
Abstract
The aim of this study was to evaluate the incidence and determinants of acute respiratory distress syndrome (ARDS) after cardiac arrest (CA). We conducted an observational, retrospective cohort study with consecutive adult out-of-hospital and in-hospital (occurred only in the emergency department, ED) CA survivors from our ED. Development of ARDS was identified by results of arterial blood gases, chest images, and transthoracic echocardiography according to the Berlin definition. The primary outcome was the poor neurologic outcome, defined as cerebral performance category ≥3 at 28 days, and secondary outcomes were 28-day mortality, recovery rate from ARDS, duration of mechanical ventilator use, and length of stay. Among 295 enrolled patients, 30 patients who received extracorporeal membrane oxygenation and 19 patents who had cardiogenic pulmonary edema were excluded. ARDS had developed in 119 (48.4%) patients on admission (mild 20 [16.8%], moderate 48 [40.3%], and severe 51 [42.9%]) and 54 (45.4%) patients recovered before hospital discharge. Development of ARDS was associated with poor neurologic outcomes at 28 days (adjusted hazard ratio (HR) 1.44 [95% confidence interval (CI): 1.05–1.98]). Moreover, more severe ARDS was associated with a higher risk of poor neurological outcomes (mild: reference; moderate: adjusted HR 1.66 [95% CI: 1.10–2.49]; and severe: adjusted HR 1.76 [95% CI: 1.16–2.65]). Therefore, development of ARDS after CA was associated with unfavorable neurologic outcomes and had a linear association with ARDS severity. Early recognition and proper management of ARDS may be useful during post-CA care.
Introduction
Cardiac arrest (CA) is a global public health problem with an estimated crude incidence of 55 cases of out-of-hospital CA per 100,000 person-years and 10 cases of in-hospital CA per 1000 hospital admissions (Berdowski et al., 2010; Andersen et al., 2019). While there have been major advances in prevention and resuscitation strategies, morbidity and mortality rates remain unacceptably high (Kong et al., 2011; Kim et al., 2016; Kang et al., 2019). This is largely due to postcardiac arrest syndrome (PCAS), which comprises postarrest brain injury, postarrest myocardial dysfunction, and systemic ischemia–reperfusion injury (Nolan et al., 2008; Stub et al., 2011).
After CA, lung injury may arise from ischemia, mechanical trauma caused by chest compression, the effects of mechanical ventilation, and the use of supplemental oxygen (Neumar et al., 2008). Pulmonary system function, which controls the concentration of oxygen and carbon dioxide, may affect brain injury severity during and after CA (Hope Kilgannon et al., 2019). Moreover, recent studies identified the lungs as a modulator of systemic inflammation following CA and that brain–lung immunologic coupling could have effects on both lung function and secondary central nervous system injury (Aslami et al., 2012; Mai et al., 2019).
Acute respiratory distress syndrome (ARDS), according to the Berlin definition, is defined as an inflammatory disorder caused by lung injury, which results in respiratory failure that is not fully explained by cardiac failure or volume overload with hypoxemia, decreased lung compliance, and bilateral opacities on chest images (Fan et al., 2018). ARDS may develop as a result of CA itself or as a result of aspiration or trauma from mechanical compression or ventilator-associated lung injury (Jia et al., 2008; Cha et al., 2017). The reported incidence of postarrest ARDS varies widely across a few studies, with a range from 5% to 65% depending on ARDS definition (Sutherasan et al., 2015). Although (very recently) one study found that ARDS was associated with poor outcomes, the clinical impact of ARDS on neurologic outcomes is not fully understood, especially based on ARDS severity.
We hypothesized that ARDS will negatively impact neurologically intact survival by disturbing adequate oxygenation and ventilation functions. Considering this, we investigate the incidence of ARDS using the Berlin definition and evaluate the impact of ARDS severity on clinical outcomes in CA survivors.
