
Abstract
Hypothermia is an effective neuroprotectant for cardiac arrest and perinatal ischemic injury. Hypothermia also improves outcome after traumatic brain injury and stroke. Although the ideal treatment parameters (duration, delay, and depth) are not fully delineated, prolonged cooling is usually more effective than shorter periods. There is the concern that extended cooling may be hazardous to brain plasticity and cause damage. In order to evaluate this possibility, we assessed the effects of 3 days of systemic hypothermia (32°C) in rats subjected to a sham stroke surgery. There were no detrimental behavioral effects or signs of brain damage. As even longer cooling may be needed in some patients, we cooled (∼32°C) the right hemisphere of rats for 3 or 21 days. Physiological variables, functional outcome, and measures of cell injury were examined. Focal brain cooling for 21 days modestly decreased heart rate, blood pressure, and core temperature. However, focal hypothermia did not affect subsequent behavior (e.g., spontaneous limb usage), cell morphology (e.g., dendritic arborization, ultrastructure), or cause cell death. In conclusion, prolonged mild hypothermia did not harm the brain of normal animals. Further research is now needed to evaluate whether such treatments affect plasticity after brain injury.
Introduction
Besides systemic complications, cooling affects cerebral blood flow and metabolism (Nakamura et al., 1999; Povlishock and Wei, 2009), which could be detrimental if prolonged. Furthermore, hypothermia influences fundamental processes, such as glutamatergic neurotransmission, which plays a role in both neurodegeneration and neuroplasticity (Lo, 2008). Therefore, treatments targeting cell death, including hypothermia, could hamper recovery after brain injury. In many cases, these central complications might be overshadowed by potent neuroprotection thereby leading one to falsely assume that cooling is only protective. Likewise, signs of degeneration in injured animals and patients treated with hypothermia may be misattributed to the initial insult (i.e., masking effect). Safety studies of prolonged hypothermia in normal animals are necessary.
Studies using sham or naïve animals suggest that there are no harmful effects of cooling, but they often involve few animals (e.g., n=3; Colbourne et al., 1999) and/or short treatments (e.g., 3 hours; Truettner et al., 2005). This makes it possible that detrimental effects went undetected. Thus we tested systemic (S) hypothermia (H) for 3 days (SH-3D) at 32°C in rats. This duration and method are similar to those used in clinical trials (MacLellan et al., 2009; Polderman and Herold, 2009). We also assessed unilateral focal (F) hypothermia (H) for 3 (FH-3D) and 21 days (FH-21D) at ∼32°C. This novel technique allows us to cool one side of the brain, which reduces or eliminates systemic complications associated with long-term cooling such as weight loss (Clark and Colbourne, 2007). Note that we used an extreme duration (e.g., 21 days) of cooling to maximize the likelihood of uncovering central side effects. Furthermore, we used a comprehensive assessment of behavior (e.g., skilled reaching, walking, and spontaneous limb use), cellular stress/injury (e.g., electron microscopy and Fluoro-Jade B staining), and neuroplasticity (dendrite arborization) to maximize our ability to detect harmful effects.
Materials and Methods
Subjects
One hundred and forty-four male young-adult Sprague Dawley rats (250–300 g) were used. Rats were housed individually with free access to food and water in standard polycarbonate cages on a 12-hour light cycle (on at 7
All surgeries were done aseptically under isoflurane (4% induction, 2% maintenance in 60% N2O and 40% O2). Local anesthesia was used (0.2 mL of Marcaine SC, Sanofi Canada, Markham, OT, Canada) to minimize post-operative pain. Implanted devices were sterilized before use. Sodium pentobarbital was used for euthanasia (∼100 mg/kg IP).
Experiment 1: Systemic hypothermia
Rats were implanted with telemetry probes (TA10TA-F40, DataSciences, Int., St. Paul, MN) into the peritoneum to measure temperature every 30 seconds (MacLellan et al., 2004). Several days later, they were subjected to a 90-minute sham middle cerebral artery occlusion (MCAO) via lateral craniotomy (Buchan et al., 1992). At 2.5 hours after sham occlusion, temperature was kept normothermic (NORMO-3D, n=8) or lowered for 3 days (SH-3D, n=8) to 32°C (2°C/hour cooling and rewarming rates) with fans and fine-water misters (DeBow and Colbourne, 2003). This treatment potently reduces ischemic cell death (MacLellan et al., 2009).
