
Abstract
Tooth loss greatly affects a person's quality of life and many turn to dental implants to replace lost teeth. The success of a dental implant depends on the amount of alveolar bone supporting the implant, and thus, bone augmentation is often necessary to preserve or build up bone volume in the alveolar ridge. Bone can be augmented with autogenous bone, allografts, or xenografts, but the limitations of such natural bone grafts prompt researchers to develop synthetic scaffolds supplemented with cells and/or bioactive agents as alternative bone grafts. The translation of these combination scaffolds from the laboratory to the clinic requires reliable experimental models that can simulate the clinical conditions in human patients. In this article, we describe the use of a porcine alveolar defect model as a platform to evaluate the efficacy of a novel combination of a three-dimensional-printed polycaprolactone-tricalcium phosphate (PCL-TCP) scaffold and adipose-derived mesenchymal stem cells (AD-MSCs) in lateral alveolar augmentation. The surgical protocol for the defect creation and regenerative surgery, as well as analytical methods to determine the extent of tissue regeneration, are described and discussed.
Impact statement
There is a huge global demand for bone grafts and bone regeneration procedures due to increasing cases of bone damage, bone disease, and tooth loss. The availability of a customizable bone graft that avoids issues such as donor-site morbidity for autografts and risks of immunological reactions and disease transmission for allografts and xenografts would be highly desirable. To study the safety and efficacy of novel bone regeneration implants and procedures, a reliable animal model is needed. In this article, we describe the use of a porcine alveolar defect model as a clinically relevant model to evaluate the efficacy of a bone regeneration implant for alveolar augmentation. Our model is applicable to a variety of scaffolds and cell types and will support the translation of novel implants into clinical applications.
Introduction
Teeth are sensory organs that have important function in aesthetics, chewing, and speech, and the loss of teeth due to caries, periodontal disease, and trauma can negatively affect a person's quality of life. 1 Many people with tooth loss turn to dental implants as the treatment of choice for tooth replacement, as dental implants can often reliably restore oral function and aesthetics. With increasing awareness and acceptance of dental implants among the public, dental implants and their respective parts and tools have become the fastest growing area in dentistry and the dental supply industry, with the global dental implant market valued at USD 3.66 billion in 2020 and expected to reach USD 5.71 billion in 2028 at a compound annual growth rate (CAGR) of 6.2% from 2021 to 2028. 2
The long-term success of a dental implant depends on the amount of bone supporting the dental implant in the alveolar ridge. 3 Following a dental extraction, the tooth socket would undergo physiologic resorption, resulting in substantial reduction of the height and width of the alveolar ridge. A systematic review reported a bone height reduction of 11–22% and a bone width reduction of 29–63% in the alveolar ridge at 6 months after dental extraction. 4 Excessive bone resorption not only causes significant aesthetic problems, but also contributes to a lack of support to the dental implant, eventually causing implant instability and loosening. Hence, bone augmentation is needed in such cases.
Grafts for bone augmentation may be derived from natural sources, for example, autograft (bone isolated from another part of the patient's body), allograft (bone isolated from another human), or xenograft (bone isolated from another animal species). As naturally derived materials have batch variability and risk of disease transmission, there is increasing attention on synthetic materials for bone grafting.
One synthetic material that we have identified to be a suitable bone graft material is polycaprolactone (PCL). 5 PCL, a bioresorbable, nontoxic, and biocompatible polymer, has been used in medical devices approved by the Food and Drug Administration (FDA), that is, implants, drug delivery devices, sutures, and bone fillers.6,7 PCL can be three-dimensional (3D) printed into scaffolds with customizable shape, size, and porosity, providing abundant surfaces for cell attachment. 8 Such 3D-printed PCL scaffolds have mechanical properties similar to bone, exhibit slow degradation kinetics, and enhance blood clot entrapment and vascular ingrowth.9,10
The bone regenerative capability of the scaffolds can be further improved by blending bioactive minerals such as tricalcium phosphate (TCP) with the bulk scaffold material, as well as loading osteogenic cells or stem cells, which can release osteogenic factors and promote bone formation within the scaffold. While the combination of 3D-printed scaffold and stem cells has been studied and reported for a number of clinical applications, there is limited information on the use of a scaffold–stem cell combination in dental applications. 11
To investigate the clinical feasibility of a scaffold–stem cell combination and validate its efficacy in dental applications, researchers need reproducible, controllable, and affordable experimental models that can simulate the clinical conditions in human patients. 12 Since in vitro systems can never fully reproduce the anatomical complexity of the oral-maxillofacial region, an appropriate animal model recapitulating a similar bone anatomy and healing process to that in humans is necessary. 13
In this article, we describe the use of a porcine alveolar defect model as a platform to evaluate the efficacy of the combination of a 3D-printed polycaprolactone-tricalcium phosphate (PCL-TCP) scaffold and adipose-derived mesenchymal stem cells (AD-MSCs) in lateral alveolar augmentation. Porcine models have been utilized for years in biomedical research and preclinical studies due to the physiological similarities between pigs and humans. 14 Although pigs have a higher bone mass and a thicker trabecular bone than humans, porcine bone tissue has a similar lamellar structure and remodeling rate to that of humans. 15 Hence, the porcine alveolar defect model is a relevant model that simulates the alveolar bone resorption and subsequent regenerative treatments seen in human patients.
Although we are using PCL-TCP scaffolds and AD-MSCs, the protocol that we are describing is also suitable for a variety of scaffold materials with customizable shapes and sizes, as well as stem cells from a variety of sources. We describe the surgical protocol for the defect generation and regenerative surgery, as well as analytical methods to determine the extent of tissue regeneration.
Overview of the Procedure
The procedure consists of two surgeries, as illustrated in Figure 1. In the first surgery, after the animal is anesthesized, bilateral mandibular mucoperiosteal flaps from the first premolars to the first molar are raised and the four premolars are extracted by sectioning the roots to ensure preservation of the cortical bone. Primary closure is performed with sutures and the extraction sites are left for 3 months to induce bone resorption. In the second surgery (3 months after the first surgery), the animal is anesthesized again and 30 mL of lipoaspirate is extracted from the abdominal subcutaneous adipose tissue.
