
Abstract
For the treatment of acute cervical spinal cord injuries, a local epidural cooling system using a percutaneous technique was proposed. In this animal study, regional low temperature was obtained stably in the cervical epidural space (CED) without decreasing temperatures at the rectum and the thoracic epidural space. Three stainless steel tubes were inserted percutaneously using the lateral approach into 3 serial interspinous spaces of the neck of 12 beagles under radiographic guidance. Two temperature probes were inserted into the CEDs at the level of the middle cooling tube. A third temperature probe was inserted into the epidural space at the Th13 level. A fourth temperature probe was placed in the rectum as a control. Iced water was circulated in the cooling tubes for 60 minutes. Temperatures were monitored every 10 seconds for 90 minutes, with the minimum temperatures during the period being recorded. The mean minimum temperatures recorded in the dorsal CED (min-CED-dorsal), the lateral CED (min-CED-lateral), the Th13 epidural space (min-T13ED), and the rectum (min-rectum), were 16.0 ± 0.6°C, 22.6 ± 1.6°C, 35.4 ± 0.2°C, and 35.5 ± 0.2°C, respectively. There was a statistically significant difference between the mean min-CED-dorsal and min-rectum temperatures (p < 0.0001). The method introduced above was effective in reducing cervical epidural temperature selectively.
Introduction
T
Most methods previously reported were largely invasive and required certain complicated techniques. It is also required that they be done under general anesthesia during each cooling treatment. The longer the cooling time, the longer the period of general anesthesia is during treatment. Paravertebral muscle cooling for local hypothermia was reported as a minimal invasive technique in rats (Vipin et al., 2015). Anatomically the distances from the epidural spaces to the interspinous spaces are shorter than those to the paravertebral muscle in humans. We intend to create a simple and effective method for epidural space cooling utilizing interspinous spaces. It may be speculated that it is possible to perform this method easily under local anesthesia. This study reports a novel system for cervical epidural cooling by circulation of iced water through interspinous spaces using a percutaneous technique. This is a preliminary report related to the cooling system using animals.
Materials and Methods
Preparation of animals
The laboratory experiments described in this study were conducted on 12 female beagles (mean weight: 9.9 kg, range: 8.2–11.1 kg). This model was chosen because the neck size of beagles is similar to that of human beings. Animal care was in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society for Medical Research and the “Guide for the Care and Use of Laboratory Animals” prepared by the National Academy of Sciences and published by the National Institutes of Health (NIH Publications No. 80-23, revised in 1996). All animal housing and experimental procedures were in accordance with the guidelines of the Institutional Animal Care and Use, Committee of the Animal Research Center, Yokohama City University Graduate School of Medicine, Yokohama, Japan (Approved Protocol F-A-15-020).
Cooling system and experimental procedure for local epidural cooling
The animals were sedated with 5% ketamine hydrochloride 7.5 mg/kg i.m. and anesthetized with pentobarbital sodium 20 mg/kg i.v. Anesthesia was maintained with pentobarbital sodium 40 mg/kg i.v., 5% ketamine hydrochloride 5.0–10.0 mg/kg i.v., and pentazocine 1.0 mg/kg i.v.
