
Abstract
Dental implants have been clinically used for almost five decades with high success rates. In vitro research models used in implant dentistry are limited to two-dimensional experiments, which are reproducible and well adapted to evaluate a single parameter but do not reproduce the complexity of clinical settings. On the contrary, the in vivo research models using animals offer similar histological and anatomical features to humans, and tissue healing can be close to a clinical situation, but those models are usually accompanied with ethical concerns, and their outcomes could not be extrapolated to humans because of interspecies variabilities. This makes the development of novel in vitro models that recapitulate physiological events occurring during dental implant placement of particular interest for current research in dentistry. Also, such models could be challenged by setting a pathological environment (peri-implantitis) to better understand the disease and eventually serve as a platform to evaluate novel treatment modalities. The aim of this systematic literature review was to cover all the in vitro three-dimensional (3D) complex models available for research in implant dentistry. To accomplish this, a comprehensive search of the literature present on Scopus and PubMed databases was done using specific keywords, as well as inclusion/exclusion criteria. Out of 1334 articles found, we have finally included 27 articles in this review with publication dates between 2001 and 2022. In those articles, the 3D models were designed to study tissue-implant interface behavior in bone or gingival tissue. The articles focused on simulating implant integration, evaluating the effect of different conditions on implant integration, or developing an infection model for the implant integration process. The methods used involved implant material and cells organized in a specific 3D structure. The 3D models developed were able to simulate the process of dental implant osseo- and soft tissue integration and lead to results comparable with conventional in vitro and in vivo models. A relatively limited number of articles were obtained, which indicates that this is an emerging field, highly dependent on progresses made in biotechnologies and tissue engineering, and that further investigation is needed to enhance these 3D in vitro models.
Impact Statement
The development of new dental implants is an accelerating field aiming to improve biocompatibility and durability of implants and to overcome complications associated with them. This highlights the importance of developing robust and reproducible models to study dental implants. There is increasing interest to switch from animal and two-dimensional in vitro models to three-dimensional (3D) in vitro models, which are tunable models that allow control over various parameters and resemble the complex cellular architecture of native tissue. It is therefore essential to explore the potential of those 3D in vitro models in the field of dental implantology to better understand the implant integration process.
Introduction
Dental implants have been used in clinics for a few decades, and the long-term success of those implants is currently well established.1,2 There are more than 1300 different types of implants in the market with different materials, shapes, connection interfaces, dimensions, and surface characteristics, 3 and this requires great scientific attention in order to optimize research models that efficiently characterize various implants’ parameters. In addition, peri-implantitis is a major clinical issue associated with dental implants in the mid- or long term; this infectious/inflammatory disease results ultimately in peri-implant alveolar bone resorption and implant loss.4,5 This requires the development of specific study models to better understand the development of such diseases and to evaluate novel therapeutic approaches.
The research tools available to evaluate biomaterials in implant dentistry are either two-dimensional (2D) in vitro experiments or in vivo studies using animal models. The in vitro methods are reproducible and well adapted to evaluate a single parameter in 2D (i.e., cell attachment or gene expression after culture on a titanium surface), but they don’t reproduce the complexity of clinical settings. 6 Indeed, the processes of osseointegration and soft tissue integration involve several cell types at different stages of differentiation, different tissues, and a continuous blood flow. Regarding animal models, they offer similar histological and anatomical features to those of humans, and tissue healing can be close to the clinical situation. Small and large animal models (rodents, minipigs, or dogs) are commonly used. 7 Although they may be adequate for the evaluation of surgical procedures, they have significant limitations. Ethical concerns are probably the most limiting today, especially when large animals such as pigs or dogs are used. Public opinion and also some clinicians are becoming more reluctant to use them for experiments. Moreover, animal tissues behave differently from human tissues after dental implant placement, and it is also difficult to extrapolate the role of a different oral microenvironment (saliva, microbiota) in the initiation and development of peri-implant diseases. Finally, in vivo experiments are expensive and can have important interindividual variability.
Thus, it is necessary to develop novel models for experimental research in oral implantology in order to combine the advantages of currently available in vitro and in vivo models. These novel in vitro artificial models should be able to recapitulate the physiological events leading to osseointegration and soft tissue integration and might be used as a tool to improve the basic knowledge of bone and soft tissue healing around dental implants. However, the major applications of these in vitro 3D models will be to serve as a study platform for biomaterials, and they could also be utilized as a peri-implantitis model.