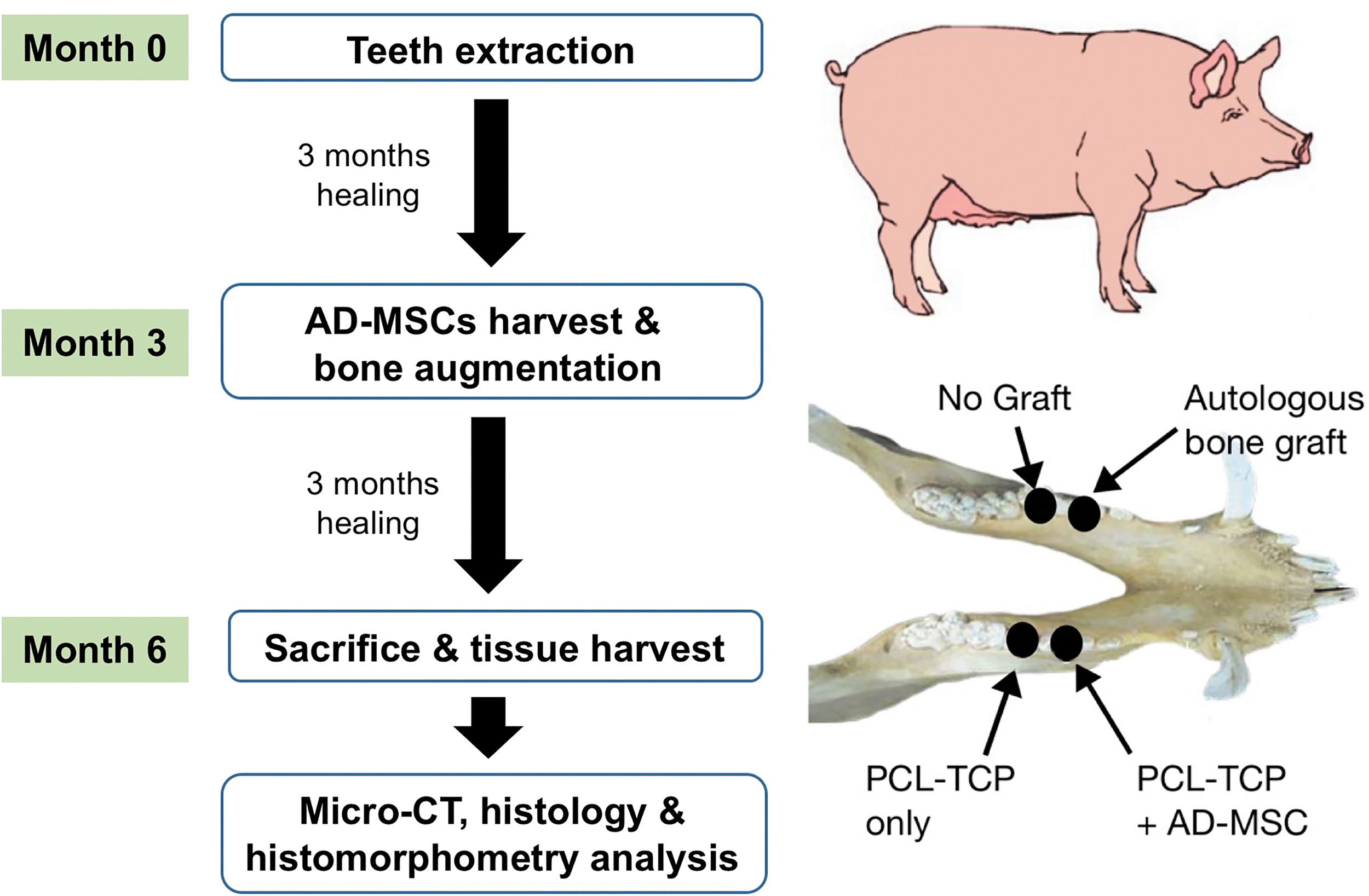
Schematic diagram for the workflow of procedure.
The lipoaspirate is processed using the AdiPrep® system to yield 2 mL of stromal vascular fraction (SVF), a concentrated cellular extract of adipose tissue containing a heterogenous population of AD-MSCs, stromal cells, and immune cells. 11 The SVF is then loaded into a porous 3D-printed PCL-TCP scaffold measuring 8 × 8 × 3 mm.
The high concentration of AD-MSCs in the SVF makes SVF suitable for autologous implantation within the same surgery without the need for cell expansion, while the porous structure of the PCL-TCP scaffold supports the proliferation of the SVF cells and the osteogenic differentiation of the AD-MSCs. Meanwhile, the bilateral mucoperiosteal flaps at the previous extraction site are raised again. Four defects of 8 mm × 8 mm (two each on the left and right sides of the mandible) are created on the buccal side of the alveolar ridge using drill burs, and each site is randomly selected to receive one of the following: (1) scaffold with cells, (2) scaffold without cells, (3) autologous bone (harvested from the drilling of the other defects), and (4) no graft. Each defect site is covered with a collagen membrane before the periosteum is closed using sutures.
The animal is euthanized after 3 months, and the tissue block containing the defects is harvested and analyzed by microcomputed tomography (micro-CT) and histology.
Experimental Design
Scaffold
A number of synthetic materials, such as alloys, ceramics, and bioactive glass, have been used as grafting materials in bone regeneration, but synthetic polymers are more popular due to their ease of processing, better reproducibility, and controlled degradation rate. In particular, aliphatic polyesters—such as poly(lactic acid) (PLA), poly(glycolic acid) (PGA), poly(lactic-acid-co-glycolic acid) (PLGA), and PCL—are the most common class of synthetic polymer in bone tissue engineering as their biocompatibility is well-reported and their use is supported by long-term clinical data. Aliphatic polyesters are easy to process, have comparable mechanical properties to human tissues, and are biodegradable with the breakdown products naturally cleared by the host's metabolic pathways. 16
PCL is the polymer of our choice due to PCL's longer degradation time, high mechanical strength, and a relatively low melting point of 58–63°C, which allows PCL to be easily 3D printed into customized structures. 17 Bioactive minerals, such as TCP, can be blended with PCL to improve the biocompatibility of the material. The scaffold that we used in our study is a 3D-printed 80% PCL-20% TCP scaffold fabricated by Osteopore International Pte Ltd. via fused deposition modeling (FDM). The unique feature of these scaffolds lies in the three-angle layering (0°/60°/120°) that results in a fully interconnected matrix architecture that provides maximum anchorage for cell attachment.9,10,18 The scaffold shape can be customized to fit the shape of the defect, but for the simplicity of our procedure, the scaffold we use is a square block measuring 8 × 8 × 3 mm.
