
Abstract
Early, prehospital cooling seeks to reduce and control the body temperature as early as possible to protect the brain and improve patient outcome in cardiac arrest, stroke, and traumatic brain injury. In this study, we investigate the feasibility of localized cooling of the porcine brain by using a novel high-flow cold air protocol, which utilizes the close proximity between the nasal cavity and the brain. Five adult pigs were anesthetized and temperature change was mapped before, during, and after cooling by using the proton resonance frequency method on a 3 T Siemens Magnetom Skyra system. Cooling was performed by inserting a tube blowing high-flow (250 L/min) cold air (−10°C) through the nasal cavity for 5–20 minutes. The brain temperature change was measured by using an MRI phase mapping technique utilizing the temperature-dependent proton resonance frequency change. MRI maps showed significant temperature reduction of the porcine brain. On average, a mean whole-brain cooling effect of −0.33°C ± 0.30°C was found after 5 minutes of cooling. The anterior part of the brain was directly exposed to the cold and showed a significantly larger temperature drop (−0.83°C ± 0.51°C) than the posterior part (−0.03°C ± 0.21°C). However, a large variability of the temperature drop was observed between the animals. This variability may be caused by not well-controlled factors confounding the MRI temperature mapping, for example, subject movement, or cooling effectiveness, for example, core temperature or nasal patency. The results indicate that the proposed high-flow cold air protocol allows for localized cooling of the frontal porcine brain, which may be clinically relevant for traumatic injuries of the frontal brain where systemic cooling is unfavorable.
Introduction
I
However, no consensus has been reached on the best and most cost-effective cooling technique (Finley Caulfield et al., 2011) and systemic cooling may not be beneficial in the heterogeneous group of traumatic brain injuries (Yokobori et al., 2011). Several different techniques are in use, most commonly the intravenous injection of cold saline solution (4°C), which delivers a rapid whole-body cooling of the patient (Polderman et al., 2005). Other techniques vary from simple surface cooling methods (Howes et al., 2010), to endovascular cooling catheters (Kandzari et al., 2004), to invasive procedures such as peritoneal lavages (Polderman et al., 2015). An overview of the many different techniques can be found in the review by Schwartz et al. (2012).
A simple portable alternative to the earlier mentioned techniques is the application of a transnasal cooling fluid (Castrén et al., 2010). This technique sprays a specially designed perfluorohexane fluid into the nasal cavity of the patient, achieving a localized cooling of the anterior parts of the brain through evaporation and thermal conduction. The method has been shown to be safe and efficient (Castrén et al., 2010), but requires special and expensive equipment and nonreusable perfluorohexane fluid, causing a high cost of cooling per patient. Another transnasal cooling method uses circulating fluid with 20°C through intranasally placed balloon catheters (Covaciu et al., 2011). However, placing the balloon catheters and the fluid circulation system may be too complex to be further developed into a portable device for emergency medical service.
The potential benefits of prehospital cooling for patient outcome are currently compromised by harmful side effects of available cooling strategies (Arrich et al., 2016). Uncontrolled infusion of cold fluid, for example, is associated with a higher risk of re-arrest and pulmonary edema (Kim et al., 2014). However, a simple and safe early cooling method, such as transnasal cooling by evaporation of perfluorohexane (Castrén et al., 2010) or a neck cooling collar (Giuliani et al., 2016), could be beneficial for patient outcome.
In this study, we propose a cost-efficient and novel technique for inducing short-term localized hypothermia in the porcine brain. Similar to the transnasal cooling method mentioned earlier, we exploit the close proximity of the nasal cavity and the brain, using a cold air compressor to blow high flow (250 L/min) cold air (−10°C) into the nasal airways for 5–20 minutes, thereby reducing the temperature of the brain through heat transfer. We demonstrate the method in five live pigs, with in vivo brain temperature measurements conducted by using MRI phase mapping.
