
Abstract
Extensive animal research facilitated the clinical translation of therapeutic hypothermia for cardiac arrest in adults and hypoxic-ischemic injury in infants. Similarly, clinical interest in hypothermia for other brain injuries, such as stroke, has been greatly supported by positive findings in preclinical work. The reliability, validity, and utility of animal models, among many research practices (blinding, randomization, etc.), are key to successful clinical translation. Here, we review methods used to induce and maintain hypothermia in animal models. These include physical and pharmacological methods. We emphasize the advantages and limitations of each approach, and the importance of using clinically relevant cooling protocols and appropriate monitoring and reporting approaches. Moreover, we performed a literature survey of ischemic stroke studies published in 2015 to highlight the continuing risk of temperature confounds in neuroprotection studies. For example, many still do not accurately monitor and report temperature during surgery (23.5%), even though almost half of these studies (46.0%) use pharmaceutical agents that likely influence temperature. We hope this review stimulates awareness and discussion of the importance of temperature in neuroprotective studies.
Introduction
T
In this review, we limit our discussion to adult rodents (e.g., rats and mice) as they are most commonly used for research in neuroprotection. Furthermore, we focus solely on models of global (e.g., cardiac arrest and forebrain ischemia) and focal (e.g., middle cerebral artery occlusion) ischemia. We begin by discussing common methods to measure temperature in rodents. Next, we review several ways to regulate temperature in anesthetized and nonanesthetized animals. We do not cover clinical cooling methods, as these have been reviewed elsewhere (Polderman and Herold, 2009). Then, we conducted a simple survey of recent preclinical neuroprotection studies to assess the potential for temperature confounds in these models. Throughout, we make several recommendations aimed at improving temperature measurement and control in rodent models of brain injury.
Monitoring Temperature
Temperature fluctuations are common after brain injury. Patients often experience altered temperature, such as poststroke fever (Badjatia, 2009). Animal models also undergo changes in temperature, which vary with model, type and extent of brain injury, choice of anesthesia, animal age, and so on. It is well established that hyperthermia occurs in several models of ischemia (Zhao et al., 1994; Coimbra et al., 1996), whereas others result in spontaneous hypothermia (Hickey et al., 2000; Barber et al., 2004) or they do not affect temperature.
Many neuroprotective treatments (e.g., glutamate antagonist) further complicate this as they have the potential to lower or raise temperature as well (Buchan and Pulsinelli, 1990; Nurse and Corbett, 1996). Drug-induced temperature alterations before, during, and/or after ischemia can readily impact injury and recovery (Polderman, 2008; Sherman and Wang, 2014). Therefore, the importance of temperature measurement after brain injury has been long recognized. Here, we discuss where, when, and how temperature has been measured in animal models of global and focal ischemia.
Timing
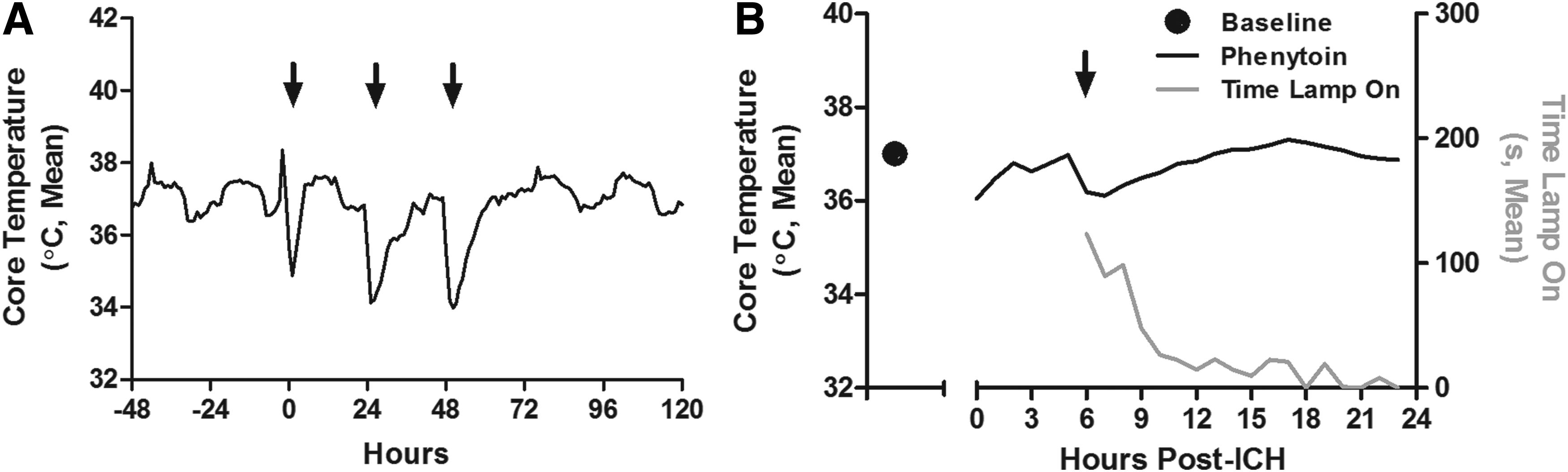