Materials and Methods
Study design and setting
This retrospective observational study was performed between January 1, 2011, and April 30, 2019, at the Asan Medical Center located in Seoul, Korea. The Asan Medical Center is a university-affiliated teaching hospital with an annual census of ∼130,000 visits in the Emergency Department (ED). The Institutional Review Board of the study facility approved our study and waived the requirement for informed consent because of the retrospective observational design (study no.: 2019-1187).
Study population
As we mentioned in our previous reports, we registered all consecutive comatose adults (age ≥18 years) who were nontraumatic out-of-hospital and in-hospital (occurred in ED, but not in the ward or intensive care unit, ICU) CA survivors (Ryoo et al., 2015; Kim et al., 2019). Survivors were defined as patients achieving sustained return of spontaneous circulation (ROSC) with a palpable pulse detected for over 20 minutes. Patients who had ROSC before ED arrival and received mechanical ventilation were also included. Patients were excluded from the registry if they had presumed traumatic arrest, do-not-resuscitate orders, and alert mentality immediately following ROSC; were transferred to another hospital due to lack of ICU; and if the patient or surrogate refused proper post-CA management, including target temperature management (TTM). We also excluded patients who received extracorporeal membrane oxygenation (ECMO) during or after CA and had cardiogenic pulmonary edema based on the result of transthoracic echocardiography.
Routine post-CA care was conducted according to the recommendations of the American Heart Association. In summary, all comatose patients after ROSC received TTM with or without the percutaneous coronary intervention (PCI) except when there were absolute contraindications of TTM (Eastwood et al., 2016). After admission, TTM was initiated as soon as possible using an Arctic Sun system (Bard Medical, Louisville, CO) to reach a target temperature of 33°C, which was maintained for the next 24 hours. After 24 hours, rewarming to 36.5°C at a rate of 0.25°C/hour was done. During the whole period of TTM, sedative and paralyzing drugs were actively used to control shivering. All patients received mechanical ventilation in a pressure-controlled mode.
Data collection
As part of our routine management protocol, we obtained the repeated arterial blood gas analysis (ABGA) measurements after ROSC. Whenever ventilator settings were changed, ABGA was performed in 20 ± 10 minutes. Moreover, ABGA was repeated every hour during the induction period of hypothermia and every 2 hours during the maintenance phase. At the time of ABGA collection, all ventilator parameters, including inspiratory pressure, respiratory rate, positive end-expiratory pressure, and minute ventilation, were recorded. All ABGAs were tested by point-of-care analyzers located in the ED or ICU (RAPIDPoint 500 systems; Siemens, Munich, Germany). We assessed patients' pulmonary function by measuring the partial pressure of arterial oxygen (PaO2)/fraction of inspired oxygen (FiO2) (P/F) ratio.
Chest images and transthoracic echocardiography were routinely performed after ROSC. All chest images were evaluated by board-certified radiologists on duty, and all reports included key terminologies to discriminate characteristics of pulmonary opacities. Three independent investigators (J.S.K., Y.J.K., and M.Y.K.) reviewed the images and reports to refine suitable classification. Moreover, about 20% of images were randomly assigned for assessment by a blinded emergency medicine physician, and agreement between the reports and reviewer was assessed. Based on these data, within 48 hours after ROSC, the development of ARDS and its severity were diagnosed using the Berlin definition (Fan et al., 2018). In brief, we discovered that those who had two consecutive PF ratios <300 mmHg had bilateral radiographic opacities on chest images that could not be explained by collapse, effusion, or nodules and had respiratory failure that could not be explained by pure cardiogenic edema within 48 hours. Pulmonary edema due to purely cardiogenic causes was considered when the measured left ventricle ejection fraction was below 30%. Severity was classified by the degree of hypoxemia: mild (200 < PF ratio ≤300 mmHg), moderate (100 < PF ratio ≤200 mmHg), and severe (PF ratio ≤100 mmHg).
