vinyl) alcohol. The improvement in hydrophilicity of the PCL-knitted mesh was confirmed through water contact angle measurements, and penetration of the collagen into the mesh was evaluated by scanning electron microscopy (SEM). Particles of minced bladder mucosa tissue were seeded onto this scaffold, and the proliferation was followed for 6 weeks in vitro. Results obtained from phase contrast microscopy, SEM, and histological staining indicated that cells migrated from the minced tissue particles and reorganized on the scaffold. Cells were viable and proliferative, with morphological features characteristic of urothelial cells. Proliferation reached the point at which a multilayer with a resemblance to stratified urothelium was achieved. This successful method could potentially be used for in vivo applications in reconstructive urology as an engineered autologous tissue transplant without the requirement for in vitro culture before transplantation.
Introduction
The concept of tissue engineering, including in vitro culture of autologous cell transplants, is an attractive alternative for reconstructing bladder tissue. Autologous cells for tissue engineering play a key role to avoid immunogenic response to the transplant. The most frequently used cells have been urothelial cells and smooth muscle cells harvested by biopsy from healthy parts of the bladder during open surgery. 8 In general, the commonly accepted procedure includes harvesting of cells or tissue from the patient, cell expansion in the laboratory, attachment of cells to a supporting scaffold, and then re-shaping the transplant before implanting it into the surgical site according to the specific needs of the patient.2,9–11 However, this strategy for tissue engineering is time-consuming, costly, and laborious. Moreover, the fact that guidelines for cell-based medical products follow strict rules for the production of pharmaceutics limits its use in standard surgical units. 12
To overcome these limitations, we propose to minimize the ex vivo processing of tissue by using only mechanical tissue and cell separation, together with the patient's body itself as the bioreactor for tissue expansion and regeneration. We also suggest the use of other epithelial cell expansion methods that have been developed for the treatment of chronic wounds. 13 Fossum et al. have successfully used minced autologous skin for tissue engineering of epithelialized subcutaneous tunnels and have shown that the patient's body can be considered an in vivo incubator for the expansion of minced autologous skin or urothelium.14,15 Hence, the use of minced tissue of bladder mucosa may serve as an alternative to in vitro culturing of urothelial cells. In the present study, we developed a scaffold suitable for rapid and direct combination with minced tissue and examined the in vitro culturing of a minced bladder mucosal tissue–scaffold hybrid. The goal was to develop a construct combining mechanical strength with tissue regeneration to provide for regeneration in vivo upon direct bedside implantation.
Both synthetic and natural polymers have been employed for this type of construct.1–2,16 Among the natural polymers, collagen has been widely used for bladder tissue engineering applications because of its favorable cell–matrix interactions.16–19 However, conventional collagen-based scaffolds in the form of hydrogels that allow rapid introduction of cells or tissues suffer from low mechanical strength and are not conducive to surgical handling. To overcome this limitation, the technique of plastic compression of collagen hydrogels was introduced by Brown et al. 20 While this approach improves the mechanical properties, it does not provide sufficient strength for bladder engineering. However, Engelhardt et al. 21 have demonstrated the potential of a hybrid plastic compressed collagen within a knitted mesh of poly (lactic acid-co-ɛ-caprolactone) to further increase strength.
In the present study, we have integrated a plastic-compressed collagen hydrogel within a poly(ɛ-caprolactone) (PCL)-knitted mesh as a scaffold for culturing minced tissue from pig bladder. The PCL-knitted mesh fiber surface is first rendered hydrophilic through a slight alkaline hydrolysis that is followed by an adsorption of poly(vinyl alcohol) (PVA) from solution to allow subsequent wetting and impregnation by the solubilized collagen. The hydrophilic mesh is then embedded between two slabs of collagen hydrogel before plastic compression, resulting in a hybrid structure, a natural–synthetic polymer. This structure is mechanically strong and easy to handle because of the presence of the PCL mesh and also provides an environment that facilitates the direct culturing of minced tissue of bladder mucosa. We selected the pig as a model. In respect to many physiological features, the pig is a good model for preclinical human studies and therefore it is logical to develop the method for this purpose.
The minced bladder tissue was seeded and cultured in vitro for 6 weeks, demonstrating the successful formation of a multilayer of stratified cells. By extending this approach in vivo, we expect to eliminate the need for long-term laboratory procedures and offer direct methods for tissue engineering of bladder wall patches in the operating room and at the surgical table.
Materials and Methods
Melt-spinning of PCL fibers
PCL (Sigma-Aldrich), with a number-average molecular weight (Mn) of ≈80,000 g/mol, in the form of white beads, was dried under vacuum before use. Dried PCL was subsequently compressed into cylindrical rods, followed by melt-spinning at 180°C under a nitrogen atmosphere according to previously published procedures. 22
Fabrication of PCL-knitted meshes
The as-spun filament was drawn at 30°C, followed by heat setting at 30°C under tension. Knitting was carried out on a Lawson Hemphill FAK-Sampler (FAK-S). The FAK-Sampler knitting cylinder is an 89-mm-diameter cylinder with 380 needles (35 needles per inch and a needle gauge of 75). Clean and dry instrument air at a pressure of 40 psi (3 bar) was used throughout the knitting process.
Preactivation of the PCL surface
An alkaline hydrolysis was performed on the PCL-knitted mesh, using 2.5 M NaOH for 40 min at 40°C with subsequent rinsing in distilled water and treatment in PVA (Merck; MW≈72,000 g/mol) solution (1% w/v) for 10 min. The treated PCL mesh was sterilized by embedding it in 70% ethanol for 30 min.
