
Abstract
The purpose of this study was to assess the natural partial oxygen pressure (pO2) of subcutaneous (SC) and intraperitoneal (IP) sites in mice to determine their relative suitability as sites for placement of implants. The pO2 measurements were performed using oxygen imaging of solid probes using lithium phthalocyanine (LiPc) as the oxygen sensitive material. LiPc is a water-insoluble crystalline probe whose spin–lattice and spin–spin relaxation rates (R1 and R2) are sensitive to the local oxygen concentration. To facilitate direct in vivo oxygen imaging, we prepared a solid probe containing encapsulated LiPc crystals in polydimethylsiloxane (PDMS), an oxygen-permeable and bioinert polymer. Although LiPc-PDMS or similar probes have been used in repeated spectroscopic or average oxygen measurements using continuous wave electron paramagnetic resonance (EPR) since the late 1990s and now have advanced to clinical applications, they have not been used for pulse EPR oxygen imaging. One LiPc-PDMS probe of 2 mm diameter and 10 mm length was implanted in SC or IP sites (left or right side) in each animal. The pO2 imaging of implanted LiPc-PDMS probes was performed weekly for 6 weeks using O2M preclinical 25 mT oxygen imager, JIVA-25™, using the pulse inversion recovery electron spin echo method. At week 6, the probes were recovered, and histological examinations were performed. We report in this study, first-ever solid probe oxygen imaging of implanted devices and pO2 assessment of SC and IP sites.
Impact statement
In vivo implantation of tissue grafts and cell encapsulation devices in small animal models are commonly used to investigate the efficacy of these devices. It is important that the implantation site provides oxygen and nutrient for survival and early development of implanted grafts. Two most commonly used sites are subcutaneous and intraperitoneal. This study investigated the native partial oxygen pressure of these two sites using oxygen imaging of solid LiPc probe over the period of 6 weeks. This is the first such study to the best of our knowledge that provides oxygen maps of implanted probes at these sites.
Introduction
Tissue engineered grafts and cell encapsulation devices have significant potential to improve human health.1–3 These devices are used for the clinical applications to avoid immunological attack by blocking the immune cell while allowing the diffusion of oxygen and nutrients as well as secreted hormones without compromising function. Multiple medical fields, such as type 1 diabetes, cartilage, bone, brain, and heart injuries, and so on, are using these devices in preclinical experimental models to optimize therapies.4–11 The site of transplantation is a factor that has profound effect on graft survival. The ideal chosen site should be easy to access for implantation and retrieval while providing adequate diffusion of nutrients and oxygen for support of cell survival until vascularization is established. Although multiple sites have been tested for graft implantation in experimental models, no consensus exists in the literature about the optimum implantation site.
The two most commonly used sites for implantation of tissue grafts and cell encapsulation devices are subcutaneous (SC) and intraperitoneal (IP).3–5,12–15 Although there are assumptions about the typical partial oxygen pressure (pO2) of these sites, no reliable data are available. Oxygenation could vary between these two sites. Therefore, it is important to know the pO2 levels at these two sites over time that could be used for choosing the appropriate implantation sites. The aim of this proof-of-concept study was to determine the native pO2 of SC and IP sites in mice.
Electron paramagnetic resonance oxygen imaging (EPROI) is becoming a well-known pO2 mapping technology in tissue grafts and cells encapsulation devices.14–19 Most of the EPROI developments in the past decade are based on trityl-based oximetry and rely on the linear relationship between the pO2 and spin–lattice and spin–spin relaxation rates (R1 and R2) of a soluble spin probe such as trityl OX063 or its deuterated analog OX071.20–24 However, there are cases when the use of trityl/solution oxygen probe is not optimal and the use of solid probe for oxygen imaging is potentially beneficial for oxygen measurements, such as, when repeated oxygen measurements are needed or when the site is not accessible through perfusion for trityl. In these cases, it is useful to utilize a solid particulate electron paramagnetic resonance (EPR) oximetry probe such as lithium phthalocyanine (LiPc), lithium naphthalocyanine (LiNc), and lithium octa-n-butoxynaphthalocyanine (LiNc-BuO) that have been established in the field for spectroscopic pO2 measurements.25–28 These crystalline probes have been proved to be extremely useful for repeated and reliable oximetry. 29
The use of LiPc crystalline probe as oxygen sensitive EPR probe was first reported in early 1990s. 30 Later, similar other particulate probes such as LiNc and LiNc-BuO were reported27–31 The effect of dissolved molecular oxygen in broadening of EPR spectral line widths of particulate probes is utilized for oxygen measurement with these probes. In literature reports, LiPc exhibited two different forms: a tetragonal of space group P4/nnc, with a = b = 19.6 Å, c = 6.4 Å and a tetragonal of space group P4/mcc, with a = b = 13.8 Å, c = 6.403 Å (25). The literature report suggests that P4/nnc structure gives a pO2-independent EPR signal (300 mG), whereas the P4/mcc structure gives a pO2-dependent EPR signal (20 mG to 1.3 G). 25 Although these materials are very stable and minimally toxic in tissues that can be used directly for experiments with animals, because of the potential for using them in human subjects, the spin probe materials have been encapsulated in biocompatible, oxygen permeable polymers to increase future clinical applications and acceptance.27,31,32
Most of the oxygen measurements using encapsulated probes in the past decades were spectroscopic, providing a single average pO2 value. However, pO2 imaging using large, encapsulated probes will provide information on the heterogeneity of the implanted location as well as visualize multiple locations if more than one probe is implanted at the same time. In this study, we performed the pulse EPROI measurement of an LiPc-polydimethylsiloxane (PDMS) probes. We constructed a solid, cylindrical shape LiPc-PDMS oximetry probe (10 mm length and 2 mm diameter) that is implantable and retrievable. One probe was implanted into the SC or IP site in C57BL/6 mice with a minimally invasive procedure and pO2 was measured once per week for 6 weeks using O2M preclinical oxygen imager, JIVA-25™. In this study, we report in vivo pO2 imaging of LiPc-PDMS probes implanted in mice at SC and IP sites. To the best of our knowledge, this is the first such report of native pO2 of these sites in mice.
