
Abstract
To date, the optimal cooling device for targeted temperature management (TTM) remains unclear. Water-circulating cooling blankets are broadly available and quickly applied but reveal inaccuracy during maintenance and rewarming period. Recently, esophageal heat exchangers (EHEs) have been shown to be easily inserted, revealed effective cooling rates (0.26–1.12°C/h), acceptable deviations from target core temperature (<0.5°C), and rewarming rates between 0.2 and 0.4°C/h. The aim of this study was to compare cooling rates, accuracy during maintenance, and rewarming period as well as side effects of EHEs with water-circulating cooling blankets in a porcine TTM model. Mean core temperature of domestic pigs (n = 16) weighing 83.2 ± 3.6 kg was decreased to a target core temperature of 33°C by either using EHEs or water-circulating cooling blankets. After 8 hours of maintenance, rewarming was started at a goal rate of 0.25°C/h. Mean cooling rates were 1.3 ± 0.1°C/h (EHE) and 3.2 ± 0.5°C/h (blanket, p < 0.0002). Mean difference to target core temperature during maintenance ranged between ±1°C. Mean rewarming rates were 0.21 ± 0.01°C/h (EHE) and 0.22 ± 0.02°C/h (blanket, n.s.). There were no differences with regard to side effects such as brady- or tachycardia, hypo- or hyperkalemia, hypo- or hyperglycemia, hypotension, shivering, or esophageal tissue damage. Target temperature can be achieved faster by water-circulating cooling blankets. EHEs and water-circulating cooling blankets were demonstrated to be reliable and safe cooling devices in a prolonged porcine TTM model with more variability in EHE group.
Introduction
Sudden cardiac arrest remains the third leading cause of death in Europe and the industrialized nations (Böttiger et al., 2017). Known as targeted temperature management (TTM), decrease of the body's core temperature to 32–36°C for at least 24 hours after successful cardiopulmonary resuscitation is an established standard in critical care therapy. In fact, the metabolic rate of oxygen declines 7–10% per degree Celsius drop in temperature. Consequently, reactions associated with reperfusion injury will be suppressed and both neurologic outcome and survival can be improved (Polderman and Herold, 2009; Arrich et al., 2016).
To date, the optimal cooling device for TTM remains unclear. External cooling devices such as water-circulating cooling blankets are broadly available and quickly applied. However, faster cooling rates and higher accuracy of maintenance temperature and rewarming rate can be achieved by use of intravascular cooling devices (IVDs) directly approaching the body's core blood. However, IVDs require expertise and are associated with major side effects including, for example, blood-stream infections and venous thromboembolism (Hoedemaekers et al., 2007; Sonder et al., 2018; Wang et al., 2018).
At present, esophageal heat exchangers (EHEs) are of scientific interest. Adjacent to the aorta, vena cava, and heart, the esophagus is an ideal place to exchange thermal energy to the body's core. EHEs have been shown to be easily inserted and do not damage esophageal tissue (Kulstad et al., 2013; Schroeder et al., 2017). Clinical trials demonstrated effective cooling rates (0.26–1.12°C/h), deviations <0.5°C from target core temperature (Kulstad et al., 2013; Markota et al., 2016; Schroeder et al., 2017, 2018), and rewarming rates between 0.2°C/h and 0.4°C/h (Kulstad et al., 2013; Goury et al., 2017). To set the performance of EHEs in the context of commonly used cooling methods, the aim of this study was to compare EHEs with water-circulating cooling blankets in a porcine TTM model. The main study endpoints were cooling rates to a target core temperature of 33°C, deviations from target core temperatures during the 8-hour maintenance period, and compliance to intended rewarming rates of 0.25°C/h. Esophageal tissue damage or other potential side effects were also examined in this prolonged experimental TTM protocol.
Materials and Methods
Animal experiments
The study was permitted by the local animal care committee and governmental authorities (Landesamt für Natur-, Umwelt- und Verbraucherschutz NRW; 84-02.04.2014.A157). The measures were in accordance with the German Federal Laws for Animal Protection and supervised by a veterinarian. The involved employees were qualified to guarantee adequate animal care and use. The study protocol and the present article comply with the Animals in Research: Reporting of In Vivo Experiments guidelines (Kilkenny et al., 2010).