Contact angle measurements
The degree of hydrophilicity of the alkaline-hydrolyzed and PVA-treated PCL-knitted meshes was determined with the use of a Video-Based Optical Contact Angle Meter (DataPhysics OCA 15EC). Small pieces (4×1 cm2) of the samples were cut and placed onto a glass microscope slide using double-sided tape to ensure a uniform viewing of surface. The glass slide was placed on the stage, and a 6-μL drop was automatically measured from the syringe while the stage moved up to place the drop on the sample surface. The drop was allowed to reach equilibrium (which typically took 5 s) before measurement. Using the SCA 10 software, we determined the contact angles on the left and right sides of the drops. For each sample, five measurements were performed, and the average of 10 samples was reported.
Preparation of the hybrid scaffold-tissue construct
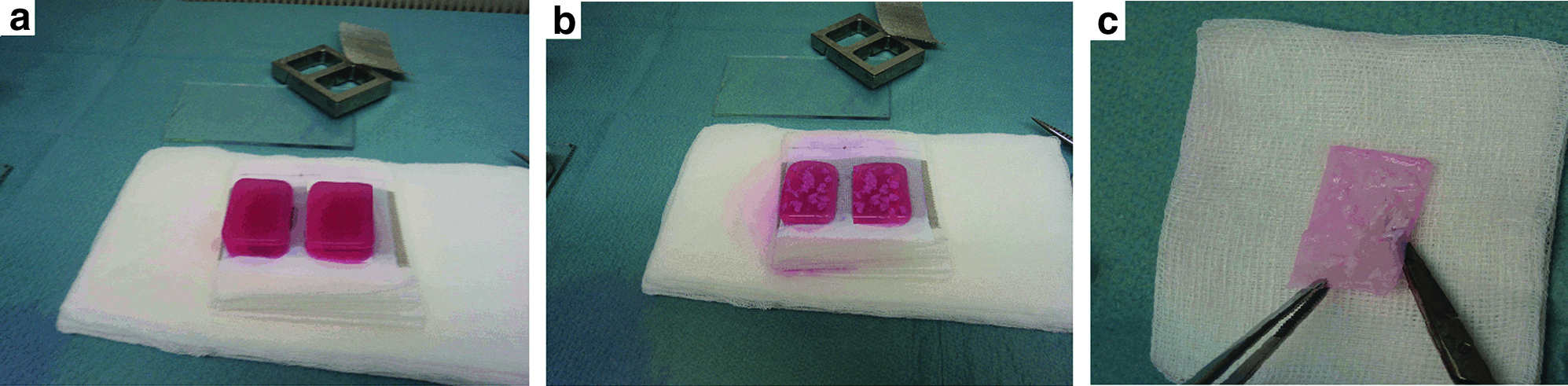
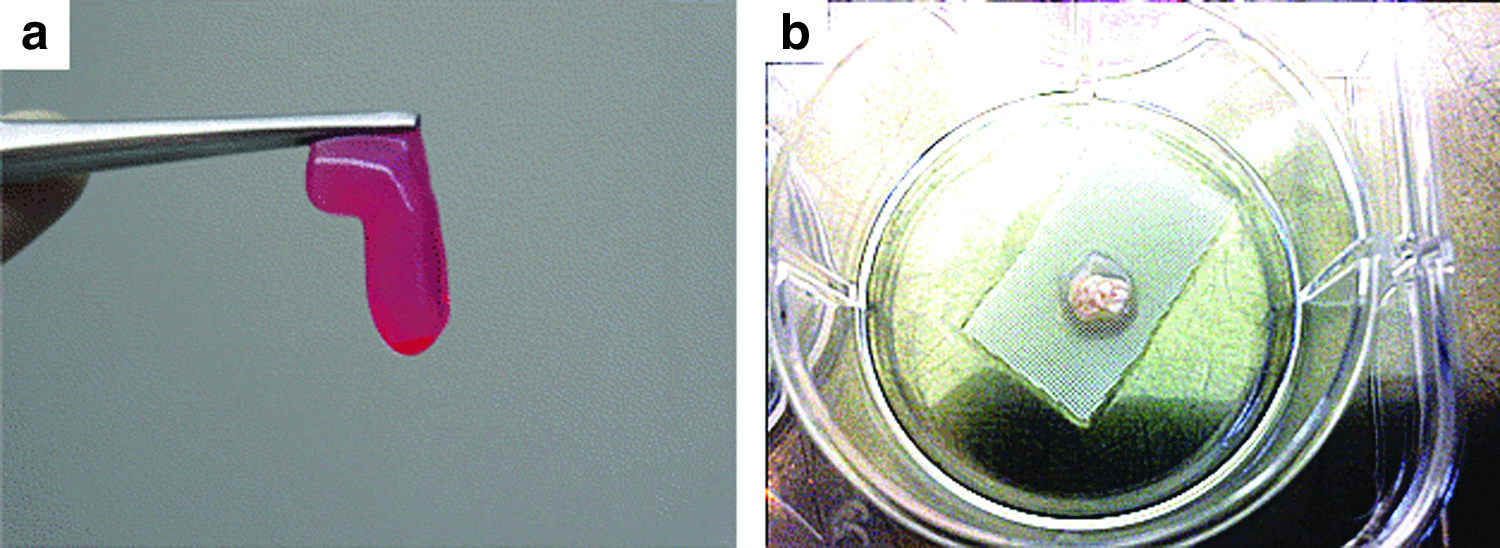
Formation of the collagen gel and plastic compression were carried out by a technique described previously, 21 in which 4.8 mL of sterile rat-tail collagen type I solution (2.06 mg/mL protein in 0.6% acetic acid; First Link Ltd.) was mixed with 0.6 mL 10×Eagle's minimum essential medium (MEM; Invitrogen). The solution was neutralized with 2.5 M NaOH, after which 0.6 mL of alpha-MEM medium was added. The first gel slab was cast from 2 mL of the 6 mL solution in a rectangular mold (20×30×10 mm) and incubated at 37°C for 10 min to form a semi-rigid hydrogel onto which the sterilized PCL-knitted mesh (20×30 mm) was placed; the remaining 4 mL of collagen solution was cast into the mold to form a second slab of collagen. Gel formation was completed inside the incubator for 20 min (Fig. 1a). The hydrogel construct was transferred onto blotting elements, consisting of a layer of sterile 110 μm-thick nylon mesh (∼40 μm mesh size) and a sterile 400-μm-thick stainless steel mesh (mesh size ∼200 μm), which were placed on top of three sterile gauze pads. The set gels (with the PCL mesh in the middle) were covered with a second nylon mesh and a loading plate (as a static weight) (120 g) for 5 min at room temperature, leading to the formation of a plastic-compressed hybrid construct with an average thickness of 420 μm.