The principal objective of this article was to provide an up-to-date systematic review of the in vitro 3D complex models available for research in implant dentistry. Secondary objectives were to detail the methods and the specific applications of the in vitro models available.
Materials and Methods
A literature review was performed on PubMed and Scopus databases. The research keywords were “dental implant osseointegration in vitro” and “dental implant integration in vitro.” The search procedure covered all the articles present on the databases between 1988 and 2023 (June).
Publications were selected if they matched inclusion criteria, defined as the following:
In vitro models Innovative culture process leading to a 3D study Dental implantology oriented
On the contrary, publications were systematically excluded from the review if they presented at least one of the following exclusion criteria:
In vivo models Conventional 2D models Systematic reviews, book chapters, and clinical case reports
The detailed screening process as shown in Figure 1 started by automatically removing reviews by filters of PubMed and Scopus. After that duplicates were removed, and all obtained records were screened by abstract reading. All articles that mentioned cell culture in the abstract were further examined by reading the materials and methods to select the articles with innovative 3D cultures to be included in this review. Also, some references matching the inclusion criteria could be identified among the references of the selected publications and were manually included in the review. In the cases where the study included both in vitro and in vivo experiments, only the in vitro part was considered.
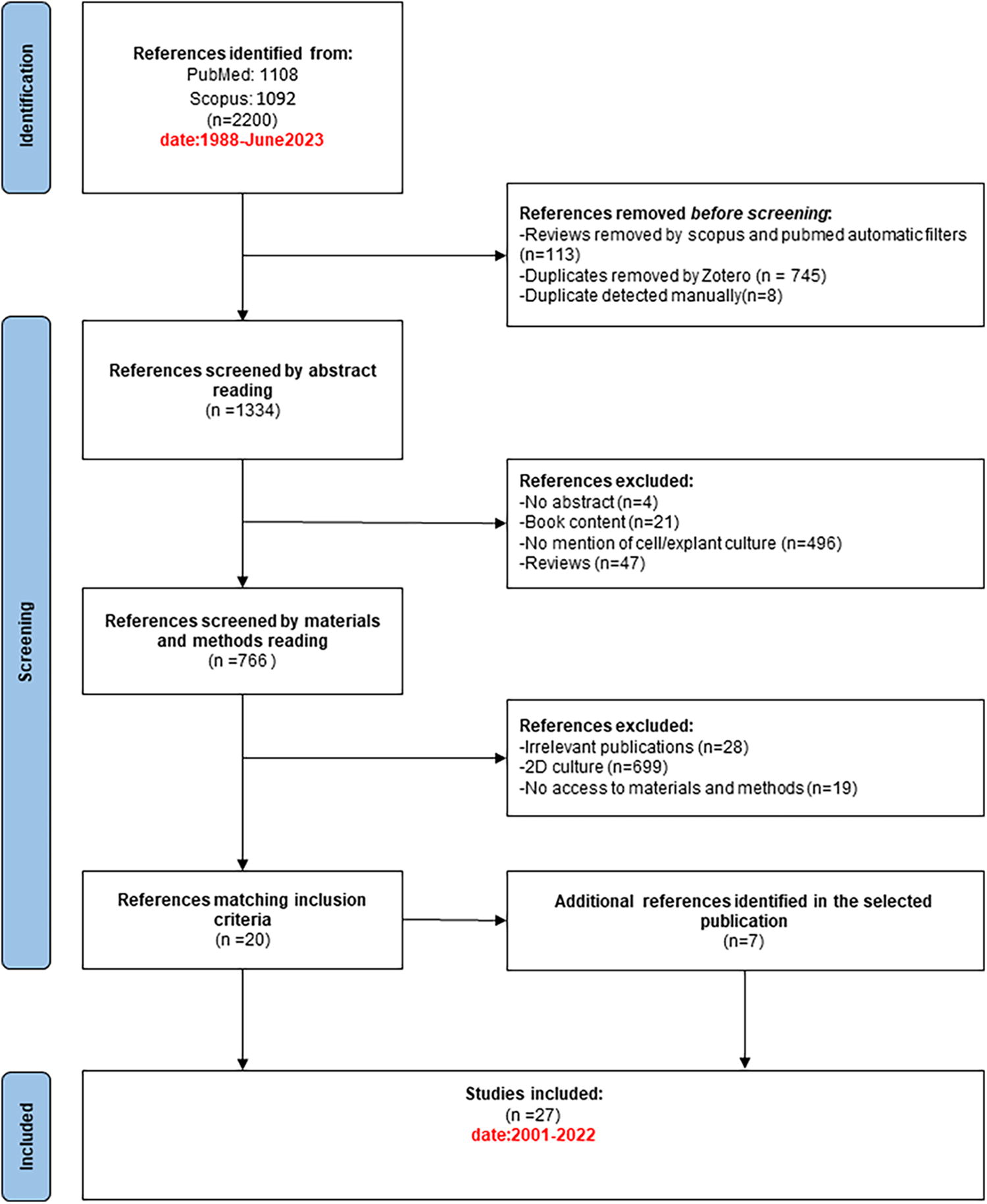
Selection process of the articles included in the review.
