
Abstract
Targeted temperature management (therapeutic hypothermia) is a treatment method used to prevent potential complications that can develop in relation to the increased temperature in the brain as a result of cardiac arrest. Due to costs and various health policies there is no comprehensive study in the world that has been able to guide the relevant literature on therapeutic hypothermia. We have presented a 25-year-old female patient in our study who developed cardiac arrest after the administration of propofol for sedation before undergoing a diagnostic upper gastroscopy procedure and received a successful therapeutic hypothermia therapy following a resuscitation of 19 minutes.
Introduction
According to data from the World Health Organization, the number of total deaths within 2014 is about 48.093 per 100.000 (total reporting countries) (WHO data, 2018). A remarkable amount of these mortality cases resulted from cardiac arrest. Cardiac arrest rates have been reported as being 50–100/100,000 across the world (Berdowski et al., 2010). In recent years, neurologic complications observed after cardiac arrest have decreased, and quality of life after discharge from hospital has increased due to many factors. These factors include increased number of people who have received emergency training, rapid access to coronary angiography, and the practice of therapeutic hypothermia. Hypothermia was advocated for by Peter Safar from the late ‘50s or early ‘60s.
Theoretically, the effects of therapeutic hypothermia include reduced cerebral metabolic need, decreased intracranial pressure, prevention of temperature-related biochemical processes, as well as extracerebral systemic results (hyperglycemia and infections, etc.) (Polderman et al., 2006). Cardiac arrest is one of the primary causes of coma and a frequent reason for admitting patients to the intensive care unit. In the case of a coma occurring after cardiac arrest, what is most difficult for the clinicians is meeting the high expectations of the patient's relatives.
Case Report
A 25-year-old female patient without any known chronic disease presented to the gastroenterology department with the complaint of epigastric pain, underwent upper gastroscopy after being sedated with propofol upon her own request, and cardiac arrest occurred during her follow-up at the reanimation room. Cardiopulmonary resuscitation (CPR) was started before the arrival of the anesthesia team. The Glasgow coma score (GCS) of the patient was three, and her pupils were fixed and dilated. A total of 2 mg of epinephrine and 3 mg of atropine were administered intravenously, spontaneous blood circulation was achieved, and she was intubated after 19 minutes of CPR. She was transferred to the intensive care unit and connected to the mechanical ventilator. At the time of admission, her pulse was 96 pulses/min (sinus rhythm), and her arterial blood pressure was 120/70 mmHg. The GCS and pupil response of the patient did not change. There was no anomaly in her chest X-ray. Arterial blood gas values at the admission were as follows: PO2 94.9 mmHg (normal 80–100), PCO2 52.8 mmHg (normal 32–48), and HCO3 9 mmol/L (normal 22–26) when 100% FiO2 was given, with a pH of 6.82 (reference interval 7.35–7.45). The settings of the mechanical ventilator were readjusted. Body temperature was 35.6°C at the time of admission. Other laboratory parameters are shown in Table 1. Upon the recommendation of the infectious diseases department, meropenem 1000 mg bid and clarithromycin 500 mg bid were started.