Procedure for seeding minced tissue onto the hybrid construct:
Minced tissue preparation
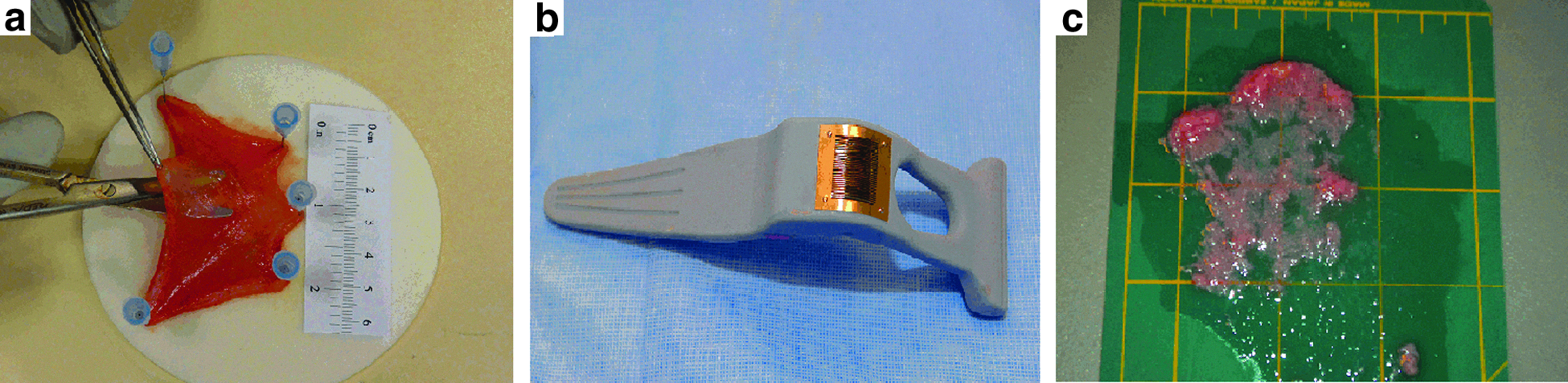
The excised pig bladder was washed twice in Dulbecco's modified Eagle's medium (DMEM), and the detrusor muscle was removed mechanically as seen in Figure 2a. The bladder mucosa was cut into pieces measuring 10×10 mm. Each piece was then minced vertically and horizontally (using the mincing device as shown in Fig. 2b) to produce∼150 particles, each measuring ∼0.3×0.8×0.8 mm, as is shown in Figure 2c.
Preparation of minced tissue.
Minced tissue-seeded scaffolds
Minced tissue was seeded on top of the hybrid construct by placing the minced particles on top of the gel slab (Fig. 1b) and plastic compression was performed afterward (Fig. 1c). Approximately 1 cm2 of minced tissue was used for a scaffold measuring 6 cm2 (1:6 expansion). The scaffolds containing minced tissue were cut and cultured in 12-well plates in keratinocyte medium:DMEM and Ham's F12 (4:1 mixture; Gibco) containing fetal bovine serum (10%; Gibco), insulin (5 μg/mL), hydrocortisone (0.4 μg/mL), adenine (21 μg/mL; Sigma), cholera toxin (10−10 mol/L), triiodothyronine (2×10−9 mol/L), transferrin (5 μg/mL), epidermal growth factor (10 ng/mL), and antibiotics (50 U/mL penicillin and 50 μg/mL streptomycin). The wells were maintained in 5% carbon dioxide and humidified air at 37°C at atmospheric pressure. After 2, 4, and 6 weeks, samples were collected and fixed in formalin.
Tensile strength
The tensile strengths of the plastic-compressed collagen and hybrid scaffold of PCL-collagen were determined using the Instron 5944 tensile tester equipped with a 50-N load-cell with a crosshead speed of 10 mm/min (gauge length=40 mm) under wet conditions. Wet samples were prepared by incubating the samples in phosphate-buffered saline for 24 h at 37°C. Samples were cut into a rectangular shape (60×10 mm). The average of five measurements is reported.