Results
We have retrieved 1108 publications on PubMed and 1092 publications on Scopus. After removing duplicates and reviews, we obtained 1334 articles. After applying the screening process, we included 27 articles. They were published between 2001 and 2022. For each article selected, we reported the objective, implant type, cells, specific 3D model, and characterization method (Table 1).
Summary of the Different Criteria Analyzed in the Selected Publications
ADSC, adipose-derived stem cells; DPSC, dental pulp stem cells; ELISA, enzyme-linked immunosorbent assay; HGF, human gingival fibroblasts; HOK, human oral keratinocytes; hPDLSCs, human periodontal ligament stem cells; MSC, mesenchymal stem cells; OMM, oral mucosa model; PCR, polymerase chain reaction; SEM, scanning electron microscopy; TEM, transmission electron microscopy; MTT, 3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyl-2H-tetrazolium bromide; ATP, adenosine triphosphate (ATP); HEPM, human embryonic palatal mesenchymal pre-osteoblasts.
Objectives
All articles included aimed to evaluate the tissue-implant interface. Eighteen were focused on osseointegration,8–25 and nine were related to the gingival soft tissue integration.26–34
The development of a model to simulate in vitro the implant integration process was the purpose of eight articles.12,15,17,19–21,26,31 Two articles reported an infection model.24,32 In the other articles, the influence of different conditions on the implant integration efficiency was evaluated.8–11,13,14,16,18,22,23,25,27–30,33,34 In particular, the role of implant material or surface pretreatment,8–10,13,16,23,25,27,28,30,33,34 the effect of different culture methods on osseointegration,11,14,18,22 and the effect of culture method on soft tissue integration 29 were evaluated.
Implant materials and designs
Although its surface was usually modified with a large variety of treatments, titanium was the principal implant material in the reviewed studies:8–29,31,32 Pure titanium or the alloy Ti-6Al-4V10,12,15,22,31 was used. Zirconia implants were also used in some studies.13,20,33,34 We found some studies using implants of plain polymer or composite reinforced with E-glass fiber 30 or hydroxyapatite 8 or hydroxyapatite and silicone rubber. 32
The studies were done with various shapes of implants, either commercially available or customized including rods or screw implants,8,9,12,13,15,17–19,21,30,33,34 discs,10,11,22,24,26–29,32 sheets, 25 cuboids, 14 bowls with flat bottoms, 20 or dental implant abutments. 31
Cells
Cell culture was used in every study to mimic the living tissue behavior. The cells used for the bone models were human, rat, rabbit, or mouse cells with osteogenic potential (detailed in Table 1). For the soft-tissue models, human gingival fibroblasts and human oral keratinocytes were used (Table 1).
Other cells present within the dental implant microenvironment were also used in some publications such as primary human periodontal ligament stem cells (hPDLSCs) 22 and M2 macrophages derived from primary monocytes. 20
Regarding the culture medium, in 13 studies, the models were cultured with an osteoinductive medium to promote mineralization.9,10,12–20,22,23 In 13 studies, basal medium adapted to the cell type was used.8,11,21,25–34 In one study, the basal medium was used for the osteoblasts, whereas osteoinductive medium was used with bone mesenchymal cells. 24
3D cell culture techniques
The implant-tissue interface was evaluated in all studies using specific experimental setups.
In several studies, the in vitro model simulated the in vivo fluid dynamics,10,11,16,23,25 using rotating condition10,11,16,23 or dynamic flow for culture 25 (Fig. 2A).
