
Abstract
This study aimed to identify factors associated with the decision to transfer resuscitated patients with out-of-hospital cardiac arrest (OHCA) who were initially examined at hospitals with limited targeted temperature management capability (HLTC) in Korea. We included adult patients with OHCA who were initially transported to HLTC from 2012 to 2015. We limited the study population with OHCA who were admitted or transferred. Potential factors associated with the transfer decision were categorized as patient- or hospital-level characteristics. The primary outcome was emergency department disposition: transfer out versus admission to HLTC. A stepwise multivariable logistic regression analysis was conducted to identify factors associated with the outcome. Of the 64,696 patients with OHCA, 37,705 (58.3%) were initially transported to HLTC. Approximately 44.7% of patients were transferred out. In terms of patient-level factors, age, socioeconomic status, and initial electrocardiogram rhythm were associated with the transfer decision. Hospital factors, such as percutaneous coronary intervention capability of HLTC (adjusted odds ratio = 0.16; 95% confidence interval = 0.14–0.19) and location of the metropolitan or urban hospital, were negatively associated with the transfer decision. Several hospital and patient factors were associated with the decision to transfer out patients with OHCA who were initially examined at HLTC.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a major public health burden worldwide. The annual incidence rates of OHCA per 100,000 persons were 54.6 in North America, 35.0 in Europe, 28.3 in Asia, and 44.0 in Australia (Berdowski et al., 2010). Although the survival rate of patients with OHCA has improved by ∼10% over several decades due to various pre- and in-hospital efforts, the survival rate has shown a wide regional variability (Chan et al., 2014).
Evidence has shown that targeted temperature management (TTM) and other types of postresuscitation care improve the outcomes of patients with OHCA (Kronick et al., 2015). A substantial variation is observed in the practice of emergency department (ED) postresuscitation and application of TTM across the regions or nations. In some European countries, only 30–50% of intensive care units (ICUs) have utilized TTM in patients with OHCA (Gasparetto et al., 2014; Kołtowski et al., 2017). In the United States, only 6% of ICUs provide TTM to more than half of resuscitated patients with OHCA (Edelson et al., 2014). According to the national sample data in the United States, TTM may be utilized in <1% of patients with cardiac arrest (Patel et al., 2011). In Korea, only 8.3% of patients who survived during admission received TTM (Kim et al., 2013). The International Liaison Committee on Resuscitation and Korean guidelines for postresuscitation care recommend that TTM is indicated for comatose patients regardless of the initial electrocardiogram (ECG) rhythm (Nolan et al., 2015; Kim et al., 2016).
Recently, several reports have shown that the number of patients receiving TTM has increased owing to the successful establishment of inter-hospital transfer (IHT) networks in mature regionalized care systems (Kajino et al., 2010; Mooney et al., 2011). Regional systems that facilitate IHT are available. However, little is known about the patients who are transferred for TTM and those who are not. Although several studies have reported the factors associated with the decision to transfer patients with critical diseases, such as acute myocardial infarction or severe trauma, in the developed regionalized system, only few studies have focused on OHCA (Sampalis et al., 1999; Henry et al., 2007; Delgado et al., 2014). Moreover, the difference in factors that affect the decision to transfer in a nonregionalized setting has not been evaluated thoroughly.
This study aimed to evaluate the factors associated with the transfer decision in successfully resuscitated patients with OHCA presenting to a hospital with limited TTM capability (HLTC) in Korea.
Methods
Study setting
The Korean emergency medical service (EMS) is a single-tier system operated by fire departments. According to the prehospital transport protocol, patients with OHCA should be transported to the nearest ED regardless of achieving return of spontaneous circulation (ROSC) at the scene. However, regional cardiac resuscitation centers are not available in Korea.
Study design and participants
This was a cross-sectional observational study that used data from a Korean national EMS-assessed OHCA registry. The cases and prehospital information obtained from the electronic EMS run sheets and medical records of each destination hospital were assessed by trained reviewers using an Utstein template (Perkins et al., 2015). Detailed information and data quality management processes for the Korean national EMS-assessed OHCA registry program have been described previously (Ahn et al., 2010).