Rats were tested on the staircase, cylinder, and adhesive tape tasks (Montoya et al., 1991; Schallert, 2006). For the staircase task, rats were food deprived to 90% of their weight during training (two trials/day over 4 weeks) prior to surgery and testing at 4, 6, and 8 weeks after surgery. The accuracy of reaching (% baseline) of the limb contralateral to the sham-operated hemisphere was analyzed. For the cylinder task, paw placements on the cylinder wall during vertical exploration for a 5-minute period were analyzed at 4 weeks after sham stroke (number of contralateral + number of 1/2 co-use/(number of ipsilateral + number of contralateral + number of co-use)×100). For the adhesive removal test, a piece of tape was placed on both limbs. The time to remove the tape was recorded (contralateral time – ipsilateral time) both prior to and 4 weeks after treatment. Fixed brain sections were cut with a cryostat (40 μm) and stained with cresyl violet to determine visually whether damage occurred with the sham surgery or cooling protocol.
Experiment 2: Focal hypothermia—physiological variables
Seven rats were implanted with probes (C50-PXT, DataSciences, Int.) into the peritoneum that measured systolic and diastolic blood pressure (BP), mean arterial blood pressure (MABP), heart rate (HR), and core temperature (Clark and Colbourne, 2007). One rat had a XM-FH-BP telemetry probe implanted (Mini-Mitter Co. Inc, Sun River, OR) to measure cortical temperature (DeBow and Colbourne, 2003). Another had both probes implanted. We did not routinely use brain probes, as they are no longer manufactured, they break easily, and they directly cause brain injury (needle tract). Baseline readings were recorded for 3 days until the cooling device was implanted.
A stainless-steel cooling device (6 mm long×2 mm wide oval-shaped stainless steel tube) was secured to the skull overlying the right motor cortex (Clark and Colbourne, 2007). After surgery, the device was connected via Silastic tubing (Dow Corning Corp., Midland, MI) to an overhead swivel (Model 1 375/D/20; Instech Solomon, Plymouth Meeting, PA) that allowed the rats to move about. Cooling (∼32°C) was initiated over 1 hour by gradually increasing the flow of cold water through the cooling strip. All rats received 21 days of focal hypothermia (FH-21D) followed by controlled rewarming over a 24-hour period (via stepwise drops in water flow) in an attempt to limit complications (Nakamura et al., 1999; Povlishock and Wei, 2009). Data were collected for a further 3 days after rewarming until euthanasia. Brains were sectioned (40 μm) using a cryostat and coronal sections were analyzed after staining with haematoxylin and eosin (H&E) and Fluoro-Jade B (Schmued et al., 1997).
Experiment 3: Focal hypothermia—behavior and histology
Rats were randomly assigned to FH-21D (n=9) or control treatment (tethered to cooling system, NORMO-21D, n=10). Cooling device implantation, hypothermia, euthanasia, and histology were performed as in experiment 2. Rats were tested on the ladder, cylinder, and corner turn tasks before and 3 days after of treatment (Metz and Whishaw, 2002; Schallert, 2006). For the ladder task, the success rate on four ladder crosses was counted. Success rate was expressed as the number of successful foot placements/total number of steps×100. For the corner turn task, the direction of turning was recorded over 10 trials. Rats (<10%) with a baseline turning bias of <30% or >70% were excluded from this analysis, but were otherwise kept in the study.
Experiment 4: Focal hypothermia—electron microscopy
Visualization of cellular ultrastructure was done via transmission electron microscopy (EM) in FH-21D (n=4) and NORMO-21D (n=2) rats. Cooling device, hypothermia, and behavioral tasks were performed as in experiment 3. Rats were anesthetized and transcardially perfused with phosphate buffered saline followed by 4% glutaraldehyde at 3 days after treatment. The brains were removed and pieces of the ipsilateral (to cooling) and contralateral primary motor cortex were analyzed (Colbourne et al., 1999). This qualitative study examined cortical cells for any abnormalities that suggested cellular damage (e.g., dilated organelles, disaggregation of polyribosomes and autophagy) and impending or outright death (e.g., mitochondrial flocculent densities, chromatin condensation, membrane breaks, and apoptotic bodies).