Laboratory Values of the Patient Before and After Therapeutic Hypothermia
There was no known history of chronic diseases, smoking, or alcohol. Conventional neuroprotective measures were applied to the patient who was admitted to the intensive care unit. Neuroprotective measures included midazolam (20 mcg/kg/min) and fentanyl (25–100 mcg/kg/h) infusion, elevation of the patient's head, and controlled mechanical ventilation to keep the arterial PCO2 value between 30 and 35 mmHg. To enable sufficient intravascular volume for the patient, tube feeding was started through a nasogastric tube to provide crystallized liquid and feeding. No hemorrhage or edema was seen in the brain tomography performed during admission (Fig. 1). Among the various therapeutic hypothermia treatment types, the use of surface cooler pads with water flow was decided upon (Holzer, 2010). External cooler pads were placed on the patient using targeted temperature management device, and the central temperature of the patient was decreased to 34°C. The body temperature of the patient was tracked with the probe placed in the esophagus. The central temperature was maintained at 34°C for 48 hours. During the 12-hour follow-up, the body temperature of the patient was gradually increased up to 36°C. As shivering did not occur during the process, no neuromuscular blocker was used. Arterial blood gas was tracked every 4 hours. The patient's hypnosedative drugs were discontinued once normal body temperature was achieved. The acidosis condition of the patient was recovered within 12 hours after admission. The pupil response of the patient became sensitive to light on hour 12, and pupils returned to their normal size and reaction on hour 52 after the recovery of normal body temperature. The GCS of the patient was 7 on day 9, but electroencephalography was applied by considering nonconvulsive status epilepticus, as the patient did not become totally