Materials and Methods
Animals
Five young adult pigs (3 months and 45 kg) were used for the experiment. The animals were purchased at Viehvermarktung Horst eG, Horstheider Weg 160, 25358 (Horst/Holst, Germany). After fasting overnight, intramuscular ketamine (10 mg/kg) and xylazine (4 mg/kg) were administered for premedication. After preoxygenation, anesthesia was induced and the animals were tracheotomized. A continuous infusion of fentanyl [0.05 mg/(kg·h)] and propofol [8 mg/(kg·h)] was used for anesthesia. The animals were mechanically ventilated by using tidal volumes of 8 mL/kg. Inspiratory oxygen fraction (FiO2) was set at 0.5, and respiratory rate was automatically adjusted between 14 and 18/min to maintain an end expiratory pCO2 of 35 to 40 mmHg (Fabius MRI; Draeger Medical Systems, Lübeck, Germany). For monitoring of heart rate and oxygen saturation, a 5-lead electrocardiogram and pulse oximetry were used. Two central venous catheters were introduced into the right external jugular vein by using ultrasound, one for volume administration and the other for maintenance of anesthesia and catecholamine administration. An arterial line was placed at either right or left femoral artery. Norepinephrine was administered to keep mean arterial pressure >65 mmHg. The animals were kept under mechanical ventilation and sacrificed 6 hours after induction of stroke in deep anesthesia by an intravenous injection of T-61 euthanasia solution. The induction of the stroke was part of a related study, and testing the cooling protocol was possible during the 6 hour time window before euthanasia of the animals. The stroke was induced in four out of the five pigs by using an experimental stroke model with PHIL™ (precipitating hydrophobic injectable liquid; MicroVention Terumo, Tustin, CA). As discussed later, the embolization was found to not affect the temperature scans and the results of this study.
All animal experiments were conducted in full compliance with local, national, ethical, and regulatory principles, and local licensing arrangements. All animal experiments were approved by the local Animal Care and Use Committee (Behörde für Soziales, Familie, Gesundheit und Verbraucherschutz, Hamburg, Germany).
Cooling protocol
Our cooling protocol exploits the close proximity of the nasal cavity and the brain. By blowing cold air into the snout of the pig, we theorized that a localized cooling of the brain could be accomplished.
To achieve this, a small tube (Ø = 1.27 cm) was inserted 0.5–1 cm into the snout of the pigs and connected to a cold air compressor (MECOTEC cryoAir MINI, Bitterfeld-Wolfen, Germany) delivering dry cold air measured at −10°C and a flow of 250 L/min, which could further be modified (Kaltluft, 2015).
No cooling was performed for the first five minutes to establish a baseline for temperature change for the experiments. Cooling was then turned on for between 5 and 20 minutes, with the temperature measurements continuing for another 10 minutes after cooling was turned off to see a return to the temperature baseline.
MRI temperature measurement
The in vivo brain temperature was measured by using phase-shift MRI imaging. Phase-shift imaging is the most common form of MRI temperature measurement, utilizing the fact that the proton resonance frequency (PRF) is dependent on temperature (Rieke et al., 2008). Changes to the PRF can, therefore, be used to indirectly monitor the in vivo temperature of the body. More specifically, by measuring the phase shift between images, the temperature-dependent change in resonance frequency can indirectly be assessed by a simple equation:
Here, φ(T)−φ(T0) is the phase difference between a reference (baseline) image with temperature T0 and the current image with temperature T, γ is the gyromagnetic ratio, α is the PRF change coefficient of −0.01 ppm/°C (McDannold et al., 2005), B0 is the magnetic field strength, and TE is the echo time. Only temperature changes could be measured by MRI, since the exact reference temperature was not known.
Before calculating the phase difference, phase unwrapping was performed by using the method developed by Maier et al. (2015). This method was specifically developed for MRI phase temperature imaging and reduced both wrapping artefacts and noise. In theory, phase unwrapping represents a linear shift and does, therefore, not affect the temperature measurement.
All imaging was done by using a gradient echo sequence with flip angle (FA) = 10°, TE/repetition time (TR) = 4/44 ms, matrix = 128 × 128 × 32, field of view (FOV) = 260 mm ×260 mm × 112 mm, with one acquisition per minute. The short TE was chosen to minimize signal loss due to large background gradients at the large air/tissue boundary between the inner snout ant the brain. However, for homogeneous tissue without large background gradients, the sensitivity of the temperature mapping method could be improved by using longer TEs.