We abstracted demographic and baseline information from our CA registry, including age, sex, and underlying diseases. In addition, we collected data about CA according to the Utstein Style recommendations, such as witnessed arrest, bystander cardiopulmonary resuscitation (CPR), and total CPR duration. The sequential organ failure assessment (SOFA) score was calculated using initial admission variables. Left ventricle ejection fraction was measured using the Teichholz method, and E/e' ratios were calculated through tissue Doppler imaging at both the septal and lateral mitral origins of the four-chamber view, following guidelines of the American Society of Echocardiography. The primary outcome of interest was poor neurologic outcome, defined by a cerebral performance category (CPC) score ≥3 at 28 days (Sandroni et al., 2018). If patients had been discharged before 28 days, we routinely telephoned the survivors and recorded the CPC score. The secondary outcomes were 28-day mortality, ARDS recovery rate, duration of mechanical ventilator use, duration of ICU stay, and overall hospital stay. Recovery from ARDS was defined when three consecutive P/F ratios were checked above 300 on ABGA, which indicated recovery from respiratory failure (Fan et al., 2018).
Statistical analyses
Statistical analyses were conducted by using the SPSS Statistics for Windows, version 23 (SPSS, Inc., Armonk, NY). All continuous variables were presented as medians with interquartile ranges. Categorical variables were assessed with the chi-square test or Fisher exact test. Normality of distribution was tested with the Kolmogorov–Smirnov test. Mann–Whitney U tests were performed for comparisons between patients with and without ARDS. Twenty-eight day survival with good neurologic outcome (CPC score ≤2) curves was calculated using the Kaplan–Meier method and compared by the log-rank test. Associations between occurrence of ARDS and 28-day neurologic outcome were evaluated by the Cox proportional hazards model to evaluate the hazard ratios (HRs) and 95% confidence intervals (CIs). According to previous CA studies, we selected variables that could affect neurologic prognosis, such as age, sex, witnessed CA, bystander CPR, TTM, shockable rhythm during CPR, presumed cardiac cause, and duration of CPR for adjustment (Hassager et al., 2018). A two-sided p-value below 0.05 was considered statistically significant.