Materials and Methods
Fabrication of LiPc-PDMS spin probe
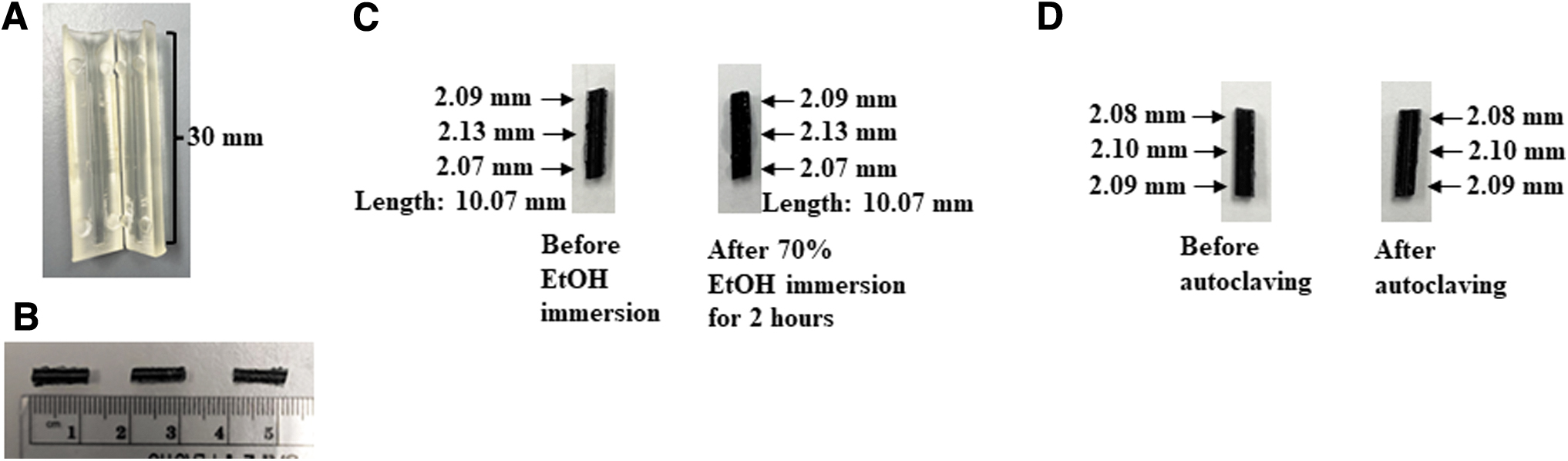
The LiPc crystals were purchased from Clin-EPR, LLC. The PDMS elastomer (A-103), crosslinker (A-103-C), and platinum accelerator (A-317) were purchased from Factor II, Inc. (Lakeside, AZ). LiPc-PDMS probes with 10 mm length and 2 mm diameter containing 20 mg LiPc were fabricated following the published protocol with few modifications. 33 In brief, 30 mm long and 2 mm diameter molds were three-dimensional (3D) printed using Formlabs clear resins (Catalog No. RS-F2-GPCL-04, dynamism) printer (Fig. 1A). PDMS elastomer and crosslinker were weighed (wt./wt.) at 10:1 ratio and mixed on the glass Petri dish using spatula for 2 min and crystals of LiPc were thoroughly dispersed into this mixture and mixing was performed for 7 min. A drop of platinum accelerator was added to the slurry and immediately degassed under vacuum.
LiPc-PDMS probe structure and sterilization.
The vacuum was applied for 5 min continuously followed by repeated cycles of applying and removing the vacuum for 5 min. The vacuum was released gently to burst the large bubbles that formed within the slurry while the slurry was subjected to negative pressure. Tiny air bubbles were burst manually using a 27G needle. The degassed slurry was spread in the foldable mold, secured with tape to prevent leakage of the slurry while curing, and then cured in an oven at 70°C for 18 h. The 30 mm long cured probe was then removed from the mold and 10 mm sections were cut to generate the final probes (10 mm length × 2 mm diameter; Fig. 1B). The probes were found to be stable and did not change their dimensions, including sterilization in 70% ethanol for 2 h (Fig. 1C) or 20 min autoclaving (Fig. 1D).
Oxygen imaging measurements
All pO2 measurements (spectroscopic and imaging) experiments were performed using a low-field 25 mT (resonance frequency 720 MHz) instrument, JIVA-25™, developed by O2M Technologies, LLC. JIVA-25 provides spatial and temporal pO2 maps in vitro and in vivo with high spatial (0.25 mm × 0.25 mm × 0.25 mm), temporal (1–10 min), and pO2 resolution (∼1 torr at hypoxic conditions and 3–5 torr at normoxic conditions).