We included adult EMS-treated patients with OHCA with a presumed cardiac etiology who were initially transported to HLTC from January 2012 to December 2015. The study population was limited to patients admitted or transferred after ROSC to HLTC to evaluate the factors associated with the transfer decision. Since the Korean guidelines for cardiopulmonary resuscitation (CPR) recommend maintaining TTM for at least 24 hours after achieving the target temperature, TTM capability was then defined as the ability to achieve and maintain a specific target body temperature for at least 24 hours (Kim et al., 2016). HLTC was classified as hospitals that did not report any cases meeting the abovementioned definition of TTM during the study period based on clinical data. We excluded patients who were transported to hospitals where all patients with OHCA were hospitalized or transferred out during the study period because the disposition of patients in these hospitals depended on institutional policy. To limit the participants to presumed candidates for TTM, we excluded patients whose time from collapse to ROSC was longer than 60 minutes. The study was approved by the Institutional Review Board of Seoul National University Hospital, and the need for informed consent was waived off (IRB number H-1401-090-550).
Outcomes and variables
The primary outcome of this study was ED disposition: transfer out versus admission to HLTC. Information about the demographic factors of patients and individual socioeconomic status (SES) was collected. The type of medical insurance was identified as a proxy measure of individual SES (nonmedical aid vs. medical aid). Data about the factors associated with OHCA, such as witnessed cardiac arrest, bystander CPR, and initial ECG rhythm (shockable vs. nonshockable), were collected. Moreover, information regarding the percutaneous coronary intervention (PCI) capability of hospitals to which patients with OHCA were initially transported, community urbanization (rural, urban, or metropolitan), and day of the week (weekday vs. weekend) were collected and considered as hospital factors. PCI capability was defined as performing PCI for patients with OHCA before discharge regardless of timing.
Statistical analysis