Sixteen healthy, domestic adult pigs (Landrace × Pietrain) weighing 83.2 ± 3.6 kg were used in this study. At least 10 days before conducting the experiments, animals were delivered to the facility, where they were kept in groups. Ambient temperatures were set to 20°C on a 12/12-hour light/dark cycle, and straw-bedded pens (9.3 m2) were provided. Animals had ad libitum access to water and were fed twice a day with adequate nutrition.
Perioperative management and anesthesia
The night before the experiment, animals were fasted and isolated but maintained visual contact to the remaining group. After premedication with an intramuscular (i.m.) injection of azaperone (2 mg/kg; Stresnil; Janssen, Neuss, Germany), ketamine (20 mg/kg; Ketavet 100; Pfizer, Berlin, Germany), and atropine (0.02 mg/kg; Braun, Melsungen, Germany), pigs were taken to the surgery room and received an intravenous (i.v.) catheter (Vasovet; Braun) in the lateral auricular vein. Animals were preoxygenated with 100% oxygen using a facial mask. Placed in a supine position, anesthesia was induced with propofol (2 mg/kg; Fresenius Kabi, Bad Homburg, Germany), and a 6.0 mm endotracheal tube (Teleflex Medical, Kernen, Germany) was inserted in the trachea by use of a 27 cm laryngoscope (Karl Storz, Tuttlingen, Germany). Pigs were ventilated with a tidal volume of 6 mL/kg at 14 breaths/min (Fabius GS; Dräger, Lübeck, Germany) using a pressure-controlled mode (30% oxygen). To maintain normocapnia (partial pressure of carbon dioxide, 40 ± 5 mmHg), ventilation was adapted over time. After induction of anesthesia, animals received enrofloxacin (2.5 mg/kg i.m.; Baytril; Bayer, Leverkusen, Germany).
A standard lead II electrocardiogram was applied to monitor cardiac rhythm (Philips Medizinsysteme, Böblingen, Germany). To maintain anesthesia, propofol [5–7 mg/(kg·h)], midazolam [1.2 mg/(kg·h); Rotexmedica, Trittau, Germany], and fentanyl [12–15 μg/(kg·h); Fentanyl; Rotexmedica] were continuously applied. Lactated Ringer's solution (Fresenius Kabi) at a rate of 5–10 mL/(kg·h) served as carrier and covered basic fluid requirement (Pehböck et al., 2015). In case of indications of reduced depth of anesthesia (hypertension, increased interdigital reflex, spontaneous breathing, and tachycardia), an additional bolus of propofol (0.5–1 mg/kg), midazolam (0.02–0.03 mg/kg), or fentanyl (1.0–1.25 μg/kg) was administered. In case of shivering, a bolus of rocuronium (0.5 mg/kg) was intended to be administered by the study protocol. Glucose (250 mL Glucosteril 5%; Fresenius Kabi) was applied if arterial blood glucose levels dropped below 3.5 mmol/L. Norepinephrine [0.1 μg/(kg·min) i.v.; Arterenol; Sanofi-Aventis, Frankfurt am Main, Germany] was administered if mean arterial blood pressure decreased to <50 mmHg.
Surgical preparations
During surgical preparation, animals were warmed using air-circulating blankets (Bairhugger; 3M Deutschland GmbH, Neuss, Germany) to maintain a physiological core temperature (38.5–39.5°C). The femoral artery was surgically exposed and a 6 F saline filled catheter (Arterial Leadercath; Vygon, Ecouen, France) was advanced for continuous blood pressure measurement (Philips M1097A; Philips Medizinsysteme) and collection of blood samples. The femoral vein was surgically exposed and a 7 F catheter (Arrow International, Reading, PA) was advanced for continuous drug application. In addition, the internal jugular vein was exposed and a 5F saline filled catheter (Arrow International) was placed to measure the jugular blood temperature that highly reflects core temperature (Polderman and Herold, 2009). A 12F catheter (Balloon Catheter; Teleflex Medical) was inserted into the bladder through suprapubic access to drain urine. Blood gas values were assessed regularly (ABLFlex800; Radiometer, Willich, Germany).
Cooling systems
After completion of surgical preparations, animals were randomized to an EHE or blanket group (n = 8). Subsequently, the catheter recording the jugular temperature was connected to a cooling device (HICO Variotherm 555; Hirtz & Co KG, Cologne, Germany).