conscious, and spontaneous eye movements could not be restored. Anticonvulsive therapy was not started upon the report that the background activity was slowing, and it was attributed to the prolonged effect of hypnosedatives. Diffusion magnetic resonance imaging (MRI) was performed on the patient, and hyperintense lesions were seen in the bilateral lentiform nucleus, thalamus, and right occipital on the axial T2 flair section (Fig. 2). A tracheostomy tube was inserted in the patient when she was unconscious with no swallowing reflex and followed-up with a mechanical ventilator when in a condition with stable airway dynamics. The mechanical ventilator was disconnected on day 11. Percutaneous endoscopic gastrostomy (PEG) was placed for feeding. On day 15 of follow-up, the patient who had stable vital findings, a GCS of 12, weak cooperation, and no swallowing reflex, was transferred to the rehabilitation unit. One hundred twelve days after the incident, the tracheostomy and PEG of the patient, who could perform all her daily activities without any problem and had no neurologic deficit, were removed, and she was discharged.
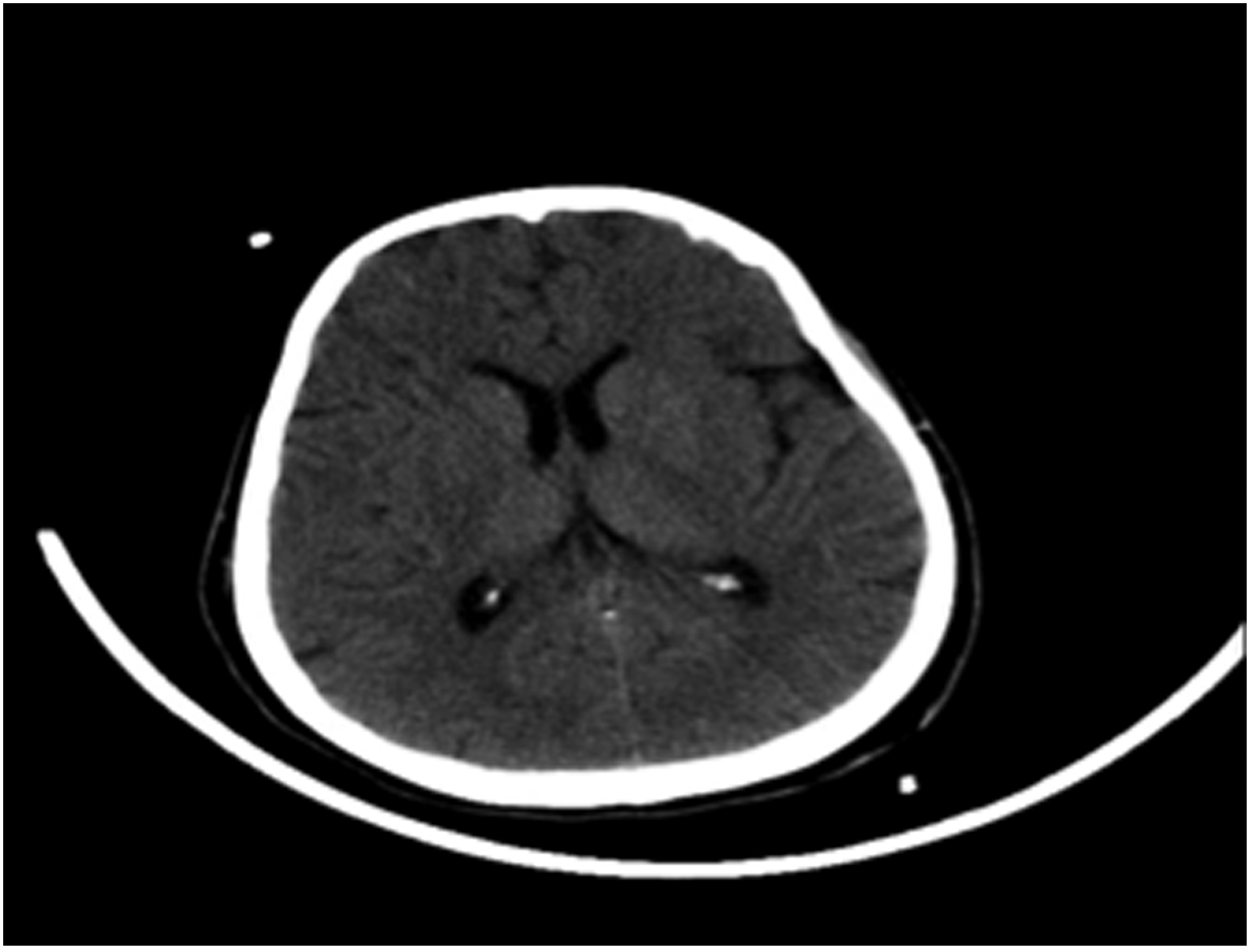
Cranial tomography section performed 30 minutes after the cardiac arrest.
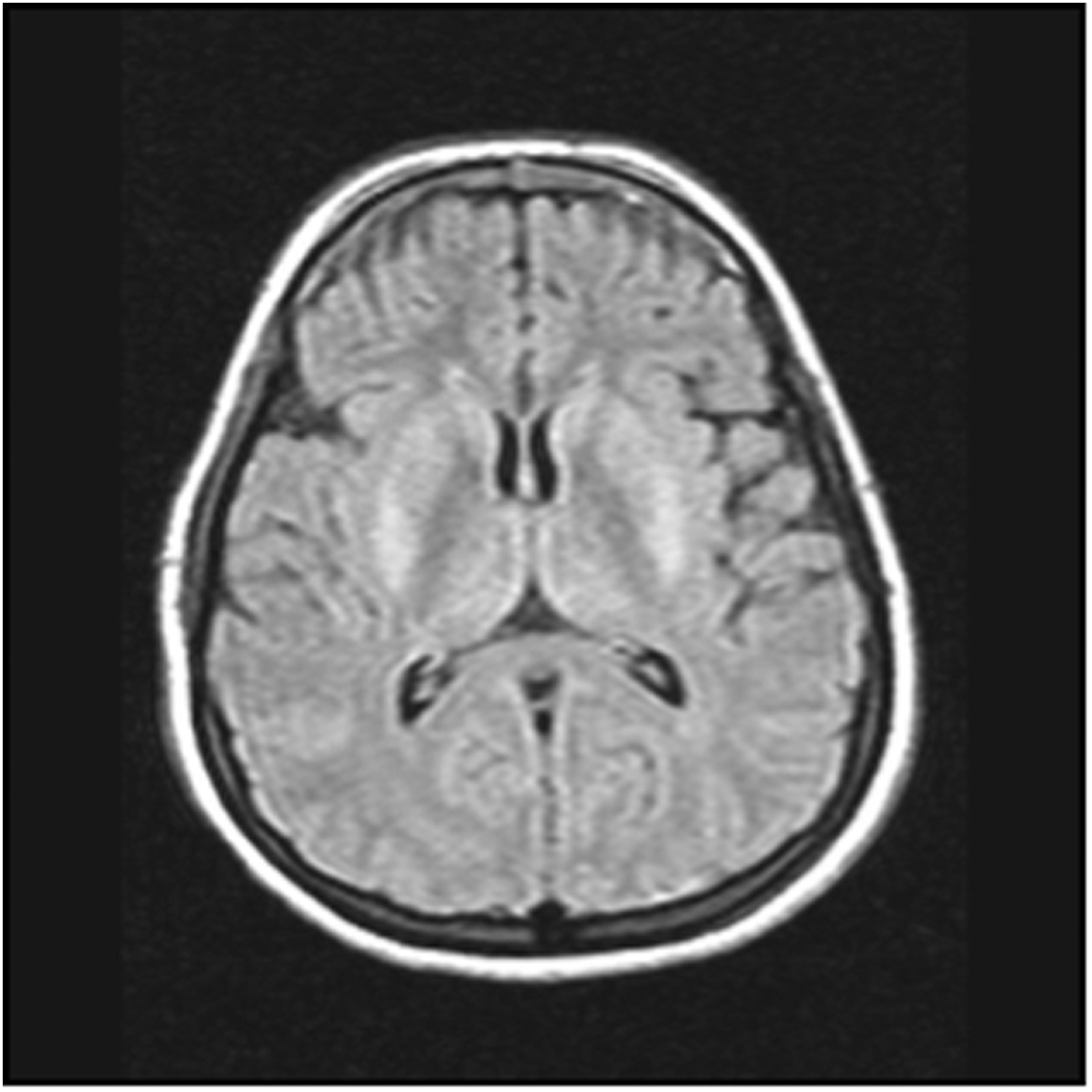
Hyperintense lesions in the bilateral lentiform nucleus, thalamus, and right occipital on the axial T2 flair section.
Discussion
Gastrointestinal diseases affect 60–70 million people a year in the United States. In 2004, 4.6 million patients were hospitalized, and about 236,000 patients died due to gastrointestinal diseases. Almost $142 billion is spent every year in the United States on gastrointestinal diseases (Everhart and Ruhl, 2009). Upper gastrointestinal endoscopy is increasingly applied in daily practice. Esophagitis, Barret esophagus, peptic ulcer, gastroduodenal lesions, and malignancies, which are the organic lesions of the