Experiment 5: Focal hypothermia—Golgi–Cox stain
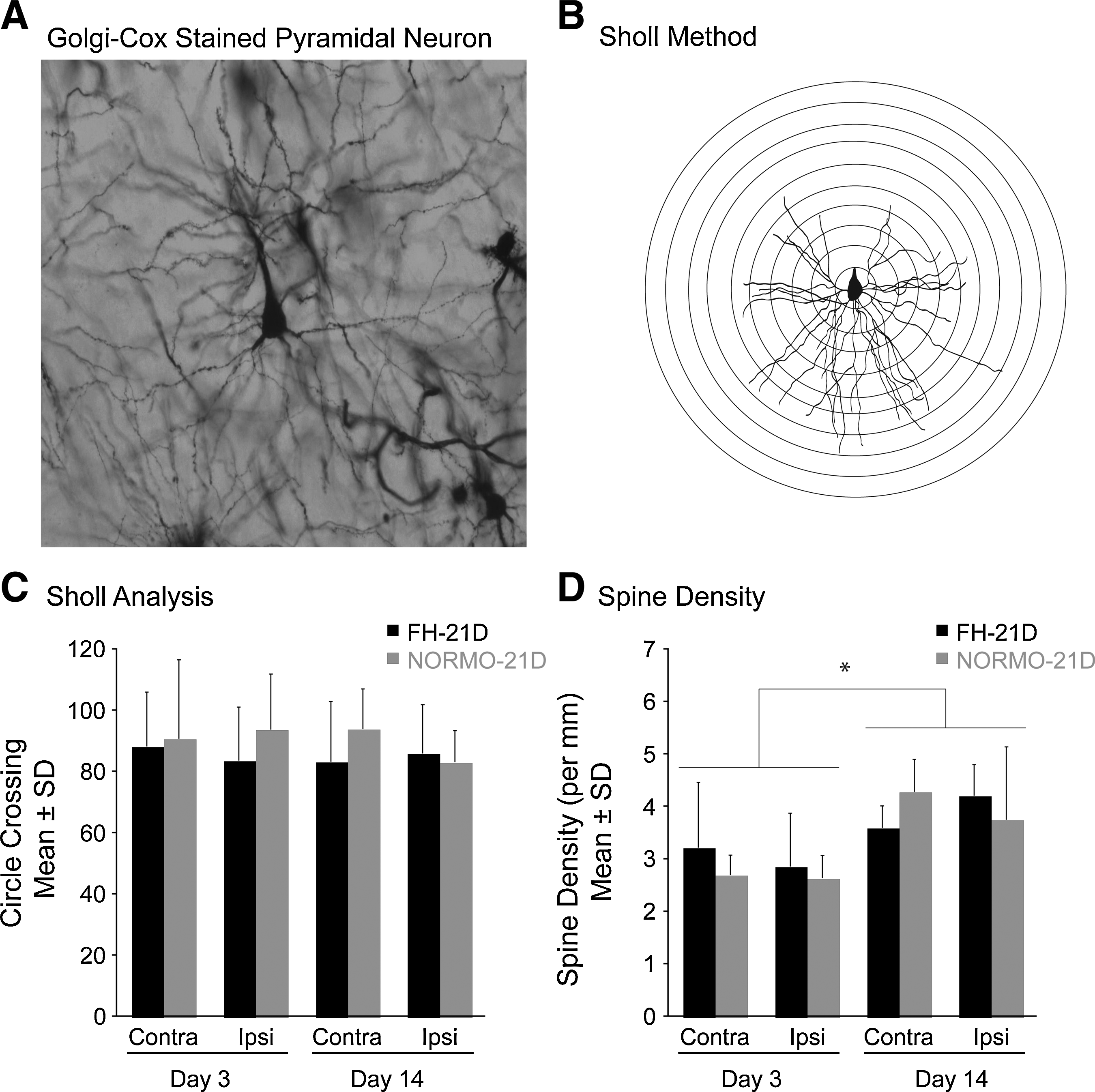
Rats were divided into FH-21D and NORMO-21D groups. Cooling device implantation, hypothermia, and behavioral tasks were performed as in experiment 3. Animals were euthanized at 3 (FH-21D, n=10; NORMO-21D, n=9) or 14 days after rewarming (FH-21D, n=9; NORMO-21D, n=9) as in experiment 3. The tissue was cut with a vibrating microtome (200 μm) and later stained using Golgi–Cox solution (Gibb and Kolb, 1998; Nguyen et al., 2008). For each animal, we traced five cells from the motor cortex in each hemisphere via Camera Lucida using a 20×objective. Sholl analysis was performed on the drawn cells by counting number of ring crossings on a transparent grid of concentric rings. Spine density was measured by drawing the terminal tips of neurons at 1000×(oil immersion) and counting the number of spines per millimeter of dendrite (Auriat et al., 2010).