In the EHE group, an uninflated manufactured EHE was blindly inserted into the esophagus. Design, composition, and safety of the EHE were evaluated in previous studies by our group (Schroeder et al., 2017, 2018). In brief, the EHE consisted of medical silicone 600 mm in length with a diameter of 11 mm. Within the tube, a forward and return flow supplied water from the cooling device and back, respectively. A third tube provided gastric suctioning. In the blanket group, two water-circulating cooling blankets (Hirtz & Co KG) were applied below (Ø 120 × 70 cm) and above (Ø 50 × 30 cm) the pig. Both EHEs and water-circulating cooling blankets were perfused with purified water. Using a closed-loop feedback system, the cooling device continuously registered core temperatures and adjusted the temperature of purified water to the requirements of the study protocol. Purified water was cooled to a minimum of 3°C and a maximum of 41°C, which was considered to be safe previously (Laptook et al., 2014; Schroeder et al., 2018).
Experimental study protocol
Ambient temperatures were measured by use of a Pt100 resistance thermometer (e.g., P-M-A-6-100-0-TS-2; Omega Engineering GmbH, Deckenpfronn, Germany), which was placed in the surgery room. All temperatures were recorded continuously (Labview; National Instruments Germany, Munich, Germany). Hemodynamic and ventilation parameters were recorded in 15-minute intervals.
Before initiation of baseline measurements, air-circulating blankets were removed. Animals were cooled to a target core temperature of 33°C as fast as possible, which was maintained for 8 hours before initiation of rewarming with an intended rate of 0.25°C/h. At the end of the experiment, pigs were killed using an overdose of pentobarbital (80 mg/kg; Pentobarbital-Natrium; CP Pharma, Burgdorf, Germany) without regaining consciousness. Esophagi were resected and divided into four segments: laryngeal, cranial, medial, and caudal segment.
Histopathology
Esophagi of animals of both groups (n = 8 per group) were compared with the animals in the blanket group serving as control. Immediately after harvesting, esophageal tissue segments were fixed in 4% formalin for 24 hours and subsequently embedded in paraffin. Laryngeal, cranial, medial, and caudal esophageal segments were cut into slices of 2–3 μm thickness. Afterward, slices were stained with hematoxylin and eosin on a glass slide. One slide of each segment was examined under light microscopy in 4 × and 20 × magnification (Olympus BX40; Olympus Deutschland GmbH, Hamburg, Germany). An animal pathologist blinded to the experimental setting assessed esophageal tissue damage according to a modified scoring protocol previously described (Lequerica et al., 2009; Schroeder et al., 2018). In brief, a numerical score for the following histological characteristics was assessed: epithelial hyperplasia, epithelial damage, edema (transmural), hyperemia, reactive submucosal glands, intraepithelial inflammation, and submucosal inflammation. Each location received a numerical score: 0 points: no specific findings, 1 point: focal tissue alteration, and 2 points: multifocal tissue alterations. Intraepithelial and submucosal inflammation received 0 points for no specific findings, 1 point if <5 mononuclear inflammatory cells per field were found and 2 points if >5 mononuclear inflammatory cells per field were found. The sum was calculated for each slice. Sum scores from 0 to 4 represented mild, 5–8 moderate, and >9 severe esophageal tissue damage (Schroeder et al., 2018).
Statistical analysis
All data were collected using Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA). Calculations, statistical analysis, and graphing were performed with GraphPad Prism Version 8.0.0 (GraphPad Software, San Diego, CA). All data were expressed as mean ± standard deviation (SD) if not stated otherwise. Esophageal damage score is ordinally scaled and was therefore described as median (lower quartile; upper quartile). Because of the small sample size, group differences were tested by the nonparametric Mann–Whitney U-test. Repeatedly measured variables were tested using two-way analysis of variance and post hoc Holm–Šídák tests. A value of p < 0.05 was considered statistically significant.