Results
Incidence and recovery of ARDS and baseline characteristics
During the study period, 295 adults were enrolled in the CA registry, and 246 patients were finally registered in this study after exclusion of 49 patients who received ECMO and had cardiogenic pulmonary edema (Fig. 1). Among the survivors, a total of 48.4% (119/246) developed ARDS on admission and 45.4% (54/119) recovered from ARDS. Overall survival to hospital discharge was 52.1% (62/119), and 35.5% (22/62) had a good neurologic outcome (CPC 1 or 2) at 28 days after CA.
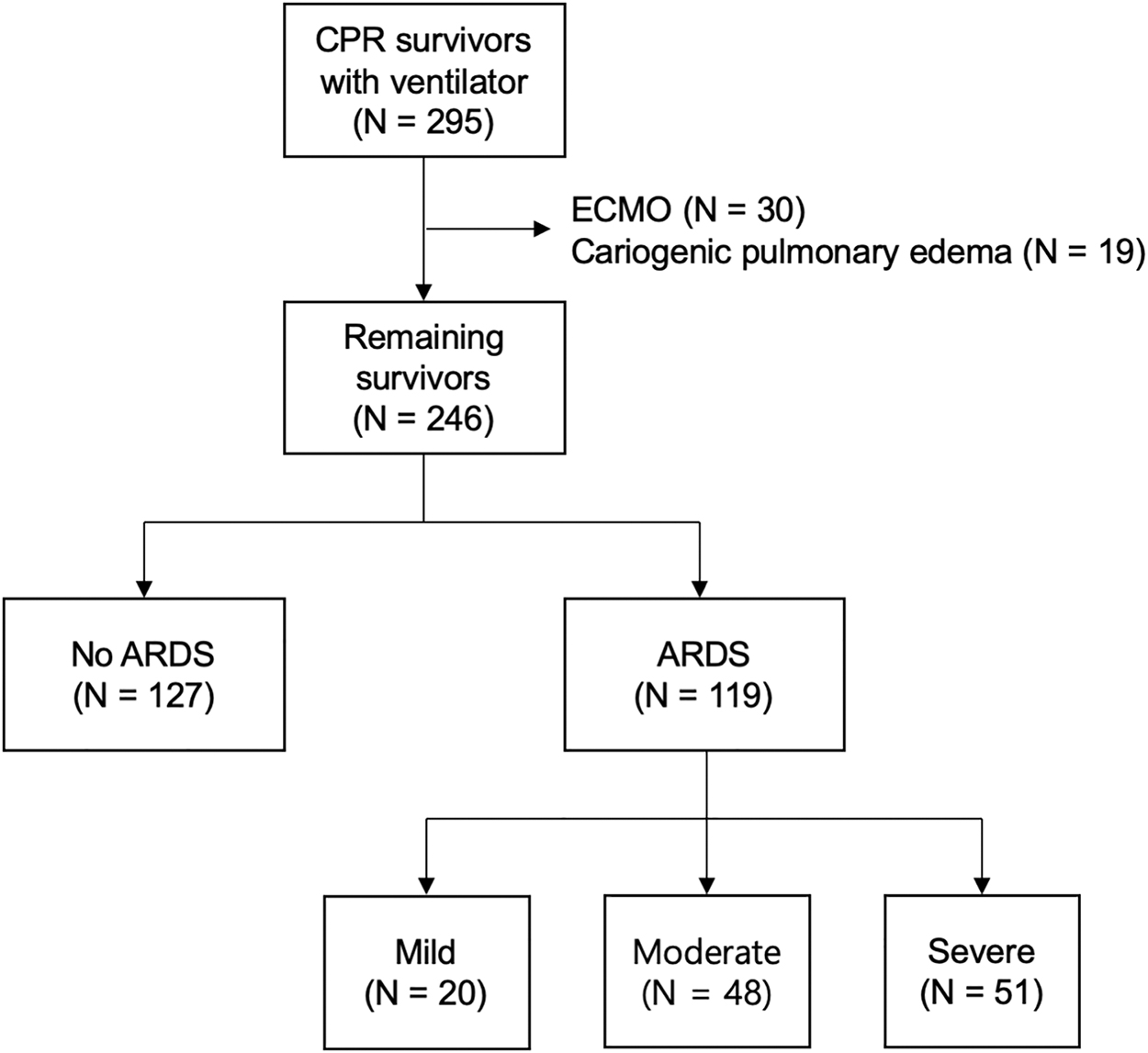
Study flowchart. ARDS, acute respiratory distress syndrome; CPR, cardiopulmonary resuscitation; ECMO, extracorporeal membrane oxygenation.
Baseline characteristics of the study population are summarized in Table 1. Median age at the time of admission was 62 years with male predominance and patients with ARDS were older than those without ARDS (66 vs. 56 years, p < 0.001). Patients with ARDS were more likely to have previous PCI history, hypertension, diabetes, and chronic kidney disease. Fewer patients with ARDS had a shockable rhythm during CPR and requirement of emergent PCI compared with patients without ARDS. Moreover, patients with ARDS had longer mean CPR duration and SOFA scores at admission. Regarding ventilator parameters, the ARDS group showed lower pH, pO2, and tidal volumes, but higher requirement of positive end-expiratory pressure, inspiratory pressure, and minute ventilation.
Study Population Baseline Characteristics
Data are presented as n (%) or median with interquartile ranges.
ABGA, arterial blood gas analysis; ARDS, acute respiratory distress syndrome; CPR, cardiopulmonary resuscitation; EF, ejection fraction; LV, left ventricle; MV, mechanical ventilator; PCI, percutaneous coronary intervention; PEEP, positive end-expiratory pressure; TTE, transthoracic echocardiography; TTM, target temperature management; sBP, systolic blood pressure; dBP, diastolic blood pressure; SOFA, sequential organ failure assessment.