For validation of our MRI temperature measurements, a temperature probe was inserted into the anterior part of the brain of the pigs with no induced stroke after the MRI measurements. A similar cooling scheme as for the MRI scans was then conducted with the temperature from the invasive probe being recorded. Further, a phantom (5 L water bowl) was scanned by MRI during cooling (blowing the cooled air in front of the base of the bowl) to further validate the MRI thermometry method.
Image processing
Images with movement artefacts were automatically detected and removed by finding outliers (three times standard deviation) in the pixel time curves. To correct for phase drift during the long scan time, a baseline drift curve was established by using three regions of interest located in areas presumed unaffected by the localized cooling. A second-order polynomial fit was then created from the average phase drift in these three regions and used as a baseline for all pixels. To adjust for different starting phases in different tissues, the initial value of the fit was set to the initial phase value of each pixel. The temperature change was then calculated by using the phase difference between each pixel and its adjusted baseline curve in combination with Equation (1).
The images were manually segmented and the brain was automatically divided into two parts, one anterior and one posterior. Mean temperature values were calculated for each region as well as the whole-brain average.
Results
All five pigs were successfully scanned and postprocessed. Some images in pig 4 had poor quality due to motion artefacts and were removed from the temperature calculation. A demonstration of the second-order polynomial baseline fit used for phase drift correction and the effect of phase unwrapping can be seen in Figure 1, and a comparison between the MRI measured temperature and the probe temperature measurement in pig number 1 can be seen in Figure 2.
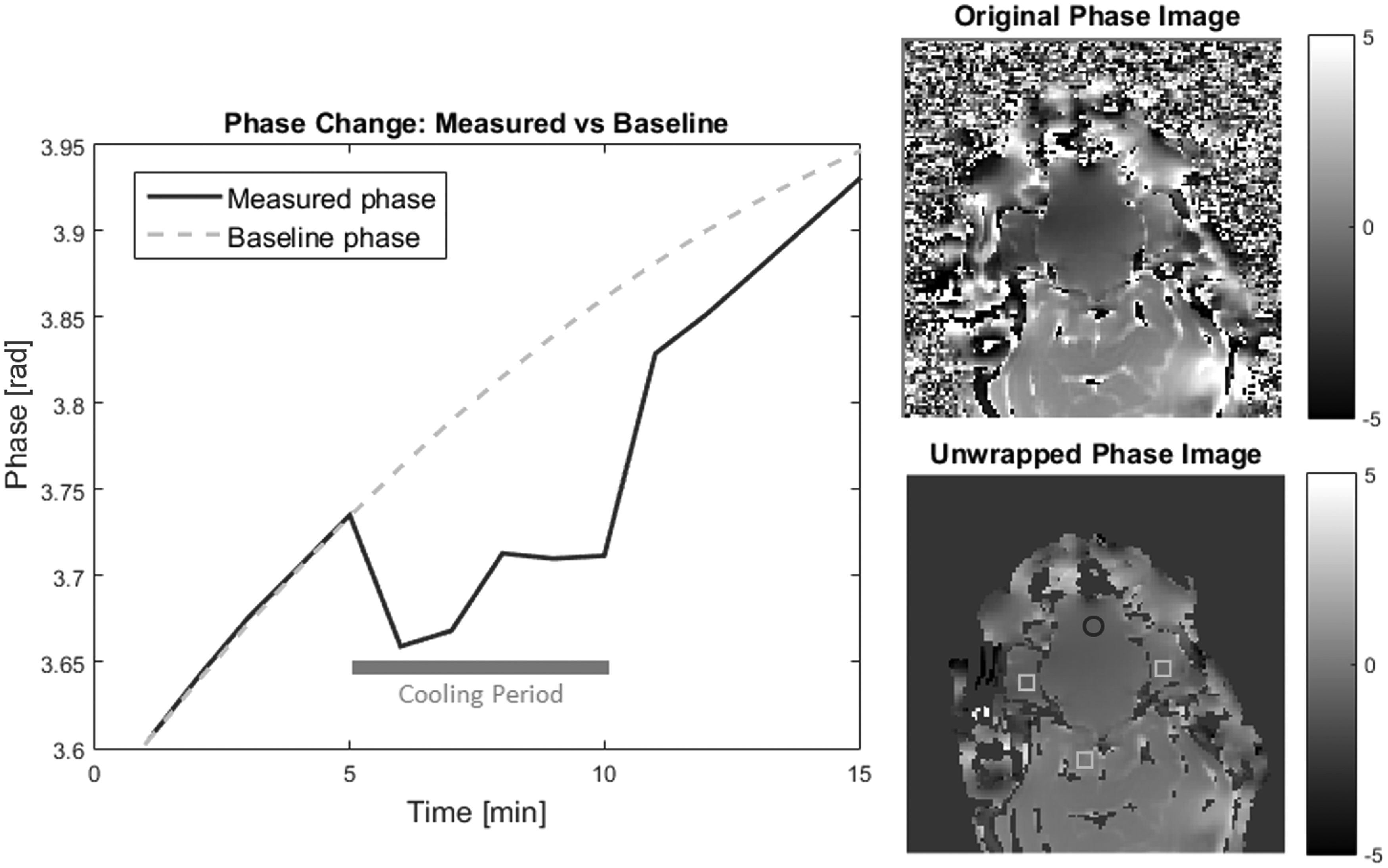
Phase imaging and processing of the MRI temperature measuring method. Left: Measured phase in a cooled region (o) of the brain vs. the baseline (□). Region locations are denoted in the unwrapped phase image on the lower right. The temperature in each pixel was calculated by using the difference between the baseline and the measured value. This allowed for efficient correction of the phase drift over time. Note the clear deviation from the baseline during cooling (time points 6–10). Right: The effect of phase unwrapping (original top, unwrapped bottom). A clear reduction in noise and more homogeneous phases are seen in the unwrapped image.
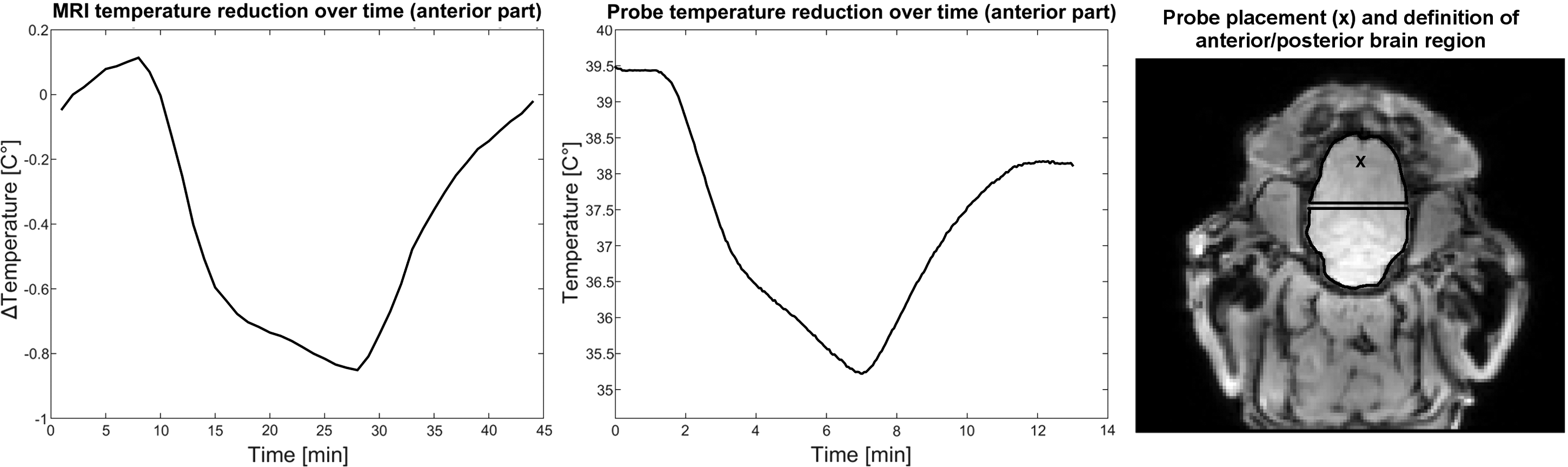
Comparison between the MRI and probe temperature measurement of pig 1. The MRI measurement was average over the anterior part of the brain, and the temperature probe was inserted after MRI into the anterior part of the brain close to the nasal cavity. Notice the similar shape of the curves. Also, note that the measurements were conducted at two separate times with different time frames and that the probe only measures the temperature at one point in the brain, whereas the MRI measurement is averaged over the anterior part of the brain.