Results
Body weight and temperature profiles
Mean body weights were 82.2 ± 3.7 kg (EHE) and 84.4 ± 3.8 kg (blanket, n.s.). Mean ambient temperatures during cooling period were 21.8 ± 0.6°C (EHE) and 22.1 ± 0.9°C (blanket, n.s.). Mean ambient temperatures during maintenance were 21.7 ± 0.8°C (EHE) and 21.8 ± 0.7°C (blanket, n.s.). Mean ambient temperatures during rewarming period were 21.7 ± 0.6°C (EHE) and 22.1 ± 0.7°C (blanket, n.s.). Mean entire time of placement of the cooling devices were 1130 ± 36 minutes (EHE) and 1181 ± 17.6 minutes (blanket, p = 0.0002). At initiation of cooling, mean core temperatures were 38.4 ± 0.2°C (EHE) and 38.3 ± 0.2°C (blanket, n.s.). Mean cooling rates were 1.3 ± 0.1°C/h (EHE) and 3.2 ± 0.5°C/h (blanket, p < 0.0002; Fig. 1). Mean difference to target core temperatures during maintenance ranged between ±1°C (Polderman and Herold, 2009) (Fig. 2). Mean rewarming rates were 0.21 ± 0.01°C/h (EHE) and 0.22 ± 0.02°C/h (blanket, n.s.; Fig. 1).
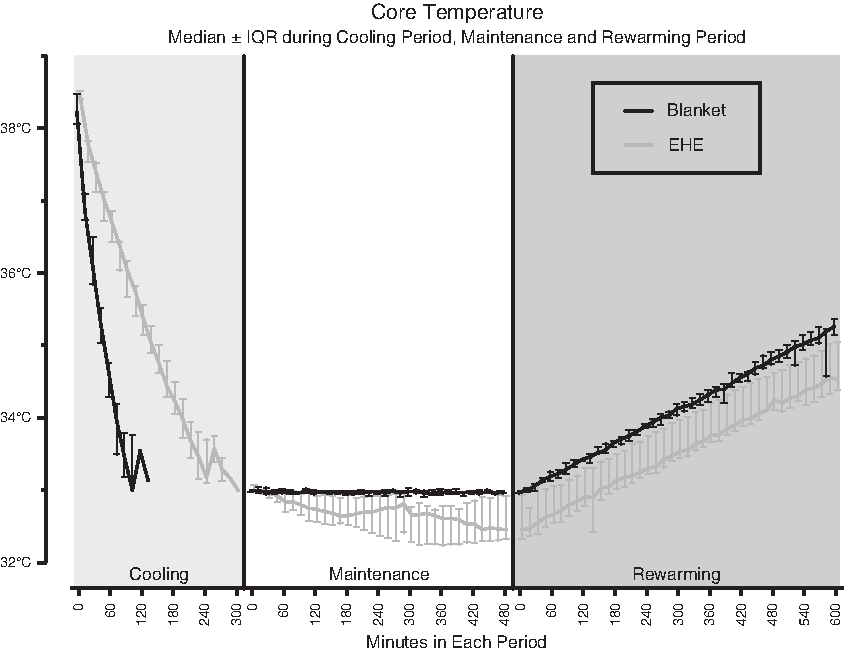
Temperature profile. Median ± IQR of core temperature in °C during the entire targeted temperature management protocol. EHEs, esophageal heat exchangers; IQR, interquartile range.
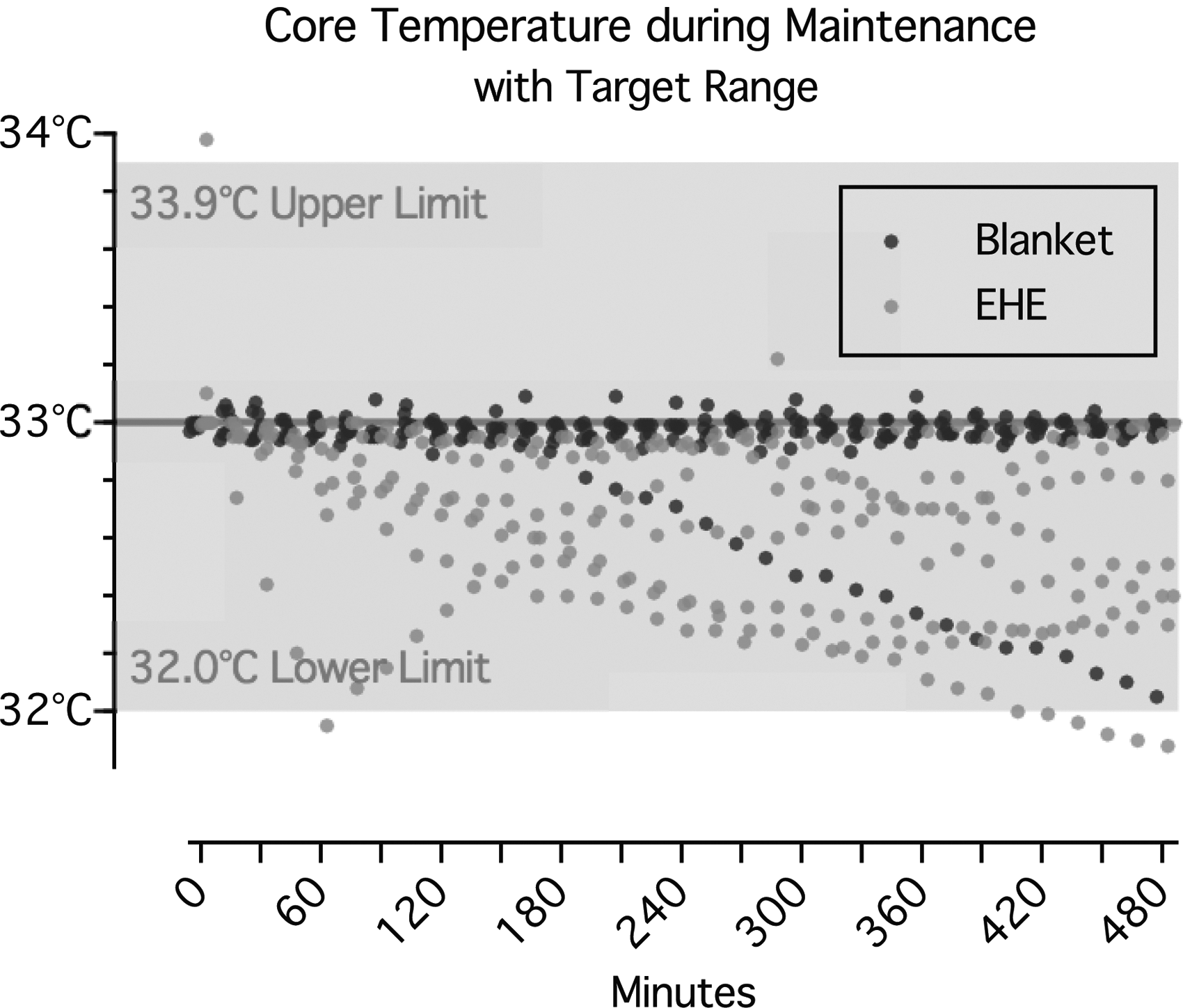
Variability of core temperature during maintenance. Core temperature in °C during maintenance for each individual randomized to EHE or blanket group. The gray area indicates the target range from 32°C to 33.9°C (Polderman and Herold, 2009).