Experiment 6: Short-term focal hypothermia
Animals were cooled (FH-3D, n=9) or tethered (NORMO-3D, n=9) for 3 days. Behavioral tasks and euthanasia were performed as in experiment 3. Brains were used for Golgi–Cox stain and analyzed for dendritic complexity as in experiment 5.
Statistics
Data are presented as the mean±SD and analyzed with ANOVA (PASW 18). A p-value of ≤0.05 was considered significant.
Results
Thirty-nine rats were excluded from this study. Of these, 36 were euthanized early because of interrupted cooling due to dislocation of the cooling device. By the end of the study, we reduced the number of technical issues. Two rats died of complications caused by brain probe implantation and one spontaneously died while cooling for unknown reasons.
Experiment 1
Body temperature was regulated as desired (i.e., induced cooling to 32°C, data not shown) and repeatedly done (DeBow and Colbourne, 2003; MacLellan et al., 2004). Body weight significantly decreased in SH-3D as compared to weight at the time of sham surgery (p<0.001). This loss persisted for the first week after surgery (SH-3D=22.43 g±6.26, NORMO-3D=2.54 g±4.89). Hypothermic animals achieved similar body weight as NORMO-3D within 1 week. There were no obvious signs of brain damage (lesion) from either the sham operation or cooling (data not shown).
