
Abstract
Background:
Ultrasonography (US) changes have been noted in patients with autoimmune thyroiditis (AT). Here, we report that some patients with late stage AT have a distinctive, previously unreported finding on US that we call the “hypoechoic triangle sign” (HET).
Methods:
On US, the HET sign was characterized as a well-defined area of low echogenicity, about 10 mm in diameter, between the lateral margin of one or both thyroid lobes, the medial wall of the carotid artery, and, posteriorly, the prevertebral muscles. Twenty-six patients with AT who had the HET sign (Group 1) were compared with 71 patients with AT who had normal serum thyrotropin (TSH) and free thyroid hormones levels (Group 2) and with 154 normal controls (Group 3). TSH was tested at least twice, first as part of their regular clinical care and then in follow-up. The groups were similar in terms of age, sex, and body mass index. Thyroid volume by US, TSH, free triiodothyronine, free thyroxine, antithyroid antibodies, and
Results:
Thyroid volume was significantly smaller (p < 0.01) in Group 1 than in Groups 2 and 3 (6.9 ± 2.18 vs. 10.4 ± 2.1 and 9.8 ± 2.5 mL, respectively). In Group 1, 61.5% of subjects were taking
Conclusions:
The HET sign seems to be specific for overt thyroid failure in patients with AT as it was not noted in patients with AT not having overt thyroid failure. The incidental finding of the HET sign during cervical US examination should prompt obtaining thyroid function tests to rule out hypothyroidism. Our study provides data regarding specificity but not sensitivity of the HET sign for AT and thyroid failure because a consecutive group of AT patients with thyroid failure was not studied. In addition, the specificity of the HET sign for AT needs to be evaluated further by studying a diverse group of thyroid diseases.
Introduction
The diagnosis of AT is usually based on laboratory tests and, less frequently, on symptoms or signs (2,3). However, in recent years, an increasing number of patients are incidentally diagnosed with AT during color-Doppler carotid artery examination or neck ultrasonography (US) for thyroid nodules or goiter (5). The diagnostic role of US is especially important in a small but not negligible number of AT patients who have negative serum tests for antibodies directed against thyroid gland (6,7).
The hallmark of AT is thyroid echogenicity that is lower than that of healthy subjects (8). Thyroid echogenicity has traditionally been evaluated subjectively, by comparison of the echogenicity of the thyroid gland with that of the anterior neck muscles (8). Computerized gray-scale sonography helps to reduce the subjective component of the evaluation, allowing a more reproducible quantitative determination of thyroid echogenicity (9 –12). However, in some cases, thyroid echogenicity may be difficult to appreciate and a routine quantitative assessment of the severity of hypoechogenicity is difficult. In advanced form of AT, hypoechoic areas are mixed with hyperechoic zones due to fibrosis, and the overall echogenicity of the gland may appear ill defined.