Demographic findings based on disposition from HLTC were described. Categorical variables were reported as counts and percentages and compared with cross-tabulation analysis using the chi-square method. Two-sided tests were conducted, and a p-value <0.05 was considered statistically significant. To explore the association between patient or hospital factors and ED disposition, a backward stepwise multivariable logistic regression analysis was performed. We consecutively added all possible explanatory variables and then removed insignificant variables. A significance level of 0.2 is required to allow a variable to remain in the model. The adjusted odds ratios (AOR) were calculated (95% confidence interval [CI]). Moreover, we conducted a subgroup analysis on patients with OHCA who were initially transported to HLTC that did not have a capability to perform PCI.
Results
Of the 64,696 EMS-treated adult patients with OHCA with a presumed cardiac origin, 37,705 (58.3%) were initially transported to HLTC. In total, 5453 (14.5%) patients were admitted or transferred after ROSC. After excluding patients who were transported to hospitals that had a mandatory institutional disposition policy for resuscitated patients with OHCA, those who were transferred out during CPR, and those who were not eligible for TTM, 4167 (76.4%) were finally included in the analysis (Fig. 1).
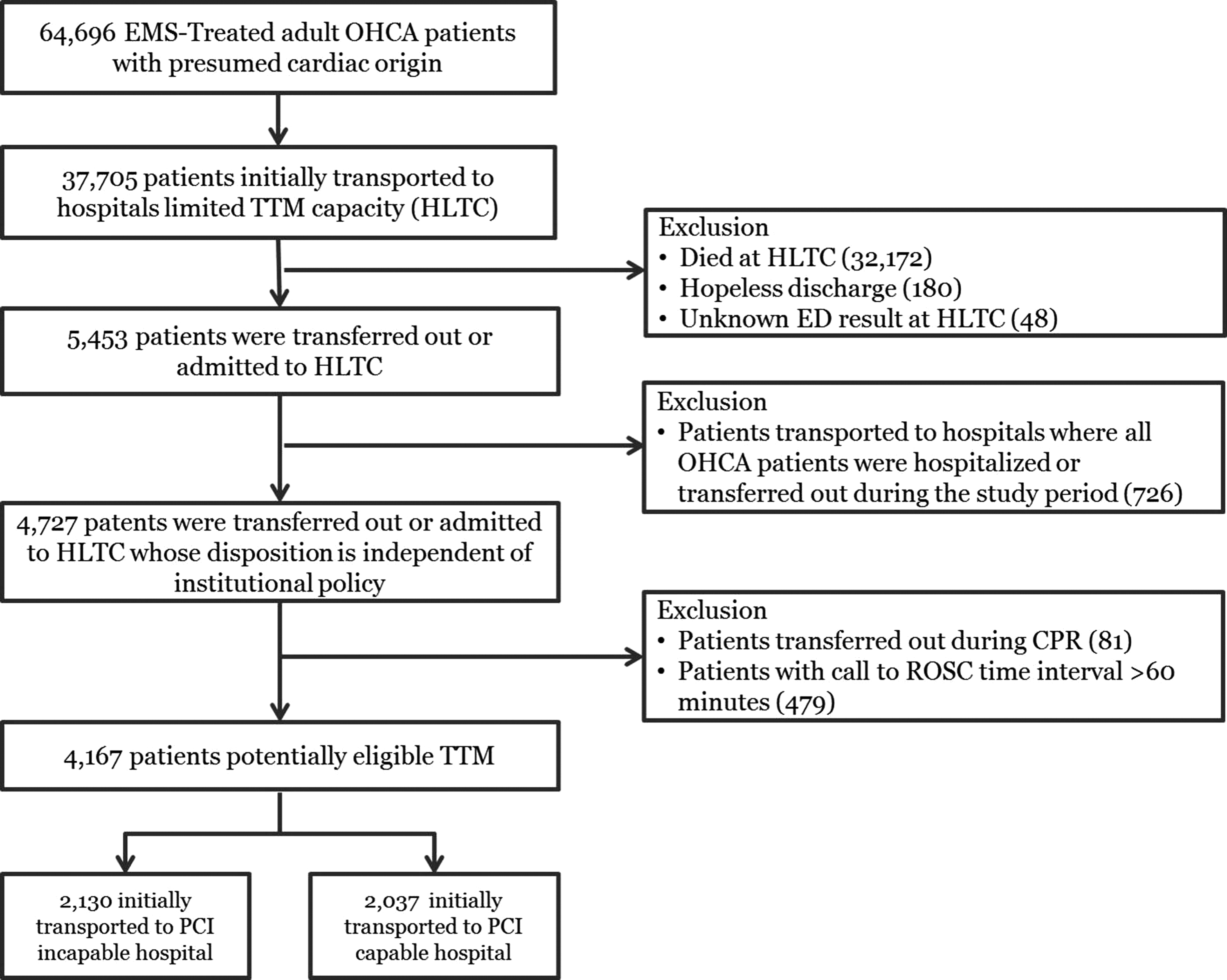
Flowchart of patient inclusion and exclusion for analysis. EMS, emergency medical services; OHCA, out-of-hospital cardiac arrest; TTM, targeted temperature management; CPR, cardiopulmonary resuscitation; ROSC, return of spontaneous circulation.
Table 1 shows the demographic characteristics of patients based on ED disposition. The admission group had a higher proportion of female and old age participants as well as patients with low SES. In the transfer out group, a higher proportion of patients presented with an initial shockable rhythm and achieved prehospital ROSC. In terms of hospital factors, a lower proportion of transfer out patients was initially transported to HLTC that are capable of PCI and located in metropolitan areas.
Demographic Findings of Study Population by Emergency Department Disposition
CPR, cardiopulmonary resuscitation; ROSC, return of spontaneous circulation; PCI, percutaneous coronary intervention; RTI, response time interval.
After adjusting for potential confounders, the PCI capability of HLTC (AOR = 0.16; 95% CI = 0.14–0.19) was most negatively associated with the transfer decision (Table 2). In terms of patient-level factors, younger patients, those with high SES, and those with an initial shockable ECG rhythm had a lower risk of admission to HLTC.
Multivariable Analysis for Factors Associated with Emergency Department Disposition
OR, odds ratio; CI, confidence intervals.