Cells
The loaded cells should ideally be autologous and isolated from tissues with a high yield of osteogenic cells or stem cells. Traditionally, bone marrow stem cells (BMSCs) are the earliest-known and most popular stem cell source for bone tissue engineering, but BMSCs are limited to their low cell yield, long expansion time, and difficult aspiration process. 19 Recently, AD-MSCs, which are capable of differentiating into all mesogenic lines including chondrogenic, osteogenic, and adipogenic cell lines, have been found to be more suitable than BMSCs in clinical applications due to their higher yield of cells (40-fold higher) in adipose extracts than bone marrow extracts. Moreover, the harvest method is less invasive and less painful, reducing donor-site morbidity.20,21
The high yield of stem cells in adipose extracts also allows AD-MSCs to be implanted into the patient in the form of SVF, without the need for cell expansion. The whole process of extraction, concentration, and implantation can be performed within the duration of the regenerative surgery, saving time and costs for the patient and clinicians.22,23
The use of AD-MSCs and SVF has been widely studied and reported for a wide range of preclinical and clinical applications, including treatments for autoimmune diseases, cardiovascular restoration, neurological regeneration, soft tissue reconstruction, and wound healing.11,21,24
While AD-MSCs and SVF have also been studied in oral-maxillofacial and dental applications, their actual adoption in the dental clinic remains limited, compared with the more established BMSCs, dental pulp stem cells, and periodontal ligament stem cells. 25 Nevertheless, the use of adipose SVF is expected to be more widely adopted by dental surgeons given that SVF can be obtained from adipose tissue via mechanical means without the need for tissue dissociation enzymes and cell culture media. This allows SVF to meet FDA's “minimal manipulation” requirement for fat graft implantation, thereby lowering the regulatory burden and production cost. 26
The graft obtained with this method also contains immune cells such as leukocytes, which secrete prohealing factors to encourage microvascular formation. In addition, the SVF graft also contains endothelial cells that further enhance angiogenesis. 21
As AD-MSCs gain attention in clinical applications, the harvesting and processing of AD-MSCs and SVF have become simpler and faster with the development and commercialization of adipose processing kits. To meet the FDA's “minimal manipulation” guidelines, collagenase-free methods using mechanical forces to breakdown the adipose tissue have been developed; Tulip Biologics® from Tulip Medical and AdiPrep from Terumo Blood and Cell Technologies (BCT) are the two commercially available products with this technology. 26 AdiPrep was selected for this project because it uses a proprietary lipid barrier disc technology, effecting cell isolation and oil and lipid separation in only 4 min.22,23 The rapid process shortens the surgery time without compromising the safety and effectiveness of the AD-MSCs.
Defect model
To simulate the conditions of a resorbed alveolar ridge in pigs, we perform tooth extractions in the pigs and leave the extraction sites to heal for 3 months.
In our original protocol, we followed the surgical method reported by Goh et al. 27 and created a cylindrical bone defect (7 mm diameter × 7 mm depth) at the crest of the alveolar ridge using trephine drills, causing complete destruction of the buccal cortical plate of the alveolar ridge. We then implanted a cylindrical scaffold (7 mm diameter × 7 mm height) into the defect. We performed this procedure on a trial pig, but 1 week after surgery we observed wound dehiscence and inflammation, and 1 month later we observed nonclosure of wound and exposure of implanted scaffold. We noticed that pigs tend to chew continuously, even in the absence of food. It is likely that the continuous chewing had caused the maxillary teeth to bite onto the crest of the mandibular alveolar ridge, resulting in wound dehiscence, exposure of the scaffold, and failure of the graft.
We did not have this issue when we performed the same procedure on monkeys (Macaca fascicularis) in a previous study, as monkeys do not have the constant chewing motion. From this experience with the first pig, we modified the design of the defect subsequently. Instead of implanting a cylindrical scaffold at the crest of the alveolar ridge, we performed a lateral alveolar augmentation by creating a square defect on the buccal side of the alveolar ridge and implanting a square scaffold (8 × 8 × 3 mm) into the lateral defect. This design avoided the traumatic biting of the wound by the maxillary teeth. The changes in the scaffold shape and implantation method are illustrated in Figure 2.
