
Abstract
Induced hypothermia has been reported to provide neuroprotection against traumatic brain injury. We recently developed a novel method of selective brain cooling (SBC) and demonstrated its safety and neuroprotection efficacy in a rat model of ischemic brain injury. The primary focus of the current study was to evaluate the potential neuroprotective efficacy of SBC in a rat model of penetrating ballistic-like brain injury (PBBI) with a particular focus on the acute cerebral pathophysiology, neurofunction, and cognition. SBC (34°C) was induced immediately after PBBI, and maintained for 2 hours, followed by a spontaneous re-warming. Intracranial pressure (ICP) and regional cerebral blood flow were monitored continuously for 3 hours, and the ICP was measured again at 24 hours postinjury. Brain swelling, blood–brain barrier permeability, intracerebral hemorrhage, lesion size, and neurological status were assessed at 24 hours postinjury. Cognitive abilities were evaluated in a Morris water maze task at 12–16 days postinjury. Results showed that SBC significantly attenuated PBBI-induced elevation of ICP (PBBI = 33.2 ± 10.4; PBBI + SBC = 18.8 ± 6.7 mmHg) and reduced brain swelling, blood–brain barrier leakage, intracerebral hemorrhage, and lesion volume by 40%–45% for each matrix, and significantly improved neurologic function. However, these acute neuroprotective benefits of SBC did not translate into improved cognitive performance in the Morris water maze task. These results indicate that 34°C SBC is effective in protecting against acute brain damage and related neurological dysfunction. Further studies are required to establish the optimal treatment conditions (i.e., duration of cooling and/or combined therapeutic approaches) needed to achieve significant neurocognitive benefits.
Introduction
Clinically induced therapeutic hypothermia is usually achieved by whole-body cooling techniques, which potentially invokes systemic side effects. For example, systemic hypothermia decreases the enzymatic activity of clotting factors when body temperature drops below 33°C, increasing the risk of coagulopathy and ensuing hypotension (Shiozaki et al., 2001; Milhaud et al., 2005; Liu et al., 2006; Hemmen and Lyden, 2007). It also dampens the immune response and poses an increased risk of infectious pneumonia in TBI patients (Bernard et al., 2002; Alderson et al., 2004). These adverse effects of whole-body cooling have raised serious concerns for its clinical application in treating TBI patients, especially for patients suffering severe hemorrhage (Romlin et al., 2007; Tieu et al., 2007). Therefore, a method to rapidly and selectively cool the brain may offer a viable alternative to achieve the beneficial effects of hypothermia while minimizing potentially serious adverse effects during the treatment of severe TBI (Milhaud et al., 2005; Hemmen and Lyden, 2007).
We recently developed a novel method of selective brain cooling (SBC) in rats using extraluminal bilateral common carotid artery (CCA) cooling cuffs that can achieve rapid and sustained reductions in brain temperature while maintaining normal (37°C) body temperature. This method has been shown to be safe and efficient for inducing SBC in normal animals and in animals with ischemic brain injury. More importantly, we have demonstrated that SBC (34°C for 2 hours) provides significant neuroprotection against ischemic brain injury in a rat model of middle cerebral artery occlusion (Wei et al., 2008a).
The primary focus of this study was to evaluate the potential therapeutic efficacy of SBC in an experimental model of TBI. The penetrating ballistic-like brain injury (PBBI) rat model reproduces clinically relevant pathophysiological aspects of a severe, penetrating brain injury caused by a low- or high-velocity bullet/fragment wound to the head (Williams et al., 2005a), including elevated intracranial pressure (ICP) and reductions in regional cerebral blood flow (rCBF) and brain oxygen tension (Bramlett and Dietrich, 2004; Williams et al., 2005a; Wei et al., 2008b; Murakami et al., 2009). Since timing and duration of treatment are critically important factors for effective management of severe TBI, a major advantage of our CCA cooling method of SBC is that therapeutic brain temperature levels can be rapidly achieved, within 20–30 minutes after induction of SBC. Several hours of cooling is sufficient to produce significant neuroprotection in TBI models (Clifton et al., 1991; Lyeth et al., 1993; Dietrich et al., 1994), and based on our previous success in applying SBC (34°C for 1.5 hours) initiated 30 minutes post-middle cerebral artery occlusion in rats (Wei et al., 2008a), we hypothesized that early initiation of SBC during the acute postinjury period would provide significant neuroprotection. For this purpose, SBC (34°C) was induced immediately after PBBI and maintained for 2 hours, followed by spontaneous rewarming. Physiological measures included ICP and rCBF monitored continuously for 3 hours and ICP was measured again at 24 hours postinjury. Brain swelling formation, blood–brain barrier (BBB) permeability, intracerebral hemorrhage (ICH), lesion size, and neurological status were assessed at 24 hours postinjury, whereas spatial learning abilities were assessed in a Morris water maze (MWM) task at 12–16 days postinjury.
Materials and Methods
Animals
All research procedures were approved by the Walter Reed Army Institute of Research Institutional Animal Care and Use Committee and were conducted in compliance with the Animal Welfare Act and Guide for the Care and Use of Laboratory Animals (National Research Council). Male Sprague Dawley rats (Charles River Laboratories, Raleigh, VA) weighing 275–325 g were used. During all surgical procedures, rats were anesthetized by isoflurane (5% for induction and 1.5% for maintenance) delivered in a mixture of 30% oxygen and 70% air.
PBBI model
Unilateral, frontal 10% PBBI was induced in rats as described previously (Williams et al., 2005a). Briefly, the head of the anesthetized rat was secured in a stereotaxic frame and a cranial window (4 mm diameter) was created on the dorsal surface of the skull (4.5 mm anterior and 2.0 mm lateral to the bregma) to expose the right frontal pole. A specially designed PBBI probe was manually advanced through the cranial window along the axis (angled 50° from the vertical axis and 25° counter-clockwise from the midline), penetrating the right frontal hemisphere to a distance of 1.2 cm from dura. The ballistic component of the injury was induced by a rapid (<40 ms in duration) calibrated water pressure pulse designed to fill the elastic tubing and form an elliptical balloon calibrated to equal 10% (6.33 mm diameter) of total rat brain volume. After PBBI, the probe was manually removed, the cranial window was sealed with sterile bone wax, and the incision was closed with wound clips. Sham animals received all surgical manipulations, including craniotomy without insertion of the probe.
