
Abstract
Inadvertent perioperative hypothermia, defined as a body temperature <36.0°C, is a common outcome of anesthesia that can cause serious consequences to patients. The aim of this study is to determine the prevalence of inadvertent hypothermia among surgical procedures from two referral centers in Brazil and to identify sociodemographic, clinical, or surgery-related predictors of hypothermia. This is a cross-sectional study, conducted at two public hospitals in Brasília, Brazil. After the exclusion of 109 patients, 312 subjects (American Society of Anesthesiologists [ASA] physical status I–III) were enrolled from July 2016 through July 2018. The main outcome measures were the prevalence of hypothermia and its predictors. The mean age of the 312 patients was 43.2 (18.2) years (range 18–85 years), and 186 (59.6%) were female. The prevalence of inadvertent hypothermia was 56.7%. Predictors of hypothermia were perioperative chills (p = 0.026), patient's body temperature on arrival in the operating room (p < 0.001), diabetes (p < 0.001), ASA status III (p < 0.001), systolic blood pressure (p < 0.001), general anesthesia (p < 0.001), medical specialty (p < 0.001), fentanyl-based anesthesia (p = 0.002), and surgery time (p < 0.001). The multivariable model prediction model for hypothermia showed fairly good discrimination (area under the receiver operating characteristic: 79.0%, 95% confidence interval 68.0 to 80.1). Approximately 6 in 10 patients undergoing surgery developed inadvertent perioperative hypothermia. The risk of hypothermia is influenced by a myriad of factors that can be used in simple and low-cost predictive models with adequate discriminatory power.
Introduction
Body thermoregulation is a vital physiological process to sustain metabolic functions and homeostasis. In humans, this process is tightly regulated and may trigger autonomic compensatory defenses against fluctuations in the temperature of the external environment (Lopez et al., 1994; Sessler, 1997).
A combination of factors unique to surgical procedures can hinder the control mechanisms underpinning this system, provoking perioperative thermal perturbations in patients. For example, during surgery, patients are exposed to a cold operating room environment and frequently receive the administration of unwarmed intravenous fluids. Moreover, neuraxial anesthesia not only decreases heat production but also increases heat loss besides inhibiting thermoregulatory compensatory responses against cold stress (Insler and Sessler, 2006; Bindu et al., 2017). As a result, inadvertent hypothermia is commonly observed in patients undergoing surgery (Persson and Lundberg, 2001).
Several lines of evidence suggest that even mild to moderate hypothermia augments the risk of serious perioperative complications (Sessler, 2001), including shivering (Jun et al., 2019), nausea, vomiting (Nalivaiko, 2018), pain (Sajid et al., 2009), hemorrhage, coagulopathies (Schmied et al., 1996; Rajagopalan et al., 2008), cardiovascular events, and mortality (Frank et al., 1997; Hart et al., 2011). It has been also reported that inadvertent perioperative hypothermia can decrease resistance to surgical-wound infection and delay postoperative recovery, prolonging patient's hospitalization (Kurz et al., 1996; Lenhardt et al., 1997).
Studies on the prevalence of perioperative hypothermia have reported estimates ranging from 20% to 90% (Long et al., 2013; Scholten et al., 2018), which most likely reflect clinical and methodological heterogeneity in the methods, including different approaches to temperature monitoring and local availability of active warming systems. Nonetheless, few data are available on perioperative hypothermia in Brazil. In this regard, a previous pilot study by our group indicated that nearly 70% of patients were at risk of developing hypothermia perioperatively, although the factors for this outcome were not completely assessed (Mendonça et al., 2019). To determine more precisely the prevalence of inadvertent hypothermia among surgical procedures, we, therefore, conducted a cross-sectional study in two major referral centers in Brazil. In addition, we investigated risk factors for hypothermia through the use of predictive modeling.
Materials and Methods
Study design
This is an investigator-initiated, two-center, cross-sectional study with prospective recruitment and data collection. The study was performed at the Hospital de Base, which is a 700-bed tertiary hospital and a regional reference center, and at the Brasília Maternal and Child Hospital, which is a specialized 300-bed hospital. Both institutions are located in Brasília, Brazil. The protocol was approved by the Institutional Review Boards at the participating institutions. We followed the STROBE checklist for reporting this study (Vandenbroucke et al., 2014).