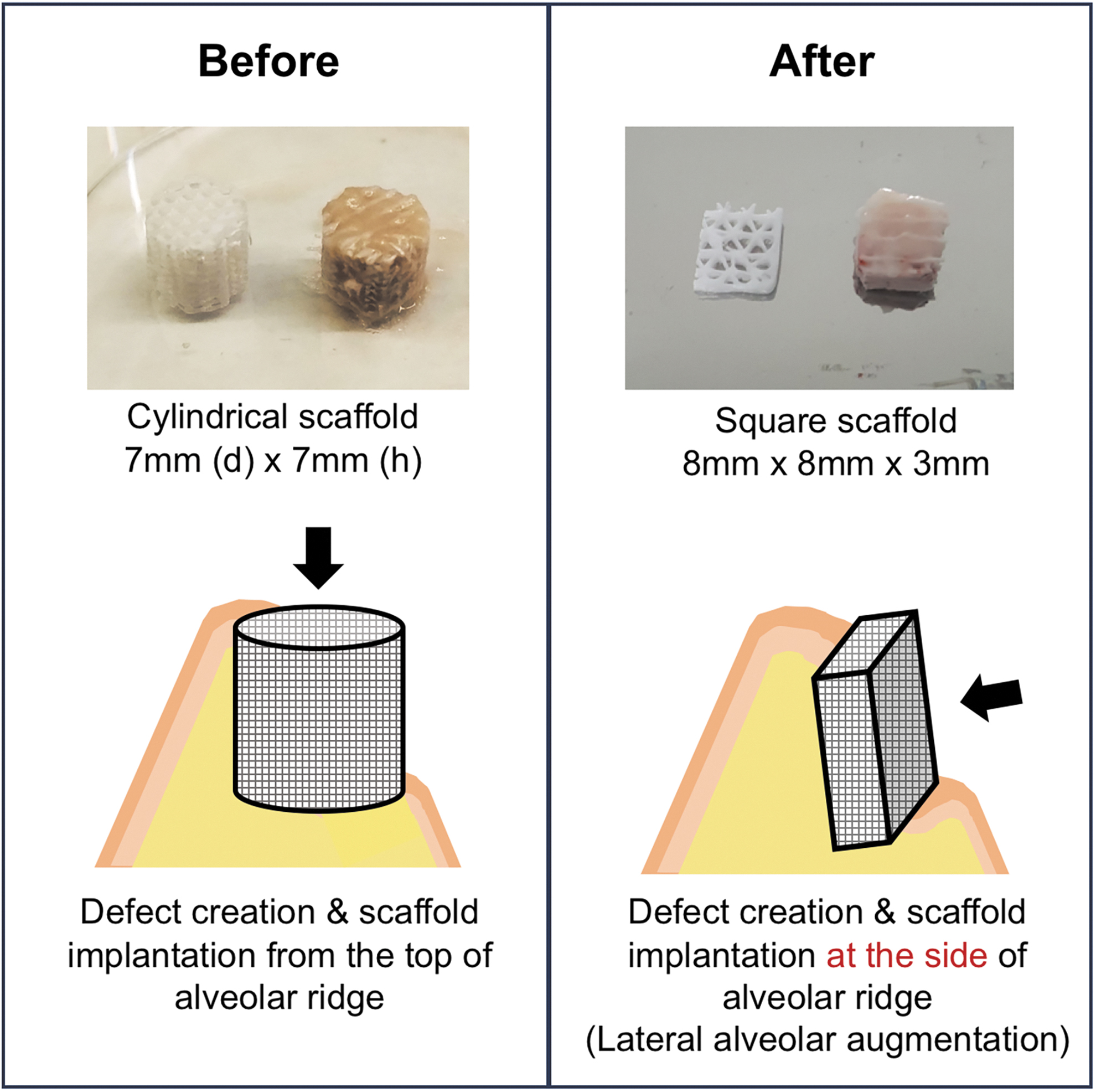
Schematic diagram of the changes in the scaffold shape and implantation method. In each of the two photographs, the left scaffold is the original scaffold, while the right scaffold is loaded with SVF. SVF, stromal vascular fraction.
After the augmentation surgery, we allow the surgery sites to heal for 3 months before we harvest the mandible for analysis. A postsurgery time point of 3 months in pigs represents midterm tissue regeneration and is a common time point for porcine oral maxillofacial regeneration studies. 28 The duration of the study can be adjusted based on the aim of the study (e.g., short-term or long-term regeneration) and the logistical conditions (e.g., funding, availability of animals). A time point of 1 month is common to study short-term tissue regeneration, while a time point of 6 months is common to study long-term tissue regeneration.
Animal
In this study, we used healthy male adult domestic pigs (Sus scrofa domesticus). The pig model is a suitable model for this study because of the similarities in size, anatomy, physiology, and genomic organization between pigs and humans. 14
The number and distribution of cells in pigs also closely resemble those in human. Pigs also have the advantage of being easily accessible as they are a popular food source. Their abundance of fat tissues, as well as the similar composition and distribution of fat tissues between pigs and humans, makes porcine AD-MSCs highly relevant in stem cell research. The osteogenic differentiation of porcine AD-MSCs has been well-studied and there are numerous studies demonstrating the suitability of porcine AD-MSCs in bone regeneration and osteochondral repair.29–31 In dental research, the similarity in size and anatomy between porcine teeth and human teeth allows the generation of defects with clinically relevant dimensions.
However, based on our observations, there are a few things to take note of when using pigs for this alveolar defect model. First, it is important to know the difference in dentition between pigs and humans, and also the time line of tooth development in pigs. Adult pigs with fully developed permanent teeth have four premolars and three molars on each side of the mandible, while adult humans have two premolars and three molars. 32 Hence, the alveolar ridge spanning the premolars is longer in pigs than in humans. The longer alveolar ridge in pigs provides us more space for defect generation and scaffold implantation, without affecting the chewing function of the canines and molars.
However, unlike humans where the eruption of permanent teeth occurs around puberty, the eruption of permanent teeth in pigs continues beyond sexual maturity (5–6 months), 33 with the eruption of the second to fourth premolar beginning at 16 months and the eruption of the molars beginning at 12 months. 34 For the purpose of this model, pigs should have full adult dentition, and hence, they should be at least 16 months of age. However, older pigs may have a problem of weight control as pigs can gain more than 10 kg per month after sexual maturity (5–6 months) before the weight plateaus after 18 months. 33
From the literature, a pig weighing 55 kg at 4 months can reach 130 kg at 8 months, 180 kg at 12 months, and 230 kg at 16 months. 34 The enormous weight of the animal may create ergonomic risks for the veterinary team when moving the animal, and also necessitates higher drug dosages for sedation, pain relief, and inflammation/infection control. A modification of diet provided in terms of amount and type may help to control the weight. Nevertheless, the pigs can still be relatively heavy, especially after they are kept for several months from the first surgery to sacrifice.
In this aspect, a better alternative to the domestic pig may be the miniature pig, which has been extensively used in many preclinical experiments including dental and orofacial research.35,36 Similar to domestic pigs, miniature pigs also possess similar anatomy and physiology to humans, and miniature pigs have the advantage of a manageable body weight (29–42 kg) with lower maintenance cost due to less food and drugs needed. However, as miniature pigs are mostly bred for research purposes and not as a food source, they are not as readily available as domestic pigs. Hence, the cost to purchase a miniature pig is higher than that for a domestic pig. As the eruption of the four permanent premolars and the first two molars in the mandible is complete by 15 months, 35 miniature pigs to be chosen for the study should be at least 15 months of age.
Besides pigs, nonhuman primates (NHPs) such as macaques are also common in dental and orofacial research due to similarities in dentition to humans. However, NHPs are not suitable in this study because they often lack sufficient subcutaneous adipose tissues, from which we can safely extract lipoaspirate.