Clinical impact of development of ARDS
Regarding clinical outcomes of CA, patients with ARDS had worse outcomes than patients without ARDS (Table 2). Patients who developed ARDS were more likely to have unfavorable neurologic recovery (81.5% vs. 60.6%, p < 0.001) and had higher all-cause mortality (61.0% vs. 37.8%, p < 0.001) at day 28. Meanwhile, patients with ARDS stayed for a shorter duration both in the ICU (7 days vs. 8 days, p = 0.060) and overall hospital admission (8 days vs. 9 days, p = 0.002). The percentage of patients who had a favorable outcome at 28 days was 39.4% in the no ARDS group, compared with 19.3% in the ARDS group (Fig. 2). Kaplan–Meier curves for estimated neurologic outcome showed that unfavorable neurologic outcomes (Fig. 3) and mortality (Supplementary Fig. S1) at day 28 after CA were significantly more likely in patients who developed ARDS compared with patients without ARDS (p = 0.001).
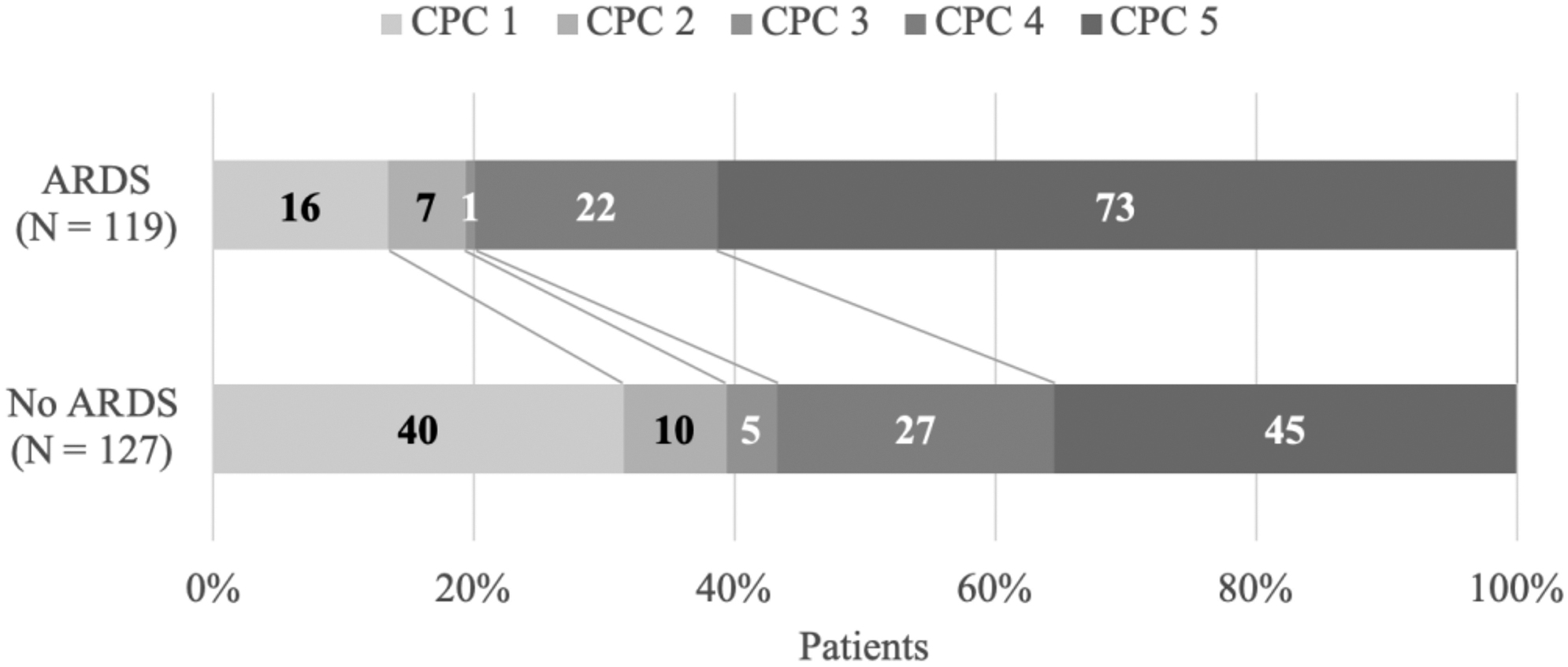
CPC score at 28 days. Category on the CPC score range from 1 to 5, with 1 indicating good performance, 2 moderate disability, 3 severe disability, 4 coma, and 5 brain death. It is dichotomized into good (CPC 1-2) versus poor (CPC 3-5) outcomes. CPC, cerebral performance category.