Registration
The study was approved by the local Research Ethics Committee (Fundação de Ensino e Pesquisa em Ciências da Saúde, FEPECS, Brasília, DF, Brazil) and registered in the national and unified research record base Plataforma Brasil under CAAE number 2294615.0.0000.5553 and report number 1.418.778.
Patients
We included patients who were admitted to the participating hospitals between July 2016 and July 2018, and who underwent urgent, emergency, or elective surgeries. We enrolled patients aged 18 to 85 years with American Society of Anesthesiologists (ASA) physical status I to III. Patients who remained intubated after surgery were considered ineligible. We also excluded patients with any health-related condition that, at the discretion of the principal investigator, might pose a risk to the patient.
Sociodemographic and clinical variables
Clinical symptoms, comorbidities, surgery, and anesthetics characteristics were recorded. We monitored patient's body temperatures in different perioperative time points. Tympanic temperature was measured on the arrival in the operating room (time 0, T0) and immediately after surgery (time 1, T1). All in-hospital measurements and procedures, such as electrocardiogram, and assessments of body weight, height, blood pressure, temperature, heart rate, and blood oxygen saturation levels (SpO2) were carried out by trained research and laboratory personnel following standardized local protocols. Hypothermia was defined as a tympanic temperature <36°C. Obesity was defined as a body mass index ≥30 kg/m2. Hypertension was established as systolic blood pressure (SBP) ≥140 and/or diastolic blood pressure ≥90 mm Hg at the time of evaluation, self-reported previous diagnosis of hypertension, and/or current use of antihypertensive drugs. Diabetes was defined based on the preoperative diagnosis.
Subgroup analyses
We prespecified subgroup analyses based on medical specialty (obstetric patients vs. nonobstetric patients) and age (≥60 years vs. <60 years). These subgroup assessments were based on findings from previous clinical studies and the well-established physiological differences displayed by women during pregnancy and puerperium (Mendonça et al., 2019).
Sample size
Based on a previous pilot study (Mendonça et al., 2019), we assumed a prevalence of 72% for this condition in our institutions. Thus, to estimate the true prevalence with 5% absolute precision based on 95% confidence intervals (CI), a total sample size of 310 participants was required.
Statistical analysis
Categorical data are presented as numbers (percentage) and continuous variables as mean (standard deviation [SD]), median (interquartile range [IQR]), or means (95% CIs). The Mann–Whitney U test was used to compare the length of hospital stay and postsurgery recovery time between groups. No missing data were observed for most variables. However, numerical results could not be obtained for a few patients. In those cases, we carried forward the most recent assessment from the patient's previous medical records. If no prior information was available, we imputed missing values using the sample mean (two patients only). Mixed-effects models with a random intercept for each subject were built to examine the trajectory of patient's body temperature over time. Fixed effects were time and group (normothermic and hypothermic), and both were considered as categorical variables. Models were fitted with an interaction term between time and group. We also used logistic regression-based prediction models to calculate the probability of hypothermia of a patient given his or her sociodemographic, clinical, and surgical characteristics. Associations for dichotomous outcomes were captured as odds ratios (ORs). OR values >1 mean that for every unit increase in the predictor, there is a higher risk of hypothermia. OR values <1 are interpreted analogously, but in the opposite direction, that is, for every unit increment in the predictor, there is a lower risk for hypothermia. First, we fitted univariate logistic regression models to assess the relationship between single predictors and the outcome of hypothermia. Our goal was to estimate the diagnostic ability of each predictor when considered individually. Then, we selected all predictors with a univariable p < 0.10 and used them in a multivariable logistic regression model. Mixed-effects and logistic regression models were fitted with robust standard errors allowing for clustering effects. We used the area under the receiver operating characteristic (AUROC) curve to quantify the model predictive performance. The AUROC curve is an estimate of how accurately a model can predict an outcome, ranging from 0.5 to 1. An AUROC of 1 is optimal (100% accuracy), and an area of 0.5 indicates that the model is no better than chance at assessing the risk of an event. To correct for model overfitting, we calculated the overall predictive performance using fourfold cross-validation (Luque-Fernandez et al., 2019), in which the study sample was randomly split into four equal parts. The model was trained with a subsample (training set, 75% of the sample) and then applied to the remaining subsample (test set, 25% of the sample). The average of AUROCs across each fold is the final estimate. Chosen optimal probability cutoff values were those that optimized the sensitivity-specificity relationship. For AUROC quantification, we used center-specific propensity scores as a sampling weight to correct for the size of the number of participants in each cluster. Ninety-five percent CIs for AUROC estimates were obtained via bootstrapping. All analyses were exploratory. Two-sided p-values <0.05 were considered statistically significant. All statistical analyses were performed with Stata (version 14.0; Stata Corp., College Station, TX).