Materials
Scaffold
A polymer mineral composite consisting of 80% PCL and 20% TCP is 3D printed into porous scaffolds with dimensions 8 × 8 × 3 mm by Osteopore International Pte Ltd. (Singapore) via FDM. The filaments are printed in a three-angle layering (0°/60°/120°) format, with a 2 mm gap between the filaments horizontally and a 1 mm gap between the layers vertically. The scaffolds are then individually packed, vacuum sealed, and sterilized by gamma radiation.
Animal
Adult male domestic pigs (S. scrofa domesticus) with complete adult dentition are used for this study. All animal procedures follow the guidelines of the American Association for Accreditation of Laboratory Animal Care (AAALAC) and are approved by the Institutional Animal Care and Use Committee (IACUC).
Equipment
The AdiPrep system from Terumo BCT, Inc. is used for the extraction and processing of adipose tissue. The AdiPrep system consists of the SmartPrep 2 machine, which is a centrifuge optimized for the concentration of SVF, and the AdiPrep disposable set (ADI-25-01), which consists of cannulas for lipoaspiration and a closed syringe system with a proprietary lipid barrier disc for adipose tissue processing. The AdiPrep disposable sets are presterilized by gamma radiation.
Surgical instruments and surgical gowns are sterilized using autoclave and allowed to cool at room temperature. Surgical consumables (e.g., scalpel blades, needles, syringes, and sutures) are obtained as presterilized.
Personnel
The surgery team consists of the following:
An experienced dental surgeon (sterile) to perform the extraction and implantation surgeries, as well as the lipoaspiration procedure. A surgery assistant (sterile) to support the dental surgeon in the surgeries and lipoaspiration. An assistant (sterile) to operate the AdiPrep system, isolate the SVF, and load the SVF into the PCL-TCP scaffolds while the surgeon and surgery assistant were creating the alveolar defects. An assistant (nonsterile) to support the opening of sterile packages, photography, and documentation. A veterinarian and one or two veterinary technicians to prepare, induce, and manage the anesthesia, reposition the animal during surgery, and postoperative management.
Protocol
Four weeks before the scheduled surgery, the experimental animals are trained to consume soft diets prepared daily by animal care personnel. The soft diet is also provided during the postoperative period. Enrichment toys made from hard materials are removed from the pen to prevent the animals from chewing on them, and exerting mechanical stress on the operated alveolar ridge.
Presurgical preparation
The animals are fasted overnight before each procedure to prevent regurgitation and vomiting during anesthesia and surgery.
Animal preparation for surgery
A pain reliever drug (up to 0.05 mg/kg buprenorphine) and antibiotics (6–8 mg/kg ampicillin/cloxacillin) are administered via intramuscular injection 30 min before surgery.
The pig is sedated with an intramuscular injection of ketamine (15 mg/kg), atropine 0.05 mg/kg (subcutaneously), and xylazine (1–5 mg/kg), which will be partially reversed by atipamezole of the same dose postsurgery.
The body weight is taken using the digital weighing scale and the animal is physically examined by the veterinarian.
Eye cream is applied to the eyes to prevent drying while under general anesthesia.
The veterinarian performs oral intubation using an appropriately sized endotracheal (ET) tube. The ET tube is secured using stainless steel wire #0.4 fixated onto upper incisor teeth.
A 21 G intravenous (IV) catheter is placed in the ear vein for fluid infusion (sodium lactate) with a flow rate of 10 mL/kg/h. The IV catheter is removed once the animal regains righting reflex at the discretion of the veterinarian.
Vital signs such as the electrical activity of the heart, respiratory rate, blood pressure, body temperature, and oxygen saturation are monitored using the patient monitoring equipment.
The surgical site is disinfected with 70% alcohol, 0.05% chlorhexidine, and povidone–iodine solution.
The animal is draped with a sterile sheet for surgery.
Surgical protocol
Stage 1: extraction of teeth (month 0)
The pig is placed under general anesthesia (5% isoflurane for induction and 2–3% for maintenance).
The perioperative area skin is prepared with an antiseptic solution and the operative field is draped in accordance with the planned procedure.
Local anesthesia of one to two capsules of scandonest (mepivacaine 2% with epinephrine 1:100,000) is injected to the surgical site intramucosally.
Bilateral mucoperiosteal flaps from the first and second mandibular premolars and the first mandibular molar are raised.
The premolars are extracted by sectioning the roots to ensure the preservation of the cortical bone.
After extraction, the sockets are curetted and rinsed with saline.
Primary closure of the mucoperiosteal flaps over the extraction sockets is performed using 4/0 Vicryl® sutures.
Stage 2: part 1—adipose tissue extraction and processing
After a healing period of 3 months from the extraction surgery, the pig is placed under general anesthesia a second time (after overnight fasting).
The animal is placed in the supine position.
The adipose donor site on the abdomen is shaved, disinfected with 1% cetrimide followed by 0.05% chlorhexidine, and finally swabbed with povidone–iodine.
Then the site is isolated with sterile drapes.
The area of aspiration is anesthetized with scandonest 2% epinephrine 1:100,000 via a 25 G needle.
A skin puncture was created through the skin with the 18 G needle (AdiPrep disposable set [ADI-25-01]).
Adipose tissue is extracted and processed according to the manufacturer's instructions of the AdiPrep system. In summary, tumescent fluid (1.8 mL scandonest 2% epinephrine 1:100,000 diluted in 50 mL sterile saline) is injected into the donor site via a 20 mL syringe (AdiPrep disposable set [ADI-25-01]) attached to an infiltrator cannula (AdiPrep disposable set [ADI-25-01]). The adipose tissue is solubilized in the tumescent fluid by pulling and pushing the syringe plunger repeatedly and is aspirated via a 20 mL syringe (AdiPrep disposable set [ADI-25-01]) attached to a harvester cannula (AdiPrep disposable set [ADI-25-01]). The adipose extract is allowed to settle, and the infranatant fluid, which sediments to the bottom, is disposed. The rest of the extract is transferred to the process disposable syringe (AdiPrep disposable set [ADI-25-01]) and centrifuged to yield the SVF.
The SVF is loaded into a PCL-TCP scaffold aseptically with a 1 mL syringe and 21 G needle until all the pores in the scaffold are completely filled. The level in the syringe before and after the loading is recorded, to determine the amount of SVF loaded into the scaffold.