Hypothermia did not affect reaching performance with the contralateral limb in the staircase task (Fig. 1A) at 4 (p=0.240), 6 (p=0.137), or 8 weeks (p=0.983) after treatment. Cooling also did not affect performance in the cylinder (p=0.171, data not shown) or tape removal tasks (p=0.054, data not shown). All groups performed at baseline levels. However, SH-3D animals were slightly faster at removing the tape than NORMO-3D animals.
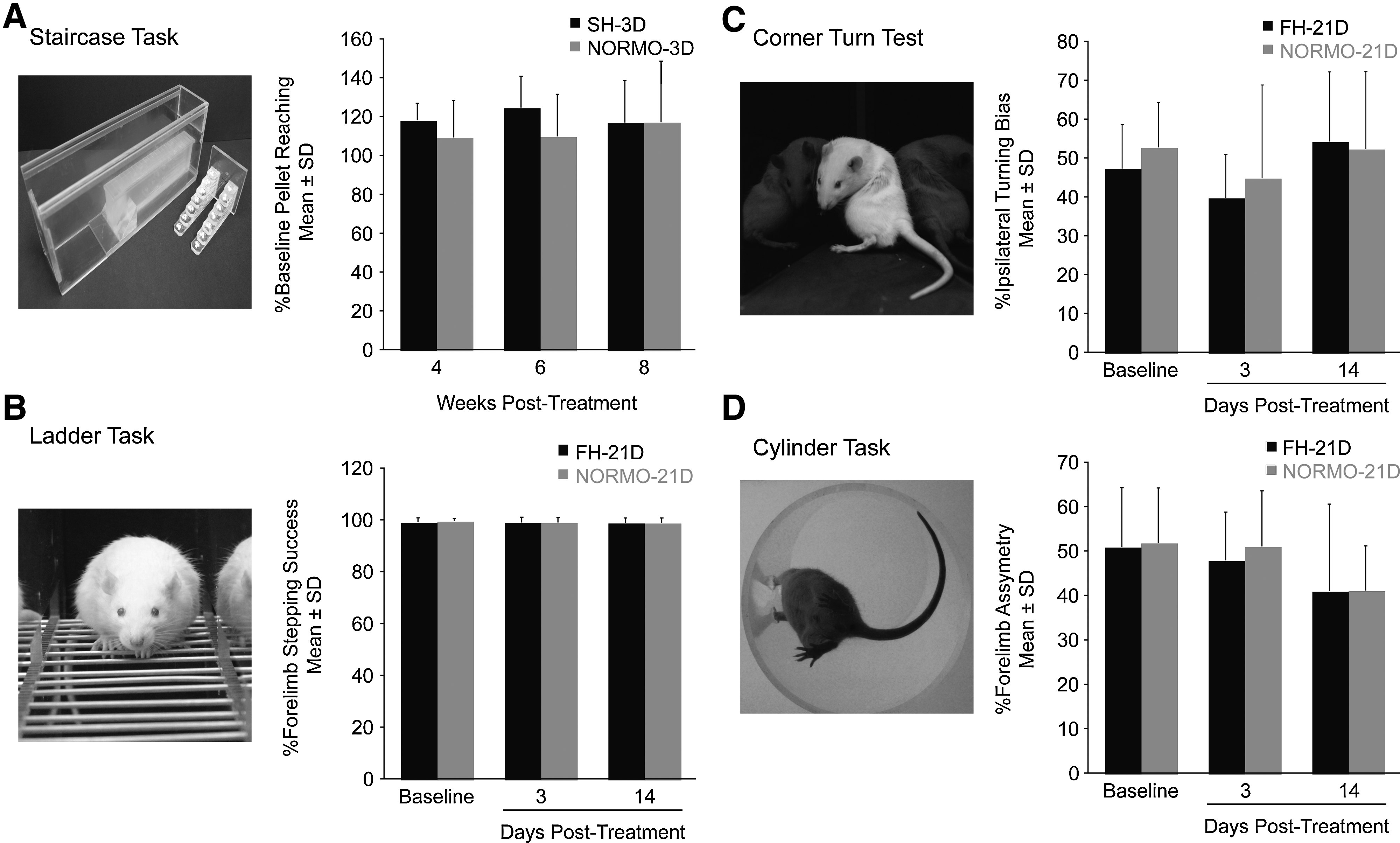
In experiment 1 we used the staircase task
Experiment 2
Brain temperature was lowered throughout the 21-day cooling period (Fig. 2A) as published with shorter treatments (Clark and Colbourne, 2007; Silasi and Colbourne, 2011). Analysis by one-way repeated measures ANOVA, which compared baseline with the cooling period and after the end of hypothermia, showed that core temperature (p=0.008), HR (p=0.003), MABP (p=0.002), systolic BP (p<0.001), and diastolic BP (p=0.008) were all significant (main effects). Planned comparisons showed slight but significant decreases for each parameter over time (Fig. 2B–D). There were no signs of neurodegeneration (e.g., Fluoro-Jade B positive cells or a visible lesion, data not shown).