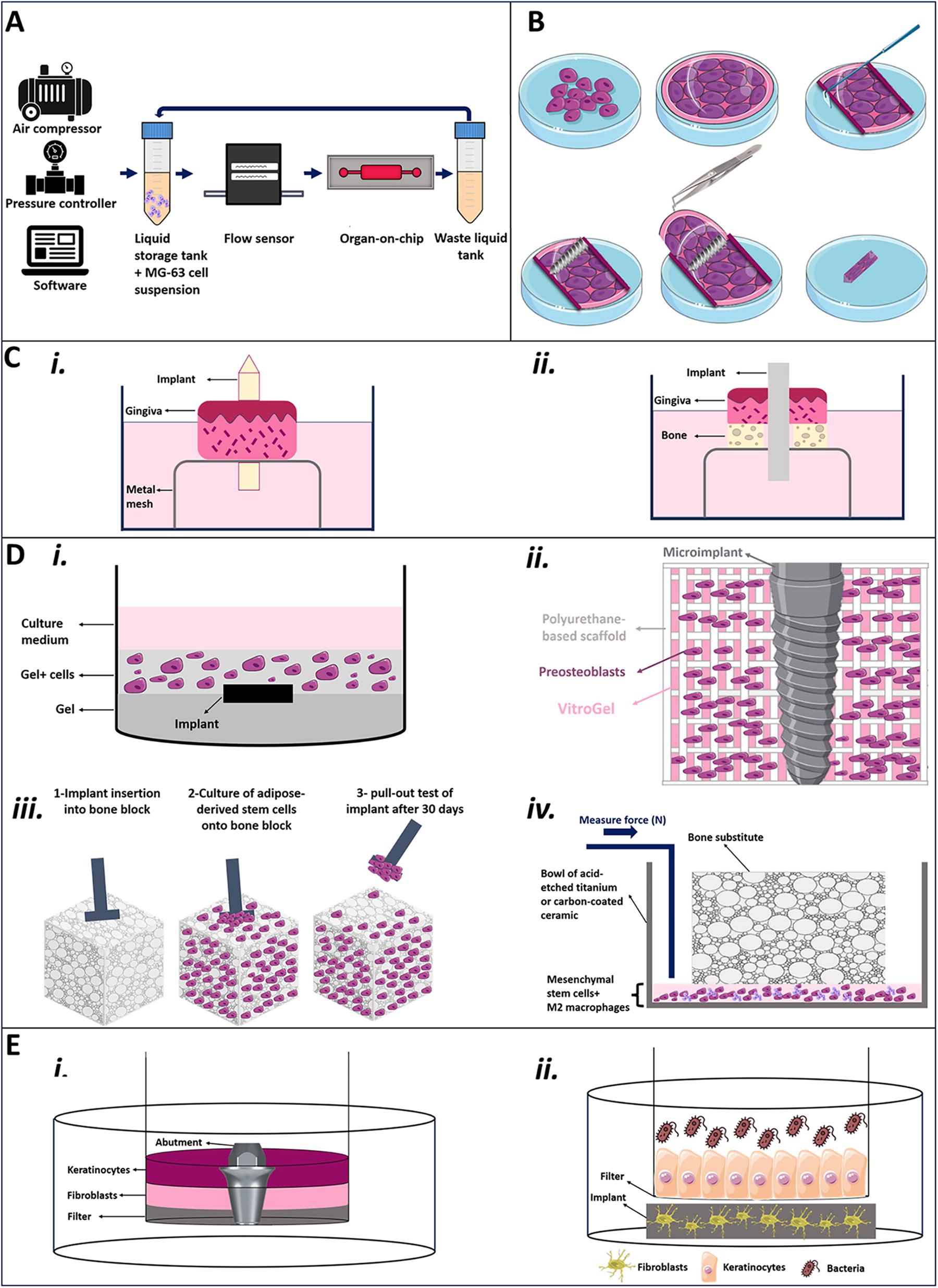
Five principal methods for 3D-engineered in vitro models.
In three models, cells were cultured on tissue plastic dishes until they produced a cell sheet,13,18,19 and then the sheet was wrapped around implants,13,18,19 and cell culture was carried out (Fig. 2B).
In six of the selected publications, animal explants were used instead of isolated cells cultured in a 3D environment.8,9,14,30,33,34 The in vitro culture of these models was done up to 5 weeks (Fig. 2C).
Most of the reviewed publications were based on the use of scaffolds.12,15,17,20–22 In the context of dental implant osseointegration and soft tissue integration, the scaffold provided a support for cell culture, therefore helping to build a 3D model with diverse materials. In four of the selected publications, a hydrogel matrix was used as a scaffold12,15,21,22 (type I collagen [COL I] gel in multilayer or bioprinted, VitroGel-3D® added into water-based polyurethane 3D scaffold), and in two studies, bone substitutes were used (Orthoss® made of bovine carbonated hydroxyapatite; 17 CERASORB® M cylinders 20 ) (Fig. 2D).