upper gastrointestinal system, can be seen in endoscopy. Esophagogastroduodenoscopy (EGD) is a reliable practice, and procedure-related complications are rarely observed (ASGE Standards of Practice Committee et al., 2012). These complications might include cardiopulmonary conditions, aspiration of food and drinks to the lungs, reactions related to the sedatives used, venous irritation caused by the medication given intravenously, and hemorrhage and perforation at the polyp resection or biopsy site.
Sedation is used in most of the cases in order for the endoscopic intervention to be performed in a comfortable and reliable environment. Mild-to-moderate level of sedation is administered in a major part of EGD and colonoscopy cases. While benzodiazepine and opiate derivatives were commonly used in the past, the use of propofol, which is an intravenous general anesthetic, has increased in recent years. Deep sedation is preferred in endoscopic retrograde cholangiopancreatography or endoscopic ultrasonography cases where the procedure duration is longer and minimal patient mobilization is desired. In patients with hemodynamic instability and another underlying respiratory failure, general anesthetics must be used with care, and the vital findings of the patient must be tracked carefully in the reanimation room until the effect of sedation dissipates.
Propofol is a short-acting and lipophilic intravenous general anesthetic. It can lead to global central nervous system depression by means of an agonist effect on the gamma-aminobutyric acid (GABA) receptors and probably through the reduction in glutamatergic activity by N-methyl-D-aspartate (NMDA) receptor blockage. Propofol-induced central nervous system depression, apnea of 30–60 seconds, apnea of >60 seconds, bradycardia, cardiac arrhythmia, and low cardiac output are seen at a rate of 3–10%, 24%, 12%, 1–3%, 1–3%, and 1–3%, respectively, in adults (Uptodate, 2018).