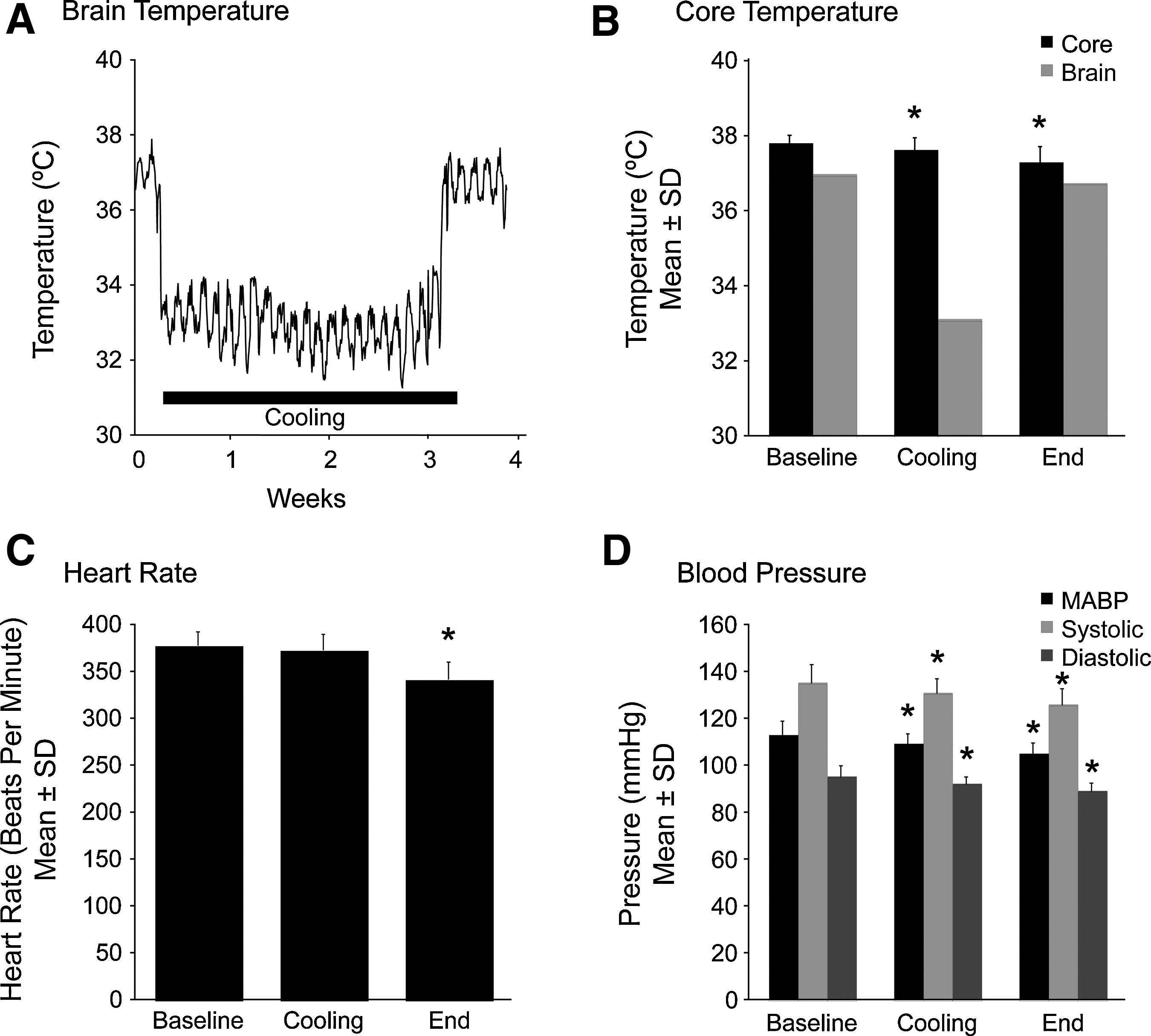
Physiological data from animals exposed to 3 weeks of hypothermia (experiment 2).
Experiment 3
Duration of hypothermia was identical in experiments 3–5, so the behavioral data from these experiments were combined for analysis (Fig. 1B–D). There were no significant differences between FH-21D and NORMO-21D groups at baseline (p=0.210) and days 3 (p=0.934) and 14 post-cooling on the ladder test (p=0.935). Similarly, there were no significant differences at these times for the corner turn test (p=0.051, p=0.705, and p=0.645, respectively). There was a trend toward significance during baseline on the corner turn test where the NORMO-21D group had slightly higher scores than the FH-21D group (p=0.051), but both groups were well within the normal range for this test. Furthermore, there were no significant differences after hypothermia treatment. Lastly, there were no significant differences on the cylinder test on any day (p=0.766, p=0.317, and p=0.989, respectively). Histological results were identical to those in experiment 2 (no injury).