To study the implant or soft-tissue interface, transwell models were developed using two different methods.24,26–29,31,32 The first approach consisted of seeding keratinocytes and fibroblasts on a layer of acellular human allograft dermis that was allowed to proliferate. Then, a hole was punched in the dermis, and the titanium discs were inserted. The structure was cultured, and an air–liquid interface was created to reproduce a 3D oral mucosal model (3D OMM).26–28 In the second approach, gingival fibroblasts were mixed with a COL I solution overnight before culture into a transwell insert. Keratinocytes were then seeded on the top, and the structure was cultured at the air–liquid interface for 10 days. A hole was then punched in the structure so that titanium abutments could be inserted in close contact with the tissues 31 (Fig. 2E, i).
From another perspective, transwell models were also used for cocultures of gingiva model + bacteria 32 (Fig. 2E, ii) and osteoblasts/gingival fibroblasts + lipopolysaccharide (LPS) to simulate peri-implantitis 24 or fibroblasts and keratinocytes. 29
Characterization of the implant–tissue interface in the 3D models
Different techniques were used to evaluate the implant–tissue interactions at the interface and the efficiency of the biological integration.
The analysis of implant integration was done using histological or cellular analysis techniques. For histological analysis, proper sectioning and staining were done to visualize the aspects of cellular interaction with the implant (detailed techniques and results of histology are shown in Table 2).
Summary of Histological Analysis Techniques Including Embedding, Sectioning, Staining, and Microscopic Techniques with Highlight of Important Results Obtained from This Kind of Analysis
DPSCs, dental pulp stem cells; FIB, focused ion beam; SEM, scanning electron microscopy; TEM, transmission electron microscopy.
At the cellular level, the osteogenic differentiation of cells was monitored through polymerase chain reaction (PCR) to evaluate gene expression of osteogenic markers. The differentiation was further validated at the protein level through enzyme-linked immunosorbent assay, western blot, immunostaining, and alkaline phosphatase (ALP) activity. The level of mineralization was also evaluated through alizarin red staining and calcium quantification. In addition, cellular behavior was assessed through different techniques such as cytoskeleton staining, scanning electron microscopy (SEM), flow cytometry, cell quantification (DNA/ATP), proliferation assay (MTT), and cytotoxicity assay (CCK8). Regarding gingival models, only two studies used immunostaining, cytoskeleton staining, and PCR to evaluate implant integration (detailed cell evaluation techniques are shown in Table 3).
Summary of Cellular Analysis Techniques and the Purpose Behind Using Those Techniques in the Studies Included in This Review
ALP, alkaline phosphatase; BMP, bone morphogenetic protein; BSP, bone sialoprotein; CD31, platelet/endothelial cell adhesion molecule 1; Col I, collagen type I; FAK, focal adhesion kinase; ELISA, enzyme-linked immunosorbent assay; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; KDR, kinase insert domain receptor; OCN, osteocalcin; OPN, osteopontin; OSX, osterix; PPARG, peroxisome proliferator-activated receptor gamma; qRT-PCR, quantitative reverse transcription polymerase chain reaction; RPL13A, ribosomal protein L13A; RT-PCR, reverse transcription polymerase chain reaction; Runx2, runt-related transcription factor 2; SEM, scanning electron microscopy; VEGF, vascular endothelial growth factor; CEMP1, cementum protein 1; CCK8, Cell Counting Kit-8; DAPI, blue-fluorescent nucleus stain.