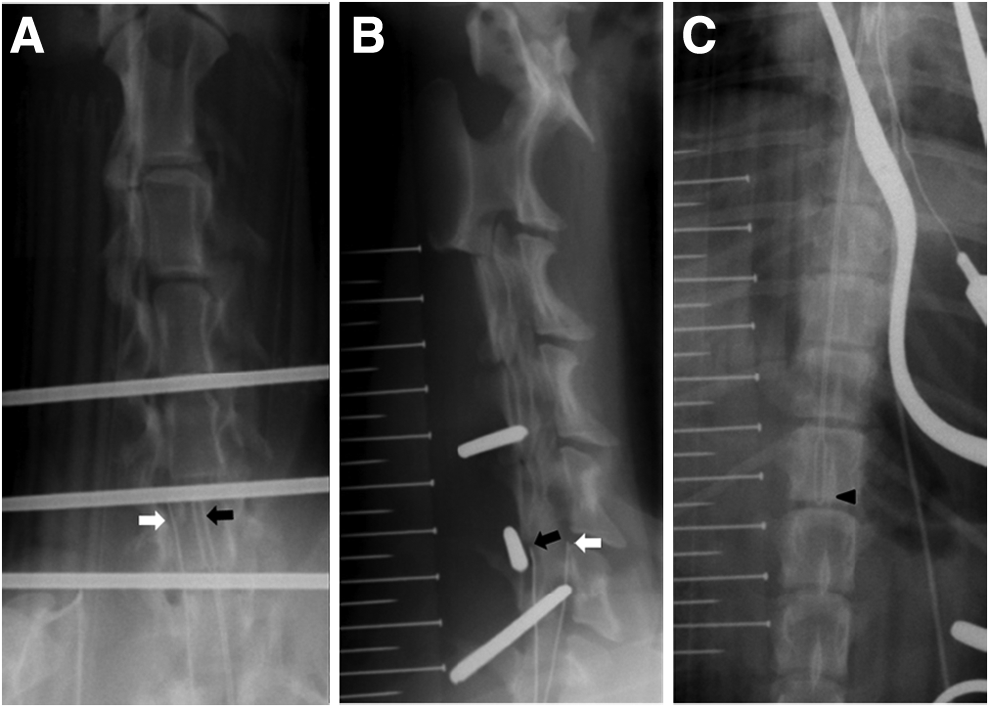
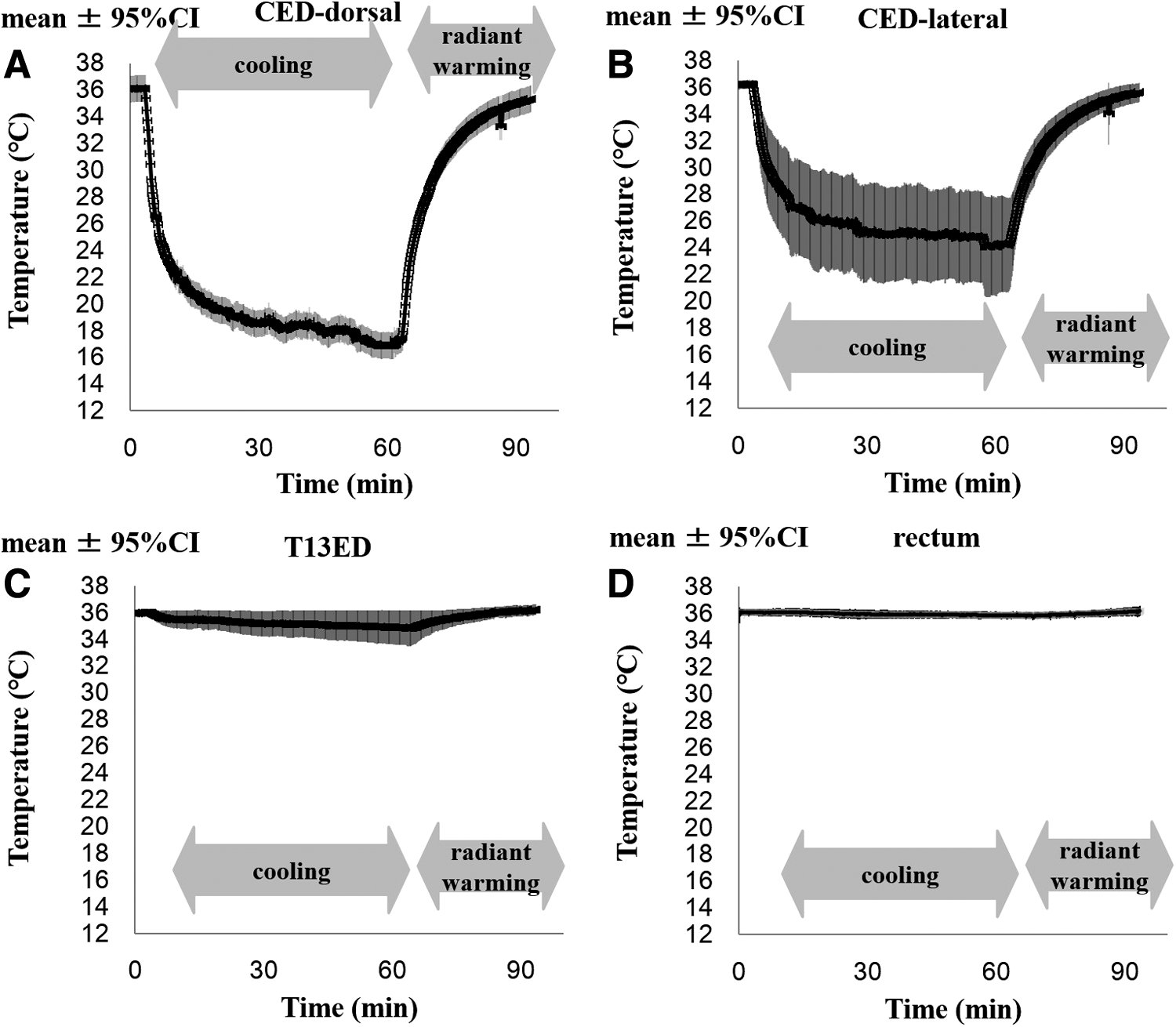
Under anesthesia, three guide wires (Kirschner wires with a diameter of 1.54 mm) were inserted through lateral approach in three serial interspinous process spaces between C3 and C4, C4 and C5, and C5 and C6 (or between C4 and C5, C5 and C6, and C6 and C7) under radiographic guidance (X-ray unit: DC-12 M, Toshiba, Japan; digital radiography sensor: Naomi, XM317B038; RF Co., Ltd., Japan). By using these guide wires, three stainless steel tubes with outer and inner diameters of 2.98 and 1.94 mm, respectively, were inserted percutaneously using the lateral approach (Fig. 1A, B). Because the interlaminar space is narrow and the upper and lower laminae covered the lateral sides of the cord, tubes that were inserted laterally never compressed or injured the cord. The three tubes were connected to an irrigation device (Perista® Pump AP-7000; ATTO, Japan). While maintaining normothermia in the animals using an electric blanket, iced water was circulated in the cooling tubes at a flow rate of 250 mL/min (temperature of input iced water: approximately −0.6°C to −0.3°C). Cooling was continued for 60 minutes (cooling phase) and then turned off for 30 minutes (radiant warming phase). Temperatures were recorded four times during the two phases (Fig. 2A–D). The animals were sacrificed after the radiant warming period.
Temperature acquisition
For inserting the three temperature probes, laminectomy was performed at Th4, which was far from the cooling site. The first spatula-type temperature probe (MF-O-K-TCN-1M; AS ONE Corporation, Japan; range: −50°C to +200°C) was inserted into the dorsal cervical epidural space (CED-dorsal) at the level of the middle cooling tube (between C4 and C5 or between C5 and C6) (Fig. 1A, B). The first wire-type temperature probe (diameter: 0.5 mm, 1-4225-02; AS ONE Corporation) was inserted into the lateral CED (CED-lateral) at the level of the middle cooling tube (between C4 and C5 or between C5 and C6) (Fig. 1A, B). The second spatula-type temperature probe was inserted