Results
General description
Sociodemographic and clinical data of the participants are summarized in Table 1. Of 421 admitted patients during the investigation period, 312 (74.1%) were assessed for eligibility (Fig. 1). Overall, the mean (SD) participant age was 43.2 (18.2) years (age range, 18–85 years). Most participants (59.6%) were women and one in four surgeries (25.3%) was from medical specializations related primarily to women's health (obstetrics and gynecology).
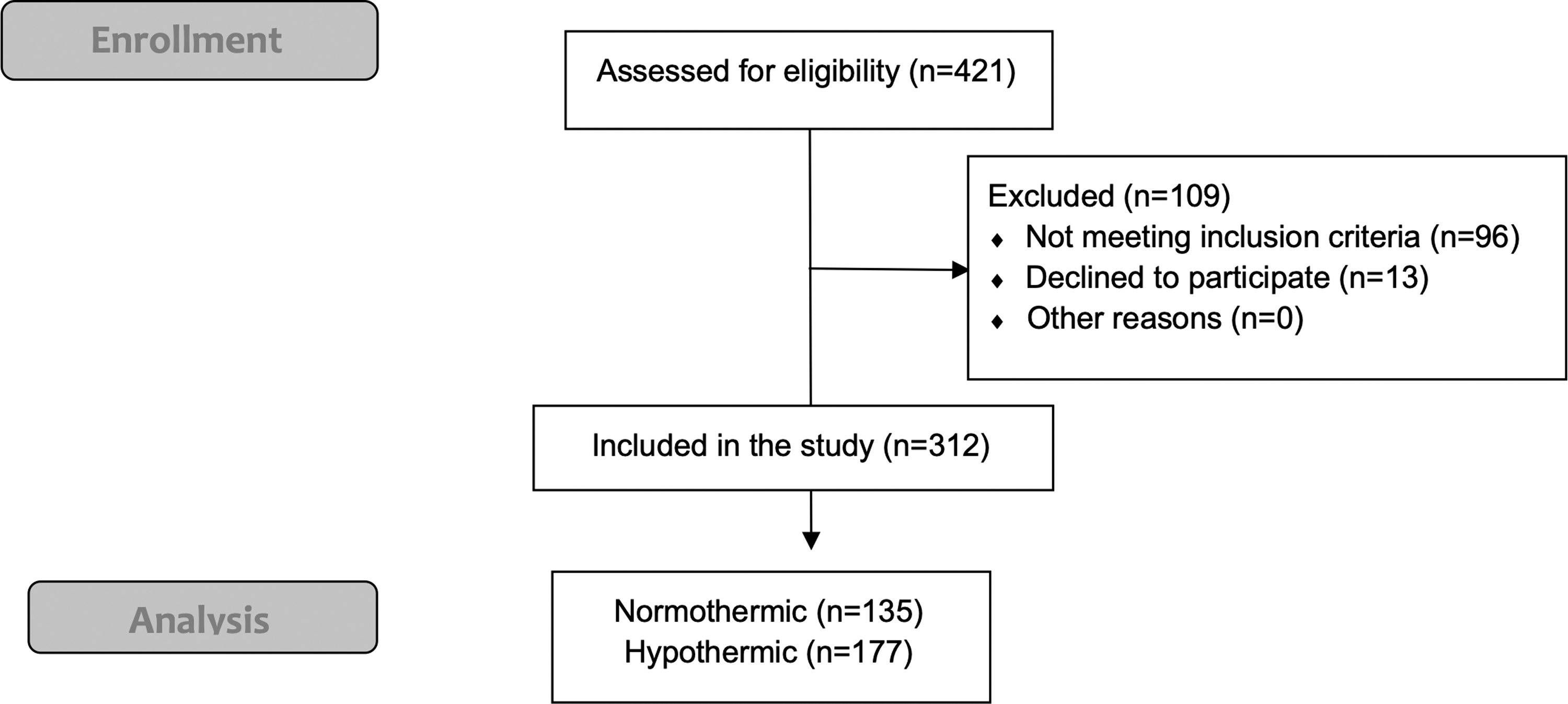
STROBE flow diagram.