Selective brain cooling
SBC was achieved using a method developed in our lab (Wei et al., 2008a). The bilateral CCAs were exposed and separated from the vagus nerve in anesthetized rats. Cooling cuffs, constructed from a section (1 cm2) of Saran Wrap, were surgically placed around the exposed segment of each CCA (∼0.5 cm below internal–external carotid bifurcation) and secured by silk suture. The cutaneous incision was closed with wound clips. To induce SBC, ice-cold water was pumped continuously through the cooling cuffs placed to cool the circulating blood as it entered the brain. SBC was initiated immediately after PBBI and maintained for 2 hours. After 2 hours, the cold water circulation was stopped and the brain was allowed to re-warm spontaneously. During the entire period of SBC and re-warming, core body temperature was maintained at 37°C using a heating blanket.
Measurement of physiological parameters
A total of 57 rats were randomly assigned to one of three groups: sham (n = 13), PBBI (n = 22), and PBBI + SBC (n = 22). Physiological parameters (ICP, rCBF, and mean arterial blood pressure [MABP]) and neurological score assessments (24 hours) were recorded for all animals. Before PBBI, the femoral artery was cannulated for monitoring MABP using a pressure transducer. Immediately after femoral artery cannulation, rats were repositioned in a stereotaxic frame (Kopf, Tujunga, CA) and a midline incision was made in the scalp. Six burr holes were drilled on the skull for the placement of probes to measure rCBF (four locations), ICP, and brain temperature (Fig. 1). Four laser Doppler probes (Moor Instruments, Devon, England) were placed on the parietal cortex (1 or 6 mm posterior and 4 mm lateral to the bregma) of both hemispheres to measure rCBF of the right-anterior (core region of injury), left-anterior, right-posterior and left-posterior regions of the brain. A microsensor ICP probe (Codman and Shurtleff, Raynham, MA) was inserted into the left-posterior area of the brain (4 mm posterior and 2 mm lateral to the bregma), 2–3 mm deep from the surface of the skull. The brain temperature probe was inserted into the right hemisphere (2 mm posterior and 2 mm lateral to the bregma, and 4 mm below the skull surface) and connected to a temperature monitor (Model TH-8; Physitemp Instruments, Inc.). Core body temperature was measured by a rectal probe (Model TH-8; Physitemp Instruments, Inc.). All probes were immobilized on the skull with sterile bone wax. All physiological parameters were monitored continuously for 10 minutes before the induction of PBBI and for 3 hours after PBBI. An additional 5-min measurement of ICP was taken at 24 hours post-PBBI in re-anesthetized rats. The digitized signals of rCBF, MABP, and ICP were recorded by Power Lab data acquiring system for PC recording (AD Instruments, Inc., Colorado Springs, CO). Cerebral perfusion pressure (CPP), calculated as the MABP minus ICP, was recorded simultaneously.
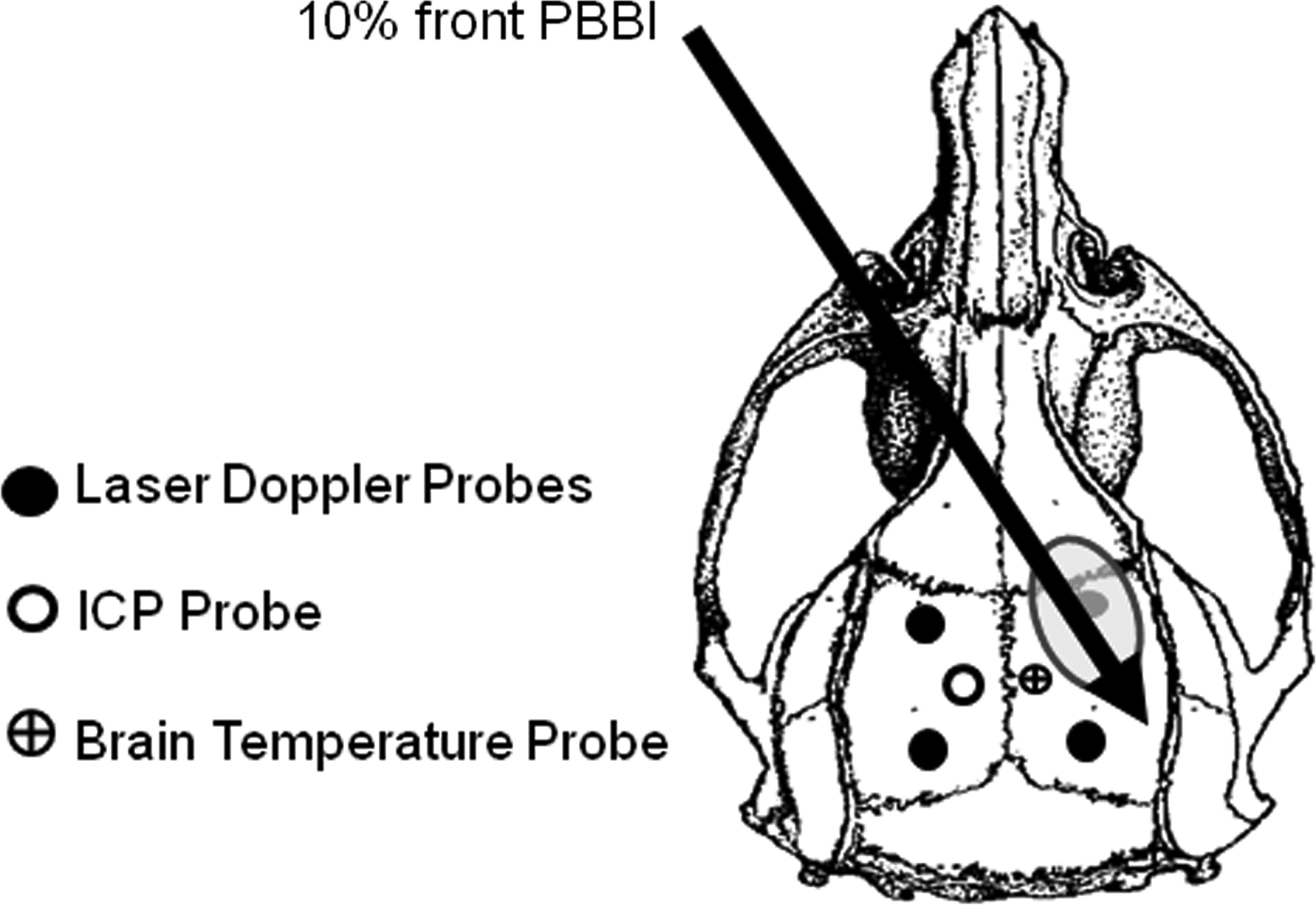
Schematic diagram of the recording probes of Laser Doppler, intracranial pressure (ICP) and brain temperature placement in rats.