into the epidural space at the level of Th13 (T13ED) (Fig. 1C). The second wire-type temperature probe (AD-1214; A&D, Ltd., Japan) was placed in the rectum as a control. The four temperatures were monitored using a digital thermometer thermocouple with an SD card data logger (CT-05SD; Custom, Japan; resolution: 0.1°C, range: −50°C to +999.9°C, accuracy: ±(0.4% +0.5°C), and measurement interval: 10 seconds). It should be noted that it was difficult to locate the CED-dorsal temperature probe at the center of the spinal column, with the probe location needing to be corrected many times.
Statistical analysis
The low temperature obtained during the cooling protocols was the primary outcome of the study. The Shapiro-Wilk test was used to test the hypothesis of normal distribution. Normally distributed data were reported as mean ± standard error (SE) and were analyzed using one-way analysis of variance, followed by pairwise comparison with the control group. Corrections for the multiple comparisons were made according to the Dunnett's test. All statistical analyses were performed using JMP 8.0.1 (SAS Institute, Inc., Cary, NC), and p < 0.05 was considered statistically significant.
Results
Twelve dogs were studied in this experiment with recordings between the C4 and C5 levels (n = 8) and between the C5 and C6 levels (n = 4). The following data are expressed as mean ± SE [range from minimum to maximum values; 95% confidence interval (CI)], shown in Table 1: temperatures were monitored every 10 seconds for 90 minutes, and the minimum temperature during that period was recorded. The mean minimum temperature in the CED-dorsal (min-CED-dorsal) was 16.0 ± 0.6°C (range: 13.0–18.4°C; 95% CI: 14.6–17.3°C). The minimum temperature in the CED-lateral (min-CED-lateral) was 22.6 ± 1.6°C (range: 15.1–34.9°C; 95% CI: 19.0–26.1°C). The mean minimum temperature in the Th13 epidural space (min-T13ED) was 35.4 ± 0.2°C (range: 34.1–36.4°C; 95% CI: 35.0–35.9°C). The mean minimum temperature in the rectum (min-rectum) was 35.5 ± 0.2°C (range: 33.9–36.4°C; 95% CI: 35.0–36.0°C) (Table 1).