Temperature should be measured during surgery, especially ischemia, and whenever temperature is manipulated or possibly affected. During surgery, we recommend measuring temperature at least every 5 minutes, or more frequently for brief periods of ischemia. After surgery, and if no temperature manipulations are performed, animals should be monitored during the first hour and every few hours in the first day to document and perhaps prevent unwanted temperature changes. Temperature alterations in the first day, even when delayed for many hours, have been repeatedly shown to impact injury [e.g., (Colbourne et al., 1999b)]. During hypothermia induction, the frequency of temperature monitoring is constrained by the cooling method. If a drug is used, measuring temperature every 30 minutes may be needed as some agents rapidly change temperature [e.g., maximal cooling is achieved 10 minutes after MK-801 administration (Colbourne et al., 1996)]. We provide an example here with phenytoin, an anticonvulsant, which decreased core temperature for hours (Fig. 1A). However, when actively regulating temperature (e.g., cooling with fans), one would likely need more frequent monitoring (e.g., every minute) to avoid unwanted fluctuations (Colbourne et al., 1996; MacLellan et al., 2009).
Location
Ideally, one would measure temperature from the ischemic territory in the brain. The most common approach is using a fine needle-type thermocouple probe (30 G or smaller). However, while this can be done in moving animals, the probe causes some injury and contributes to heat loss, risk of infection, and potential alterations in intracranial pressure. Thus, many investigators estimate brain temperature from readings taken elsewhere in the body. Locations, such as the peritoneum or rectum, do not always perfectly predict brain temperature, and rodents can easily experience local brain hypothermia despite maintenance of core temperature during surgery (Busto et al., 1987; Colbourne et al., 1993; Brambrink et al., 1999). Measurements from the skull, temporalis muscle, or tympanic membrane are better predictors of brain temperature (Brambrink et al., 1999). After surgery, surrogate locations (e.g., peritoneum) correlate reasonably well with brain temperature (DeBow and Colbourne, 2003). Regardless of these findings, it is wise to establish the strength of such relationship in each unique setting.
Devices
Wired thermocouple devices are easily used to measure temperature during surgery (e.g., rectum). Except for an occasional measurement, their repeated use after surgery is not recommended as it may cause stress and induce artefacts, such as stress-induced fever, in ischemia models (Clark et al., 2003). Therefore, for prolonged and repeated monitoring, other methods are preferred, such as infrared thermometers (Saegusa and Tabata, 2003; Katz et al., 2013), or wireless devices that can be used in freely moving animals, such as telemetry probes and implanted data loggers (DeBow and Colbourne, 2003; Ellis et al., 2006). Data loggers collect data that can be later retrieved, whereas implanted telemetry probes, commercially sourced or homemade, send information continually or continuously to a receiver. Thus, telemetry probes are better suited to servo-regulating temperature (Colbourne et al., 1996; DeBow and Colbourne, 2003). Telemetry probes can measure temperature from different locations (e.g., brain and core) and can also record physiological variables, such as electroencephalographic activity (Klahr et al., 2015). Although more expensive, we consider telemetry to be the superior approach as it reliably provides frequent, real time, high quality data (e.g., Fig. 1A).