Preparation of mice for pO2 measurements
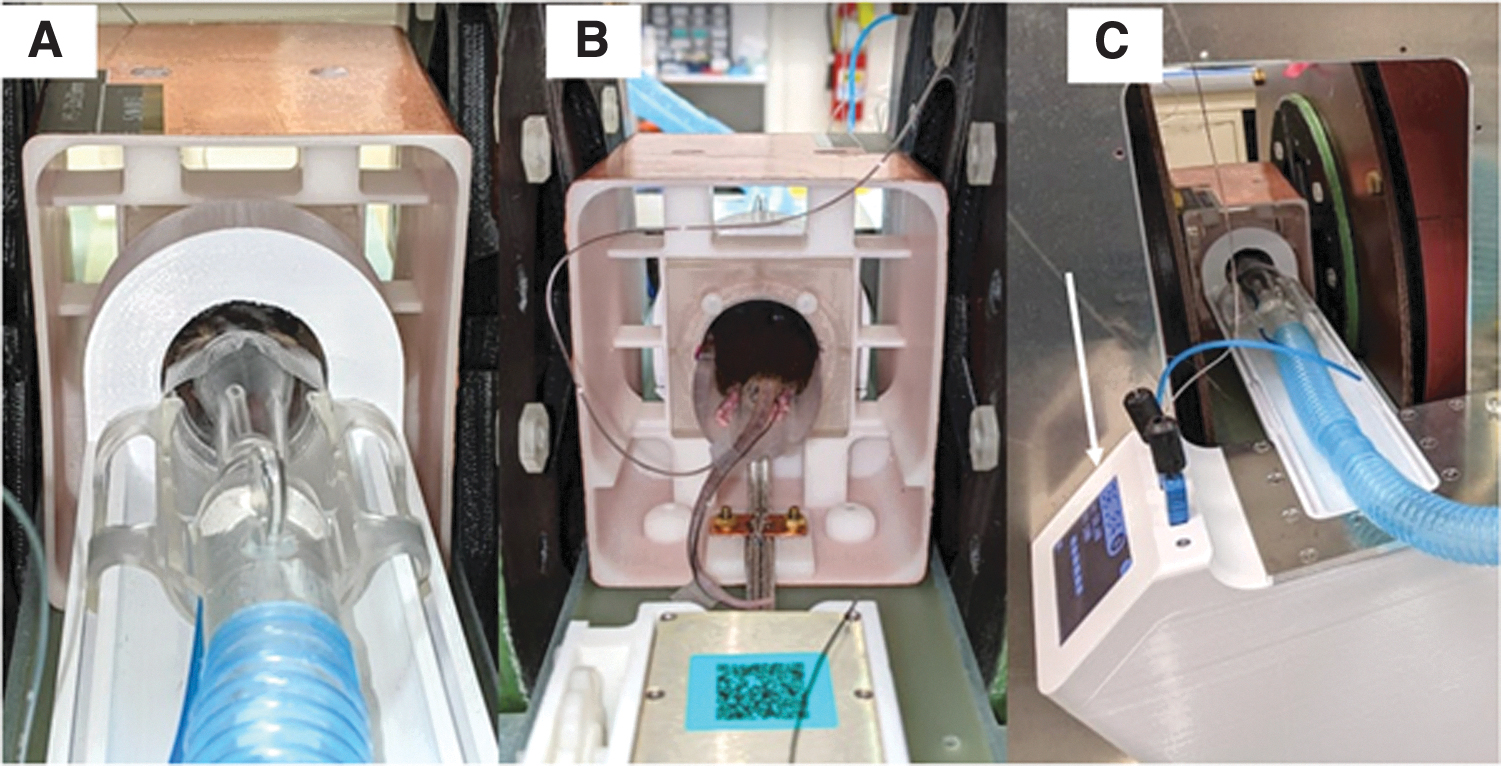
The mice were anesthetized with an isoflurane-medical mixture (1.5 L/min). Anesthetized mouse was laid on the cradle ventrally. Head of the mouse was held into the anesthetic nose cone using tape. The chest cavity of mouse was gently pressed against the breathing pad detector and secured to the cradle by tape so that rate of breaths per minute (bpm) can be detected on the monitor. Rectal probe was inserted and secured with the tail using tape. Both heartbeat line and rectal probe were connected to the vital monitor. After validating the breathing rate (90–110 bpm) and body temperature (37°C), the cradled mouse was moved immediately to the 32 × 35 mm mouse resonator in JIVA-25 (Fig. 2A, B). At the machine, anesthesia line was connected to the isoflurane vaporizer, breathing monitor and temperature probe was connected to the vital monitor installed on JIVA-25 as given in Fig. 2C.
An animal being imaged using
Mice
All animal experiments were performed under an approved protocol from the University of Illinois at Chicago Institutional Animal Care and Use Committee (UIC IACUC). Male C57BL/6 mice (n = 4) were obtained from Jackson Laboratories (Maine, ME). Mice were received at 7 weeks of age and housed for 1 week for acclimatization in a humid- and light- (12 h light/12 h dark) controlled room. Food and water were allowed ad libitum.