CED, cervical epidural space; CI, confidence interval; min-CED, minimum CED; min-rectum, minimum rectum; min-T13ED, minimum T13 epidural space; SE, standard error.
There was a statistically significant difference between the mean min-CED-dorsal and min-rectum (control) temperatures (difference: 19.5°C, p < 0.0001). There was a statistical significant difference between the mean min-CED-lateral and min-rectum (control) temperatures (difference: 12.9°C, p < 0.0001). The difference between the mean min-T13ED and min-rectum temperatures, however, was not statistically significant (difference: 0.1°C, p = 0.9999) (Fig. 3).
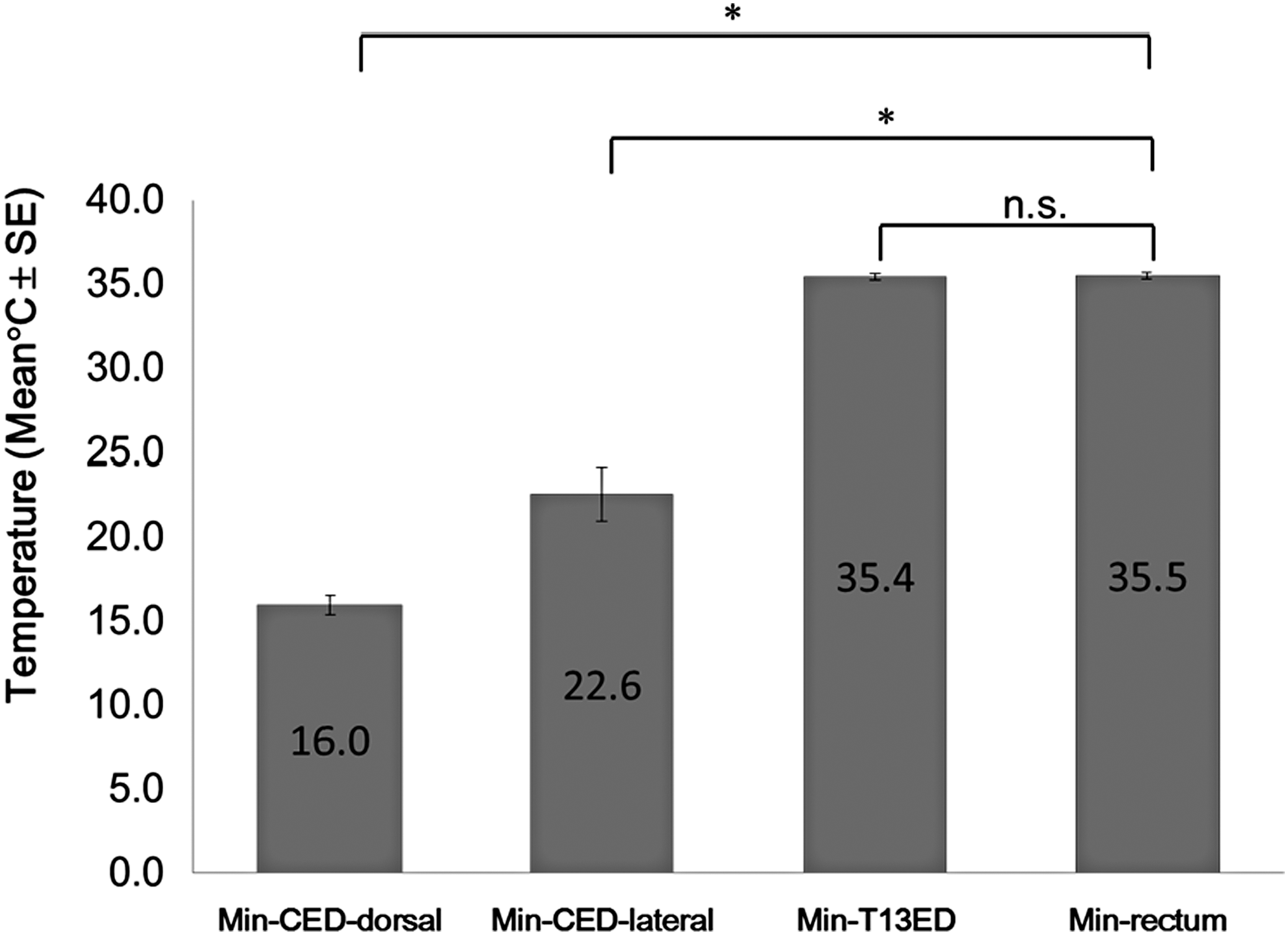
Mean min-CED-dorsal, CED-lateral, T13ED, and rectum temperatures. Data were analyzed by using one-way analysis of variance followed by Dunnett's test against min-rectum as a control. There was a statistically significant difference between min-CED-dorsal and min-rectum. There was also a statistically significant difference between min-CED-lateral and min-rectum. The difference between min-T13ED and min-rectum was not statistically significant. *Difference from control value, p < 0.0001. min-rectum, minimum rectum; min-T13ED, minimum T13 epidural space; n.s., not significant; SE, standard error.