The MRI temperature measurement curve of the water phantom shows a rapid decrease during cooling and a slow increase after cooling stopped. Further, only the lower part of the phantom was cooled, since the cold air was blown at the base of the water bowl and no active heating or convection took place in the phantom (Fig. 3).
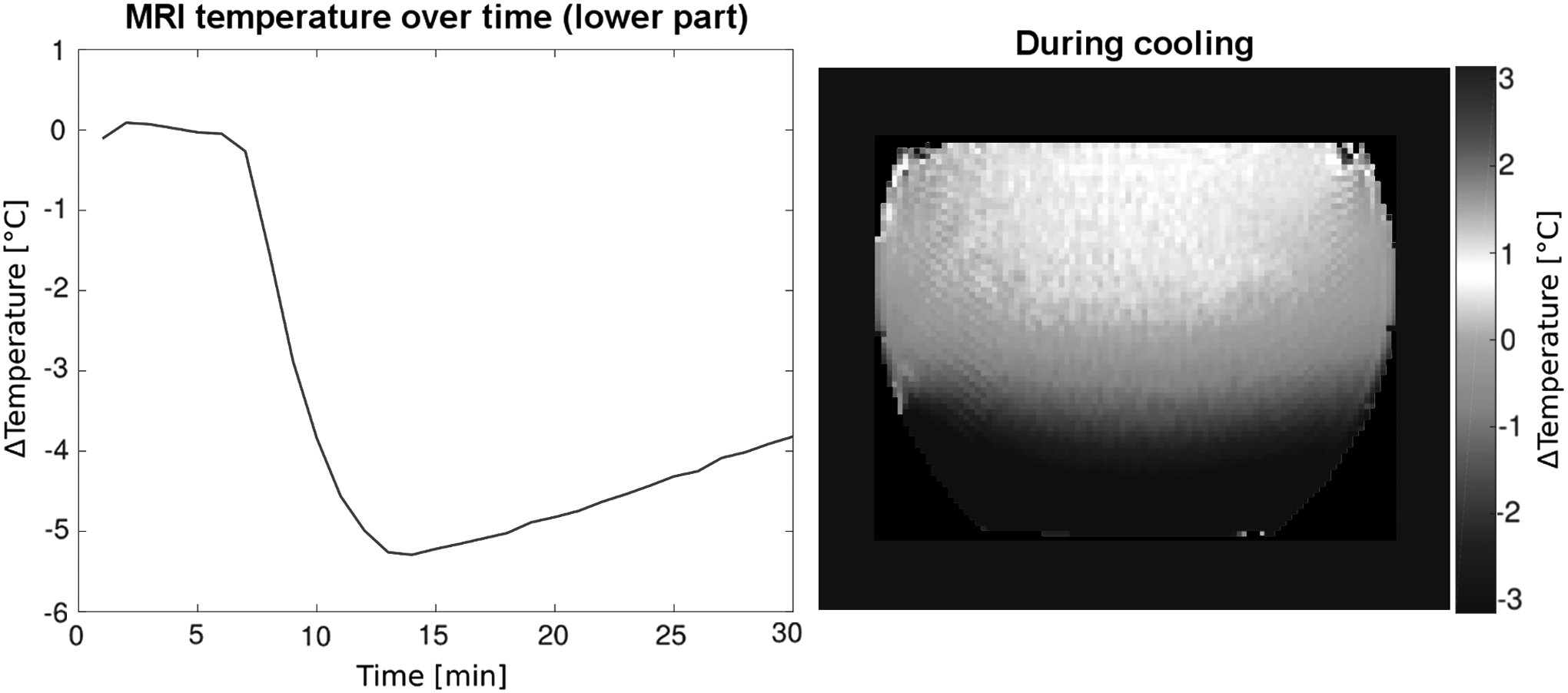
MRI measured average temperature in the lower part of the phantom. Notice that the cold water stays at the bottom of the bowl and that the temperature increase after cooling is much slower, since no convection or active heating takes place in the phantom.