Experiment 4
We examined cellular ultrastructure of the cortex underneath the cooling device by EM. Cooling did not cause cell damage in any of the groups (Fig. 3) and there were only normal healthy-looking neurons. Behavioral results are described above.
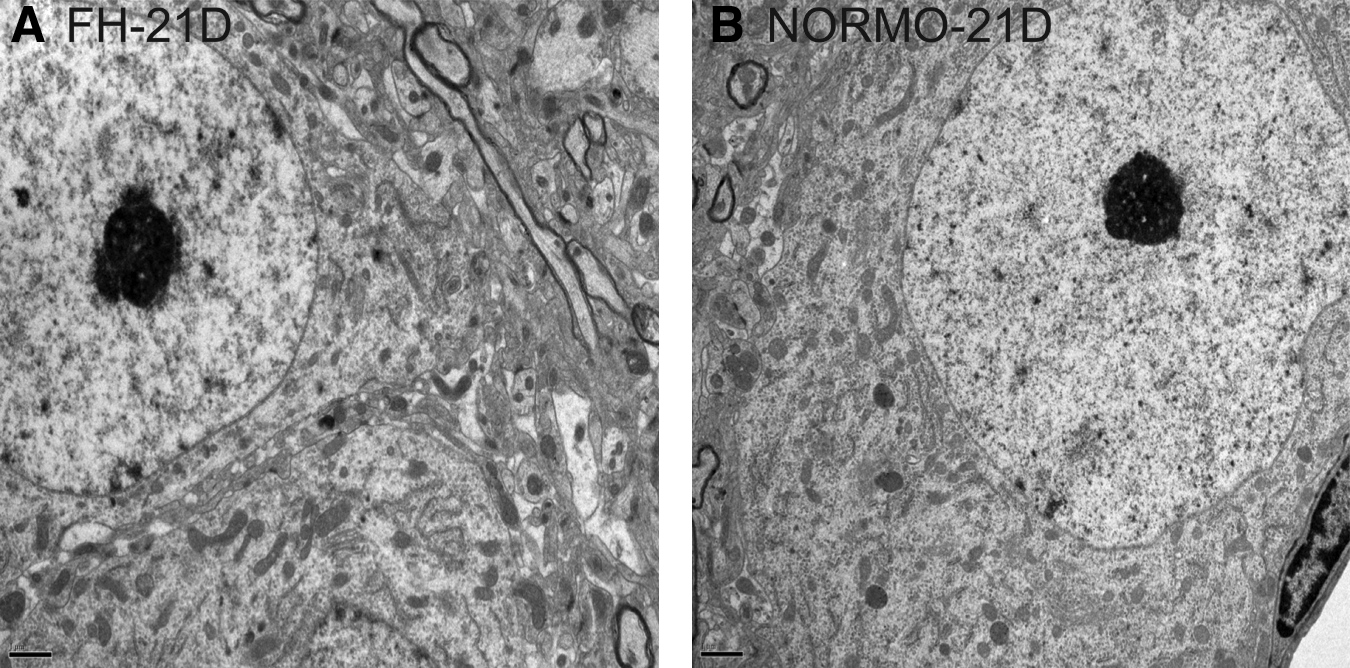
EM visualization of neurons of rats that underwent 3 weeks of cooling (FH-21D) and tethering (NORMO-21D) in experiment 4. There were no signs of neurodegeneration or stress in either FH-21D
Experiment 5
Rats were euthanized at 3 or 14 days after treatment. There were no significant main effects or interactions for Group (FH-21D vs. NORMO-21D), Hemisphere and Time (3 vs. 14 days) for dendritic complexity (p≥0.209 for main effects and interactions; Fig. 4A–C). We found a significant increase (p<0.001) in spine density counts on day 14 (3.98±0.90) when compared to day 3 (2.86±0.84; Fig. 4D). However, we did not find any other main effects or interactions between variables (p≥0.141). Thus hypothermia did not affect spine density. Behavioral tasks results are described above.
Experiment 6
Rats were cooled for 3 days (FH-3D) and dendritic complexity was assessed 3 days later. There were no main effects or interactions for dendritic complexity (p≥0.124) or behavioral scores (p ≥ 0.147; data not shown for cylinder, ladder, and corner turn tests).