Hemodynamic and electrolytes
Mean heart rate and mean arterial blood pressure were not significantly different between the groups during the entire TTM protocol (Supplementary Figs. S1 and S2). Mean ± SD throughout the whole experimentation for sodium were 141.1 ± 1.9 mmol/L (EHE) and 140.3 ± 1.6 mmol/L (blanket, n.s.; Supplementary Fig. S3). Chloride levels were 112.3 ± 4.9 mmol/L (EHE) and 109.9 ± 4.3 mmol/L (blanket, n.s.; Supplementary Fig. S4). Potassium levels were 4.3 ± 0.2 mmol/L (EHE) and 4.3 ± 0.2 mmol/L (blanket, n.s.; Supplementary Fig. S5). Calcium levels were 1.43 ± 0.05 mmol/L (EHE) and 1.41 ± 0.03 mmol/L (blanket, n.s.; Supplementary Fig. S6). pHs were 7.40 ± 0.04 (EHE) and 7.41 ± 0.03 (blanket, n.s.; Supplementary Fig. S7). Base excesses were 0.45 ± 2.49 mmol/L (EHE) and 1.7 ± 2.06 mmol/L (blanket, n.s.; Supplementary Fig. S8). Hematocrit levels were 23.1 ± 0.9% (EHE) and 23.2 ± 0.8% (blanket, n.s.; Supplementary Fig. S9). Blood glucose levels were 4.0 ± 0.1 mmol/L (EHE) and 4.2 ± 0.2 mmol/L (blanket, n.s.; Supplementary Fig. S10).
Side effects
Shivering was not detected in any group during the entire TTM protocol. Thus, muscle relaxation using rocuronium could be avoided in all animals. There were no clinically relevant differences in brady- or tachycardia, hypo- or hyperkalemia, hypo- or hyperglycemia, hypotension, or overcooling.