A mean group temperature reduction of −0.33°C ± 0.30°C was found for the whole-brain average during 5 minutes of cooling. When considering the anterior and posterior part separately, the mean temperature reduction was stronger for the anterior part with −0.83°C ± 0.51°C and almost not visible for the posterior part with −0.03°C ± 0.21°C. The individual temperature changes averaged over different brain parts during the three cooling periods are visualized in Figure 4 and summarized in Table 1. Representative temperature images from the cooling periods are seen in Figure 5.

Average temperature in the anterior part of the brain during the three cooling periods. Before cooling, during cooling (5 minutes after cooling started), and 10 minutes after cooling stopped. A significant (p < 0.05) temperature reduction is seen during the cooling period in all five pigs.
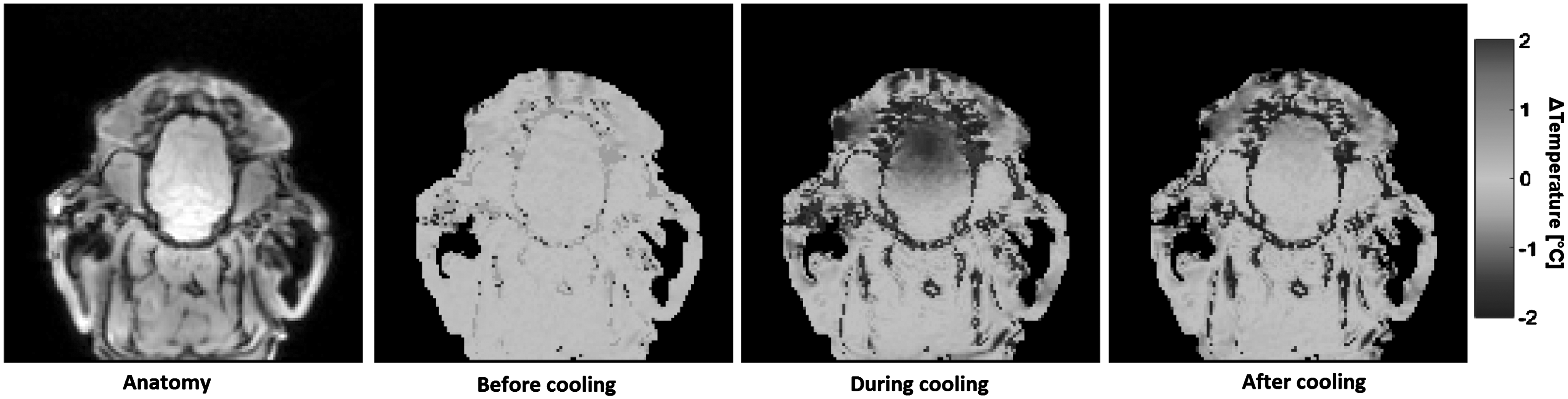
Anatomy and temperature maps during the three cooling stages (pig 3). Note the clear temperature reduction in the anterior part of the brain during cooling as well as the return to normal after cooling has stopped.
Temperature change was averaged for the anterior, posterior, and whole-brain region.
Pre, before cooling; During, 5 minutes after cooling started; Post, 10 minutes after cooling stopped.
A significant temperature reduction (Wilcoxon rank-sum, p < 0.05) was observed in the anterior part of the brain in all five pigs during 5 minutes of cooling. This was not the case for the whole-brain average, with only three pigs showing significant whole-brain temperature change, or for the posterior part of the brain.
The temperature in the anterior part of the brain after only 3 minutes of cooling was on average 73% ± 14% of the minimum temperature reached, indicating a fast-acting cooling effect.