Stage 2: part 2—alveolar defect generation and immediate osseous augmentation/reconstruction
The animal is rotated to the prone position and the ET tube is reattached.
After aseptic site preparation and local anesthesia placement, bilateral mucoperiosteal flaps are raised at the previous mandibular extraction sites. The alveolar ridge would have undergone physiological resorption after 3 months of healing.
Four sites on the buccal cortex (two each on the left and right sides of the mandible) over an area of 8 × 8 mm will be punctured with surgical round bur to induce bleeding.
The defects are randomly selected to receive one of the following:
Group 1: PCL-TCP scaffold loaded with SVF Group 2: PCL-TCP scaffold only Group 3: autologous bone (harvested from the “no graft” site by bur drilling) Group 4: no graft.
The PCL-TCP scaffold or autologous bone is secured to the buccal cortex with a titanium microscrew, which will help with the identification of the defect site during micro-CT analysis and histological analysis.
The defect sites are covered with a collagen membrane, BioGide®, to prevent infiltration of epithelial cells and fibroblasts. The periosteum is released and primary closure is achieved using 4/0 Vicryl sutures.
Immediate postsurgical care and radiological imaging
Vital signs and hemostasis are checked by the attending veterinarian before extubation.
The general condition of the animal is assessed and only returned to its pen when swallowing, palpebral/corneal reflexes are present.
The animal is kept warm with a vertical thermal heater while recuperating.
Buprenorphine (0.01–0.05 mg/kg) is administered intramuscularly 6 h after surgery. Ketorolac trometamol (Toradol; 15–30 mg/kg) is administered intramuscularly from 2 to 6 days postsurgery as pain reliever/anti-inflammation.
Ampicillin/cloxacillin 6–8 mg/kg is given intramuscularly for 3–5 days to prevent infection.
The veterinary team monitors the pain and extends the 0.05 mg/kg buprenorphine dose at 6–8-h intervals up to 3 days if necessary.
Postoperative monitoring
Radiological imaging (periapical X-ray with handheld X-ray machine) of the surgical sites is performed (i) immediately after the second surgery, and (ii) before the harvest to monitor the surgery sites.
The operation site is examined 1 week, 1 month, and 2 months postsurgery with the animal under sedation to check for adverse events such as postoperative infection, dislodgement of scaffold, wound dehiscence, pain, or allergy.
Long-term postsurgical care
The long-term care of the animal involves wound and pain management. Analgesic can be administered intramuscularly for a period of 3 days or more as to be advised by the attending veterinarian.
The animal is monitored for changes in general demeanor and behavior patterns, changes in posture and gait, vocalization, and daily activities.
Close communication between the surgery team and the animal caretaker/veterinarian will ensure early detection of deterioration of the animal.
The animal is kept on a soft diet for the entire duration of the study to prevent excessive forces on the operated alveolar ridge from the animal's chewing motions.
Specimen retrieval
The animal is euthanized at 3 months after the second surgery (6 months after the first surgery). Before sacrifice, the animal's body weight is recorded and compared with the average weight of the same strain of pigs at the same age. The study areas are assessed clinically for any inflammation, soft tissue dehiscence, or infection.
A perfusion fixation method is used for the sacrifice. The animal is sedated using ketamine (15 mg/kg) before anesthesia is induced with 4–5% isoflurane, and maintained with 2% isoflurane. Subsequently, 2 mL of heparin is given intravenously. The thoraces of the animal are opened by cutting the sternum to expose its heart. A 16 G IV catheter is inserted into the left ventricle, and perfused with 300–500 mL of Hartman's solution followed by 800 mL of a mixture of 2.5% paraformaldehyde and 2% glutaraldehyde. The right atrium is cut to allow the blood and fluid to flow.
The mandible is separated from the rest of the body. Both the right and left mandibular segments containing the experimental sites are harvested for downstream analyses. The specimens are submerged in 10% paraformaldehyde for fixation for 3 days and then soaked in 70% ethanol for long-term storage.
Analysis by micro-CT
The mandible specimen is gently tapped with tissue paper to remove excess 70% ethanol and the dimensions of each specimen are measured and recorded.
It is optional but preferable to wrap the mandible specimen in parafilm to prevent drying of the specimen, as the loss of moisture during long scans may affect the quality of the CT data.
The specimen is placed into the Mediso nanoScan® single-photon emission computed tomography/computed tomography (SPECT/CT) (or a similar instrument) and scanned with the following parameters:
Number of projections: 720 Scan method: semicircular multifield of view (FOV) X-ray power: 70 kVp, 280 μA Exposure time: 170 ms
The micro-CT data are analyzed in VGSTUDIO MAX 3.5 (or a similar CT analysis software). The threshold values for background, ISO value, and material are set at −1000, 2600, and 12,000 Hounsfield units (HUs), respectively. The region of interest, a rectangular block with the same dimension of the scaffold (8 × 8 × 3 mm), is positioned onto each surgical site where the scaffold was originally implanted. The bone volume fraction and bone density in each region of interest are calculated and recorded.
Analysis by histology and histomorphometry
The mandible specimens are dehydrated progressively in 70%, 95%, and 100% ethanol for 1 day each, followed by infiltration in xylene, methyl methacrylate (MMA), and 95% MMA/5% dibutyl phthalate (DBP) for 2 days each (with 1 h of vacuum degassing at the start of each infiltration step). The specimens are finally embedded in 95% MMA/5% DBP/0.2% Perkadox-16 at room temperature.
The MMA-embedded specimens are sectioned with a diamond blade saw (e.g., EXAKT 300 CP Band Saw; EXAKT). Each section is attached to an acrylic slide with a clear adhesive, and polished progressively with P320, P800, P1200, and P2400 sandpaper on a rotary grinder (e.g., EXAKT 400 CS Micro Grinding System; EXAKT) until the section is around 50 μm thick.
The polished sections are stained with methylene blue and basic fuchsin. 37
Descriptive histology is performed on the stained sections to evaluate bone regeneration and any inflammatory reaction. Histomorphometry measurements are done to evaluate the bone area fraction and histologic grading.
Representative images from stage 2 surgery and the harvest are illustrated in Figure 3.