Electron microscopy
Hybrid PCL-collagen constructs were examined by scanning electron microscopy (SEM). Specimens were fixed in 10% formalin for 1 h. Afterward, the specimens were washed with distilled water before being passed through a graded ethanol series to remove water, then immersed in hexamethyldisilazane (Sigma-Aldrich) for 15 min. Samples were then air-dried, mounted on stubs, and sputter-coated with gold before being examined on a digital scanning electron microscope (SEM—Zeiss 1550).
Histology
All samples were fixed in 35% formaldehyde solution, embedded in paraffin, and cut into 4-μm sections. After rehydration, slides were stained with hematoxylin and eosin (H&E) for routine histology. Tissue specimens were also evaluated by immunostaining for cytokeratins and proliferation markers, using primary antibodies against various cytokeratins (MNF-116; Pancytokeratins 5, 6, 8, 17, and 19; DakoCytomation), and a primary antibody against cellular proliferation (Ki-67; Lab Vision, Rabbit Monoclonal, clone SP6).
Results
Surface treatment of the PCL textile mesh
Our initial attempt at surface modification following reported procedures23,24 gave an instantaneous change in the water contact angle on the PCL mesh from 104±5.3° (untreated sample, Fig. 3a) to 79±6.9° after alkaline hydrolysis (Fig. 3b). After storage of the surface-treated sample, the improved hydrophilicity was not stable. The contact angle increased with time (to 91±5.7°). Hydrolysis followed by PVA adsorption treatment resulted, however, not only in a stable hydrophilic surface but also in an even more hydrophilic surface with a contact angle of 41±11.2° (Fig. 3c).

Contact angle measurement of the surface of PCL-knitted mesh:
Plastic compression of collagen onto the PCL mesh
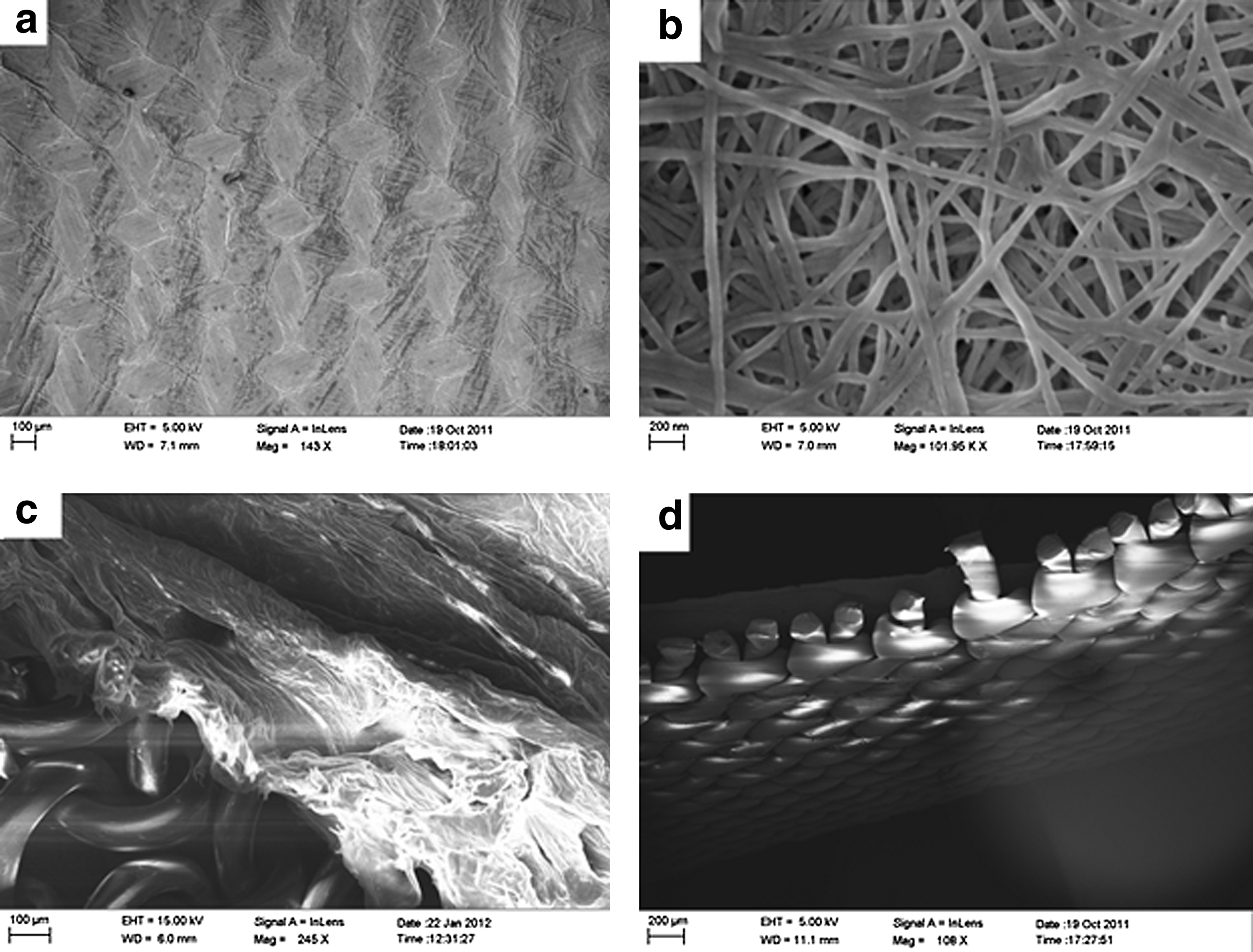
Through the use of a hydrophilic PCL-knitted mesh, we achieved a stable hybrid construct of PCL-collagen with no disintegration after plastic compression and tissue culture. Figure 4 shows the surface of the collagen after plastic compression on a PCL-knitted mesh in (Fig. 4a) macroscale, (Fig. 4b) microscale, and (Fig. 4c, d) in cross sections of the hybrid construct. As seen in Figure 4a, macroscale observation revealed collagen fibers aligned along of the surface on which the compression was carried out (here, knitted mesh), and we saw a nanofibrous structure on the microscale, with an average diameter of 47±6 nm, comparable to that of native extracellular matrix (ECM) 25 (Fig. 4b). It is also clear that the hydrophilicity enhancement procedure was successful, since a homogenous composite was achieved after plastic compression on seeded scaffolds (Fig. 4d).