Univariable Logistic Regression Models for Inadvertent Hypothermia
ASA status, American Society of Anesthesiologists physical status classification system; BMI, body mass index (kg/m2); 95% CI, 95% confidence interval; OR, odds ratio.
Prevalence of hypothermia
The number of hypothermia cases and prevalence by covariate are presented in Table 1. The prevalence of hypothermia differed between centers: in the Maternity hospital, 63 (90%) of 70 patients developed postsurgery hypothermia, whereas 114 (47.1%) out of 242 patients in the General hospital had abnormally low body temperature after surgery. Overall, among the 312 admitted patients, 177 (56.7%, 95% CI 27.4 to 86, adjusted for cluster effects) developed inadvertent hypothermia.
Body temperature in the early postoperative recovery period
Patient's body temperature on arrival in the operating room was a major predictor for hypothermia (OR = 0.22, 95% CI 0.11 to 0.45, p < 0.001). At the start of surgery, body temperature levels in patients who developed hypothermia were significantly lower than those from their normothermic counterparts (mean difference = −0.76°C, 95% CI −0.80 to −0.72, p < 0.001). The mean values of the first recorded body temperature at the recovery room were 35.8°C (95% CI 35.7 to 35.9) and 36.58°C (95% CI 36.54 to 36.61) in the hypothermic and normothermic groups, respectively (p < 0.001). Mean temperature levels were significantly lower in hypothermic patients compared to their normothermic counterparts at all evaluated time points (p < 0.008 for all comparisons) (Fig. 2).
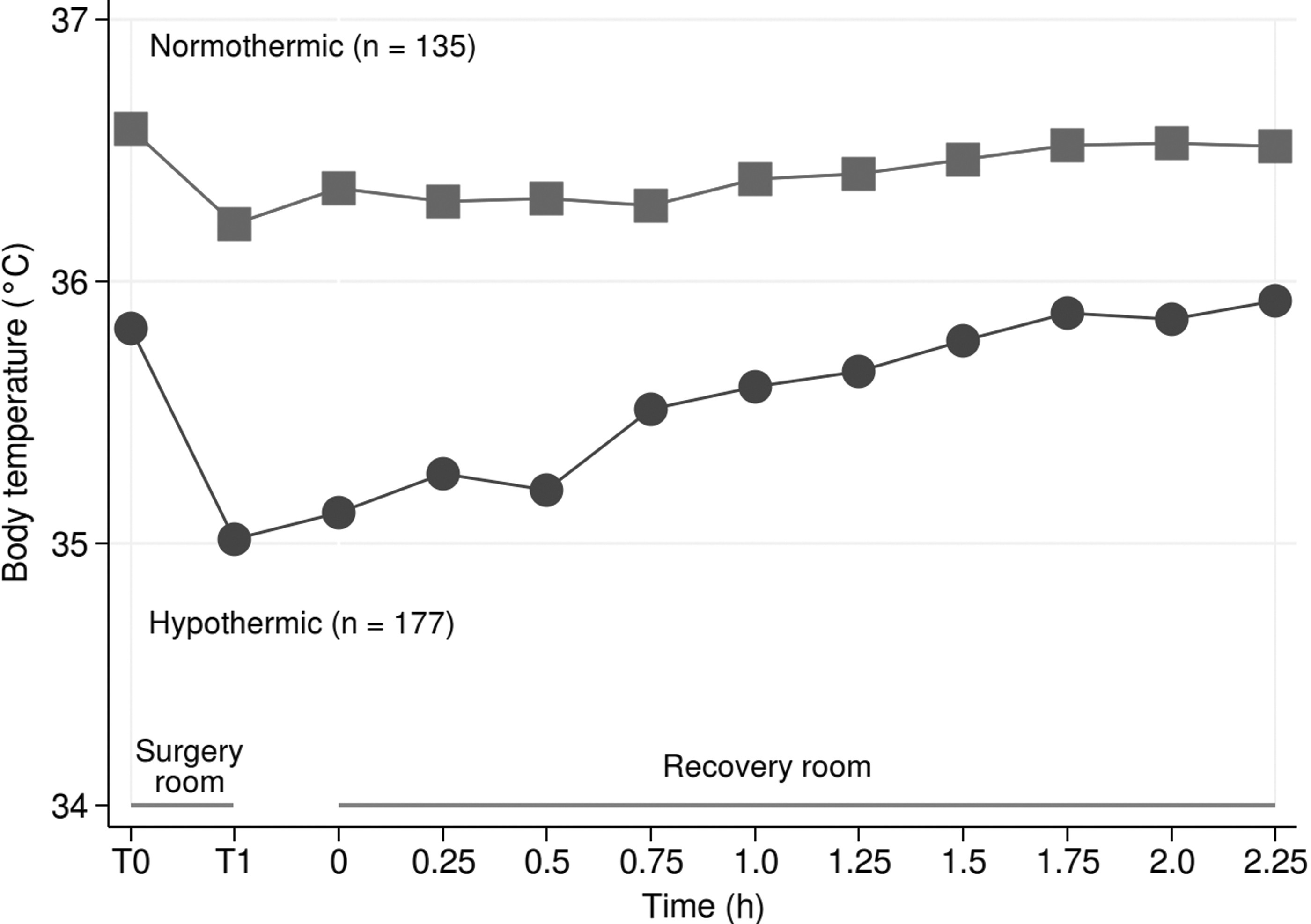
Body temperature trajectory. T0 denotes the time immediately on arrival in the operating room, whereas T1 stands for the time immediately after surgery. The length of time between T0 and T1 may vary among patients. Results are summarized as mean (95% CI). 95% CI, 95% confidence interval; PACU, postanesthesia care unit.