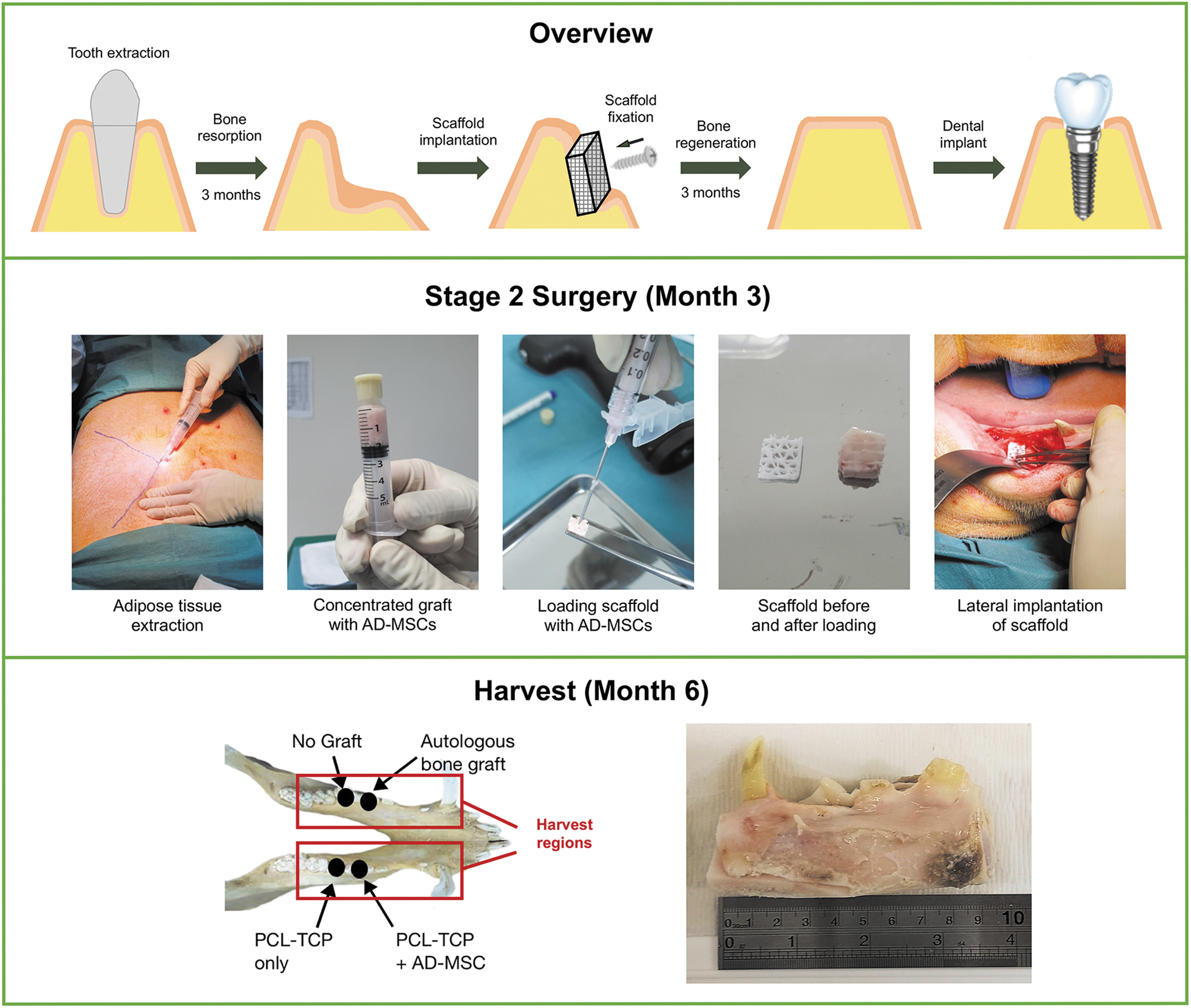
(i) Overview of the study, showing the resorption of the alveolar bone after tooth extraction and the augmentation surgery performed to regenerate the alveolar bone for dental implant installation. (ii) Representative images from the stage 2 surgical procedure, where adipose tissue is extracted and concentrated to yield an SVF graft rich in AD-MSCs. The graft is loaded into a porous PCL-TCP scaffold and the loaded scaffold is implanted laterally on the buccal side of alveolar ridge. (iii) A summary of the harvest procedure, showing the location of the harvest regions and a representative image of a harvested specimen. AD-MSCs, adipose-derived mesenchymal stem cells; PCL-TCP, polycaprolactone-tricalcium phosphate.
Anticipated Results
The protocol described by us is a combination of several established and validated protocols:
Lateral ridge augmentation is an established clinical procedure to regenerate alveolar bone in patients,38,39 and the porcine lateral alveolar defect model that we used is a validated clinically relevant animal model that simulates the pathology and regeneration of resorbed alveolar ridge in human patients.40,41
PCL is a biocompatible material used in FDA-approved medical devices and the PCL-TCP scaffold adopted in our study has been used clinically under special access conditions. The usage of the PCL-TCP scaffold in bone regeneration and orofacial applications has been documented in numerous preclinical and clinical studies.27,42–44
The role of AD-MSCs and SVFs in bone regeneration has been well studied in both humans11,21 and pigs.14,31 The protocol of using a close syringe microcannula system to extract and process adipose tissue is established and has been well-reported.20,23,45
Before starting the main study, we conducted a pilot study on one pig to test our protocol. From our observations in the pilot study, we made some improvements to our protocol, including the change of location of the defect from the crest to the lateral aspect of the alveolar ridge, and a corresponding change of the scaffold shape to reduce risk of dehiscence (as depicted in Fig. 2). After reviewing the previously reported protocols and analyzing the data from the pilot study, we are confident that our protocol can be reliably used to evaluate the efficacy of the AD-MSC-loaded PCL-TCP scaffolds in lateral alveolar augmentation in pigs.
To accurately determine the extent of bone formation in the defect and investigate the host response to the implant, the harvested specimen has to be carefully analyzed by a number of analytical methods. The most common analytical means to evaluate bone formation and host–implant interaction are micro-CT and histomorphometry, which are discussed below.