Regulated Normothermia
Maintaining normothermia is often desired, and key to avoiding variable temperature confounds. For instance, during surgery, animals should be adequately draped and kept away from cold surfaces and airflow, and their temperature should be actively regulated, such as with heating pads/lamps, preferably with a feedback control system (Busto et al., 1987; Colbourne et al., 1993; Brambrink et al., 1999). After surgery, animals can be maintained normothermic in temperature-regulated chambers. This has considerable impact on outcome. For instance, we showed that preventing spontaneous hypothermia resulted in considerably more CA1 sector damage with dramatically less variability and much higher statistical power in the rat 4-vessel occlusion model (Colbourne et al. 1999a).
Use of heating pads or lamps are also commonly used to prevent drug-induced hypothermia, such as with NBQX, an AMPA receptor antagonist (Nurse and Corbett, 1996). Such confounds can be prevented, as shown in Figure 1B where phenytoin-induced hypothermia was prevented with a servo-controlled infrared lamp. Though a simple approach, one must be cautious as heating methods can overheat animals or create unwanted temperature gradients in the brain (Plahta et al., 2004). Thus, one should make sure both the brain and core are kept normothermic. Conversely, if animals are hyperthermic or induced hypothermia is required, they can be actively cooled by numerous methods.
Regulated Hypothermia
Here, we summarize approaches to inducing whole body and localized hypothermia in anesthetized and nonanesthetized animals (Table 1).
This is not an exhaustive list; other possible methods include use of Peltier devices, intraperitoneal infusion of chilled saline, etc. References provide a sample application of the hypothermia method.
Rodents do not readily tolerate the prolonged anesthesia required for this method.
Special surgery is required when the system is servo-regulated (e.g., with telemetry probe).
The maximum duration tolerated depends on the agent used.
✗ denotes “no” whereas ✓ denotes “yes”.
Systemic forced cooling
Many methods used to induce systemic hypothermia involve decreasing temperature for short periods (e.g., minutes to a few hours) with the use of anesthetics. For instance, alcohol applied on the skin, infused cold saline, or use of ice packs, cooling blankets, and cold baths have all been used to reduce temperature in rodents during anesthesia (Wang et al., 2010; Lagina et al., 2012). One must be cautious when using anesthetics, however, as these can potentially provide additional neuroprotection and/or introduce/augment temperature gradients (Koerner and Brambrink, 2006). Because anesthetics are not well tolerated in small rodents for extended periods, cooling durations when using these drugs tend to be short and not match the current clinical usage ranging from 1 to 10 days (The Hypothermia After Cardiac Arrest Study Group, 2002; Gluckman et al., 2005; Staykov et al., 2013; van der Worp et al., 2014). Cooling can be achieved without anesthetics, although mild whole body hypothermia is not well tolerated beyond several days in small rodents. One simple approach is to house animals in cold rooms, which can induce or facilitate mild hypothermia (Yanamoto et al., 2001). A more complicated approach is to use telemetry to monitor and regulate temperature, which is then regulated by servo-regulating fans, water misters, and heating lamps (Colbourne et al., 1996; DeBow and Colbourne, 2003).
The sole use of drugs to induce mild to moderate hypothermia has not been yet firmly established in patients, but it is an exciting possibility. Still, several animal studies use drugs to induce systemic hypothermia. There are a wide variety of these drugs, which involve gases (e.g., H2S), cannabinoid agonists, neurotensin analogs, dopaminergic agonists, and capsaicin receptor agonists (Gordon et al., 2003; Leker et al., 2003; Florian et al., 2008; Fosgerau et al., 2010; Katz et al., 2013). The main advantage of delivering drugs is its easy administration and potential to avoid side effects associated with forced cooling. There are disadvantages, of course, including risk of toxicity, and potentially variable control, such as habituation after repeated dosing often required for prolonged cooling. Systemic cooling methods have been combined with other agents, such as HBN-1, a combination of ethanol, vasopressin, and Lidocaine in saline (Katz et al., 2013). The HBN-1 drug combination lowered metabolic rate, blocked shivering, and minimized peripheral vasoconstriction when compared to intravenous induction of hypothermia (Katz et al., 2013). As species differences are a concern, it is necessary to carry out dose-response experiments to adjust dosage for one's study group (Fosgerau et al., 2010).