Hypothermia and recovery time
Patients with inadvertent hypothermia had a median hospital stay of 48 hours (IQR: 24–72 hours), which was comparable to that observed in normothermic patients: 48 hours (IQR: 24–72 hours), p = 0.24. Median postanesthetic recovery time was also similar between hypothermic and normothermic patients: 105 minutes (IQR: 75–120) versus 90 minutes (IQR: 75–120), respectively, p = 0.28.
Predictors for hypothermia: sociodemographic and clinical characteristics
Diabetic patients displayed smaller odds of having hypothermia compared to nondiabetic patients (OR = 0.48, 95% CI 0.34 to 0.69, p < 0.001). SBP levels were inverse (OR = 0.99, 95% CI 0.98 to 0.99, p < 0.001). No association was observed with heart rate (OR = 1.00, 95% CI 0.97 to 1.03, p = 0.90) or SpO2 levels (OR = 1.33, 95% CI 0.89 to 1.98, p = 0.16).
Predictors for hypothermia: anesthesia- and surgery-related variables
When considered individually, general anesthesia was significantly associated with reduced odds of hypothermia (Table 1). Perioperative chills (shivering) were significantly associated with the odds of hypothermia, but there is large uncertainty in that estimate (OR = 27.3, 95% CI 1.49 to 500.5, p = 0.026).
Opioid-based anesthesia is not a reliable predictor for hypothermia, but fentanyl was associated with marginally significant reduced odds of hypothermia (Table 1).
The odds of hypothermia increased with the duration of the surgery, especially in surgeries lasting between 31 and 120 minutes. However, no evidence of an increased risk of hypothermia was seen in surgeries that exceed two or more hours in duration (Table 1).
Predictors of hypothermia: active warming systems during the surgery
Neither availability of a heated air system in the operating room nor availability of warmed intravenous infusions was significantly associated with lower odds for hypothermia. Besides, no effect of thermal warming mattresses was observed.