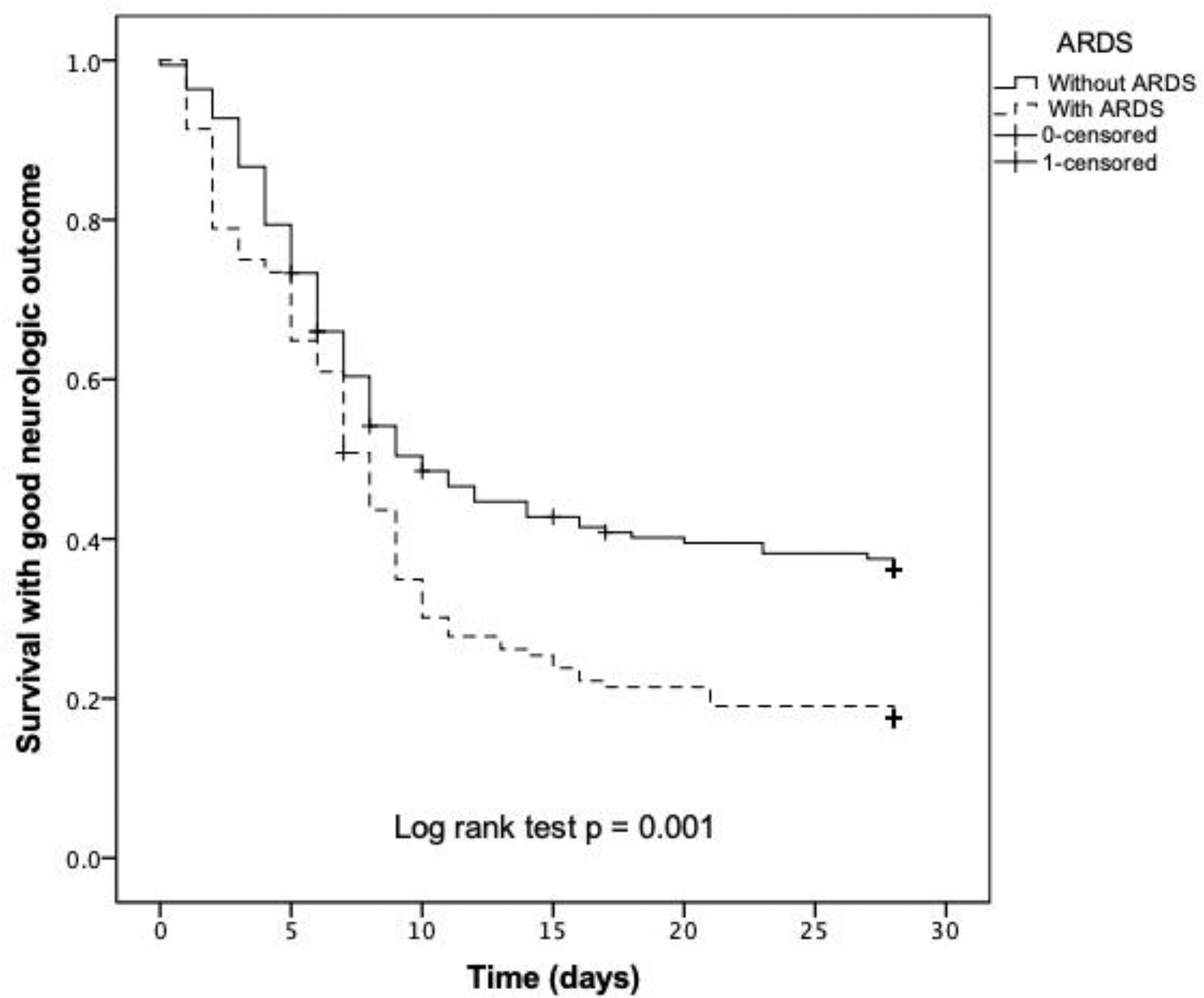
Survival rates with good neurologic outcomes at 28 days in patients with and without ARDS.