In animal studies, and in the clinic, cooling the whole body can have systemic effects, such as increasing BP and shivering (Polderman and Herold, 2009). This aspect is more easily monitored in patients, who can be given drugs to decrease discomfort. Pharmaceuticals can also have systemic side effects (e.g., hypotension) and potentially interfere with mechanisms of injury and recovery. Conversely, some drugs are used to simply block the side effects of cooling. For example, an animal study revealed that the use of pethidine, an antishivering drug, with hypothermia is safe and does not affect neuroprotection (Sena et al., 2012). The use of such sedatives to minimize shivering and discomfort is a common clinical practice that still has not been regularly implemented in animal models (Polderman and Herold, 2009). Slow rewarming (e.g., increasing 1 degree every hour) should also be implemented after systemic cooling given that fast rewarming rates have been associated with larger infarct volumes, and greater inflammation after focal ischemia (Berger et al., 2007; Marion and Bullock, 2009). Even slower rates may be needed in patients to avoid any complications (Polderman and Herold, 2009).
Selective brain cooling
Focal brain hypothermia is used in the clinic for infants with hypoxic ischemic injury (Gluckman et al., 2005). Local cooling is also under investigation in adults (Rothman, 2009; Abou-Chebl et al., 2011). Cooling just the brain or part of it could avoid many of the systemic side effects associated with whole body hypothermia (e.g., shivering and infection risk), thereby potentially allowing more aggressive treatments (deeper and/or more prolonged cooling). Nonetheless, focal cooling is not without risk, as it can have side effects such as altering regional blood flow (Kuluz et al., 1993) and worsening bleeding after an intracerebral hemorrhage (John et al., 2015).
As with systemic hypothermia, many of the focal approaches, such as cooling the common carotid arteries, involve the use of anesthesia (Kuluz et al., 1993; Barone et al., 1997; Ding et al., 2004; Wei et al., 2008; Wang et al., 2010). For that reason and others, they are often only useful for brief cooling. External focal cooling without anesthesia can be implemented for long periods. We achieved this by implanting a cooling device (coil or tube) on the skull that was later perfused with chilled water (Clark and Colbourne, 2007). To cool nonanesthetized rats, the device was connected through flexible tubing (encased in a protective shield) and a swivel (to allow mobility) to a cold-water source. An advantage of this method is that it does not appear to alter several physiological variables (e.g., heart rate, blood pressure, core temperature- Auriat et al., 2012) or cause damage even when applied for weeks (Clark and Colbourne, 2007; Auriat et al., 2012). One of the limitations of this approach and others (e.g., Peltier devices) involving surface cooling is that it creates a gradient whereby the cortex is cooled more than deeper brain structures such as the striatum (Clark and Colbourne, 2007; Morizane et al., 2012). These gradients also extend out laterally away from the area under the cooling device (Clark and Colbourne, 2007). The extent of other risks, such as rebound edema with rapid rewarming (John and Colbourne, 2016) are also not well studied.
Current Practices in Neuroprotection Studies
Almost 40 years ago, Borison and Clark developed an extensive list of pharmaceuticals, which has been updated several times since, describing the impact of numerous drugs on temperature (Borison and Clark, 1967). Despite such work, and many original studies and expert reviews in ischemia, the issue of inadequate temperature measurement/control persists (Saver et al., 2009). Thus, one has to wonder how many findings are confounded by spontaneous or drug-induced temperature alterations in both positive and negative studies, leading to both under- and overestimating treatment effects. As such, we speculate that the true success rate could be markedly different had temperature and other physiological variables been adequately considered. While the initial research regarding temperature confounds in neuroprotection studies are decades old, and though there are numerous reviews on this topic, it has been our continuing impression that contemporary studies have not adequately addressed these concerns (DeBow et al., 2003). To determine whether these issues still plague the neuroprotection field, we conducted a small survey of recent publications.