Multivariable model for prediction of hypothermia
Ten variables were included in the prediction model of hypothermia (full model: ASA status, medical specialty, regional anesthesia, general anesthesia, diabetes, SBP, patient's temperature on the arrival in the operating room, perioperative shivering, fentanyl, and surgery time). In a multivariable logistic regression model, five variables remained significant predictors of abnormally low body temperature after surgery: surgical specialty (p < 0.001), diabetes (p < 0.001), fentanyl usage (p = 0.002), surgery time (p < 0.001), and patients' temperature on arrival in the operating room (p < 0.001). The average AUROC was 79.0% (95% CI 68 to 80) (Fig. 3). A simplified model, including only the five variables that remained statistically significant, provided a comparable diagnostic accuracy: AUROC was 80.6% (95% CI 72.3 to 83.4).
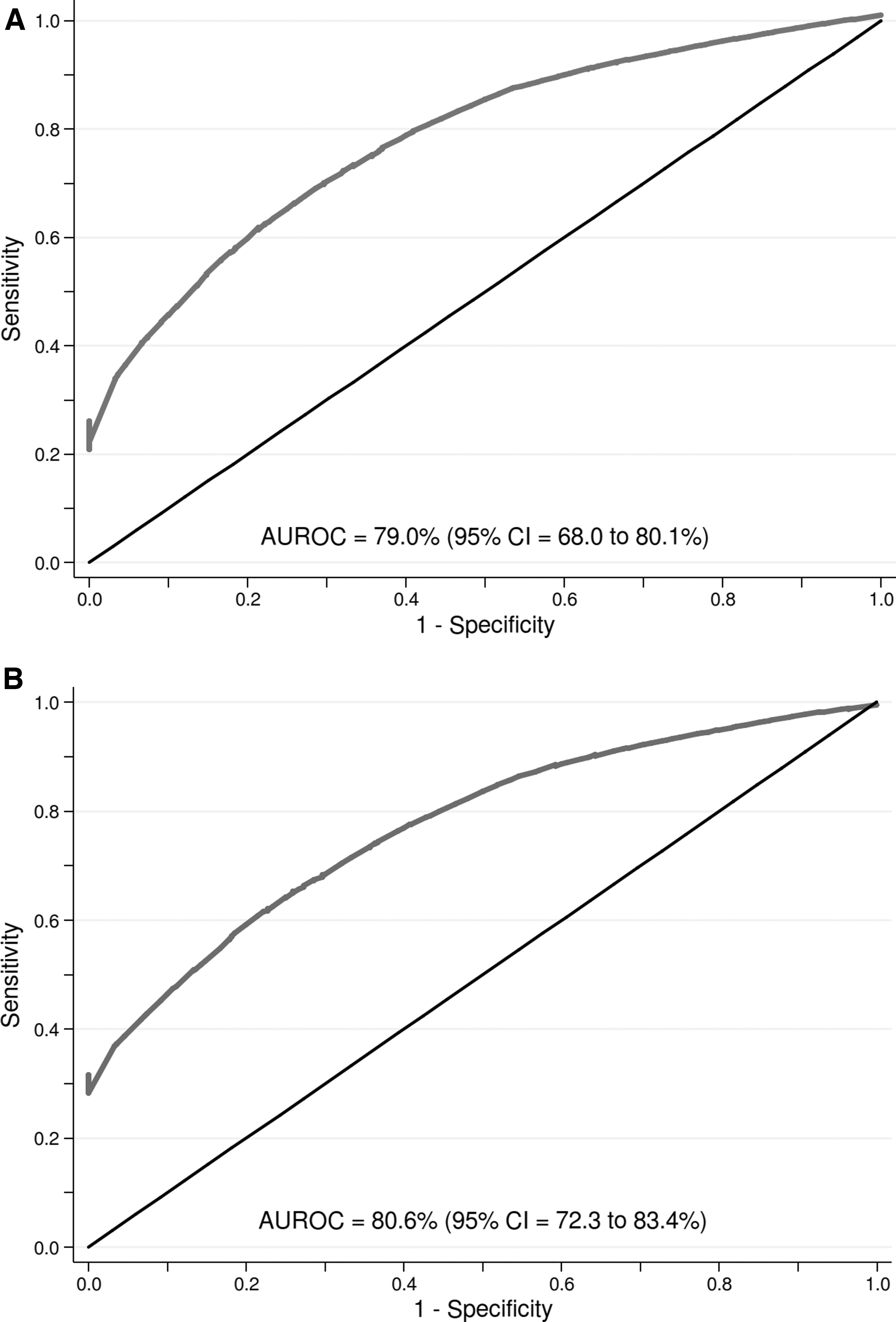
AUROC curve (n = 312 patients).