Neurological score
Neurological deficits were evaluated at 24 hours post-PBBI using a modified clinical examination (Bederson et al., 1986; Tortella et al., 1999; Williams et al., 2005a). Neurological scores were calculated based on a 12-point sliding scale ranging from 0 (normal) to 12 (severely impaired) comprised from four separate, equally weighted neurological exams that measured (1) contralateral forelimb flexion during tail suspension, (2) shoulder adduction (body upward curling behavior) during tail suspension, (3) impaired resistance to lateral push, and (4) abnormal circling behavior.
MWM task
Cognitive abilities were assessed in separate groups of animals (sham = 6; PBBI = 9; PBBI + SBC = 8) from 12 to 16 days post-PBBI in a spatial learning task using the MWM with a video-tracking system (Noldus EthoVision XT). The water maze apparatus consists of a circular pool (75 cm deep; 175 cm diameter) filled with clear water (22°C ± 1°C, room temperature) to a depth of 60 cm. A clear, Plexiglas platform is submerged to a depth of 1 cm from the water surface and placed ∼35 cm from the wall of the pool in the center of the northwest quadrant. The position of the platform remained constant throughout the experiment.
At the start of each trial, the rat was placed in the pool (snout facing the pool-wall) at one of the four equally spaced starting positions: north, south, east, and west. Starting positions were pseudo-randomly determined, alternating between short and long distances to the platform. Each rat was allowed to swim freely in the pool until it found the submerged platform or until 90 seconds had elapsed. Once the rat mounted the platform, it was allowed to remain on the platform for 10 seconds before being removed from the pool and placed back in their home cage. Animals that could not locate the platform within the allotted time were gently guided to the platform and allowed to rest for 10 seconds. Between trials, animals were placed back in their home cages on warm water-circulating blankets. Rats were given four trials per day (30 minutes intertrial interval) for 5 consecutive days. All trials were recorded with a digital video-tracking system. Primary outcome measures include (1) latency (seconds) to find the hidden platform and (2) swim distance (meters) to the hidden platform.
Histology
At 24 hours and 16 days postinjury, rats were deeply anesthetized and transcardially perfused with 4% paraformaldehyde. Coronal sections (40 μm) from each group at 24 hours (sham = 3; PBBI = 9; PBBI + SBC = 9) and at 16 days (sham = 6; PBBI = 9; PBBI + SBC = 8) postinjury were cut from +4.0 to −7.0 mm anterior-posterior (AP) to bregma. One set of coronal sections was stained with hematoxylin and eosin. Each section was digitally imaged and the regions of interest were demarcated by an investigator blinded to the treatment for quantitative analysis of lesion volume (24 hours and 16 days postinjury) and acute (24 hours) ICH volume and brain swelling as described by Martins et al. (2003) and Williams et al. (2005b). Sequential integration of the respective areas from each section yielded the total lesion and hemorrhage volumes (mm3). Similarly, total ipsilateral and contralateral hemispheric volumes were measured to yield the percent hemispheric swelling of the injured hemisphere (Williams et al., 2005a).
BBB permeability to albumin
An additional set of brain sections was used for evaluation of BBB permeability at 24 hours post-PBBI by immunohistochemistry of albumin using polyclonal antirat albumin antibody (Hsu et al., 1981). Briefly, after inactivating the endogenous peroxidase activity with hydrogen peroxidase, sections were incubated free-floating in 0.1 M phosphate-buffered saline (pH 7.4) containing 1% normal goat serum, 0.3% Triton X-100, and a rabbit polyclonal anti-rat albumin antibody (1:80,000; MP Biomedicals, Solon, Ohio). The immunoreaction product was observed according to the avidin–biotin complex method using the Vectastin elite ABC kit (Vector Lab., Burlingame, CA) and 3′,3′-diaminobenzidine (Sigma-Aldrich, St. Louis, MO) as a chromogen. After dehydrated in ethanol, the sections were cleared in xylene and coverslipped with Permount® (Fisher Scientific, Fair Lawn, NJ). The BBB permeability was measured based on 6 coronal brain sections (at 2-mm intervals from +4.0 to −7.0 mm from bregma) using a computer-assisted image analysis system (Loats Associates, Westminster, MD). The increased optical density from the ipsilateral hemisphere divided by the optical density from the contralateral hemisphere yielded the hemispheric percent increase in BBB permeability in the injured hemisphere over the contralateral hemisphere.
Statistical analysis
Outcome metrics were analyzed using either repeated-measures or one-way analysis of variance, followed by Fisher protected least significant differences (PLSD) post hoc analysis when appropriate. All data are presented as the mean ± standard error of the mean; p-values <0.05 were considered significant. For all experiments, trained investigators performing behavioral and neuropathological assessments were blinded to the experimental groups.
Results
SBC (3°C below the body temperature) was achieved within ∼20 minutes after the onset of the cooling. Brain hypothermia status was maintained at 34°C for 2 hours, at which point spontaneous re-warming was initiated. Brain temperature returned to the precooling levels within ∼30 minutes of SBC withdrawal (Fig. 2). Body temperature was maintained at 37°C during the entire duration of SBC.