In our experience, US in some patients with advanced AT may show a unilateral or bilateral distinct hypoechoic zone located in the neck between the carotid artery and one or both lobes of the thyroid gland (Figs. 1 and 2). This we have been referring to as the “hypoechoic triangle (HET) sign.” The present study was performed to determine the prevalence of hypothyroidism in patients with the HET sign and AT and the prevalence of the HET sign in patients with AT who were euthyroid or did not have overt hypothyroidism.
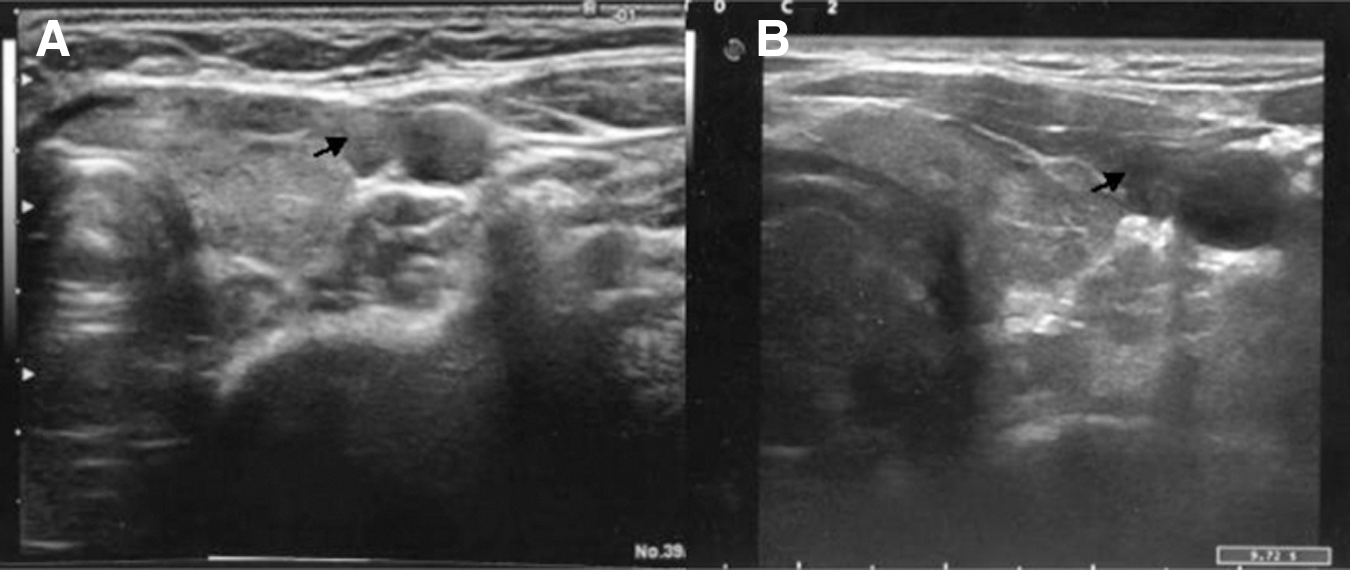
B-mode pictures of the cross section of the neck: a well-defined elongated hypoechoic area is positioned along the posterior and medial margin of the thyroid gland. (See arrows)
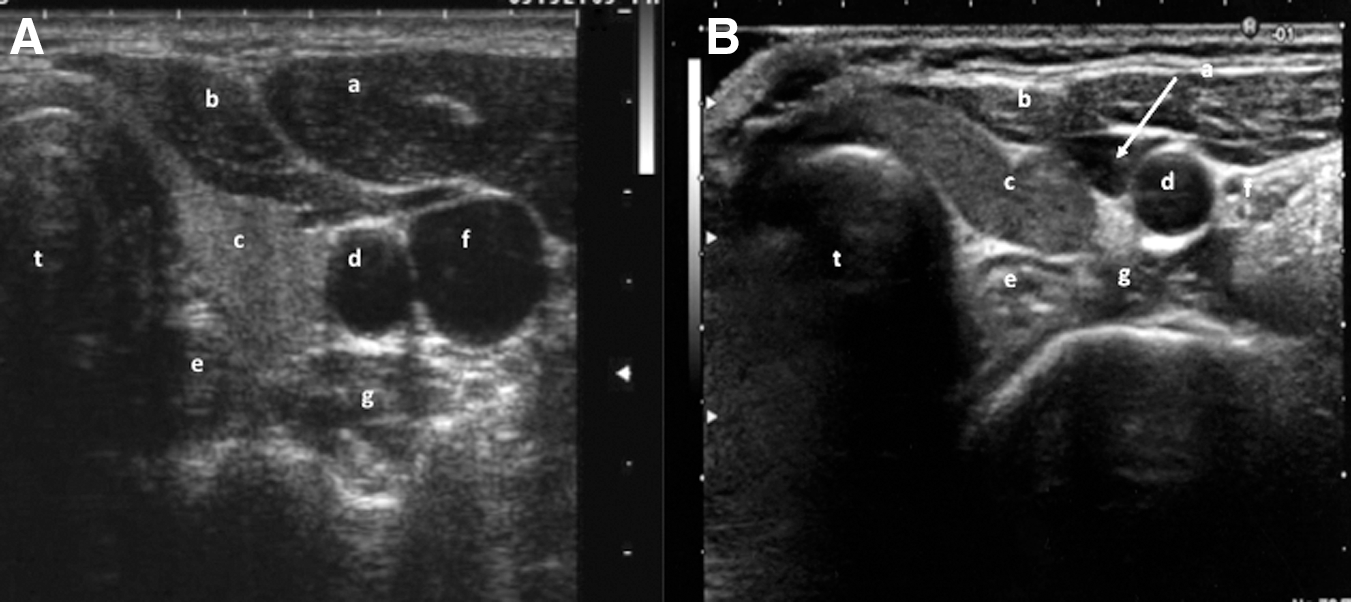
Indications of the major cervical structures that limit the hypoechoic triangle sign on a B-mode cross section of the neck.
Patients and Methods
From January 2008 to December 2008, we (A.L.P. and A.P.) observed, among the patients referred to the outpatient thyroid and dermatology clinics of our institutions, 26 patients with AT (22 women and 4 men; age: 44.5 ± 12.9 years) who had the HET sign. The sonographic finding that was defined as the HET sign was as a well-defined area of very low echogenicity, about 10 mm in diameter, located between the lateral margin of one or both lobes of the thyroid gland, the medial wall of the adjacent carotid artery, and, posteriorly, the prevertebral muscles (Fig. 1). These patients who had the HET sign, which had been noted as part of their regular clinical care, were assigned to Group 1. During the first 3 months of 2009, we consecutively examined 71 patients with AT who were not taking thyroid hormone and who had a record of normal values for serum thyrotropin (TSH) and free thyroid hormones. These patients were assigned to Group 2. During the formal study period, the TSH assay was repeated. Nine of 71 patients (12.6%) in Group 2 had borderline high TSH (>3 and <6 mIU/L) but normal serum free triiodothyronine (FT3) and free thyroxine (FT4) values. Group 3 consisted of 154 normal subjects, meeting certain exclusion criteria. Exclusion criteria were a history of thyroid disease, age less than 20 or greater than 70, or body mass index that was less than 20 or greater than 30. The three groups were similar with respect to age, sex, and body mass index and they all resided in mildly iodine-deficient area (13,14) with a median urinary iodine excretion of 94 mcg/day (Table 1).