Innovative techniques were also used in many of the studies to characterize implant osseointegration. In two studies, the interaction of cells with the implant was evaluated by pullout test 17 or other mechanical setup 20 that measure the force needed to extract the implant from a cell-populated bone substitute. In one study by Jia et al., the authors used the tissue-on-chip model with continuous perfusion of cell suspension to study the cell movement velocity, direction, acceleration, and cell attachment number of MG-63 cells present within close proximity to the implant surface. To evaluate those parameters, various devices were used such as a particle tracking velocimetry system, microcomputed tomography (micro-CT), and a viscometer. 25
In addition, various new techniques were implemented in the gingival model. For example, a permeability test was performed by Chai et al. to evaluate quantitatively the biological seal around the implants in the 3D oral mucosal model by tracing tritiated water passing through this seal. 27
In one study, gingival explant–implant interface was analyzed by dynamic mechanical analysis measurement, which executes dynamic loading conditions representing natural mastication to evaluate implant integration. 33 However, a more realistic explant model compromising both gingival explant and underlying bone was also characterized by dynamic mechanical analysis and in silico analysis. 34
Relevance of existing complex 3D models for dental implant research
In all articles related to bone integration, microscopy and/or histological analysis showed that the different models enable to achieve a close contact between cells and implants.8–18,20–23 In most of the studies, the cells spread on the implant surface and dense ECM fibrous networks formed at the implant–tissue interface.8,9,11–18,23 The quantification of specific osteogenic markers (bone sialoprotein [BSP], alkaline phosphatase [ALP], collagen type I [COL I], runt-related transcription factor 2 [Runx2], osteopontin [OPN], osterix [OSX], or osteocalcin [OCN]) showed that the cells were well differentiated.10,11,13,16–18,23,24 Mineralized tissue formation was observed at the interface using alizarin red staining.10–12,18–20,23,24 In addition, an increase in the vasculogenesis markers was observed over time.10,16,23
Similarly, in all studies focused on implant–soft tissue interactions, an oral epithelium closely attached onto the scaffolds and comprising abundant collagen fibers was observed.26–28,30–32 In addition, an infection model was developed to study the interactions between cells, bacteria, and implant surfaces. 32 In one study, both bone and gingival cells were used to mimic the peri-implantitis, revealing how gingival fibroblasts impacted osteoblastic differentiation during peri-implantitis. 24 In addition, it was shown that the coculture of fibroblasts and keratinocytes supported soft tissue integration, and it could serve as a test platform for dental implants. 29 Explant models could also be used to compare implant surfaces, as these tissues remained vital during the period of culture and the soft tissue integration was successfully obtained.33,34
Several in vitro 3D models have been used for dental implant material selection: cell behavior on zirconia was similar to control titanium samples in one study. 13 It was observed that zirconia could be enhanced by TiO2 coating33,34 and by carbon coating. 20 Moreover, plain polymer or composite reinforced with E-glass were compared for soft tissue integration, and the composite implants were slightly more favorable. 30 In addition, it was shown that hydroxyapatite is less convenient for cell adhesion than titanium. 8
It was also observed that implants with rough surface enhanced cellular adhesion.9,17 The comparison of a rough (TriVent®) and slightly rough phosphorous-coated titanium oxide surface (TiUnite®) revealed that both surfaces were biocompatible and promoted osteogenic differentiation. However, the rough surface promoted early differentiation, whereas the other surface promoted only cell proliferation. 16 Laser-sintered titanium alloy promoted osteointegration in a better manner than acid-etched titanium, 10 and hydroxyapatite coating of titanium implant enhanced matrix formation in comparison with anodic oxidizing and precision blasting. 12 In some studies, neither the differentiation rate 9 nor the soft-tissue attachment27,28 was influenced by the topology of the implant surface. Also, surface treatment of titanium with anodization or conventional machining did not trigger any difference in epithelial attachment and soft tissue integration. 31
In the three studies comparing 2D and 3D culture processes, the results demonstrated that the 3D in vitro model promoted implant integration and provided more information than conventional 2D models.11,27,29 On the contrary, it was observed that 3D in vitro models were sensitive to study the effect of implant surface micromorphology on adjacent cells’ motility within 20 µm from the implant surface, and this could not be detected in vivo. 25
Discussion
The constant innovations in dental implantology require new characterization methods of the tissue–implant interface that are not based on animal testing. We have conducted a systematic review of the in vitro 3D models for dental implant research, and 27 articles were selected. This is an emerging field, which is highly dependent on the progresses made in biotechnology and tissue engineering. Considering the novel information that these models can provide, they could be used for a large number of applications, such as fundamental understanding of osseointegration and soft tissue response to implantation,11,12,14,15,17–22,26,29,31 screening of biomaterials,8–10,13,16,20,23,25,27,28,30,33,34 or peri-implantitis studies.24,32
In vitro models enable to assess the cell behavior for adhesion, proliferation, migration, morphological changes, and differentiation. 35 Cells with osteogenic potential were used in studies focusing on bone-to-implant interactions in 3D as they can differentiate toward osteoblastic cells that can enhance the bone integration process.35,36 Primary osteoblasts, human bone marrow-derived mesenchymal stromal cells (hBMSCs), and human adipose-derived stem cells (hADSCs) are widely used to study the biological response to different implant surface37–41 as they proved their osteogenic potential when cultivated on 3D scaffolds for the evaluation of bone regeneration. 40 A distinct characteristic of primary cells is their ability to resume the physiological events leading to the production of a living tissue. However, passaging those cells in vitro can lead to a phenotypic alteration, which makes them a finite source of cells. 42 Even though primary cells can mimic the physiological processes, culturing them in 2D is not ideal to reproduce the clinical situation. Therefore, 3D in vitro models could be useful to better reproduce the dynamics of the in vivo implant integration.