Every year, cardiac arrest occurs in almost 375,000 people in the United States. About 300,000 of these cases occur outside the hospital. The main reasons associated with sudden cardiac arrest are coronary atherosclerosis, congenital anomalies of the coronary arteries, coronary artery embolism, and coronary artery vasculitis (Myerburg and Castellanos, 2015). If cardiac arrest occurs, advanced cardiac life support (ACLS) must be initiated immediately. Defibrillation must be applied for effective CPR and shockable cardiac arrhythmias as part of the ACLS. The concept of effective resuscitation must be considered important. The most significant problems encountered after performance of effective resuscitation and achievement of spontaneous blood circulation are a poor neurological picture and the associated deterioration in the prognosis and decrease in life quality and survival. Reduced cerebral and coronary perfusion may occur as a result of insufficient resuscitation, and the neurologic sequela risk of the patient may increase after the cardiac arrest. While the survival and discharge rate after nonhospital cardiac arrest is 5%, this figure can increase to 25–40% if the patient is under intensive care follow-up. The rate of recovery of survivors without neurologic sequela is as low as 10–20% (Polderman et al., 2008).
Even though the brain accounts for 2% of the body's weight, it uses 15% of the cardiac output and 20% of the oxygen in the body. The amount of oxygen consumed for each 100 g of brain tissue is 3.5 mL/min, and loss of consciousness and neuronal damage are observed when the oxygen supply falls below 2 mL/100 g/min. Anaerobic conditions become dominant in a short time after cardiac arrest, and the high metabolic needs of the brain cannot be met. Therefore, brain functions deteriorate rapidly after cardiac arrest, and consciousness is lost in a period as short as 15 seconds. Irreversible brain damage starts to develop 4–6 minutes after cardiac arrest, continues for 72 hours, and ends with apoptotic neuron death. The mechanisms of postresuscitation damage can be summarized under four main headings as follows: cerebral hypoperfusion, increased intraneuronal calcium, mitochondrial degradation, and blood stasis (Acikalin et al., 2011). In the first of these, ischemia, loss of integrity in the cell membrane, and necrosis develop in the tissue as a result of the failure to produce sufficient ATP after the cerebral hypoperfusion that is related with pump insufficiency at the moment of cardiac arrest. Permanent hypoperfusion may develop as a result of vasoconstriction, platelet aggregation, pericapillary edema, and abnormal calcium transport (Alzaga et al., 2006). Restoring blood flow in the brain after ischemia is called reperfusion and deepens the injury caused by ischemia, which is referred to as ischemia–reperfusion injury. As a result of this pathogenesis, in which interleukin, nitric acid, reactive oxygen derivatives, and proteases play a role, a breakdown in the blood–brain barrier is caused. Due to the increase in interleukin, mixed vasogenic and cytotoxic brain edema occurs with the contribution of the increase in vascular permeability. Reactive oxygen radicals created after reoxygenation trigger the lipid preoxidation and other oxidative damage processes. In the second of these, cellular depolarization is disrupted due to the Na-K pump insufficiency that develops as a result of membrane deformity. Neurotransmitters such as arachidonic acid and glutamate are released with the lipolysis that develops due to phospholipase activation and calcium increases in the neurons. Increased intracellular calcium triggers cellular damage by activating the intracellular proteases. The third of these is the Na-K-ATPase pump dysfunction that develops due to ATP production insufficiency as a result of mitochondrial degradation. Increase in intracellular sodium and water causes depolarization. The intraneuronal calcium that rises accordingly increases the cytoskeleton damage. The fourth of these is the blood stasis damage that occurs during cardiac arrest.