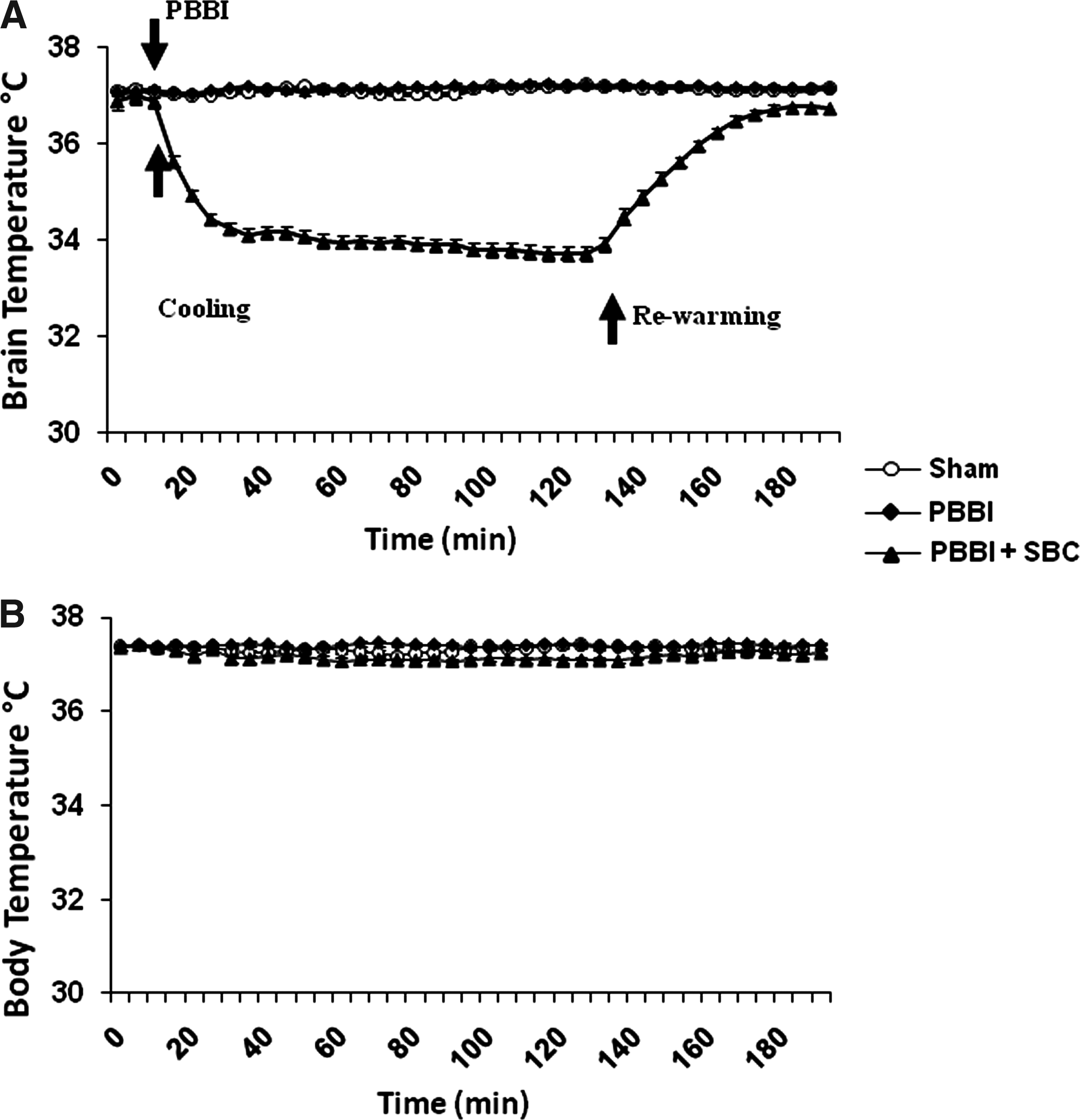
Real-time recording of brain and rectal temperature. (
Physiological parameters
Before injury, there were no significant between-group differences in MABP, ICP, or CPP (Fig. 3A–C) and these parameters remained stable (unchanged) in sham animals during the 2 hours SBC treatment phase and during the 1 hour post-SBC phase (i.e., 3 hours postsurgically). Immediately after PBBI, the ICP rapidly increased, reaching significantly elevated levels within 5 minutes postinjury, and increased to levels that measured 2.5-fold greater than normal by 3 hours post-PBBI (sham: 6.7 ± 0.8 mmHg, PBBI: 18.0 ± 1.1 mmHg). By 24 hours after PBBI, the ICP level had increased 3.5-fold compared to normal levels detected in sham animals (sham: 9.4 ± 0.7 mmHg, PBBI: 33.3 ± 2.7 mmHg). The elevated ICP was accompanied by a concomitant reduction in CPP, which was significantly lower than normal by 15 minutes post-PBBI, and continued to decrease, reaching 82% of the control level (sham: 103.3 ± 5.3 mmHg, PBBI: 85.0 ± 4.0) by 3 hours post-PBBI. In contrast, with rapid post-PBBI induction of SBC, the magnitude of changes in both ICP and CPP was significantly diminished. As shown in Figure 3B and C, SBC caused significant (∼35%) reductions in injury-induced elevations in ICP in the PBBI + SBC group (11.7 ± 0.7 mmHg) by 3 hours postinjury. Moreover, by 24 hours postinjury the ICP levels in the PBBI + SBC group (18.7 ± 1.5 mmHg) were 45% lower than the PBBI rats without SBC treatment (Fig. 3D). Injury-induced reductions in CPP were also mitigated as a result of the SBC treatment and significant recovery (98.3 ± 2.2 mmHg; 115%) was achieved by 3 hours postinjury compared to PBBI along group (85.3 ± 3.9 mmHg).