Discussion
Main findings
In this study, we identified that the overall prevalence of inadvertent hypothermia in our population was 56.7%. The present data indicate that, although the availability of new technologies for prevention of postsurgery hypothermia has grown over time, the proportion of patients with abnormally low body temperature on arrival in the recovery room remains high.
Based on our study, all identified risk factors for hypothermia were preventable, easily anticipated or readily managed clinically. Patients who developed inadvertent hypothermia were more likely to be from medical specializations such as urology or obstetrics and have lower body temperature and oxygen saturation levels at the entrance to the operating room compared to their normothermic counterparts. Active warming systems during the surgery were associated with a lower risk of hypothermia, but these associations became less significant in multivariable models that adjusted for other covariates. These observations, thus, indicate a complex interplay between clinical, sociodemographic, surgery- related, and active external rewarming systems-related variables.
Comparison with previous studies
When assessing the association between postsurgery temperature and outcomes, previous studies found that hypothermic individuals show significantly increased discomfort and dissatisfaction, higher rates of shivering, postoperative nausea and vomit, pain compared to normothermic individuals (Sessler, 2001; Sajid et al., 2009; Nalivaiko, 2018; Jun et al., 2019). However, unlike previous reports (Kurz et al., 1996; Lenhardt et al., 1997), we did not detect an association between the development of perioperative hypothermia and prolonged postoperative recovery times or increased length of hospital stay. In our cohort, most hypothermic patients achieved adequate body temperature within 2 hours in the recovery room and were discharged, on average, within the same period compared to normothermic individuals. This may have been the effect of the pilot study carried out previously (Mendonça et al., 2019). Despite the absence of a protocol, the team was attentive to the diagnostic and treatment of hypothermia, which may have accelerated the recovery of these patients.
Our results also suggest that patients who received remifentanil or fentanyl were at the lowest risk of hypothermia, whereas those who received sufentanil are at the highest. These results are in line with experimental studies indicating that some opioids drugs, such as alfentanil and fentanyl, are capable of suppressing shivering and enhancing adipose tissue thermogenesis via mu-opioid receptor activation (Cao and Morrison, 2005). The higher rates of inadvertent hypothermia among patients who received sufentanil compared to other anesthetic opioids are also in full agreement with our previous pilot investigations.
Limitations
There were important limitations to our study. First, our analysis was restricted to two public hospitals. As a result, our findings are not necessarily generalizable to other centers, particularly those in high-resource settings. Second, despite the adequate sample size to estimate the population prevalence of hypothermia with sufficient precision, our study revealed important hospital-level effects. As a result, our estimates were prone to type II errors (i.e., false-negative results) due to the higher than anticipated between-hospital heterogeneity. In addition, site-level confounders could not be fully adjusted for in the analyses. Third, our analysis was based on cross-sectional evaluations, and, therefore, we were unable to identify whether patients who developed hypothermia were associated with worse long-term outcomes compared to normothermic patients. This is a relevant topic for future research, especially in public health care settings like ours.
Interpretation
Our analyses also corroborate the view that a relatively simple model may provide good discrimination for detecting patients who will develop inadvertent hypothermia, which may help perioperative hypothermia prevention practices. Given that the tested predictors are neither invasive nor expensive, the implementation and further development of models like ours may represent a first step toward the routine use of clinical scores for predicting which patients are likely to develop abnormally low body temperature after surgery. By holding the potential to reduce short- and long-term hypothermia-related complications, these predictive models may allow for more efficient use of health care resources, and mitigating health care costs.
Conclusion
Approximately 6 in 10 patients undergoing surgery developed inadvertent perioperative hypothermia, thus illustrating that this represents a challenge to be overcome. Our study indicates that the risk of hypothermia is influenced by a myriad of factors that can be used in simple and low-cost predictive models with adequate discriminatory power.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.