Discussion
We have demonstrated that localized cooling of the porcine brain is possible by using high-flow cold air passed through the nasal cavity. A fast and significant cooling effect was seen in all five animals. The observed temperature reduction was considerably higher in the anterior parts of the brain, which is consistent with the location of the nasal airways and indicates that the cooling did, in fact, occur through upper airway exposure.
The proposed protocol for localized brain hypothermia requires minimal preparation, delivers a fast cooling effect to the brain, and is easily switched on and off. This gives the method a lot of flexibility and control, making it well suited for both large and small animals. Other than a suitable cooling device, the method requires no sophisticated technology or knowledge and can be easily applied by anyone wishing to perform hypothermia studies in animals.
We found an average initial cooling rate of the whole brain of 0.33°C in 5 minutes, which extrapolates to a temperature reduction of 4°C in 1 hour, if we assume the initial cooling rate constant for the whole time. A cooling rate of 4°C/h is competitive with other cooling techniques (Schwartz et al., 2012) like rapid infusion of refrigerated fluid (4°C/h), extensive surface cooling with ice packs (0.9°C/h) or high flow ice cold water circulation (3°C/h) and endovascular cooling catheters (3°C/h). The other transnasal cooling technique using evaporating perfluorohexane fluid reduced tympanic temperature by an average of 1.3°C before hospital arrival (26 minutes) (Castrén et al., 2010), and using circulating fluid with 20°C through intranasally placed balloon catheters reduced average brain temperature by 1.8°C in 60 minutes (Covaciu et al., 2011). Our transnasal high-flow cold air cooling method would deliver an average whole-brain temperature reduction of 1.7°C in 26 minutes or 4°C in 60 minutes, respectively.
Combining transnasal high-flow cold air cooling with surface cooling of the head and neck by using ice packs or circulating ice-cold water would reduce brain temperature more rapidly and nonlocally, which could facilitate whole-brain neuroprotection more efficiently and faster.
A drawback of the method is the direct exposure of the airways to a high flow of dry cold air, which damages the nasal mucosa (nose bleeds were seen in all five animals). The nosebleeds were observed by low quantities of light red mucus coming out of one nostril, when the cooled air was blown into the other. No strong bleeding was observed, and no red mucus came out of the nostrils after cooling (air blowing) was stopped. Severe mucosal damage, anticipated by the high air flow rate into the snout, may be diminished due to the cooling effect of the cold air and the only short-term application in our feasibility study. Therefore, the method is best suited for short-term induction of hypothermia and not for long-term cooling maintenance. A future air cooling device, able to deliver colder air at lower flow rates, may reduce drying-out and, therefore, damage of the nasal mucosa and maintaining an effective cooling due to air colder than −10°C.
As seen in the temperature images, the system does not provide a homogeneous cooling to the whole brain. This is unsurprising since only the anterior part of the brain is directly exposed to the cold air, but it could reduce the effect of the method in some cases, such as a posterior cerebral artery stroke. However, perfluorohexane-based transnasal cooling sprays has shown promise in clinical trials (Castrén et al., 2010), and they also provide a inhomogeneous cooling of the brain. However, a localized cooling effect may be preferable in traumatic injury of the frontal brain.
Temperature changes were recorded by using MRI phase imaging. Although other temperature measurement techniques such as infrared imaging (Siewert et al., 2014) or temperature probes might be more accurate, they do not give the in vivo brain temperature maps possible by MRI. MRI thermometry was, therefore, considered a superior choice for our purposes (Winter et al., 2016).
Moreover, the validation comparison between MRI temperature and an inserted temperature probe showed a good agreement in the shape of the recorded temperature curves. Note that although there is a difference in the measured temperatures and time scales between the two methods, the probe curve represents only one spot in the brain, which was probably close to the nasal cavity, and that the MRI temperature curve is averaged over a larger region. Further, the animal (pig 1) was already weakened due to its long time under anesthesia and, therefore, the animal's metabolism may have not sufficiently counteracted the cooling as it did in the earlier cooling experiment in the MRI scanner. Since multiple clinical studies already demonstrated the maturity of MR thermometry for in vivo applications [see conclusion section of Winter et al. (2016)], no more animals were allowed by the local animal care and use committee for further validation of the MRI method.