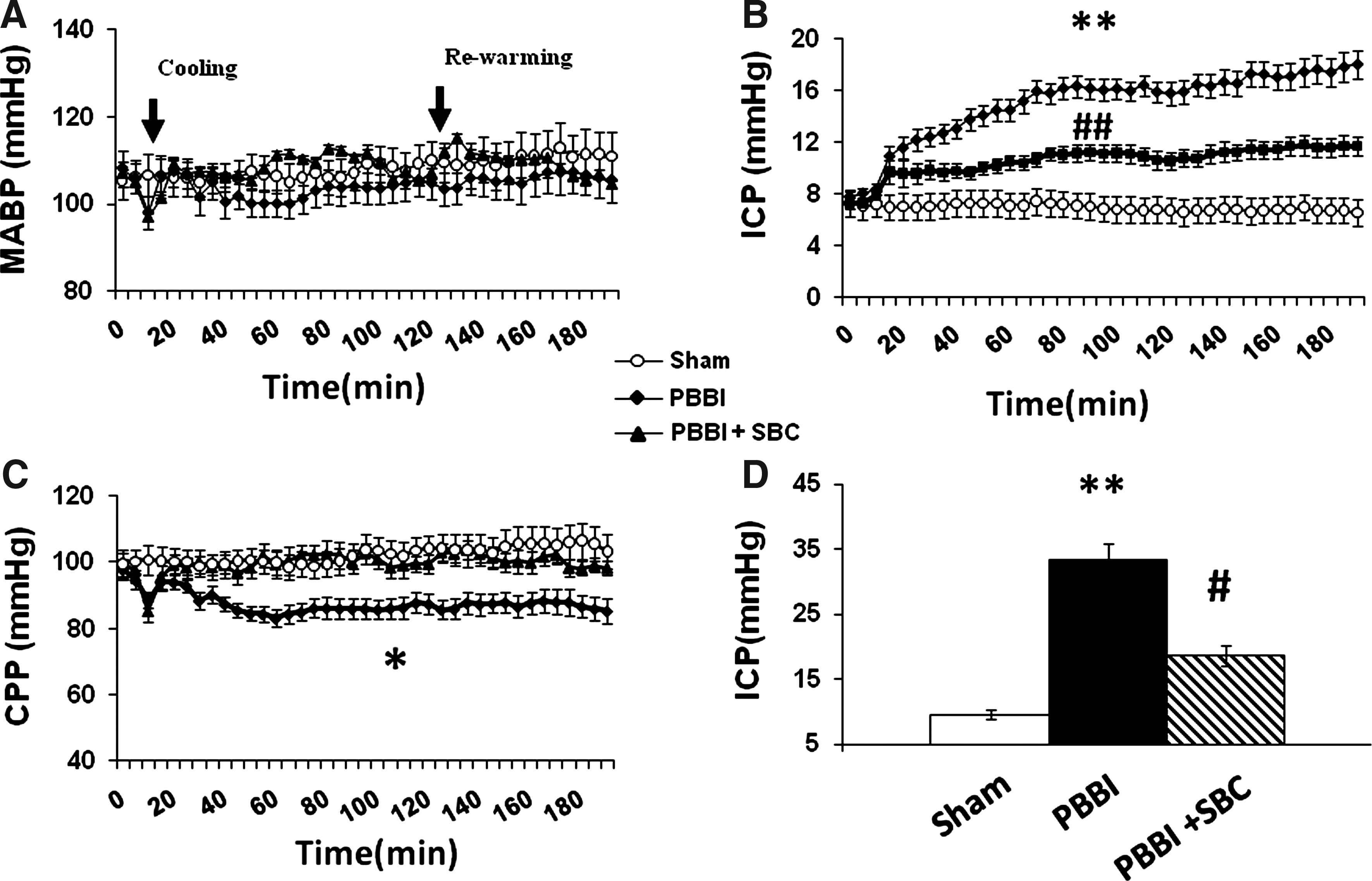
Therapeutic effects of SBC on ICP levels and cerebral perfusion pressure (CPP) levels in PBBI rats. During the initial 3 hours after PBBI (
Measurements of rCBF were monitored in four regions of the brain (Fig. 1). Within 5 minutes after PBBI, a significant reduction in rCBF (∼80% of the baseline level) was detected in the right anterior region, the area most proximal to the site of injury. No significant changes in rCBF were detected in any of the other three brain regions measured after PBBI. SBC treatment did not significantly affect the PBBI-induced hypoperfusion detected near the injury core (Fig. 4).
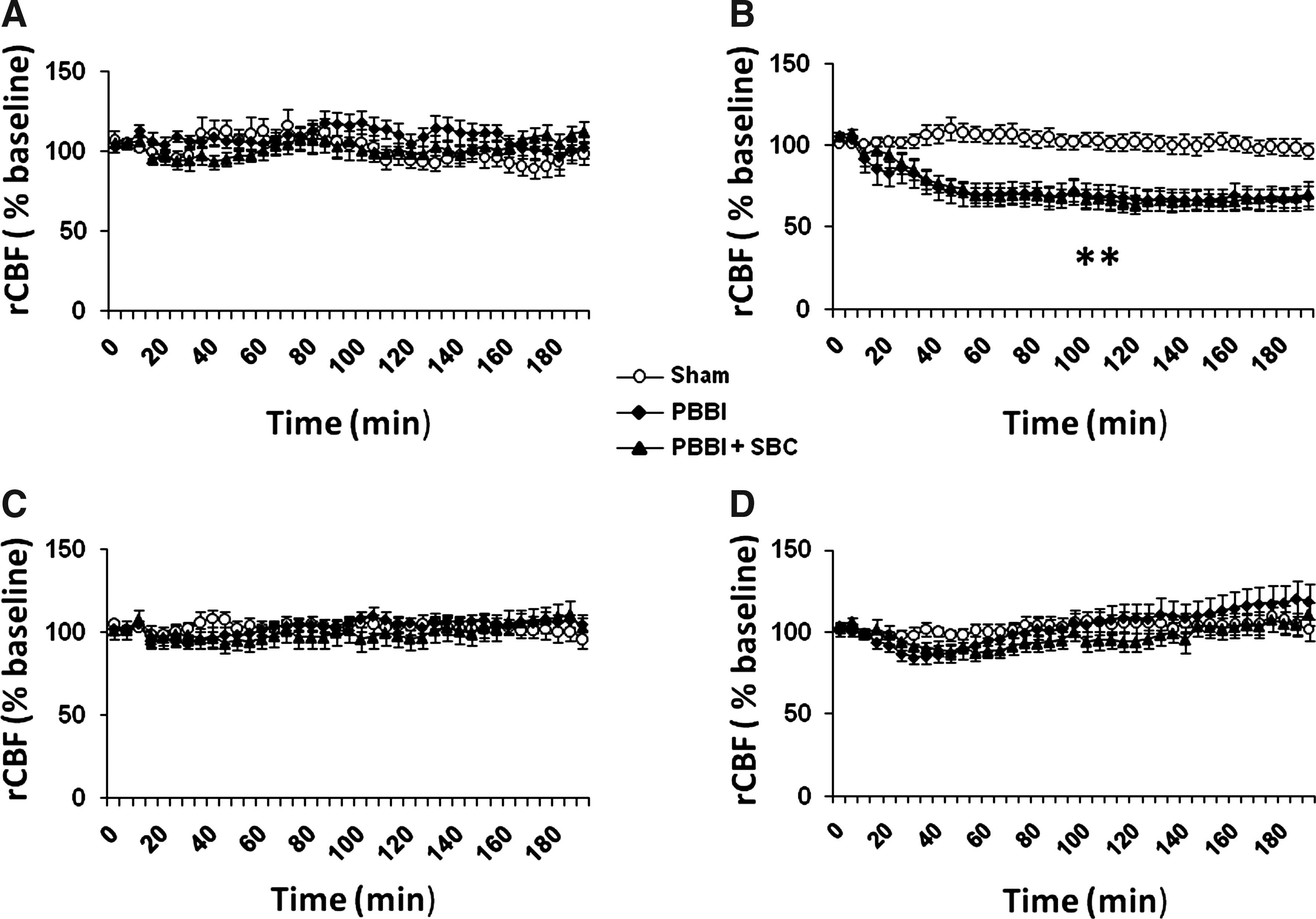
SBC had no effect on acute PBBI-induced hypoperfusion proximal to the injury core. Regional cerebral blood flow (rCBF) was measured at the four brain regions, that is, (
Histology
At 24 hours postinjury, PBBI produced significant increases in BBB permeability to albumin, brain swelling, and ICH in the injured hemisphere, and severe brain damage along the injury track. As previously described (Williams et al., 2005a), the lesion permeated the frontal cortex and progressed through the dorsolateral striatum toward the lateral amygdala. SBC treatment significantly reduced BBB permeability to albumin (44.2%), brain swelling (44.6%), ICH (40.3%), and lesion volume (43.1%) at 24 hours postinjury (Fig. 5). However, at 16 days postinjury, no significant difference was detected on measures of lesion volume between PBBI (83.8 ± 10.9 mm3) and PBBI + SBC (83.0 ± 8.3 mm3).