Implantation of LiPc-PDMS probes
Sterile LiPc-PDMS oximetry probes were (one per animal) implanted subcutaneously and into the IP cavity of 8-week-old mice either on the left or right side. Right and left was designated when a mouse is in a prone position, that is, anatomical right and left. The mice were designated mouse No. 1,SC,R, mouse No. 2,SC,L, mouse No. 3,IP,R, and mouse No. 4,IP, L where R and L stand for right and left side (Supplementary Fig. S1). Mice were anesthetized under isoflurane inhalation with a flow rate of medical air at 2.0 L/min.
In brief, the hair was removed at the site of implantation, and the skin cleaned by betadine scrubbing followed by wiping with 70% ethanol. A small transverse incision (4–5 mm) was made either at the right lower quadrant or left lower quadrant. An SC pocket was made using a sterile blunt probe and then a LiPc-PDMS probe was implanted gently, and incision was closed with 4-0 monofilament nonabsorbable nylon suture. For IP, the probe was inserted either into the right or left part of the peritoneum cavity and sutured as mentioned previously. The sutured skin was allowed to heal for at least 24 h before making EPR measurements. pO2 imaging was performed once per week for 6 weeks using JIVA-25.
Histology and immunostaining
At the end of the week 6 oxygen measurement, mice were killed. The LiPc-PDMS probe along with surrounding tissues were recovered. For SC implantations, accompanying and surrounding tissues were excised and in the case of IP implantation, tissues that attached to the probe were harvested. Probes were gently removed from the tissue using a sterile surgical blade. Tissues were fixed in 10% neutral-buffered formalin for 24 h followed by 70% ethanol for another 24 h. Tissues were processed, embedded, and sectioned at Research Histology Core at the University of Illinois at Chicago. Slides were stained with hematoxylin and eosin stain (H&E) for the histology.
Immunofluorescence staining was carried out to check for possible probe-induced vascularization and foreign body reaction. The antibodies used for the endothelial marker was CD31 (American Research Product, Catalog No. DIA-310) and for the fibrotic reaction it was fibroblast activation protein (FAP; Catalog No. PA5-99313; ThermoFisher). The secondary antibody used for the CD31 was Alexa Fluor 488-conjugated Affinipure Anti-Rat IgG (Catalog No. 712-545-153; Jackson Immunoresearch) and for FAP it was rhodamine (TRITC)-conjugated