Surface of plastically compressed collagen-PCL-knitted mesh in
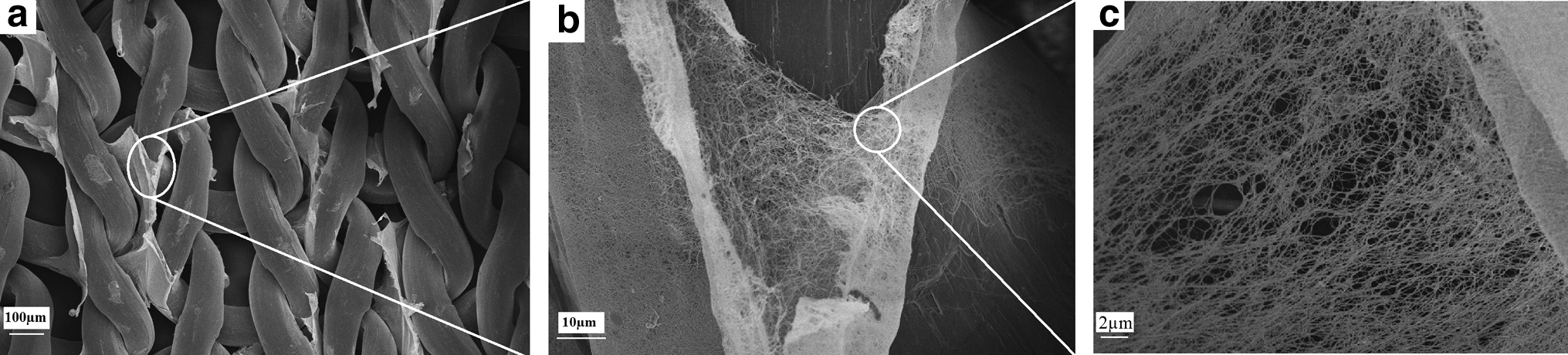
To further confirm the appropriate attachment of the collagen to the PCL-knitted mesh, the collagen layer was manually separated from the surface of the knitted mesh after plastic compression. The plastic-compressed collagen not only covered the surface but also appeared in-between PCL threads, indicating integration between the filaments (Fig. 5). This result is in contrast to the spontaneous delamination seen in the absence of surface hydrolysis, when no anchoring of the collagen onto or into the PCL mesh was achieved (not shown).
Scanning electron microscopy (SEM) images of
Tensile strength
Tensile testing of the PCL-collagen hybrid showed an increase in tensile strength, from 0.6±0.12 MPa for plastic-compressed collagen alone to 17.9±2.6 MPa for the hybrid construct of PCL-collagen. Mechanical handling of the plastic-compressed collagen (without support) was not possible due to its poor dimensional stability (Fig. 6a). Moreover, seeding of minced tissue particles on top/within a cube of collagen gel and then implementing plastic compression (without any support) made the plastic-compressed collagen prone to rupture and/or dimensional change.
Cell seeded scaffolds
The presence of minced tissue inside the plastic-compressed collagen led to a large contraction in the construct during in vitro culture (Fig. 6b), as a result of the rapid contraction of natural ECM by the cells.26,27 Using the PCL-knitted mesh overcame this problem, and no contraction was seen over the 6 weeks of in vitro culture.
Seeding of scaffolds with minced tissue resulted in successful proliferation of urothelial cells. Plastic compression was performed after spreading of the minced tissue particles on the collagen top layer. The compression resulted in a slight penetration of minced particles into the plastic-compressed collagen. Phase-contrast microscopy of minced tissue-seeded scaffolds (after 4 weeks) showed that cells have migrated from the minced tissue to the surface of the hybrid scaffold (Fig. 7).