It is worth mentioning that when developing a complex model for biomaterial evaluation and screening, the purpose would be to produce an artificial tissue that will never be implanted. Cell lines are therefore good candidates for this application. They are already validated models for conventional 2D in vitro models, especially for biocompatibility and screening studies of biomaterials. Other advantages of cell lines are their large availability, their robustness, and their high culture reproducibility from one experiment to another, which is not the case with primary cells. Despite that, we have observed that the comparison and screening of implant materials were majorly done using primary cells.10,13,16,20,23,28
The major 3D models used for biomaterial screening are dynamic cultures10,13,16,23,25 or explant models.8,9,30,33,34
Various dynamic culture models10,13,16,23,25 were used to obtain a continuous flow, to control precisely many parameters, and to be closer to the in vivo experimental conditions. 43 Indeed, the use of a bioreactor can simulate the in vivo exchange of nutrients, wastes, and cell signals. 44 Under these conditions, osteoblasts tended to quickly form aggregates with gross morphological features close to that of human bone and produced a high rate of mineralization. 45
Alternatively, to cells, the use of explants for biomaterial screening was observed.8,9,30,33,34 Explants are highly available and can bring more information than cell attachment studies. Moreover, explant models are less expensive and less time-consuming than animal models. Regarding the bone explant models, they can lead to bone formation in an enclosed environment. 46 One limitation is the loss of cohesion of the tissue during long-term culture experiments. 30 In addition, these methods are still animal-dependent, and extrapolation to humans is scarce because of cross-species differences.
In the cell sheet wrapping technique, cells are already bound to one another with an extracellular matrix.13,18,19 It allows the even distribution of cells on the implant, thus nourishing it with an exogenic source of cells. However, these models are considered very similar to 2D models.
We observed that several of the 3D cell culture techniques are scaffold based.12,15,17,20–22 They are made out of several materials, and they could be a reliable alternative to explant cultures. They enable cells to grow directly on the implant surface, with a mechanical support to guide and initiate the development of new tissues. However, cells embedded in hydrogels may not grow properly because of reduced access to nutrients, and an anisotropic cellular behavior can occur. The same phenomenon can be observed in solid blocks when the mineralized matrix obliterates the pores.
The biological response to implants’ surfaces can be assessed with a large variety of tests, which can provide information on cell attachment, proliferation, and differentiation.39,47,48 Most of the methods used in 2D conventional models can be adapted to 3D models. Moreover, methods used in conventional in vivo models such as histology can also be adapted for the 3D in vitro models. In some cases, new methods must be specifically developed for 3D models.
This review showed that in most of the 3D models described, key osteogenic gene expression could be observed by PCR revealing the cell’s commitment to osteogenesis.10,11,13,16–18,22,23 Early (ALP, BSP, col1a1) and late markers (OCN) of differentiation were observed in the 3D models considered in this review. Moreover, Runx2 and OSX expression, which are essential transcription factors associated with the process of bone formation, were also examined. 49
One of the most difficult osseointegration parameters to assess in vitro is the mechanical stability, and it remains a crucial parameter to consider to evaluate osseointegration of dental implants. Primary stability refers to the absence of mobility of the implant to preserve hard and soft tissue, whereas secondary stability is linked to the intimate contact at the implant–tissue interface and the dynamics of osseointegration. 50 The primary stability can be assessed by several methods in vivo, for example, via resonance frequency analysis or measurement of the torque and force needed to extract an implant from a substrate (unscrew and pullout tests). 51 Cadaver bone is often the substrate for mechanical testing, but other materials such as bone composite or polyurethane blocks can be used.50,52 However, these materials are not suitable to assess the secondary stability, justifying in vivo investigations. 53 The tests performed by Sivolella et al. and Ehlicke et al. enabled to analyze the contact between dental implants and the mineral matrix produced by cells on bone blocks. Therefore, they investigated the potential of an in vitro tissue-engineered model to evaluate the secondary stability of the implant without the ethical issues of animal testing.17,20
From another perspective, one of the major objectives to be assessed with 3D in vitro models is to study peri-implantitis: the mucosa and gingival soft tissues should also be considered in those models because they act as a barrier to protect the underlying bone from the bacterial environment. 48 The integrity of the biological seal around the implant is therefore crucial to prevent peri-implantitis. Cell-culture models conceived to study implant–soft tissue interactions are generally based on keratinocytes and/or fibroblasts.47,54–56 Several models of oral mucosa are composed of either normal oral keratinocytes or squamous carcinoma cells, but lacking fibroblasts have already been developed. 26 However, it was reported that fibroblasts are essential for the differentiation of epithelial cells. 57 Thus, the development of models with both cell types is of critical importance to enable the organization of different cellular layers to form a stratified tissue that would be similar to the mucosa epithelium. This was successfully achieved by the transwell models.26–28,31,32 Furthermore, using the transwell model enabled the quantification of the biological seal (that was not possible before using the conventional qualitative histomorphometric analysis). 27 Thus, once the parameters of transwell models are optimized, it would be interesting to use them for mechanical assessments of the implant attachment (pullout measurements).