Discussion
Results of this experiment
Using the aforementioned method (Kaneko-Noishiki cooling or KN cooling method), it is possible to ascertain from the results that the cervical spinal cord space can been cooled down (to approximately 16°C) without cooling either the rectum or the thoracic spinal cord space. Thin tubes were inserted percutaneously into the interspinous spaces with circulating iced water. The cervical epidural temperature decreased rapidly and selectively. The procedure is quite simple and the results quite remarkable. The results showed that the temperature at the epidural space of cervical spinal cord can be reduced from 37°C to 16°C according to the flow rate of the iced water circulation.
General anesthesia was used to sedate the dogs that were healthy. It is possible, however, to perform this method clinically under local anesthesia. Short-term general anesthesia may be required during the initial procedure of inserting the tubes, but constant cooling can be obtained with local anesthesia. Thus, complications often caused by long-term general anesthesia and/or general hypothermia may be avoided during the treatment.
Merits of this procedure
The main merit of this percutaneous technique is that it is minimally invasive. It involves selective cooling of only the cervical cord and has minimal effects on the systemic body temperature. General anesthesia may not be needed while cooling, even if the treatment is prolonged for weeks and months. The procedure and maintenance of this regional cooling are simple and easy to do. To prevent pneumonia or bed sores, it is possible to perform this cooling method at bedside in various positions, such as in a sitting position or in a recumbent position.
Another merit of this procedure is the quick start of treatment. Generally speaking, secondary neurological cell damages occur approximately 15 minutes after cervical cord injury (Hulsebosch, 2002). Decompression of the injured spinal cord within 24 hours after trauma has been associated with improved neurological outcomes in human subjects (Fehlings et al., 2012). Meanwhile, it takes only 20–30 minutes to insert three cooling tubes by one self in the above technique. Starting treatment promptly with this system is useful then, and there is a possibility that this regional cooling can be applied clinically in the near future.
Previous studies of systemic hypothermia
Mild systemic hypothermia technologies ranging from 32°C to 34°C were reported to be neuroprotective in central nervous system injuries such as traumatic brain injury (Marion et al., 1993; Shiozaki et al., 1993) and traumatic spinal cord injury (Yu et al., 2000; Hartemink et al., 2004). Some studies, however, reported that systemic hypothermia can cause lethal complications such as cardiac arrhythmia, infection, and coagulopathy (Kwon et al., 2008). Systemic hypothermia was reported using the endovascular cooling procedure (Dididze et al., 2011; Dietrich et al., 2011). It was explained in the study that the controlled temperature (33°C) did not bring any complications. Clinically, however, these cooling methods mentioned above need general anesthesia. Up to date, there is no report of systemic hypothermia without general anesthesia.