The subgroup analysis showed similar results. We included 2130 patients who were transported to HLTC without PCI capability in the subgroup analysis. Moreover, ∼64.4% of patients were transferred out from HLTC. Table 3 shows the demographic characteristics of patients in the subgroup according to ED disposition. The admission group had a higher proportion of female and old age participants as well as patients with low SES. The transfer out group had a higher proportion of patients who presented with an initial shockable rhythm and who achieved prehospital ROSC. In terms of hospital factors, a lower proportion of patients were transferred out from HLTC that were located in metropolitan areas. Independent associations were observed between the transfer decision and patents' age, SES, initial rhythm, and urbanization level of hospital location.
Demographic Findings of Patients Initially Transported to Percutaneous Coronary Intervention-Incapable Hospital
Discussion
Based on the rigorous analysis of patient- and hospital-level characteristics, this study suggests that several factors are associated with the decision to transfer a patient from HLTC in Korea.
Most previous studies have defined TTM capability based on the results of a survey on the adoption of TTM in ICUs rather than actual clinical data (Edelson et al., 2014; Kołtowski et al., 2017). In this study, we defined TTM capability as the ability to achieve and maintain target temperature for at least 24 hours instead of just initiating TTM with a comprehensive literature review and author discussion. Some patients may have received TTM at an HLTC but were then transferred before 24 hours post initiation. The evaluation of TTM capability using real-world data is more reliable than the assessment of self-reported TTM capability. We measured the duration of TTM application by calculating the time interval between the timing of achieving target temperature and discontinuing TTM or transfer out from the ED before 24 hours. In this study, consensus on the definition of the TTM capability of hospitals was achieved with a comprehensive literature review and author discussion. The methods of TTM range from the conventional, such as cold saline infusion, to external or internal cooling using expensive commercial devices. The application of TTM using conventional methods may not be difficult to initiate. We defined TTM capability as the ability to achieve and maintain target body temperature for at least 24 hours instead of just initiating TTM.
When a physician decides to transfer resuscitated patients with OHCA, they must consider multifaceted factors. The medical staff should assess the risks and benefits of transfer before they decide to transfer a patient. If the medical staff decides not to transfer, the patient may eventually lose the opportunity to receive TTM. When the medical staff decides to transfer, risks, such as hypoxia or hypotension, that can occur during IHT must be considered. In a previous paramedic system report, 6% of patients experienced re-arrest, and 23% of patients with OHCA presented with critical events during IHT (Hartke et al., 2010). In another previous study, due to potential hypoxic or hypotensive insults during IHT, the effects of TTM on neurological recovery were modified in patients who experienced IHT (Park et al., 2016). The mobile ICU has not been adopted to improve the safety of patients during IHT in Korea in the study period. With regard to patient-level factors, young age, higher SES, or initial shockable ECG rhythm were significantly associated with transfer. In this study, it was not surprising that patients with OHCA who have a higher probability of survival were more likely to be transferred to other hospitals. In these patients, the benefit of neurological recovery due to TTM can attenuate the risks, such as hypotension or hypoxia, during transportation. One of the notable patient factors in this study was low SES, and a significantly higher proportion of admission in HLTC rather than transfer to a potentially higher-level hospital was observed. We used the type of medical insurance as an alternative measure of individual SES. The medical aid program is a public medical assistance program targeting low-income individuals (Kim et al., 2015). However, some medical services, including the use of some commercial devices needed for TTM, are not reimbursed under the medical aid program. In a previous study examining the transfer of patients with severe trauma in the United States, insured patients compared with uninsured patients had a higher likelihood of admission to a nontrauma center rather than transfer to a trauma center (Delgado et al., 2014). Uninsured patients in the United States have less reimbursement potential. SES showed a different direction in terms of its associations with the transfer decision according to the reimbursement range of a medical insurance system. Resolving economic barriers to establish a regionalized system for medical care is challenging (Kocher et al., 2010).
The urbanization level of HLTC location is a notable hospital factor associated with the transfer decision. These results were consistent with those of the subgroup analysis limited to participants initially examined at hospitals with low capability for PCI (Table 4). One possible explanation was overcrowding in metropolitan or urban areas in Korea (Cha et al., 2016). Regionalization, including designated hospitals for the postresuscitation care of patients with OHCA in urban and metropolitan areas, must be urgently carried out.