Methods
For this survey, we searched the PubMed database from January 1st to August 31st 2015. Search terms included ischemi*, neuroprotect*, cytoprotect*, and therap*. Articles were filtered to only include rodent models and to exclude review articles. Full text articles were then obtained using EndNote (Endnote X7; Thomson Reuters, New York, NY) and were reviewed to select articles examining the use of neuroprotective therapies for global and focal cerebral ischemia (Fig. 2). Studies that used genetic manipulations, nonpharmaceutical therapies, and/or tissue plasminogen activator as the sole agent were excluded. Included articles were read to determine variables relating to temperature control. Each drug was considered individually, even in studies that used more than one neuroprotectant. All neuroprotective agents examined in the included articles were independently evaluated for their effects on temperature.
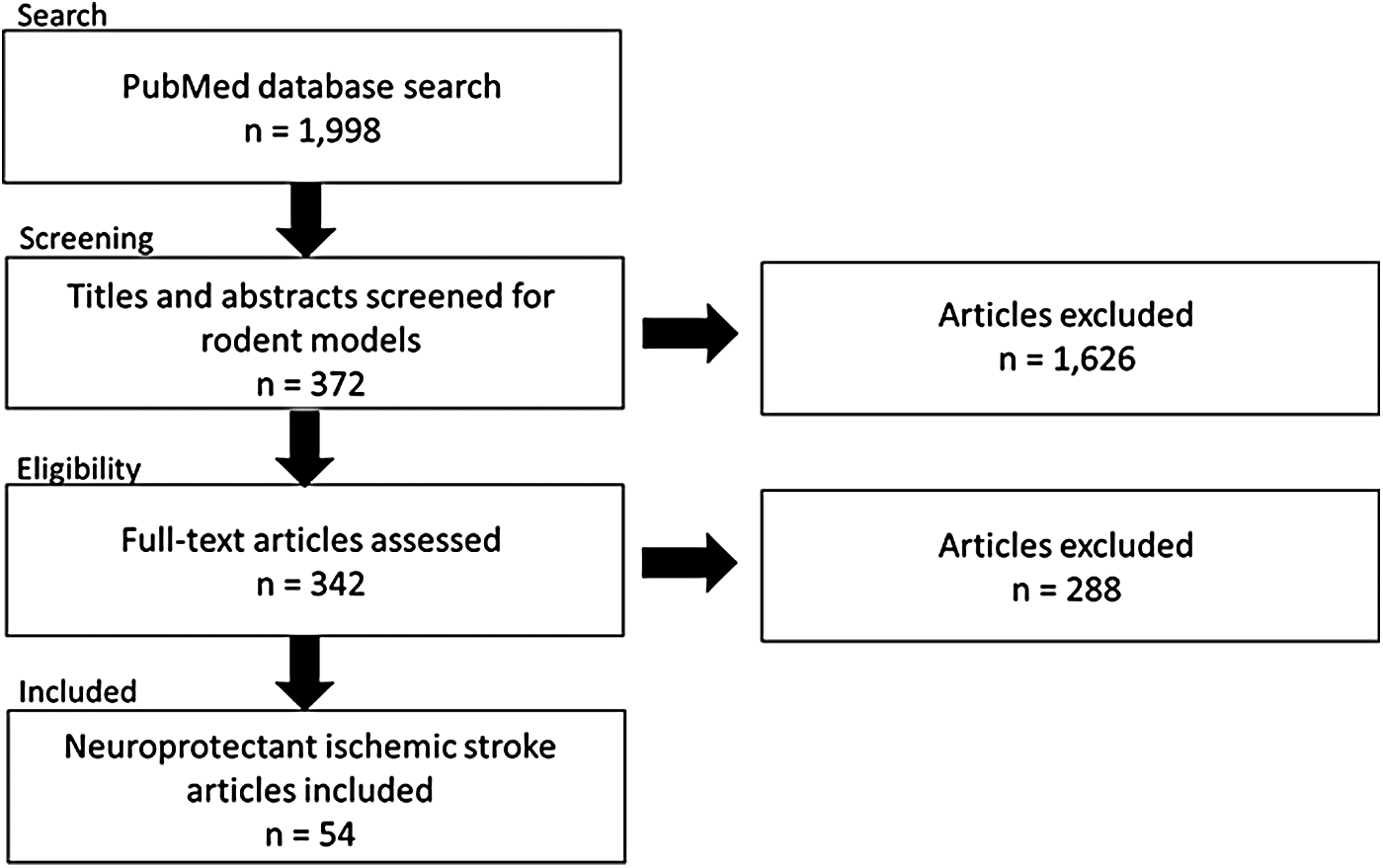
Literature search method flowchart. The PubMed database was searched for articles on neuroprotection in rodent models of global and focal ischemia published between January 1st and August 31st 2015. Search terms included ischemi,* neuroprotect,* cytoprotect,* and therap.* Articles were filtered to only include rodent models and to exclude review articles.
We assessed the following variables: time of neuroprotectant administration relative to stroke onset, neuroprotectant type, animal model, temperature monitoring and maintenance method during surgery, and temperature monitoring following surgery. Furthermore, we noted whether other physiological variables [e.g., regional cerebral