Affinipure Anti-Rabbit IgG (Catalog No. 711-025-152; Jackson Immunoresearch). Finally, mounting media containing 4′,6-diamidino-2-phenylindole (DAPI; Catalog No. F6057; Fluoroshield, Sigma) was used and cover slipped. H&E images were acquired by inverted light microscope (Leica DMi1) and fluorescent images were taken by inverted fluorescent microscope (Olympus BX51). Image quantification was carried out using ImageJ software.
Statistics
The p-values for the CD-31 quantification were calculated using an unpaired, one-tailed t-test on MS Excel. Significance was established for differences with values of p < 0.05.
Experiment
LiPc-PDMS probe calibration
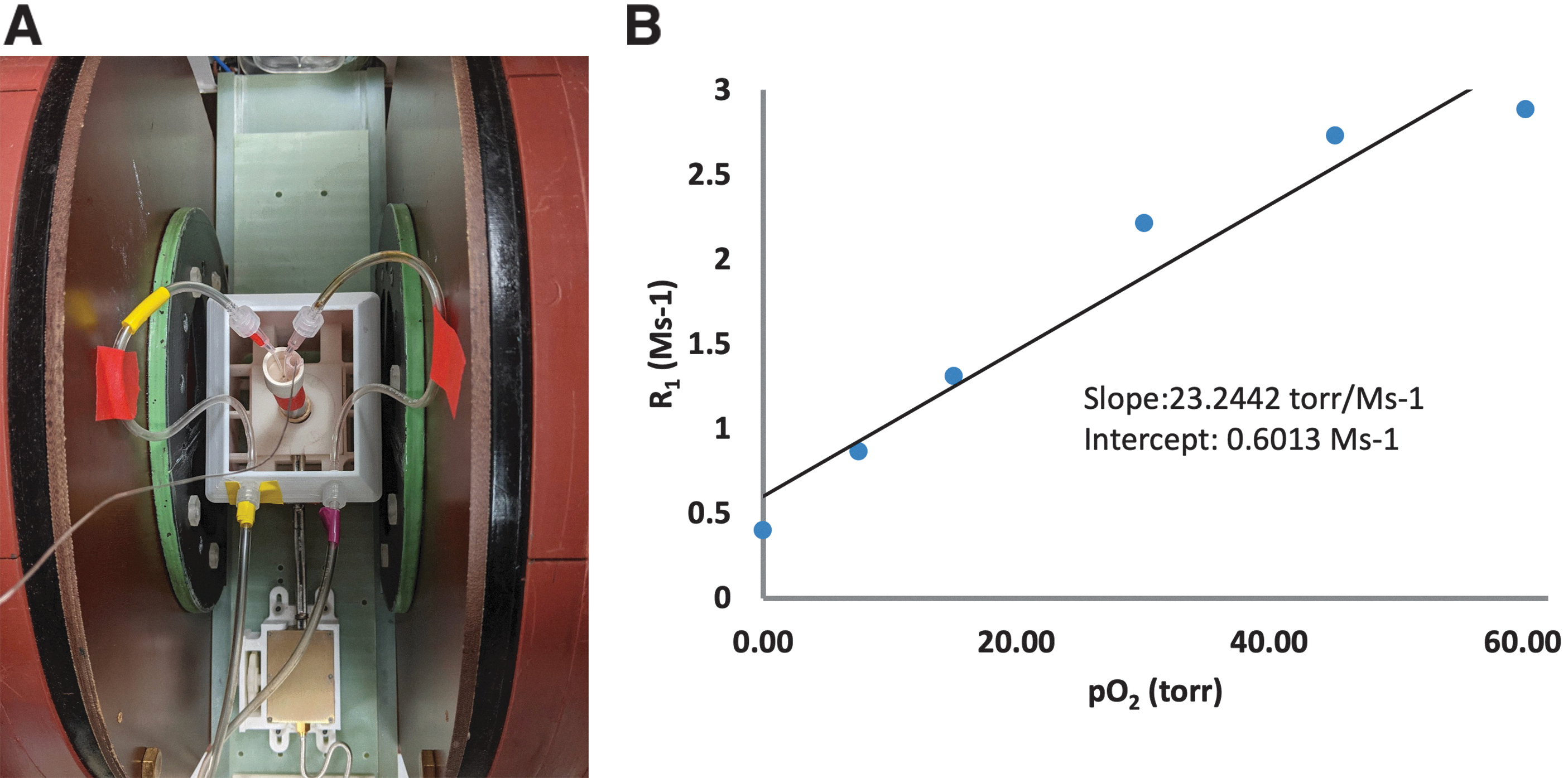
The pO2 calibration of the LiPc-PDMS probe were performed by placing a probe in a 10 mm tube in JIVA-25, 16 × 32 mm horizontal resonator as given in Figure 3A and bubbling the gas mixture (room air and N2) to achieve the final desired equilibrium oxygen concentration between 0% and 8%. The Spectroscopic T1 provides average pO2 values and was used for obtaining pO2 versus R1 calibration. The experimental parameters were as follows: pulse sequence: inversion recovery electron spin echo (IRESE), pulse lengths 60 ns, 8-phase cycles scheme with free induction decay (FID) suppression, spin echo delay 500 ns, 80 logarithmically spaced delays from 350 ns to 40 μs, 55 μs repetition time with 0, 1%, 2%, 4%, 6%, and 8% oxygen concentration. Relaxation rates (R1 = 1/T1) were calculated using a single exponential fit. The curves were fitted using single exponential recovery to extract spin–lattice relaxation rates R1 (1/T1) values that were converted to pO2 (Fig. 3B). The pO2 calibration details are as follows: O2 relaxation rate at 0 mmHg was 0.6013 × 106 s−1, with a slope of 23.2442 × 10–6 mmHg s−1.
Oximetry probe calibration.
Oxygen imaging
The pO2 imaging of LiPc-PDMS probes were performed using IRESE imaging sequence with THE following parameters: pulse lengths 60 ns, 8-phase cycles scheme with FID suppression, spin-echo delay 400 ns, equal solid angle spaced 654 projections, 67 baselines, 1.5 G/cm gradient, 8-time delays from 410 ns to 15 μs, 55 μs repetition time, overall, 10 min image duration. R1 (1/T1) images were reconstructed using filtered back projection in isotropic 64 × 64 × 64 cube with 0.66 mm voxel linear size. The R1 maps were calculated voxel by voxel by fitting data to the single exponential fit and converted to pO2 maps using the calibration values obtained from the calibration experiment. 21