Multivariable Analysis for Factors Associated with Emergency Department Disposition of Patients Initially Transported to Percutaneous Coronary Intervention-Incapable Hospital
OR, odds ratio.
Limitations
The results of this study must be cautiously interpreted. We did not include clinical and physiological characteristics, such as mental status and hemodynamic instabilities, that were measured in postresuscitation states; some of the variations in transfer rates may be explained by unobserved differences in these variables. In addition, no information about the outcomes of patients who were transferred out is available. A previous study has reported that transferred patients with OHCA had better survival and neurologic recovery (Park et al., 2016). Moreover, survival bias should be considered. Admitted or transferred patients were more likely to be younger and have witnessed a cardiac arrest or initial shockable rhythm than those who were not resuscitated (Appendix Table A1).
Conclusions
We identified several patient and hospital factors associated with the transfer decision in resuscitated patients with OHCA who were initially examined at HLTC.
Footnotes
Acknowledgments
This study was financially supported by the Korea Centers for Disease Control and Prevention (funding code 2012-E33010-00).
Author Disclosure Statement
No competing financial interests exist.
Appendix
Demographic Findings of Patients Initially Transported to Hospitals with Limited Targeted Temperature Management Capability by Emergency Department Result
| Total | ED survival | ED death | p | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Total | 29,636 | 100.0 | 4646 | 100.0 | 24,990 | 100.0 | |
| Gender | <0.001 | ||||||
| Male | 18,611 | 62.8 | 3165 | 68.1 | 15,446 | 61.8 | |
| Female | 11,025 | 37.2 | 1481 | 31.9 | 9544 | 38.2 | |
| Age | <0.001 | ||||||
| 18–64 | 9970 | 33.6 | 2320 | 49.9 | 7650 | 30.6 | |
| >65 | 19,666 | 66.4 | 2326 | 50.1 | 17340 | 69.4 | |
| Insurance | 0.87 | ||||||
| Medical aid | 2737 | 9.2 | 426 | 9.2 | 2311 | 9.2 | |
| Nonmedical aid | 26,899 | 90.8 | 4220 | 90.8 | 22,679 | 90.8 | |
| Witnessed status | <0.001 | ||||||
| Yes | 13,141 | 44.3 | 2944 | 63.4 | 10,197 | 40.8 | |
| Bystander CPR | <0.001 | ||||||
| Yes | 13,182 | 44.5 | 1781 | 38.3 | 11,401 | 45.6 | |
| Initial rhythm | <0.001 | ||||||
| Nonshockable | 25,293 | 85.3 | 3042 | 65.5 | 22,251 | 89.0 | |
| Shockable | 4343 | 14.7 | 1604 | 34.5 | 2739 | 11.0 | |
| Prehospital ROSC | <0.001 | ||||||
| Yes | 1321 | 4.5 | 1107 | 23.8 | 214 | 0.9 | |
| RTI | <0.001 | ||||||
| 0 ≤ RTI <4 | 4739 | 16.0 | 1011 | 21.8 | 3728 | 14.9 | |
| 4 ≤ RTI <8 | 14,417 | 48.6 | 2433 | 52.4 | 11,984 | 48.0 | |
| 8 ≤ RTI <12 | 8608 | 29.0 | 1072 | 23.1 | 7536 | 30.2 | |
| 12 ≤ RTI <16 | 1872 | 6.3 | 130 | 2.8 | 1742 | 7.0 | |
| Urbanization | <0.001 | ||||||
| Metropolitan | 13,832 | 46.7 | 2507 | 54.0 | 11,325 | 45.3 | |
| Urban | 11,058 | 37.3 | 1663 | 35.8 | 9395 | 37.6 | |
| Rural | 4746 | 16.0 | 476 | 10.2 | 4270 | 17.1 | |
| Weekend | 0.91 | ||||||
| Yes | 8617 | 29.1 | 1354 | 29.1 | 7263 | 29.1 | |
| PCI capability | <0.001 | ||||||
| Yes | 11,241 | 37.9 | 2264 | 48.7 | 8977 | 35.9 | |
RTI, response time interval; ROSC, return of spontaneous circulation; CPR, cardiopulmonary resuscitation; PCI, percutaneous coronary intervention; ED, emergency department.