blood flow (rCBF)] were evaluated during surgery. We also determined whether each neuroprotectant used was known to affect temperature by searching PubMed and Google Scholar with “(“neuroprotectant”) AND (temperature OR *therm*).” If previous studies did not report on whether the drug affected temperature, then the class of drug or targeted receptor was searched to determine “likely,” “unlikely,” or “unknown” effects. “Likely” was defined as a compound used in other published study or belonging to a family of drugs found to affect temperature, “unlikely” as a drug belonging to a family that was previously found to not affect temperature, and “unknown” indicates no studies relating the neuroprotectant to a temperature effect.
Results and Discussion
Fifty-four articles determining the neuroprotective effects of 63 different agents were included in this survey. Ninety two percent of these articles claimed that the neuroprotectants reduced injury. Of all studies, 76.5% maintained temperature normothermic, while 23.5% did not report having measured or maintained temperature during surgery (Fig. 3A). In contrast, only 33.3% and 17.5% of focal ischemia studies measured rCBF and BP, respectively, whereas only 28.6% of global ischemia studies measured BP, with none measuring rCBF. Of the 57.8% of total studies that did not measure rCBF or BP, only two studies reported it as a potential confound. Physiological variables were generally not monitored after surgery, and indeed, only 17.2% of all the studies reported regulating temperature following surgery recovery, and of these none mentioned whether temperature was actually measured (Fig. 3B).