Experimental Results
pO2 map
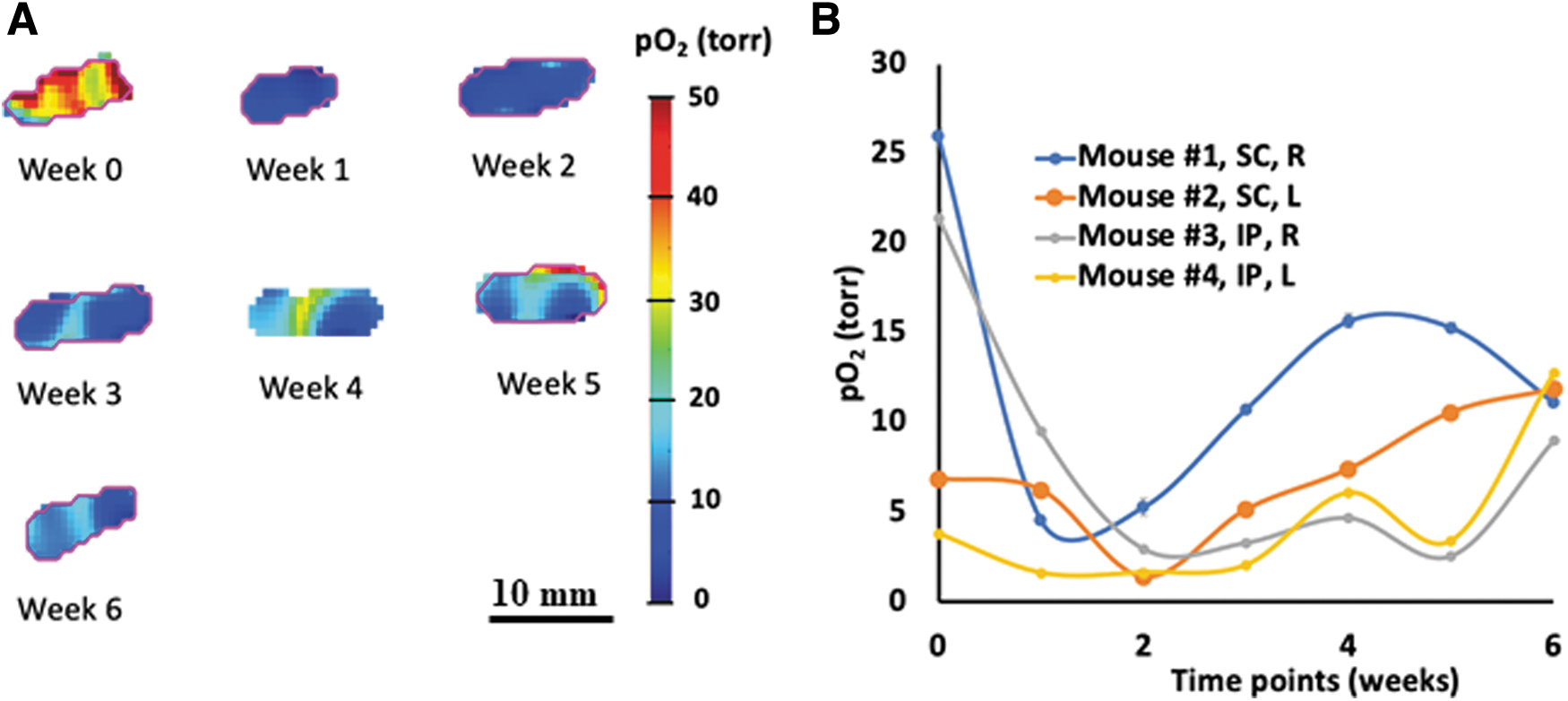
Figure 4A provides an example of pO2 map set for mouse No. 1 with left SC implant. Similar maps were obtained for all animals. These maps demonstrated the ability of JIVA-25 to obtain repeated pO2 maps of in vivo tissue oxygenation at SC and IP sites using pulse EPROI. Figure 4B provides the average pO2 as a function of time for all animals. Mouse No. 1 (Right SC) and No. 3 (Right IP) showed normal pO2 at week 0, whereas mouse No. 2 (Left SC) and No. 4 (Left IP) were hypoxic at this time point. At subsequent weeks (weeks 1–5), probes were hypoxic in all mice except mouse No. 1 and by the sixth week, moderate oxygenation was observed for all animals. The pO2 levels between mouse 3 (right IP) and mouse 4 (left IP) showed a significant difference at week 0; however, this difference became insignificant by week 6 (Fig. 4B). No significant difference in pO2 levels was observed between SC and IP sites at week 6. Table 1 provides weekly pO2 values.
Partial oxygen map of
Weekly Partial Oxygen Pressure Statistics of Implanted Probes in Subcutaneous or Intraperitoneal Cavity
Mean pO2 values was calculated from IRESE sequence obtained weekly for each mouse. Average voxels are indicated in parentheses.
IP, intraperitoneal; IRESE, inversion recovery electron spin echo; Lt., left; pO2, partial oxygen pressure; Rt., right; SC, subcutaneous; SE, standard error.
Histological analysis
In vivo stability of LiPc particulates has been reported earlier by other investigators (31–33). After completion of sixth week pO2 imaging, mice were killed and location of LiPc-PDMS probes in SC and IP were confirmed visibly (Fig. 5A–D). LiPc-PDMS probes were well tolerated by all animals. No sign of infection or rejection were observed in the implant location externally during the 6-week period of the experiment. Histological analysis showed slight inflammation in the muscle in subcutaneously implanted LiPc probes (Fig. 5A, B). Numerous nuclei at the interface represent polymorphonuclear leukocytes (PMNs; inset in Fig. 5A, B). The presence of PMNs demonstrates that the implant triggered an acute inflammatory response, which is normally expected of any foreign material that is implanted. As mentioned previously acute inflammatory response and subsequent formation of a fibrous tissue did not have any significant effect on the in vivo oxygen-sensing ability of the probe.