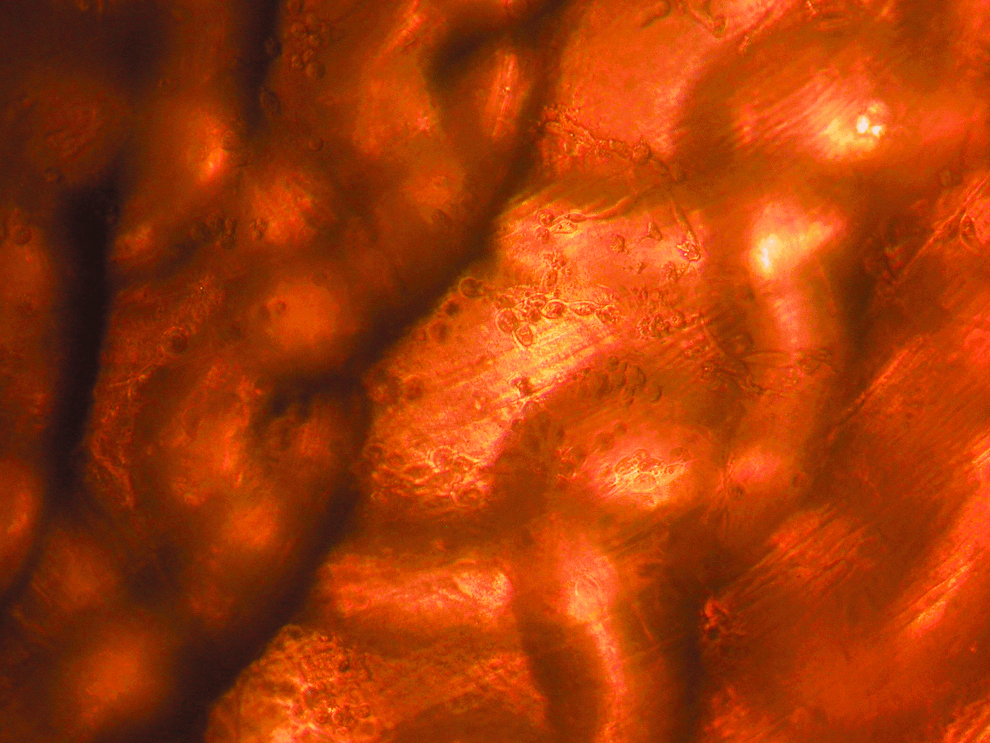
Phase-contrast microscopy of minced bladder mucosal particles seeded onto a PCL-collagen construct after 4 weeks in cell culture (original magnification ×20). Color images available online at
SEM images of the seeded scaffolds at 2, 4, and 6 weeks are shown in Figure 8. Although the nanofibrous structure of the plastic-compressed collagen is clearly visible in Figure 8a, the substrate structure was completely covered with proliferated urothelial cells after 4 (confluent, Fig. 8b) or 6 weeks (multi-layered, Fig. 8c). The integrity of the collagen scaffold corroborated with what has been reported earlier for compressed collagen where no weight loss was observed for 21 days culture using fibroblasts. 28
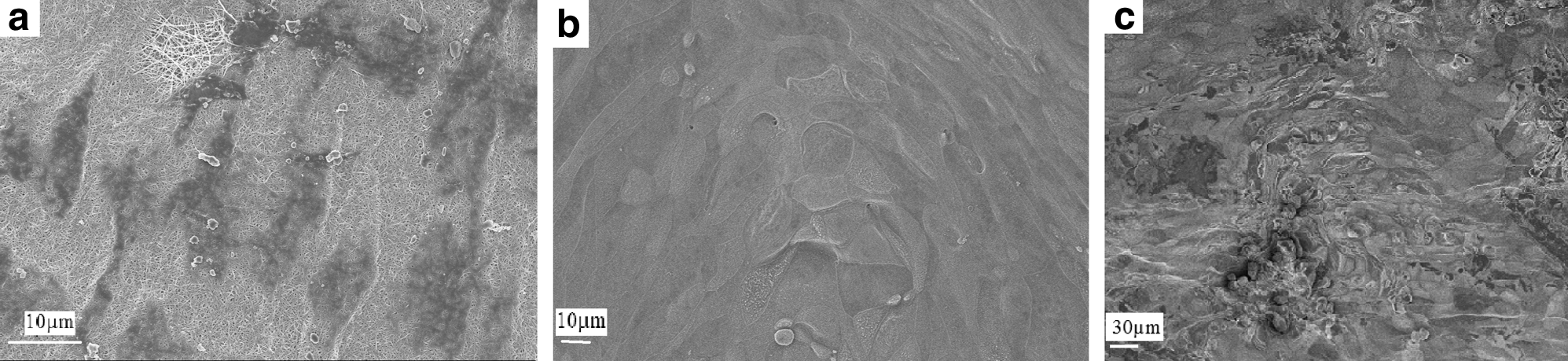
SEM images of minced tissue particles seeded on PCL-plastic-compressed collagens construct after
Histological staining was performed at 2, 4, and 6 weeks. H&E staining indicated that epithelial cells (stained dark pink) were present around the plastic-compressed collagen (stained pale pink); the PCL mesh is seen in white (unstained) between the two collagen layers. Thus, it appears that the construct has kept its integrity, and no delamination occurred during the first 6 weeks. We also observed single-layer epithelium after 2 weeks and multi-layered epithelium after 4 weeks by histologic staining (Fig. 9a–c). After 6 weeks, cells were present within the collagen as well, indicating remodelling of the scaffold (Fig. 9c). The cells were positive for the antibody Ki-67, indicating proliferation throughout the whole experiment, and were also positive for antibody MNF 116, indicating their epithelial origin (Figs. 9d–f and 10).