Histopathology
We did not detect relevant esophageal tissue damage (Fig. 3). Median damage scores were 6 [3; 6] (EHE) and 5 [3.25; 5.75] (blanket, n.s.) for laryngeal esophageal segments, 3 [2; 3] (EHE) and 4 [3; 5] (blanket, n.s.) for upper esophageal segments, 2.5 [1.25; 3.75] (EHE) and 3 [1.25; 4] (blanket, n.s.) for medial esophageal segments, and 2 [1; 3] (EHE) and 1 [1; 2.5] (blanket, n.s.) for lower esophageal segments. Occasional mild mononuclear acute inflammatory transepithelial infiltrates were found in laryngeal esophageal segments in both groups but not in other tissue segments.
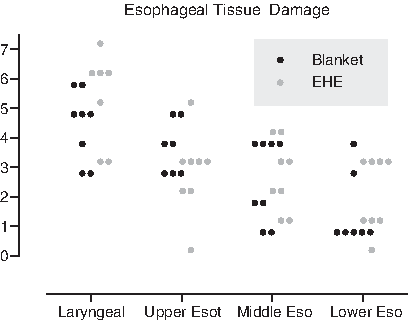
Esophageal tissue damage score. Adapted esophageal tissue damage score for each individual randomized to EHE or blanket group.
Discussion
In this prolonged experimental TTM study protocol use of water-circulating cooling blankets resulted in faster cooling rates than EHEs. Both devices met the prerequisites during maintenance and rewarming period but with more variability in EHE group. No clinically relevant esophageal tissue damage or other relevant side effects were observed.
Despite enormous scientific efforts, the most advantageous cooling method and the optimal time to reach the target core temperature after cardiac arrest still remains unclear (Nolan et al., 2015; Kim et al., 2018). There is scientific evidence that rapid cooling after cardiac arrest may be favorable to reduce cerebral damage (Bernard et al., 2002; Polderman and Herold, 2009; Che et al., 2011). On the contrary, faster decline of the core temperature predicts poor neurological outcome (Haugk et al., 2011). Thus, evaluation of cooling rates is of major importance in choice of the adequate cooling method and was the focus in this study.
Interestingly, surface cooling rates in this study exceeded surface cooling rates of human studies by three times (Hoedemaekers et al., 2007). However, narcotized swine suffer from undesired surface cooling of ∼4.8°C/h (Dingley et al., 2018). In addition, cooling rates of ∼8–12°C/h are also reported by other groups evaluating cooling blankets in pigs (Haugk et al., 2010; Weihs et al., 2011). Haugk et al. (2010) even reported a faster cooling rate of 8°C/h by surface cooling compared with endovascular cooling in pigs. We conclude that multiple factors may influence cooling rates by surface cooling in pigs: (1) weight and age (Haugk et al., 2010), (2) structural differences to the human skin such as bristles, higher amount of subcutaneous fat, and less vasculature (El-Kattan et al., 2000), (3) higher resting metabolism (Pehböck et al., 2014), and (4) a relatively large body surface of adult pigs (Kelley et al., 1973). Although our model with body weights corresponding to adults (>80 kg) is as close to human conditions as possible, porcine models may be overly sensitive for surface cooling, which significantly affected our results.
In the present and previous experimental studies, EHE reached cooling rates between 1.2°C/h and 2.8°C/h depending on the weight of the pigs (Kulstad et al., 2013; Schroeder et al., 2017, 2018). Finally, extrapolation to clinical conditions may reveal cooling rates considered to be effective for neuroprotection (Polderman and Herold, 2009). However, clinical data containing four patients after return of spontaneous circulation and one study involving 17 comatose survivors after out of hospital cardiac arrest point toward lower cooling rates (0.26–0.42°C/h) achievable by EHE compared with water-circulating cooling blankets (Moulaert et al., 2009; Goury et al., 2017; Hegazy et al., 2017; Kim et al., 2018). Thus, further clinical studies are needed to demonstrate benefits of EHE in patients suffering from cardiac arrest and other therapeutic indications for TTM.