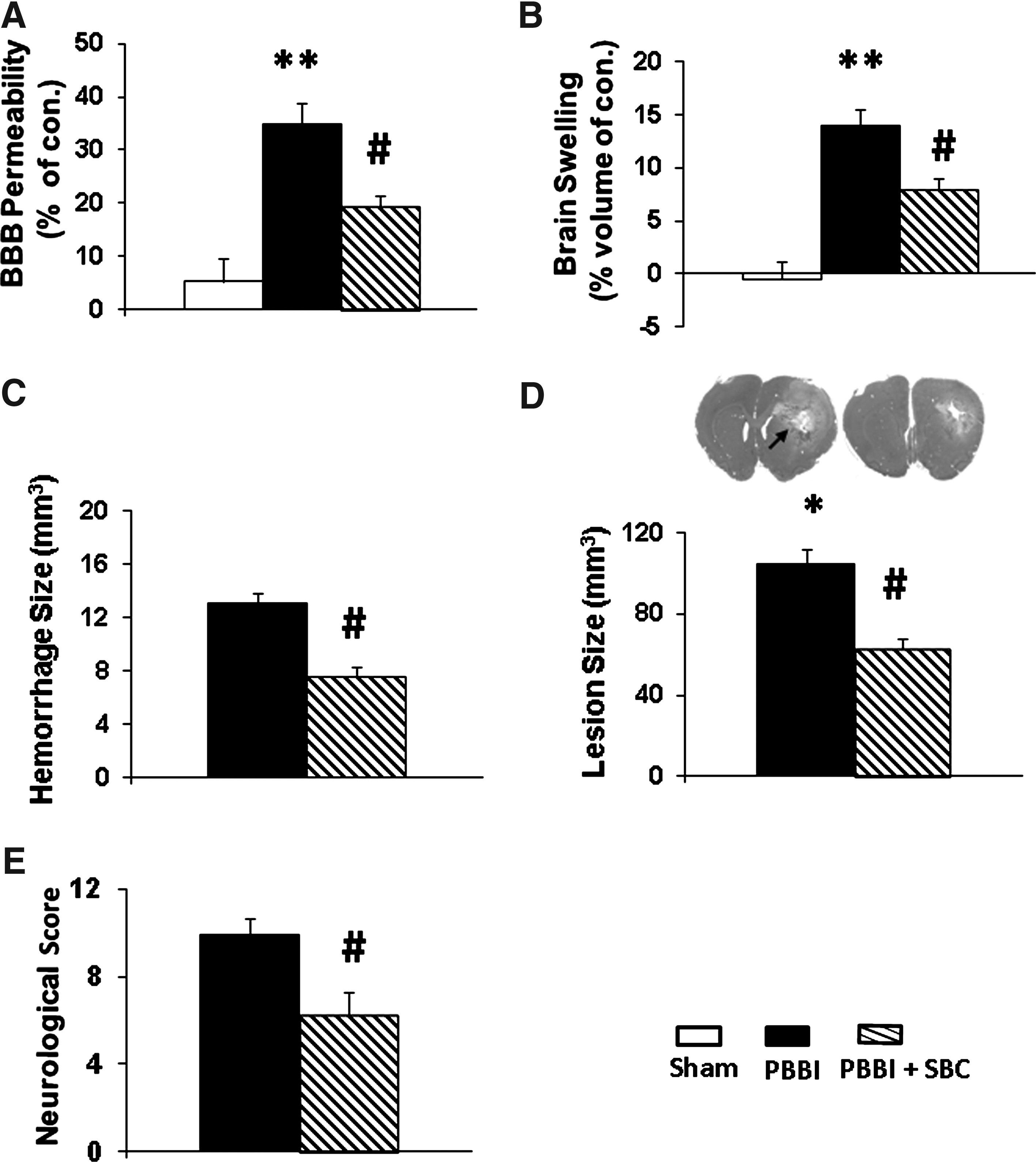
SBC attenuated PBBI-induced histopathological consequences and neurological deficits measured 24 postinjury. (
Acute and chronic neurofunctional outcome
At 24 hours post-PBBI, injured animals displayed neurological abnormalities (Fig. 5E) that were significantly improved by the SBC therapy. MWM performance analyzed using a 3 × 5 analysis of variance (treatment × days), where days served as the repeated measure, revealed a significant injury effect on measures of latency (F2,22 = 15.04, p < 0.05) and swim distance (F2,22 = 12.51, p < 0.05) to the hidden platform. However, post hoc analysis showed that SBC was not effective in reducing PBBI-induced cognitive abnormalities on this task (Fig. 6).