Microcomputed tomography
Typical information that can be obtained from a micro-CT scan of a mandible specimen (Fig. 4) includes bone volume fraction (bone volume/tissue volume), bone mineral density, alveolar ridge height, alveolar ridge width, alveolar ridge cross-sectional area, and so on. The data of the “PCL-TCP with AD-MSC” group are then compared with the data of the “PCL-TCP-only” group, “autologous bone” group, and “no graft” group.
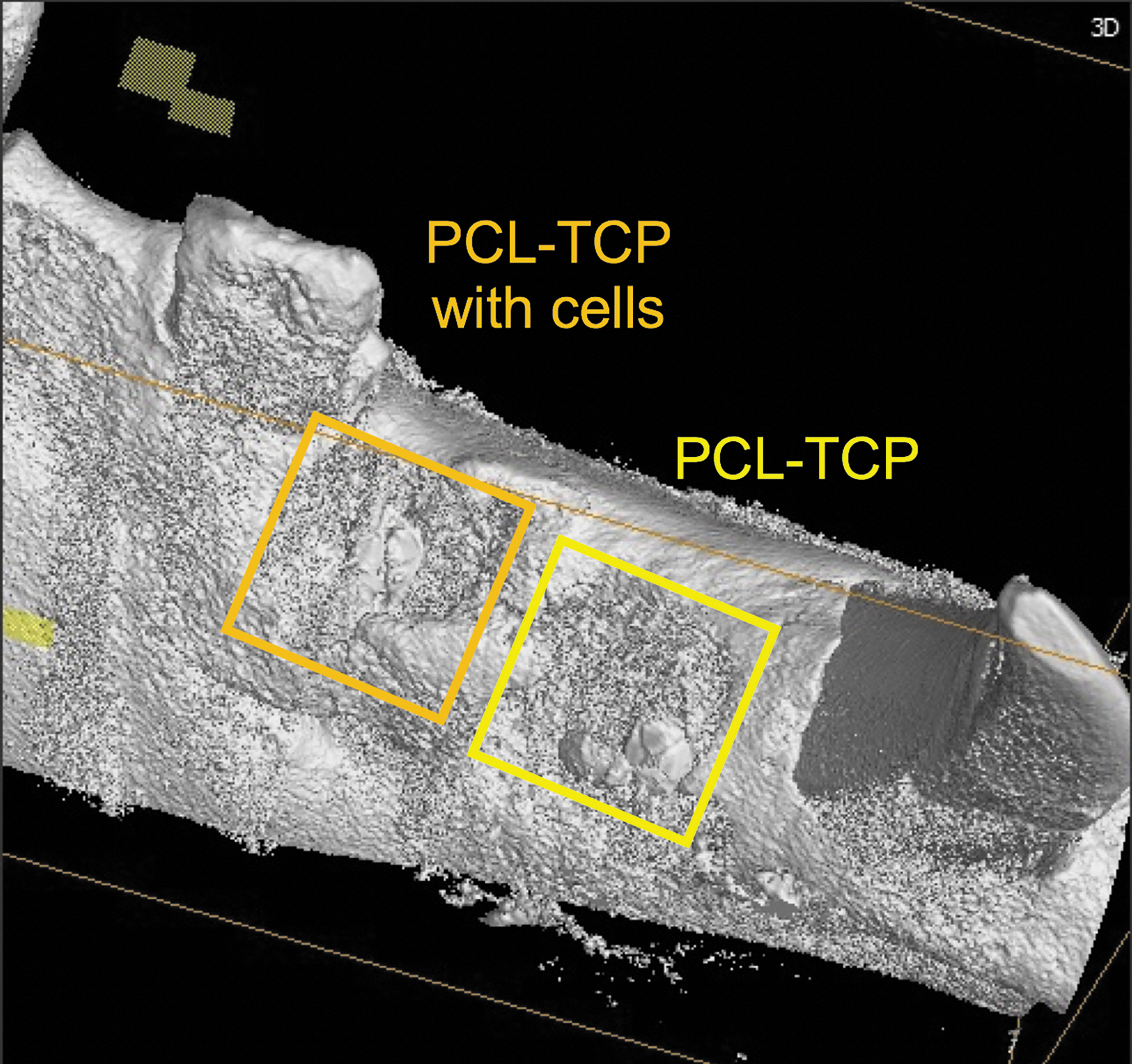
Micro-CT image of a mandible specimen with the “PCL-TCP with cells” group and the “PCL-TCP-only” group, 3 months after the implantation surgery. Micro-CT, microcomputed tomography. (Image generated by VGSTUDIO MAX 3.5 software.)
Histology and histomorphometry
Stained sections can be subjected to descriptive histology where the observations are qualitatively recorded and interpreted. For quantitative analyses, the stained sections are subjected to histomorphometry measurements, where important anatomical landmarks are identified to define the regions of interests to make quantitative measurements. The measurements may subsequently be used for calculating bone area fraction. Scoring systems can also be applied for analyses of biological processes such as tissue regeneration and immune response. 46
Conclusion
In this protocol, we have described the use of a clinically relevant porcine alveolar defect model to evaluate the efficacy of a novel combination of a 3D-printed PCL-TCP scaffold and AD-MSCs for lateral alveolar augmentation. Pigs are suitable for experiments involving AD-MSCs due to the abundance of accessible adipose tissues and the similarity in cell number, cell distribution, and cellular characteristics between pigs and humans. From a dental perspective, we recommend the use of older pigs with full adult dentition. Researchers who are concerned about the huge weight gains of domestic pigs can consider using miniature pigs. Our protocol can be adapted for a variety of scaffolds and cell types, and we hope that our protocol can support the translation of novel implants into clinical procedures in the field of dentistry and orofacial surgery.
Footnotes
Acknowledgments
The authors thank the veterinary team from the National Large Animal Research Facility (NLARF) and SingHealth Experimental Medicine Centre (SEMC) for its assistance with the animal study, the product team from Osteopore International Pte Ltd. for its support in scaffold development and optimization, and the product team from Terumo BCT Asia Pte Ltd. for the loan of equipment and technical support for the AdiPrep system. The authors also acknowledge Ms. Victoria Kang for her assistance in photography and surgery preparations.
Disclosure Statement
The authors declare that there is no competing financial interest.
Funding Information
This study was cofunded by Osteopore International Pte Ltd. and the National Additive Manufacturing Innovation Cluster (NAMIC), Singapore (Grant ID: 2019046).