Our aim was to simulate a TTM protocol as close as possible to critical care conditions. Thus, after reaching the target core temperature, we maintained this temperature for 8 hours and simulated rewarming at a rate of 0.25°C/h as is actually recommended. Although the rewarming rate was comparable in both groups, higher temperature fluctuations during maintenance (>0.5°C) were demonstrated in the EHE group, which could lead to long-term side effects such as pneumonia and wound infections. Interestingly, EHEs were comparably effective during maintenance in other studies (Kulstad et al., 2012, 2013; Naiman et al., 2016; Hegazy et al., 2017; Schroeder et al., 2017, 2018; Khan et al., 2018). As discussed above, the porcine model with its characteristics may have also influenced maintenance period, which could explain deviations from target core temperature in this study.
One major concern using the EHE may be possible esophageal tissue damage during long-term exposure to cold or heat. The EHE remained in place for at least 18 hours in this “prolonged” study simulating the situation in the critical care unit. Even in this prolonged setting we did not detect clinically relevant esophageal tissue damage, which is in accordance to previous studies (Kulstad et al., 2013; Schroeder et al., 2017). Presumably, food-related mild mononuclear acute transepithelial invasion of inflammatory cells leads to higher esophageal tissue damage in laryngeal segments, which is reported to be a physiological process (Desai et al., 2005) and in line with other studies investigating EHE in porcine models (Schroeder et al., 2017, 2018). Mild laryngeal tissue damage is also conceivable during endotracheal intubation in 80 kg pigs demonstrating prominent throat tissue, which was, however, uncomplicated in this study. Furthermore, we did not observe any other unwanted side effects such as brady- or tachycardia, hypo- or hyperkalemia, hypo- or hyperglycemia, hypotension, hypoxemia, or shivering (Buse et al., 2017).
Several limitations have to be considered. First, this study was conducted in the absence of cardiac arrest. The core temperature is mainly dependent on neurologic damage (Perman et al., 2015) and impaired hemodynamics. Both were at a physiological level in our study, which may have influenced performance of cooling and rewarming. Finally, there is a large body of evidence that general anesthetics such as fentanyl, propofol, and midazolam affect vegetative thermoregulatory control and decrease core temperature (Sessler, 2008). To avoid inhomogeneous baseline temperatures, we reduced perioperative hypothermia during surgical preparation by covering and actively rewarming the pigs with air-circulating blankets. Thereby, we were able to confirm clinical data in a controlled experimental environment.
Conclusions
Target temperature can be achieved faster by water-circulating cooling blankets. EHEs and water-circulating cooling blankets were demonstrated to be reliable and safe cooling devices in a prolonged porcine TTM model with more variability in the EHE group. EHE may usefully supplement cooling methods for TTM.
Footnotes
Acknowledgments
We are thankful to Manuela Lerwe and Irmgard Henke, Center for Experimental Medicine, University Hospital of Cologne, Cologne, Germany for their particular expertise in histopathological tissue preparation. We also thank Karsten Ehlert; Hirtz & Co. KG, Cologne, Germany for his technical expertise. This work was supported by “The Central Innovation Program for Small and Medium-sized enterprises,” German Federal Ministry for Economic affairs and Energy (KF2429611AK3) (H.H.). Equipment and funding was provided by Hirtz & Co. KG, Cologne, Germany.
Author Disclosure Statement
B.W.B. is European Resuscitation Council Board Director Science and Research; Chairman of the German Resuscitation Councils (GRC); Member of the “Advanced Life Support” Task Force of the International Liaison Committee on Resuscitation; Member of the executive committee of the German Interdisciplinary Association for Intensive and emergency Medicine (DIVI); Associate Editor of the European Journal of Anaesthesiology, Co-Editor of “Resuscitation”; Editor of the journal “Notfall + Rettungsmedizin.” He received professional fees for lectures from the following companies: Medupdate, Forum for Medizinische Fortbildung, Baxalta, Bayer Vita, Zoll, BARD. T.A. received research grants sponsored by Corpuls, CytoSorbens, Pulsion, Medtronic, Köhler Chemie, Centre of Integrated Oncology Köln-Bonn (CIO). H.H., D.S., T.A., and T.N. received funding from the “The Central Innovation Program for Small and Medium-sized enterprises,” German Federal Ministry for Economic affairs and Energy. This work was supported by Hirtz & Co. KG, Cologne, Germany (Equipment). No author received charges, and so forth, from industrial partners or from a third party. No author has any financial or personal relationship with other people or organizations that could inappropriately influence this work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.