In addition, the current infection models available in dental implant research are based on coculture of cells and bacteria. Those models can be subdivided into peri-operative contamination models where cells have to integrate into contaminated implant 58 and postoperative models where cells integrated into an implant are challenged by bacteria. 59 We have observed in some reports that the transwell system is particularly suitable for obtaining a postoperative infection model as it enables to target one layer of cells and evaluate its role in pathological conditions.24,32 However, the major limitation of those transwell models is that the implant was inserted after the construction of the tissue:26–28,31 this process has an inherent risk to damage the cellular structure. In addition, the models lacked other cellular components such as the peripheral immunological defense system, which are involved in implant complications such as peri-implantitis.
Finally, it is worth mentioning that the 3D models present in this article do not mimic entirely what occurs in vivo. In fact, osseointegration is a complex process that involves various overlapping biological events. One of the events to be considered is the immune response, and it was shown that immune cells, especially macrophages, play an important role in osseointegration process of dental implants;60,61 it was also demonstrated that the process of soft tissue integration can be influenced by the immune microenvironment. 62 Another event to consider is angiogenesis, which is essential for the delivery of nutrients, oxygen, and osteoprogenitor cells.60,63 Finally, it is also shown that neurogenesis is involved in the osseointegration process. 64 This complex system of cellular interactions cannot currently be completely reproduced in vitro. Therefore, at this stage, 3D models are not sufficient to entirely replace animal experimentation. However, those models can present an initial step in biomaterials screening and could therefore reduce the overall resort to in vivo experiments and speed up the process of biomaterials selection.
Conclusions and Future Perspectives
Current dental implant research is based on well-described 2D in vitro models for biomaterials screening at low cost and also on in vivo preclinical models to mimic the clinical setting in patients. This two-step approach currently encounters some limitations, such as (among others) the discrepancy between in vitro and in vivo results and the regulatory rules for in vivo research being more and more severe in most countries.
In the attempt to facilitate the screening of biomaterials and to provide new tools for dental implant research, novel 3D in vitro models are being developed, on the basis of tissue engineering techniques. We have observed in this review that these models have been developed to study bone or soft tissue integration and that the results are comparable with conventional in vitro and in vivo models. However, some specific methods of characterization must be developed, especially to visualize the bone-to-implant interface. There are currently only a few applications of these models, and they are related to biomaterials screening or establishment of novel peri-implantitis models. In addition, there is only one model within the covered publications that mimics both bone and soft tissue integration of dental implants simultaneously, and this model does not completely reproduce the in vivo situation. Optimizing the parameters of such 3D models and broadening their utilization spectrum would be a promising step in dental implantology research that would reduce both the time and the cost lost using conventional research models.
Footnotes
Authors’ Contributions
Conceptualization: G.S., C.B., L.C., M.L.S., O.C., S.C.; Methodology: G.S., S.C.; Validation: G.S.; Formal analysis: G.S.; Visualization: G.S., C.B.; Investigation: G.S., C.B.; Writing—original draft: G.S., C.B., S.C.; Writing—reviewing and editing: O.C., S.C.; Supervision: S.C.; Project administration: S.C.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study is part of a project funded by two grants: Agence Nationale de la Recherche (ANR IDEAL-3D 2022–2026) and International Team of Implantology (1308–2018).