Previous studies of local cooling
A number of studies have addressed epidural cooling methods after laminectomy for the treatment of spinal cord injury: irrigation with a coolant in the epidural space in dogs (Albin et al., 1967; Kuchner et al., 2000) and rats (Ha and Kim, 2008; Ok et al., 2012), an epidural cooling saddle in dogs (Hansebout et al., 1975) and humans (Hansebout et al., 1984; Hansebout and Hansebout, 2014), and Peltier modules in rats (Morizane et al., 2012). Although these methods offer neuroprotective benefits after a traumatic spinal cord injury, they require partial laminectomy to access the injured spinal cord. Some procedures require exposure of the dura. Invasive laminectomy requires substantial preparation time and long-term general anesthesia, both associated with some complications. Methods using an epidural cooling catheter offer a neuroprotective benefit in ischemic spinal cord injury and do not require laminectomy (Moomiaie et al., 2007; Purdy et al., 2013). However, it is difficult to apply these methods in cases of edematous injured spinal cords or in cases of spinal canal stenosis or deformity. Because the cooling method presented in this study is performed near the epidural spaces behind the laminae and yellow ligaments, it may be applicable to cases with the above-mentioned complications.
Appropriate epidural temperature for traumatic spinal cord injury
In clinic, an appropriate temperature for local epidural cooling at the injured spinal cord site has not been determined yet. Several researchers have reported that reduction of epidural temperature has a neuroprotective effect. One study reported that maintaining a dural surface temperature of 6°C for 4 hours in conjunction with steroid treatment had a neuroprotective effect in humans (Hansebout et al., 1984; Kuchner et al., 2000). In contrast, another study reported that local hypothermia (16°C for 2 hours) provided significant protection in cases with pressure-induced ischemic damage, but provided less protection for severe traumatic spinal cord injuries (Dimar et al., 2000). Another reported that 3 hours of local cooling at 35.3°C, 30.5°C, and 24.1°C was ineffective in inducing motor function recovery after a traumatic spinal cord contusion injury in rats (Casas et al., 2005). Another reported that secondary neuronal injury occurs over the time course of 15 minutes to several weeks (Hulsebosch, 2002). Furthermore, a recent study reported that moderate and sustained epidural hypothermia (30°C for 48 hours) significantly reduced apoptosis in neurons and glial cells, inhibited the activation of microglia, and improved functional recovery after a spinal cord contusion injury in rats (Ha and Kim, 2008). In another study, motor function in a hypothermia group (dural surface temperature: 33°C for 48 hours) was significantly higher than that in a normothermia group of rats (Morizane et al., 2012). These studies concluded that sustained local hypothermia is effective for treating severe traumatic injuries.
It will be necessary in the future to determine the most appropriate temperature and timing for local hypothermia in humans. The results of this experiment show that temperatures at the site of the cervical spinal cord can be decided easily and exactly by controlling the flow rate of iced water circulation. For this reason, there is a possibility that the KN cooling method can be used clinically in the near future.
Scope of cooling effect
Based on the results, it was apparent that the mean min-CED-dorsal temperature as well as the mean min-CED-lateral temperature were significantly lower than the mean min-rectum temperature. This suggests that the cooling effects might extend along the cervical spinal cord slightly. The cervical laminae in dogs are very thick, and therefore, the cooling effects might be limited to the lateral temperature.
Limitations of this study
This animal study has several limitations, most substantial of which being the fact that the experiments were conducted on uninjured spinal cords. Further studies are necessary to evaluate the neuroprotective effects of the presented technique. Because this method requires no laminectomy, the core of the spinal cord was not approachable; so the core temperature could not be evaluated. Because the spinous processes of dogs are small, they did not disturb the insertion of cooling tubes. Clinically speaking, degenerative changes such as metaplasia of the spine and/or narrowing of the interspinous spaces due to reduced disc height are seen often and must be taken into account, as these changes may make it difficult to insert the tubes. When this method is applied to humans, improvements may be required in terms of the luminal diameter, wall thickness, and quality of the material of the tubes.
Conclusion
This study is the first study that applies percutaneous focal cooling of the spinal cord through interspinous spaces. The ability to cool down the cervical spinal cord space until nearly 16°C without cooling of the rectum and the thoracic spinal cord space was shown. This method is simple to perform and less invasive for patients in that it may be useful as a new technique for selective cooling on the spinal cord under local anesthesia, for treating spinal cord injuries. Improvements to this method will be done and its neuroprotective effects need to be examined.
Footnotes
Acknowledgments
The authors thank Mr. Takashi Kakazu, Research Associate, Department of Neuroanatomy, Yokohama City University, for helping with the experimental procedures and preparing the X-ray system. The authors also thank Dr. Yasuyuki Isono, PhD, for editing the data.
Author Disclosure Statement
The authors report no conflicts of interest concerning the materials or methods used in this study or the findings reported in this article.