Comparison of Clinical Outcomes Between Patients With and Without Acute Respiratory Distress Syndrome
Data are presented as n (%) or median with interquartile ranges.
LOS, length of stay.
Adjusted hazard ratios for poor neurologic outcome
The Cox proportional analysis was used to identify independent risk factors for poor neurologic outcomes (Table 3). We selected well-known factors for the multivariate model that have been identified in previous studies to affect neurologic outcomes such as age, sex, witnessed arrest, bystander CPR, presence of shockable rhythm, presumed cardiac cause, and CPR duration (Hassager et al., 2018). Development of ARDS was an independent risk factor for poor neurocognitive functions in CPR survivors (adjusted HR 1.44 [95% CI: 1.05–1.98] p = 0.025). In addition, unfavorable outcomes increased proportionally according to severity based on the Berlin definition (moderate vs. severe: adjusted HR 1.66 [95% CI: 1.10–2.49] p = 0.015 vs. adjusted HR 1.76 [95% CI: 1.16–2.65] p = 0.007).
Cox Proportional Analysis of Risk of Poor Neurologic Outcomes at Day 28
HR, hazard ratio; CI, confidence interval; CPR, cardiopulmonary resuscitation.
Discussion
This study found that 48.4% patients developed ARDS after ROSC based on the serial results of ABGA, chest images, and echocardiography used to diagnose ARDS among comatose CPR survivors, and the occurrence of ARDS is independently related to poor neurological outcomes. In addition, the severity of ARDS according to the Berlin definition has a linear relationship with neurologic deficit. These results extend the knowledge that ARDS is a life-threatening condition of respiratory failure, which affects not only mortality but also neurologic outcomes in CA survivors.
The true incidence of ARDS following CA is not well studied. This is largely because ARDS contains heterogeneous entities, there is no single diagnostic test, and inaccuracies limit effective surveillance (Pham and Rubenfeld, 2017). Prior studies reported the incidence of postarrest ARDS (defined as an initial P/F ratio ≤300 with no information about chest imaging and echocardiography) ranging from 5% to 65% among survivors (Elmer et al., 2015; Sutherasan et al., 2015); meanwhile, one recent study found that 48% of patients developed ARDS after ROSC according to the Berlin definition (Johnson et al., 2019). This is consistent with our findings of 48.4% and implies that development of ARDS following CA is not uncommon. Possible reasons for the high incidence of ARDS after CA are that CA and resuscitation increase typical risk factors for development of ARDS, such as aspiration during apnea periods, lung contusions from chest compression, and barotrauma from mechanical ventilation (Cha et al., 2017). Supplementary high fractional oxygen during acute care and secondary infections also contribute to both lung and brain injury. In addition, PCAS-induced inflammation, immune cell activation, and alveolar permeability alteration can also induce ARDS (Junttila et al., 2013; Sedy et al., 2015).