Discussion
Moderate and very prolonged durations of hypothermia caused no deleterious behavioral effects or signs of brain injury in normal rats, which illustrates that cooling is safe at least when major systemic complications are avoided. Despite problems such as weight loss and changes in BP, several days of systemic hypothermia can be safely induced in rodents. Complications, however, prevent longer usage. Thus we used our focal cooling system that caused minimal side effects when several days of cooling are used (Clark and Colbourne, 2007). Here we show that this method has only minor systemic effects even when 3 weeks of focal cooling was used. Regardless, neither 3 days of focal or systemic hypothermia nor 21 days of focal cooling adversely affected post-treatment behavior or caused cell death.
Our study has several limitations. First, we did not assess the impact of cooling on brain plasticity after injury, although other studies have begun to evaluate this with encouraging results. For example, we found that 7 days of focal cooling did not alter neurogenesis or plasticity markers after global ischemia (e.g., Silasi et al., in press). Moreover, hypothermia aids neurogenesis in several injury models (Kuo et al., 2010; Silasi and Colbourne, 2011), possibly by elevating neurotrophins and attenuating inflammation (Boris-Möller et al., 1998; D'Cruz et al., 2002; Monje et al., 2003). Our goal here, though, was to test normal rats and avoid the complicating influence of brain injury. Second, in the case of negative findings one must question whether a treatment effect was missed or whether a related treatment would have had an impact (e.g., deeper cooling or faster rewarming). We used extremely long durations of cooling to maximize the likelihood of observing harmful effects. Besides, the use of multiple experiments with several behavioral and histological endpoints strongly supports the notion that prolonged mild hypothermia is safe. Furthermore, the lack of signs of cell death or stress depicted by EM and other assays fit with previous research showing that hypothermia does not alter cellular ultrastructure and physiology (Colbourne et al., 1999; Dong et al., 2001), but it would be prudent for future studies to include additional sensitive endpoints of cellular stress or markers of early stages of cell death (e.g., apoptosis). Third, we cannot directly compare systemic and focal cooling because of multiple methodological differences (e.g., surgical procedures and brain temperature profiles), so we cannot comment on whether one is better with respect to plasticity. However, systemic cooling might be somewhat more effective against focal ischemia (Clark et al., 2009). Fourth, our cooling methods differ in several ways from those used in patients (Polderman and Herold, 2009). Notably, most clinical trials have used shorter treatments (van der Worp et al., 2007), but there are cases of very prolonged cooling (e.g. Hendrick, 1959; Kollmar et al., 2010). Furthermore, clinical studies use additional drugs, such as meperidine to minimize shivering, that may affect outcome directly or through an interaction with hypothermia. Also, whereas the cooling method used in this study would not be used in patients, there is clinical interest in focal brain cooling (Covaciu et al., 2008; Polderman and Herold, 2009). Fifth, one must consider the potential role of age and comorbidities that were not presently evaluated. For example, it appears that cooling is less beneficial in old animals subjected to global ischemia (Corbett et al., 1997), and this may stem from a reduction in treatment efficacy, as well as a harmful effect on brain plasticity, which naturally declines with age (Burke and Barnes, 2006). Sixth, we do not have an explanation for the difference in spine density between 3- and 14-day survival times, but it might relate to transient effects of tethering animals. It was not due to cooling, which had no effect on spine density or dendritic complexity. Finally, a practical concern regarding extended cooling is that it might delay and/or interfere with rehabilitation, thus harming overall outlook.
Further work is needed to optimize hypothermia treatments by maximizing the neuroprotective effects of cooling while avoiding harmful systemic and central side effects. We encourage researchers to include sham animals in their hypothermia studies. While these possibilities temper our conclusions about the safety of hypothermia treatment for the brain, the present and previous findings strongly support the assertion that mild hypothermia is a safe and effective treatment for multiple types of brain injury, especially ischemia.
Footnotes
Acknowledgments
Research supported primarily by a grant to F. Colbourne from the Canadian Institutes of Health Research (CIHR).
Disclosure Statement
No competing financial interests exist.