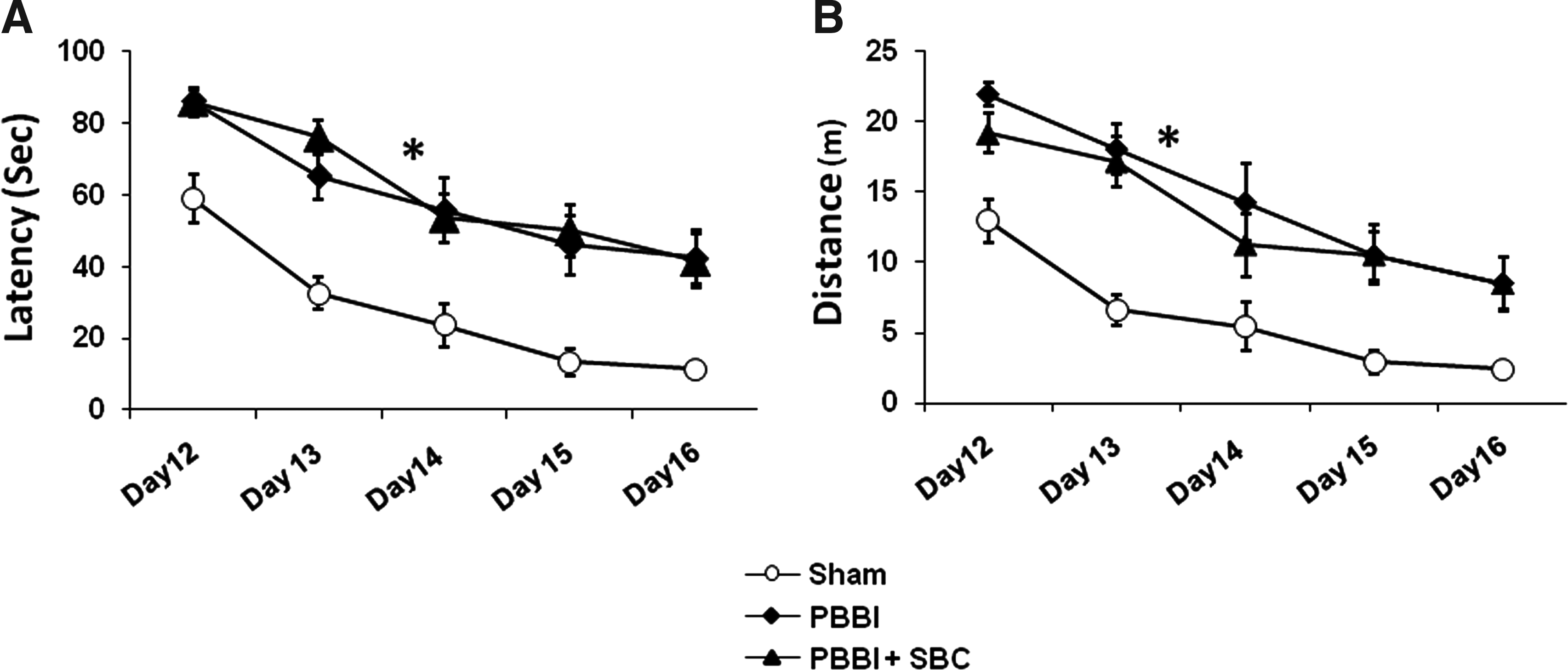
SBC had no effects on PBBI-induced cognitive impairment evaluated by Morris water maze task on days 12–16 (
Discussion
This study focused on the potential neuroprotective effects of SBC on improving acute cerebral physiological dysfunction and reducing histopathological damage caused by PBBI in rats. Results show that 2-hour SBC initiated immediately after PBBI provided significant protection against injury-induced abnormalities in ICP and CPP during SBC that was evident out to 24 hours postinjury. In addition, SBC also protected against acute (24 hours) PBBI-induced brain swelling, BBB permeability, ICH, lesion size, and acute neurological deficits. Overall, these results demonstrate the potential for SBC-mediated neuroprotection in a model of severe, penetrating TBI providing important proof-of-principle therapeutic benefits.
Neuroprotective effects of SBC therapy in treating TBI have been demonstrated previously in animal models using controlled surface cooling (e.g., the use of a cooling helmet or packed ice on the skull, or nasophyaryngeal cooling) to avoid side effects caused by a whole body cooling (Natale and D'Alecy, 1989; Towfighi et al., 1994; Einer-Jensen and Khorooshi, 2000; Trubel et al., 2004; Cheng et al., 2006; Clark and Colbourne, 2006; Covaciu et al., 2008; Doll et al., 2009). These methods have been shown to be experimentally successful and clinically applicable, but they are all significantly limited in their ability to provide sufficient and rapid cooling of deep brain structures, especially in humans, within a short period (Natale and D'Alecy, 1989; Mellergard, 1992; Towfighi et al., 1994; Einer-Jensen and Khorooshi, 2000; Trubel et al., 2004; Cheng et al., 2006; Clark and Colbourne, 2006; Covaciu et al., 2008; Doll et al., 2009; Marion and Bullock, 2009). For example, in an earlier study (Mellergard, 1992) where multiple surface cooling techniques were used to achieve SBC in humans (including cooling helmets, icepacks, and/or nasopharyngeal cooling), significant reductions in epidural or nasopharyngeal temperature by 1°C–6°C could be achieved, but the intraventricular temperature was only reduced by 0.6°C over a 2-hour cooling period. More recently, results of a clinical study of SBC that employed a combination of nasal airflow and bilateral head fans failed to demonstrate significant reductions in the brain temperatures of TBI patients (Harris et al., 2007). At least in part, the difficulties in achieving global SBC in humans may be because the scalp and skull are effective insulators to protect the brain from inadvertent hypothermia. In this sense, the thickness of the human skull structure presents a major challenge to SBC strategies that employ surface cooling techniques for severe TBI patients. Another disadvantage of skull surface cooling is that it quickly becomes impractical when treating penetrating TBI where open wounds exist (Cernak, 2005). Therefore, despite the long-standing existence and appreciation of the clinical potential for SBC methods, its translation to effective clinical applications has been met with limited success.
To address the limitations of surface brain cooling techniques, we developed the CCA cooling cuff method of SBC, which has been shown to be able to safely reduce the global brain temperature by at least 3°C within 30 minutes in rats (Wei et al., 2008a). Notably, a similar CCA cooling method for inducing selective brain hypothermia was also confirmed through a computerized simulation model demonstrating that SBC via CCA cooling is able to achieve a uniform 3.1°C reduction in core brain temperature within 1 hour in humans (Wang and Zhu, 2007). Admittedly, a disadvantage of the CCA cooling cuff method over surface cooling methods is that a surgical procedure is required to insert the cooling cuffs around the CCA. However, for patients who have sustained a severe TBI and undergo various surgical interventions during the acute phase of the injury, the minimally invasive implantation of CCA cooling cuffs may be clinically feasible and should not pose additional serious risk to these patients.