We found that development of ARDS showed poor clinical outcomes, such as higher 28-day mortality. Median duration of ICU length of stay was shorter in the ARDS group, but this might be because of higher early mortality in the ICU (Supplementary Fig. S1). We also found that ARDS was associated with not only hospital mortality but also poor neurologic outcomes. Prior studies have already revealed that the occurrence of ARDS after CA had higher in-hospital and 28-day mortality (Sutherasan et al., 2015; Harmon et al., 2018). Moreover, similar to our results, a recent retrospective study found that ARDS patients were more likely to have worse neurologic status at discharge than that of non-ARDS patients (Johnson et al., 2019). Poor neurologic outcomes related to ARDS may largely be due to mismatch between supply and demand of O2 and CO2. Johnson et al. (2017) included 544 patients and found that hyperoxemia (defined as PaO2 > 300 mmHg) at 12 hours was associated with a poor CPC score at discharge. Furthermore, Vaahersalo et al. (2014) tried to find the optimal level of CO2 during the first 24 hours, through analyzing the result of ABGA, and reported that hypercapnia (defined as PaCO2 > 45 mmHg) was associated with better long-term neurologic outcomes. The authors of these studies postulated that radical oxygen species caused by hyperoxia and vasoconstriction due to hypocarbia disturbed brain recovery.
We also found that the severity of ARDS according to the Berlin definition has a linear relationship with the likelihood of neurologic deficit. It has been well reported that greater ARDS severity is related to higher mortality. Ballani et al. (2016) recently analyzed 2,337 ICU patients and announced that increased ARDS severity contributed to both the pulmonary and nonpulmonary components of the SOFA score and correlated with longer ICU stay and in-hospital mortality. To the best of our knowledge, it is the first study to identify a correlation between ARDS severity based on the Berlin definition and the proportion of poor neurologic outcomes among CPR survivors. Our findings may be explained by the mismatch of O2 and CO2 levels found in patients experiencing ARDS, which could disrupt regeneration of the brain function (Skrifvars et al., 2019). Severe transient brain ischemia may also induce lung injury as part of the systemic inflammatory immune response. Numerous experimental studies have reported that brain injury was sufficient to affect peripheral organs by activation of the immune response (Mai et al., 2017). Meanwhile, ARDS may simply reflect the severity of illness because the SOFA score at admission was significantly higher in the ARDS group. It is also possible that higher mortality was caused by PCAS-induced multiorgan failure and not by ARDS. Nonetheless, our findings show that the severity of ARDS could be an important prognostic marker or additional treatment target for improving neurologic outcomes after CA.
There were some limitations to this study. First, even though patients in this study received consistent post-CA care by the emergency ICU team, its retrospective design imposes intrinsic limitations and our results may not be generalizable. Second, we did not exclude all possible cardiogenic pulmonary edema, even ABGA, chest imaging, and echocardiography were used for diagnosing ARDS, and the incidence of ARDS might be overestimated. However, discriminating all hydrostatic edema cases induced by cardiogenic causes could be impossible in real situations and the Berlin definition also showed flexibility in the diagnosis of ARDS. Third, the exclusion of patients who received ECMO, had a terminal illness, or were transferred to another hospital may contribute to selection bias. Fourth, although we input the necessary data for Cox regression analysis for adjustment due to the registry design, we could not consider other factors such as quality of CPR, real-time ventilator settings, vasopressor dosage, presence of combined infections, and volume status that could potentially impact patient outcomes. Last, temperature correction of PaO2 could change the PF ratio, and the inclusions or severity of ARDS could be different from our results. However, the effect of temperature might not have a significant influence because most patients (107/119, 90%) were diagnosed with ARDS on admission (before TTM).
Conclusions
In conclusion, development of ARDS following cardiac arrest was associated with unfavorable neurologic outcomes and risk of poor neurologic outcomes increased with the severity of the ARDS. Considering the findings of this study, further research investigating ARDS management strategies that may improve outcomes is warranted.
Footnotes
Acknowledgments
The authors thank the patients and nursing staff of the ICU, as well as the Emergency Medicine residents on duty who registered all survivors in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.