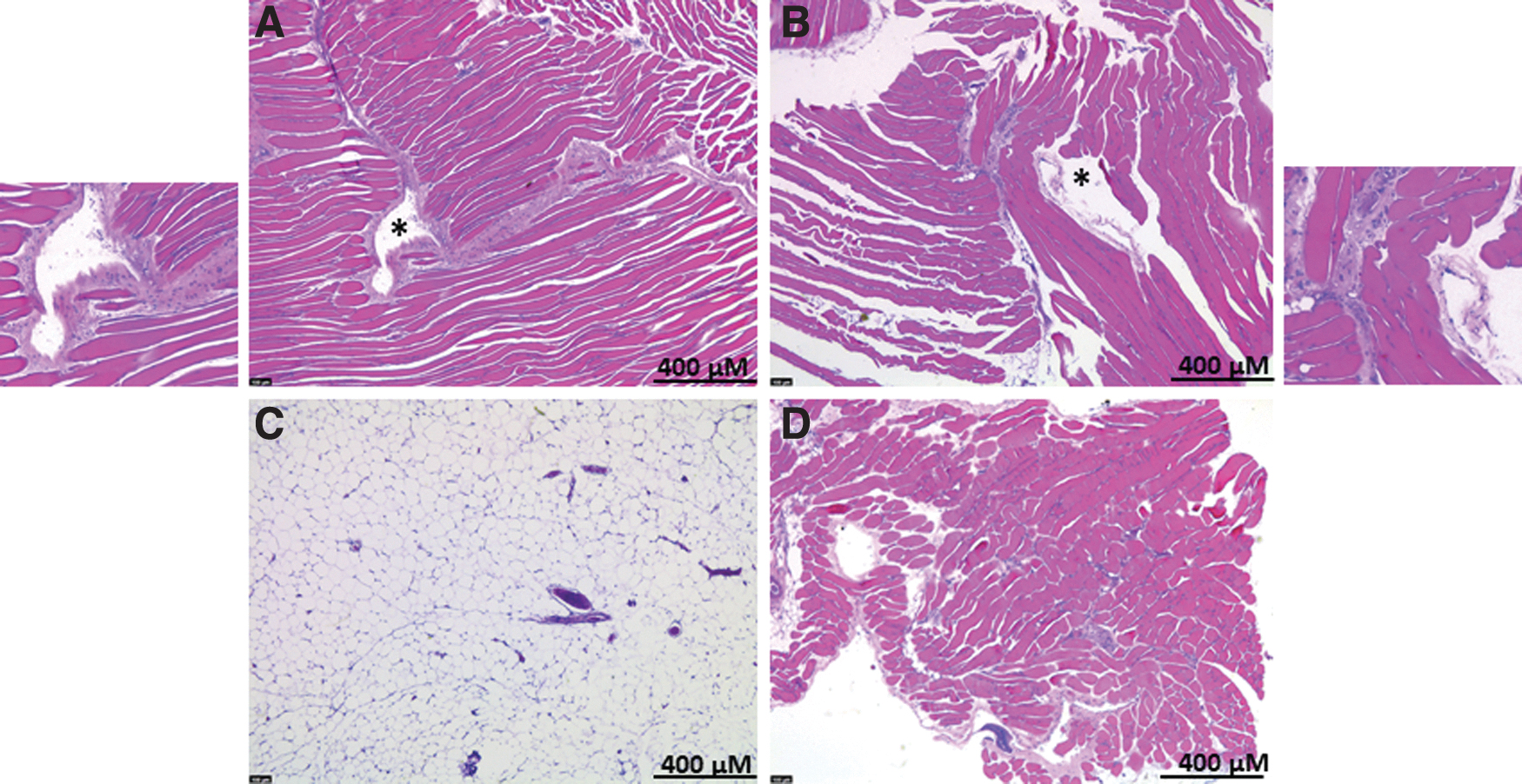
Representative images of H&E staining showing histology of tissue where LiPc-PDMS probe was implanted for 6 weeks. Subcutaneously implanted oximetry probe in mouse No. 1, right SC
The SC implants were enveloped by a fibrous capsule between the skin and muscular layer at the time of excision. The IP implant was found to be engulfed within adipose tissue in mouse 3 (right, IP) and it was adherent to the visceral organs in mouse 4 (left, IP) (Supplementary Fig. S2). Further examination revealed that the LiPc probe in mouse 4 was adhered to the pancreas, colon, and muscle (Supplementary Fig. S3). There was no impact of the SC or IP milieu on the dimension of cylindrical probe.
LiPc probe induced vascularization
We also evaluated for any possible LiPc-induced vascularization in SC and IP tissues using an endothelial marker, CD-31. Figure 6A shows staining for the blood vessels in the probe implanted area that was quantified by ImageJ (Fig. 6B, C). No apparent difference in staining was noted between SC-implanted probes in mouse 1 and mouse 2. A significant difference was found between IP-implanted probes (Fig. 6) where probe embedded in the fatty tissue in mouse 3 (right, IP) had lower CD-31-positive cells compared with mouse 4 (Left, IP). Average of pancreas, muscle, and colon was taken for quantification in mouse 4 (Supplementary Fig. S3). Staining showed several CD-31-stained vessels in muscle. However, this early vascularization did not improve pO2 of devices.