Histologic appearance hematoxylin (HTX)-Eosin): from single layer to multilayer epithelium
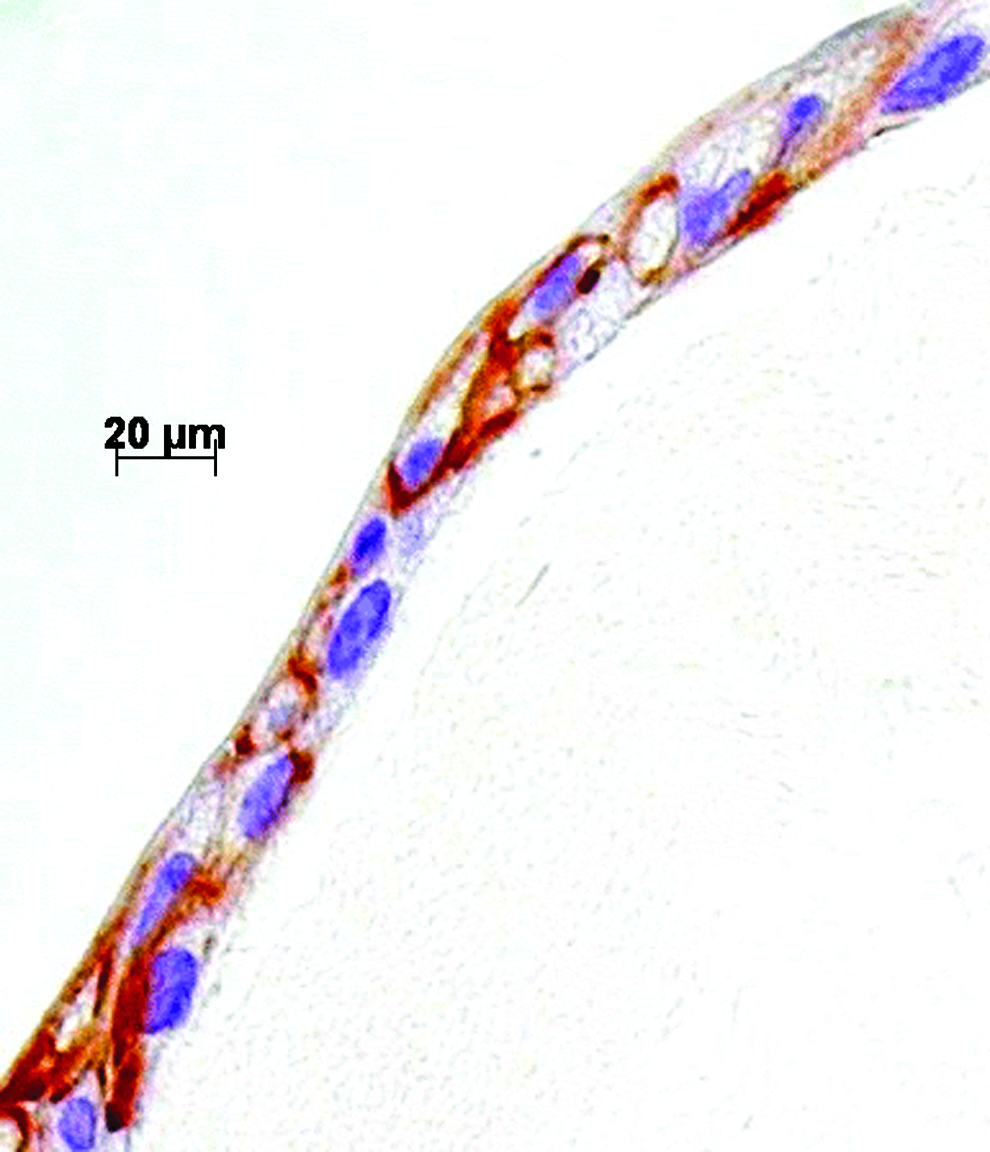
Cell cytoplasm positive for MNF 116 with HTX staining of nuclei.
Discussion
To date, the algorithm for tissue engineering with autologous cells has involved four important steps: cell harvesting, cell expansion in vitro, preparation of the transplant by co-culturing on a carrier, and finally transplantation back to the patient. In the clinical trials performed thus far, autologous cells have first been harvested from the patient by open bladder biopsy (urothelial cells and smooth muscle cells) 10 or from bladder washes (urothelial cells only). 29
In vitro processing, including enzymatic treatment and cell expansion, has been performed in a laboratory environment and included artificial exposure to growth factors, hormones, and cell culture medium. Cells have sometimes been deep-frozen and thawed before transplantation. Even under optimal conditions, in vitro expansion and preparation of transplant requires time-consuming cell culture for a minimum of 3–8 weeks (depending on size of the transplant). Cell culture is laborious, and in order to guarantee safe manufacturing conditions, the method has been restricted to very few high-technology laboratory-hospital settings.
We wanted to address the limitations that might account for the limited application of tissue engineering to clinical urology. Therefore, we decided to combine an algorithm of using the body as a bioreactor with a tissue carrier that could be molded in a three-dimensional (3D) fashion, could be handled surgically, and would be biodegraded as the new cells expand, reorganize, and remodel.
Fossum et al.14,15 have simplified the approach by mincing autologous skin epithelium or bladder mucosa for tissue transplants based on the method introduced by Meek. 13 They showed that the transplanted minced tissue remains viable, proliferates, and reorganizes on tubular latex scaffolds that serve as 3D molds and are later removed.14,15 A synthetic–natural hybrid of poly(lactide-co-caprolactone)-knitted mesh-plastic-compressed collagen has also been developed and evaluated by Ananta et al. using neonatal foreskin fibroblasts inside and on top of the collagen gels. By in vitro cell culture, they demonstrated a homogenous cell distribution and good biocompatibility with their construct. 19
In the present study, we have designed a 3D hybrid construct made from a biodegradable knitted mesh integrated with minced bladder mucosa. Plastic compression of collagen gel is a method for fabricating collagen constructs with densities resembling native extracellular matrix. With this technique, the mechanical properties are improved over those of hydrogels and sponges of collagen. Plastic compression is easy to do and requires only 5 min to perform, including the insertion of the minced epithelium. However, the mechanical properties obtained are still inferior to those of strong tissues such as skin, 30 tendon, 31 and bladder (our target tissue) that are expected to undergo frequent contraction and extension.