The importance of ICP and CPP monitoring after severe TBI has been well established in preclinical and clinical studies where it has been amply demonstrated that increases in ICP and decreases in CPP are associated with unfavorable outcomes (Carter et al., 2008). Moreover, strategies to reduce elevated ICP and improve CPP often reduce mortality and improve overall prognosis (Olivecrona et al., 2007). In the current study, SBC significantly reduced ICP and improved CPP during the acute postinjury phase, and these benefits were sustained out to 24 hours postinjury with no rebound effects after re-warming. These results are consistent with what has been reported in a number of clinical trials of severe TBI where therapeutic hypothermia produced significant reductions in ICP that were sustained even after re-warming (Masaoka et al., 2000; Gal et al., 2002; Soukup et al., 2002; Clifton, 2004; Hayashi et al., 2005). The finding that SBC can improve ICP and CPP parameters in a model of severe PBBI provides further support for SBC as a therapeutic strategy for TBI.
The cause of elevation of ICP after TBI is largely attributed to brain swelling due to injury-related inflammatory responses. However, ICH also plays an important role in eliciting intracranial hypertension because of the formation of a hematoma (Marmarou, 1992; Hemphill et al., 2005). In the PBBI model, ICH is prominent immediately (within minutes) after the injury because of mechanical tearing and laceration of the cerebral vasculature, whereas brain edema develops more slowly during the initial 24 hours after injury (Williams et al., 2006). Thus, it appears that in the PBBI model, ICH may be contributing more directly to the acute increase in ICP detected immediately after PBBI. In addition, previous studies have demonstrated that the injury-induced inflammatory response (including leukocyte infiltration, upregulation of inflammatory cytokines, increased BBB permeability, and brain edema formation) is evident by 24 hours post-PBBI (Williams et al., 2006; Wei et al., 2009). These orchestrated inflammatory reactions are likely to contribute to the further elevation of ICP to clinically critical levels in the later hours and days after the injury. In the present study, SBC therapy initiated immediately after PBBI caused significant reductions in both ICH and brain swelling formation, which may explain the SBC-mediated neuroprotective effects against injury-induced elevations in ICP and lesion volume.
One of the main dangers of increased ICP is that it can cause secondary ischemic damage by decreasing CPP and causing widespread reduction in rCBF, and consequently a worsened outcome (Kokoska et al., 1998). In this study, CPP was significantly reduced by nearly 20% after PBBI, but the reductions of rCBF were limited to brain regions proximal to the injury site and thus were more likely due to focal neurovascular damage as opposed to decreased CPP.
PBBI causes irreversible brain tissue damage along the injury track, and, similar to other models of TBI, the development secondary injury can produce further tissue damage that extends beyond the injury core (Vespa et al., 2002; Williams et al., 2006; DeWitt and Prough, 2009). One of the important indicators of a successful neuroprotection therapy is to prevent the expansion of brain damage by limiting the secondary injury and ultimately to improve functional recovery. However, experimental research often generates evidence showing that a decrease in brain lesion size may not directly translate into improvement in functional recovery and vice versa (Dixon et al., 1998; Zhao et al., 2005). We previously demonstrated that neuroprotective compounds, such as NNZ-2566 and dextromethorphan, significantly ameliorated PBBI-induced neurofunctional deficits without reducing the lesion size (Lu et al., 2009; Shear et al., 2009; Wei et al., 2009). In the present study, we demonstrated that 2 hours of SBC were sufficient to significantly reduce lesion size and improved clinical signs of neurologic impairment at 24 hours postinjury. However, these acute neuroprotective effects did not translate into improvements in cognitive function measured by an MWM task 12–16 days after the injury, nor did they translate into reduced lesion volume at 16 days post-PBBI. Thus, we hypothesize that the reduction of lesion size observed at 24 hours post-PBBI in the present study after SBC treatment was due to the beneficial effects of SBC on cerebral physiological dysfunction.
In spite of ample evidence illustrating the benefits of experimental hypothermia as an important strategy for providing neuroprotection against TBI, questions remain to be answered with regard to its optimal application as a clinical therapy. It has been recognized that the potential benefits of hypothermic intervention are largely impacted by the target temperatures and/or different durations, time of initiation, and re-warming rate (Markgraf et al., 2001; Ueda et al., 2003; Jiang et al., 2006; Sahuquillo and Vilalta, 2007). Slow re-warming optimizes the hypothermic protection, whereas rapid posthypothermia re-warming in both injured and normal brains leads to adverse consequences, and may even exacerbate TBI-induced pathology and dysfunction (Povlishock and Wei, 2009), illustrating the highly complex balance that must be achieved when using therapeutic hypothermia strategies for treating TBI. We demonstrated that spontaneous re-warming accomplished by discontinuing the ice-cold water circulation did not generate any adverse effects in normal rats, nor did it have any adverse effects in ischemia injured rats (Wei et al., 2008a). Since the hypothermic parameters critically affect the overall outcomes, it is necessary to determine a set of parameters that can provide an optimal neuroprotection, including improvements in postinjury cognition. Accordingly, our studies are focused on examining different combinations of cooling parameters providing optimal efficacy and safety as a therapeutic treatment for severe TBI.
In summary, the current study demonstrates that 2 hours of moderate SBC (∼3°C below the body temperature) induced immediately after PBBI significantly attenuated injury-induced cerebral physiological dysfunction. As a first study using hypothermia as a neuroprotection therapy in the rat model of PBBI, we captured the major, acute clinically relevant pathophysiological events (i.e., ICP, CPP, rCBF, brain swelling, and ICH) of severe brain trauma, and demonstrated that rapid and selective induction of SBC promotes significant neuroprotection during the acute (<24 hours) postinjury phase.
Footnotes
Acknowledgments
This work was supported by core funding provided by the U.S. Army Medical Research and Materiel Command, Combat Casualty Care Research Program.
Disclaimer
Research was conducted in compliance with the Animal Welfare Act and other federal statutes and regulation relating to animals and experiments involving animals and adheres to the principles stated in the Guide for the Care and Use of Laboratory Animals, NIH publication 85–23. Material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting true views of the Department of the Army or the Department of Defense.
Disclosure Statement
The authors declare that no competing financial interests exist.