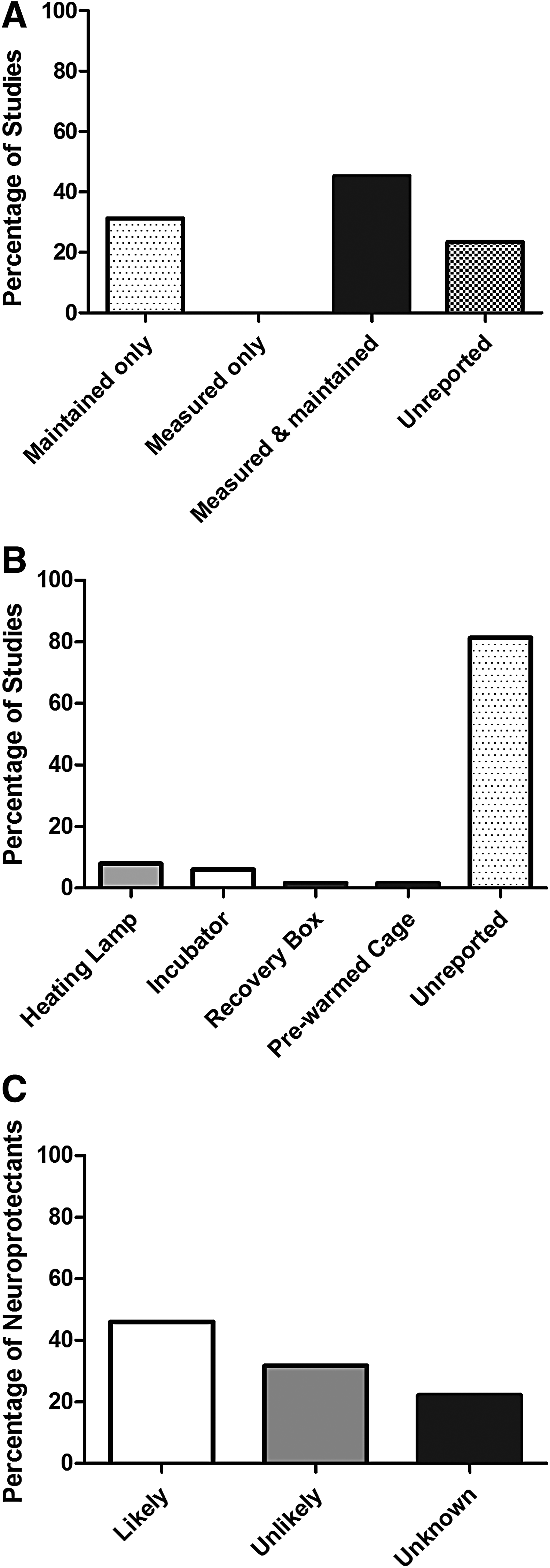
With regard to drug confounds, none of the retrieved studies measured temperature after inducing ischemia despite many (46.0%) using neuroprotectants that we believe are likely to affect temperature (Fig. 3C). Across studies, neuroprotectants were administered anywhere between 360 hours before to 192 hours after stroke induction, with an interquartile range of −0.5 to 1 hour. This suggests that most drugs were administered around the time of stroke induction.
While our survey suggests that contemporary neuroprotection studies inadequately measure and control temperature, there are limitations to consider. Notably, we included a limited sample size (54 articles); so it is possible that this slightly misrepresents the entire literature. This is not our impression, however, and our findings fit with those we recently reported on in intracerebral hemorrhage models (MacLellan et al., 2012). As seen in intracerebral hemorrhage studies, researchers may have simply failed to report whether and how they monitored or regulated temperature. We suspect that this is a somewhat common problem, despite the recent publication of reports advocating improved experimental design, analysis, and reporting to reduce bias and improve translational efficacy in stroke research [e.g., (Dirnagl, 2006; Fisher et al., 2009)].
Conclusion
Despite the well-known impact of hypothermia and hyperthermia on outcome in neuroprotection studies, it appears that many researchers still fail to accurately measure or report temperature after ischemic brain injury and drug administration. Unfortunately, this will likely contribute to further translational disappointments. Our review is intended to shed light on this enduring issue and to provide information on temperature measurement and control methods. For this reason, we provide a series of suggestions to guide researchers when designing experiments or when reviewing studies (Table 2). Along this line, we strongly encourage reviewers and journals to more rigorously consider physiological variables in neuroprotection work and to require such information in the instructions for authors. Interestingly, stroke journals generally do not specifically require such variables to be reported (e.g., in their instructions to authors). Some direct authors to external guidelines (e.g., ARRIVE guidelines) for appropriate scientific reporting. At the very least, we hope for more accurate and complete reporting of temperature measurement and control methods in scientific articles. This should help the translation of neuroprotectants from the bench to the clinic.
Footnotes
Acknowledgments
Research supported by the Canadian Institutes of Health Research to F.C., who is also supported by a Canada Research Chair in Intracerebral Hemorrhagic Stroke award.
Author Disclosure Statement
No competing financial interests exist.