Cranial imaging helps to identify the structural changes in the brain and determines the amount of damage after anoxia. Even though its use has increased for coma prognosis in patients during the last few years, it is still used less than other prognostic methods. It provides important information on the exclusion of intracranial hemorrhage in cardiac arrest cases with unknown origin. While the intracerebral causes of the cardiac arrest are rarely seen, it would be useful to carry out a routine brain computerized tomography (CT) at the time of patient admission so as not to delay postresuscitation care and therapeutic hypothermia. Findings supporting hypoxia in cranial tomography are the reduction in the white-gray matter separation and sulcal edema. Reduction in the white-gray matter separation 2 hours after the cardiac arrest is associated with poor prognosis (Inamasu et al., 2011). As brain MRI has a higher resolution than tomography, it enables easier identification of the structural anomalies in the cortex, deep gray nuclei, and hippocampus. Even though the superiority of MRI over CT in terms of result prediction has not been shown in any clinical study, clinicians focus on the use of MRI (especially diffusion-weighted MRI). In patients with poor prognosis, a limited diffusion might be seen that gives rise to the consideration of cytotoxic edema in the occipital and middle temporal region, as well as the putamen (Mlynash et al., 2010). Given the levels of evidence, the structural findings of postanoxic damage observed with brain CT or MRI provide a weaker prediction in terms of prognosis compared to brain stem reflexes and electrophysiologic findings. In practice, several centers carry out a brain CT scan to investigate the cerebral cause for cardiac arrest with unknown origin. In patients who cannot recover from coma, even though they do not have prognostic symptoms with regards to poor results according to the clinical, electrophysiologic, and blood tests, a brain MRI scan is performed for the completion of multimodal evaluation.
Postcardiac arrest management consists of basic and advanced life support, as well as long-term care. Treatment of the patient after cardiac arrest is complex, requiring more than one simultaneous intervention. Postcardiac arrest approach involves identification of the cause and treatment of cardiac arrest, minimalization of the brain damage, management of the cardiovascular dysfunction, and management of problems that might develop due to global ischemia and reperfusion damage. The short-term objectives are identification of the cause and treatment of cardiac arrest once cardiovascular collapse, oxygenation, and electrolyte imbalance are recovered. The long-term objective is the prevention of the development of postcardiac syndrome that might develop due to ischemia and reperfusion damage (Nolan et al., 2008). The most significant manifestations of postcardiac arrest syndrome are neurologic. About 80% of cases stay in a coma for more than 1 hour after a cardiac arrest, and neurologic recovery is seen in less than half of the patients who are admitted to intensive care (Jennett and Bond, 1975). While coma or a persistent vegetative condition might develop in cases that are affected more by hypoxia, cognitive function and other neurologic deficits might be seen in some cases at varying levels. Even when the coronary angiography procedure is being performed, therapeutic hypothermia can be used by means of surface cooling (ice packs, cooling pads, etc.), intravenous saline administration, or intravascular cooling methods to minimize the neurologic damage (Forkmann et al., 2015). In the reported case series, good results were obtained from patients in cardiogenic shock (Skulec et al., 2008).
Hyperthermia development starts within 48 hours after cardiac arrest. Failure in the management of high body temperature is associated with negative neurologic results. In an observational study, including 151 patients, it was determined that mortality risk increased at each degree increasing above 37°C within the first 48 hours after cardiac arrest (Zeiner et al., 2001). While high temperature seen in the early stage is associated with poor clinical results, it was found that late-onset fever did not show the same destructive effects (Gebhardt et al., 2013). As the cellular metabolic processes and ATP consumption increase as a result of each degree of increase in body temperature, oxygen consumption of the brain also increases at a rate of 8% (Smith and Bleck, 2002).
However, cerebral oxygen consumption decreases at a rate of 6–7% due to each degree of body temperature decreased by means of hypothermia. Hypothermia prevents membrane damage and electrolyte imbalance by blocking the generation of oxygen radicals during the postcardiac arrest reperfusion period. Besides this, it has been shown in studies that hypothermia has effects, such as protection of the high energy phosphate stores, reduction of the cerebral metabolism, and reduction in the lactate and glutamate concentration. The suppression of the generation of oxygen radicals decreases the severity of apoptosis in cells and suppresses the inflammatory mechanisms (Al Saneni and Grotta, 2002; Alzaga et al., 2006).