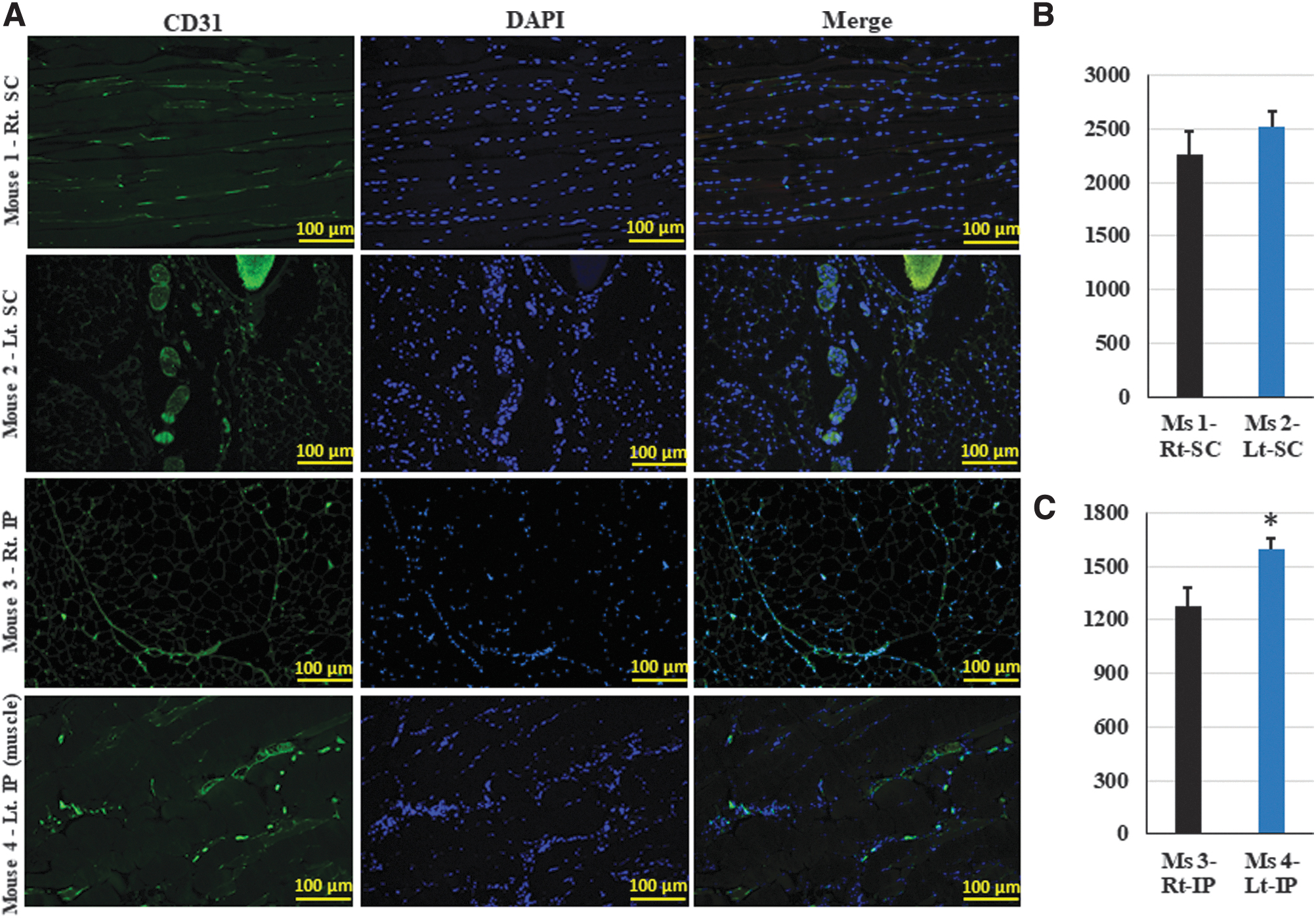
Effect of LiPc-PDMS probe on vascularization in SC and IP sites.
Discussion
This proof-of-concept study shows the ability of repeated pO2 imaging using solid LiPc-PDMS probe implanted in SC and IP sites in mice. The milieu in both compartments is different, which warrants evaluating pO2 that would be available for the survival of implanted cells. Although there was a significant difference between the sites at week 0, at the end of 6-week study, both SC and IP sites did not have significant difference in pO2 values. Weekly pO2 data suggest that LiPc probes were equally capable of measuring oxygen in SC and IP; however, probe in the IP cavity recorded more variations. There was a subtle but significant difference in the pO2 between right and left side in IP.
Oxygen imaging provides 3D oxygen profiles and can shed light into spatial heterogeneity of the implantation sites. We noticed that pO2 maps of implanted probe were heterogeneous in all cases as evident from the pO2 maps of a device for 6 weeks as given in Figure 4. The spatial heterogeneity in an implanted graft may come from the proximity to a blood vessel, generation of new blood vessels during the study period, change in biomaterial characteristics, or from fibrosis developed around the graft that may deplete the oxygen supply. These conditions and therefore oxygenation of the graft is a dynamic process and change throughout the implantation period. Each of these situations is a common occurrence for a tissue graft in a course of a typical implantation period; therefore, oxygen imaging could prove to be a vital tool for tissue graft assessment.
Conclusion
To the best of our knowledge, this is the first time that EPR oximetry has been applied to investigate in vivo oxygenation kinetics of SC and IP sites in mouse model. Our experimental results showed that JIVA-25 is capable of repeated pO2 imaging with solid LiPc-PDMS probe using pulse EPR oximetry. The pO2 data show that the average oxygen remained low throughout the study period, and there was no significant difference between SC and IP sites.
Footnotes
Authors' Contributions
N.V.: Experiment design, methodology, data interpretation, writing—original draft preparation. E.S., S.P., and S.H.: Experiment, methodology. W.S. SOP for preparing LiPc-PDMS probes. H.M.S.: Discussion and data interpretation. B.E.: Data interpretation, software validation. M.K.: Conceived idea, experiment design, data interpretation, writing—reviewing and editing.
Acknowledgment
The authors thank Research Histology and Fluorescence Imaging facility at the University of Illinois at Chicago.
Disclosure Statement
No competing financial interests exist.
Funding Information
The study received funding support of JDRF through research grant to O2M (PI: M.K., Grant No. 3-SRA-2020-883-M-B).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.