In such a scaffold, the requisite structural and mechanical properties are provided by the PCL-knitted mesh, which is able to withstand forces from urine storage, filling/emptying, and those exerted on it by the pelvic muscles. 32 The literature reports a maximum tensile stress of human bladder tissue stiffness ranged from 0.5 to 2.6 MPa, which may be compared to 17.9 MPa for the PCL-based scaffold. The average stiffness and extensibility of the PCL-collagen construct was 10.5 MPa and 67% elongation at break, which may be compared to 1–4.1 MPa and 69% in humans.33,34 How the compliance affects the in vivo outcome will be of great interest in future studies.
Collagen, the most abundant protein in the body, was selected for our biomatrix. In its native form, it is known to exhibit minimal inflammatory and antigenic responses,35,36 although care has to be taken, especially to inter species immune reactions when translating the technique to the in vivo setting, as such responses do occur. 37 It has also been reported that the formation of a dense collagen region during plastic compression of collagen gels has increased hydraulic resistance of hydrated gels, as well as diminishing the fluid flow through the construct.38,39 In addition, after transplantation, the bladder could have a tube for drainage during the time of healing. Risk for intraperitoneal leakage is then small.
Collagen has been shown to be helpful in retaining the phenotype and activity of many cell types, and it contains cell-adhesion peptide sequences (e.g., RGD) that contribute to specific cellular interactions. 40 The preparation of this hybrid scaffold was, however, challenging. Initial attempts to implement plastic compression of collagen around the PCL mesh failed to give reproducible and stable constructs that would allow for long-term culture. We attributed this result to poor wetting and spreading of the collagen solution into the hydrophobic PCL fabric. Therefore, we investigated methods for modifying the PCL surface to make it hydrophobic. Alkaline hydrolysis of the PCL followed by PVA treatment improved the hydrophilicity of the PCL mesh, as has previously been reported for similar cases, 41 and as a result an integrated structure was obtained. Furthermore, the scaffold could be sutured for in vivo applications without shrinkage (Fig. 6).
Scaffolds seeded with minced tissue showed that the method resulted in successful proliferation of urothelial cells (Figs. 7 and 9). In addition, it was evident that cells migrated from the minced tissue specimens and proliferated on and inside the collagen-PCL construct. The newly formed cells reorganized on the surface and formed a multilayer epithelium before 6 weeks (Figs. 8 and 9). Furthermore, the cells were positive for Ki-67 and MNF116, indicating an epithelial origin and proliferation throughout the whole experiment.
Like traditional cell culture from tissue explants, the initiation process required cell migration of progenitor cells that then regenerated and reorganized in the culture dish. This process often requires 1–2 weeks under ordinary cell culture conditions.42,43 In our composite material, instead of reorganizing and expanding in the bottom of the culture dish, the cell regeneration and reorganization took place on the collagen surface and a confluent proliferating monolayer had already formed after 2 weeks (Fig. 9a, d). Later on, cell division took place in the bottom of the multi-layered epithelium (Fig. 9f), indicating the formation of a basal membrane on the collagen surface and an organization resembling that of a normal transitional urothelium.
Conclusion
To overcome the hurdles posed by regulatory requirements and the high costs associated with in vitro culturing of urothelial cells in the tissue engineering of bladder wall patches, we have introduced minced tissue from the bladder mucosa as part of a hybrid tissue–scaffold that can serve as an alternative to cultured cells and can be employed directly at the surgical table. The hybrid tissue–scaffold consisted of a PCL-knitted mesh integrated between two layers of plastic-compressed collagen, into which minced bladder mucosal tissue had been incorporated. The mechanical properties were significantly improved by the incorporation of a PCL-knitted mesh when compared to plastic-compressed collagen alone, and surface treatment of the PCL mesh assured proper collagen infiltration upon bedside processing.
SEM images and histological staining showed that urothelial cells could migrate from minced tissue particles to cover the hybrid construct within 2 weeks and produce a multilayer stratified urothelium in 6 weeks. These results suggest the potential for applying minced tissue particles onto/inside an appropriate scaffold for tissue engineering of clinical constructs such as bladder wall patches. Our current aim is to use this hybrid construct in vivo so that a piece of bladder wall can be harvested and the mucosa extracted and minced, then distributed onto/inside the collagen slab and compressed to create the hybrid construct. With the current work, we anticipate being able to expedite the process of bladder wall repair by using this one-stage procedure (that can be done in less than 30 min). After compression, the hybrid construct can potentially be sutured back into the right position, so that the patient's body can be used as the bioreactor. The advantages of this method include that autologous cells can be applied with no risk of rejection by the immune system, and no need for time-consuming and expensive in vitro cell culture, since both the cell harvesting and transplantation back are done in one step.
Footnotes
Acknowledgments
We thank Dr. Deborah McClellan for editorial assistance and Prof. Elof Eriksson, Harvard Medical School, for kind provision of the mincing device. Grants from the Swedish Society for Medical Research and the Promobilia Foundation supported this work.
Disclosure Statement
No competing financial interests exist for any of the authors.