In the guidelines published in 2005, the American Heart Association (AHA) recommended that, in out-of-hospital cardiac arrest cases, if the patient's cardiac rhythm is ventricular fibrillation or ventricular tachycardia at the site of the incident, and he/she returns to spontaneous circulation after resuscitation is performed, the patient should be cooled down to a body temperature of 32–34°C and kept at that temperature for 12–24 hours (AHA guidelines, 2005). In the AHA guidelines published in 2010, the recommendation was updated so that the body temperature of comatose patients (failure to give meaningful responses to verbal commands, etc.) who developed spontaneous circulation after cardiac arrest related to ventricular fibrillation occurring outside the hospital should be cooled to 32–34°C for 12–24 hours. However, the latest guidelines of the AHA published in 2015 updated the recommendations on therapeutic hyperthermia once more. The latest suggestion is to achieve a targeted body temperature of 32–36°C and maintain such temperature for at least 24 hours in all comatose patients who have spontaneous blood circulation after cardiac arrest. In the first scientific publications performed on therapeutic hypothermia, the body temperature of the patient was recommended to be kept under 30°C, but this is not advised today as reduction of the central temperature under this degree causes certain coagulation disorders. In several studies, it is recommended that therapeutic hypothermia be started as soon as possible in postcardiac arrest patients and that patients must be protected against fever for at least 48 hours (Zeiner et al., 2001; Bernard et al., 2002; Kirkegaard et al., 2002; Gebhardt et al., 2013; Nielsen et al., 2013).
Another important problem that delays achievement of the targeted body temperature is shivering. Shivering increases the body's temperature and must be suppressed (Kim et al., 2007; Badjatia et al., 2008; Hostler et al., 2009). Therefore, fentanyl, dexmedetomidine, midazolam, meperidine, and propofol are used in patients receiving therapeutic hypothermia. But use of propofol may be controversial because of its observed harmful effects on injured neurons in multiple animal studies, as well as increased myocardial injury in patients undergoing coronary artery bypass grafting. In hypotensive patients, continuous midazolam infusion is preferred as an alternative to propofol. Neuromuscular blockers that are effective in shivering treatment can mask a patient's potential seizures. If they are to be used, follow-up must be performed with electroencephalogram continuously (Abend et al., 2009). During the therapeutic hypothermia procedure, the core body temperature of the patient must be measured continuously. While the golden standard method for this is the central venous measurement, measurement with esophagus, bladder, and rectal probes is also possible. Esophageal temperature measurement is the most accurate measurement method for tracking body temperature during the application of therapeutic hypothermia (Erickson et al., 1993).
Once the targeted time is completed at the targeted temperature, rewarming of the patient must be applied gradually, and body temperature must not be increased by more than 0.5°C per hour. In some studies, body temperature increase is recommended to be between 0.2°C and 0.25°C per hour (Badjatia et al., 2008). Rewarming can cause cerebral edema, electrolyte disorders, and convulsions in patients. In studies on animals where traumatic brain damage was created, it was determined that rapid warming limited the positive effects of therapeutic hypothermia (Suehiro et al., 2001).
Conclusion
The positive effect that therapeutic hypothermia has on the neurologic results of a patient was emphasized in this case on which therapeutic hypothermia was applied at the early stage following cardiac arrest. Given the postcardiac arrest care of patient, duration of stay at the hospital, health costs, and negative neurologic results, this treatment, whose ease-of-application and relationship with positive neurologic results have been shown in studies, should be applied in all successful post-CPR cases, regardless of the reason of cardiac arrest, provided that there is no contraindication.
Footnotes
Author Disclosure Statement
No competing financial interests exist.