It is clear from Figures 4 and 5 that a significant temperature change occurs during the cooling period, but the temperature data show a large degree of variability, which compromises the averaged brain temperature drop over all animals. So far, the detected cooling effect of −0.33°C is small but fast (within 5 minutes), which may be clinically relevant, if the initial cooling rate could be maintained for a longer period. However, the temperature drop, especially in the frontal part of the brain, is considerably strong in some animals. Although the accuracy of the MRI temperature measurements is hard to determine, several factors affect the phase mapping technique like subject movement. This may not completely explain the large variability seen. We suspect other factors that may have directly confounded the cooling effectiveness, such as the angle and connection of the nasally inserted tube or the core temperature before cooling. Controlling these factors in a future study may reduce the observed variance and produce more accurate and consistent measurements. Only then, the clinical relevance can be reasonably judged by the achievable cooling effect.
Four out of the five analyzed pigs suffered from an induced stroke by embolization of cerebral arteries obstructing the blood flow effectively as confirmed by angiographic perfusion measurements. Corresponding tissue damage was also clearly visible 6 hours after embolization in diffusion-weighed MRI in the afflicted pigs. Thus, brain cooling strategies that rely on unaffected blood flow, for example, injection of cold fluid or cool pads, are obstructed in case of stroke. In contrast to such cooling methods, intranasal cooling directly exposes the frontal brain to the cold and effectively cools by heat conduction and is, therefore, not affected by blood flow failure of obstruction. This is consistent with the temperature changes and maps we observed, where no influence or effect on the temperature distribution is apparent due to the induced stroke.
As in pigs, the nasal airways in humans are in close proximity to the frontal lobe. This suggests that the method could be transferable to humans. Being easy to use, fast acting, and minimally invasive, the method might have a future potential for use by first responders in an emergency. However, due to potential damage of the nasal mucosa by the high flow of dry air, further improvements of the air cooling device, that is, colder air at lower air flow, must be implemented and tested. For self-breathing conscious patients or volunteers, the current high flow of cold air could be safely administered via a face mask with enlarged exhale valves, allowing the cold air to easily escape, and instructing the subjects to take rapid and deep breaths in through the nose and out through the mouth.
Local cooling may also lower whole-body temperature as demonstrated in sheep with transnasal perfluorohexane evaporation (Wolfson et al., 2008) or a neck cooling collar (Giuliani et al., 2016). However, body temperature was only monitored and not recorded by the anesthesiologist in our study and no obvious drop in body temperature after the cooling in the MRI was noticed or mentioned. Further, no temperature monitoring was possible during the cooling experiment in the MRI, since only non-MRI safe temperature probes were available for our study.
Conclusion
We have demonstrated the feasibility of a novel high-flow cold air hypothermia protocol, showing a significant temperature drop during brain cooling in five pigs. The proposed protocol is easily implemented and delivers a quick local cooling effect to the frontal brain. This technique is of potential clinical relevance, since current prehospital cooling techniques, such as uncontrolled infusion of cold fluid, are compromised by harmful side effects. Further, a localized cooling effect may be preferable in traumatic injury of the frontal brain. However, more control of air flow and temperature is desirable for a future portable air cooling device, since a high variability of the cooling effect was observed. Further studies are also needed to more accurately determine the minimum temperatures reached during cooling and the long-term effects of the dry, cold air on the nasal mucosa.
Footnotes
Acknowledgments
The study was funded by the Federal Ministry of Education and Research (BMBF) Germany (grant number 031A530). Equipment was provided free of charge by MecoTec GmbH (Bitterfeld-Wolfen, Germany: CryoAir cold air therapy device) and by Dräger Medical GmbH (Luebeck, Germany: Fabius MRI Anaesthesia Machine).
Author Disclosure Statement
F.T. is the founder of a therapeutic hypothermia start-up company, Medical Cooling. All other authors declare they have no conflicts of interest.