Data are expressed as mean ± standard deviation.
Nine of the 71 patients (12.7%) in Group 2 had a borderline elevation of serum TSH in a single occasion, which was not confirmed in a successive test.
BMI, body mass index; ns, nonsignificant.
A further neck US examination was separately performed by two experienced sonographers (F.M.S. and G.B.), using a commercially available real-time scanner (MyLab 70; Esaote, Genoa, Italy) equipped with a 13–18 MHz linear transducer. Sonographic examination included multiple longitudinal and transverse scanning performed while the patient lay supine with the head slightly hyperextended. In each patient, thyroid volume was calculated using the ellipsoid formula for volume (width × length × thickness × p/6) as previously described (15). The echogenicity level of thyroid gland was compared with the echogenicity of prethyroid muscles (sternohyoid and sternothyroid) and scored as normoechoic, hypoechoic, or markedly hypoechoic. Patients gave written informed consent to use their clinical data for research purposes and institutional approval was obtained from IRCCS Ospitale Dermosifilopatico of Santa Maria and San Gallicano. Three randomly selected patients from Group 1 had a three-dimensional (3D) US reconstruction of the area of HET sign to achieve a coronal image of the neck (Fig. 3). 3D sonographic reconstruction was performed by means of the Maylab 70 software (Esaote). Color- and power-Doppler evaluation of the hypoechoic zone was performed to demonstrate the presence of vascular signals. A gray-scale examination was performed by means of the GIMP 2.4.7 software; the analysis of the distribution of gray scales was carried out on the hypoechoic triangle zone and the surrounding adipose and muscle tissues (Fig. 4).
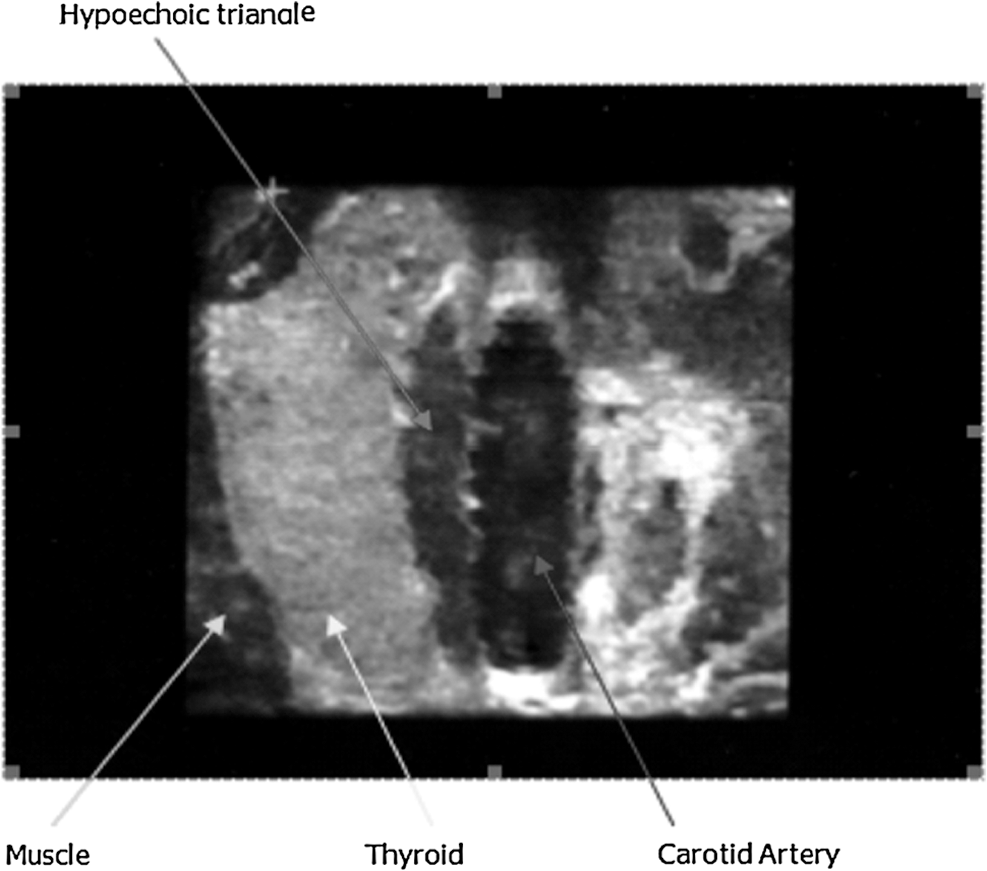
A three-dimensional ultrasound reconstruction of one randomized selected patient from Group 1 with hypoechoic triangle sign. This is a coronal image of the neck. Three-dimensional ultrasonography demonstrated a well-defined craniocaudal elongated hypoechoic area positioned along the posterior and medial margin of the thyroid gland.
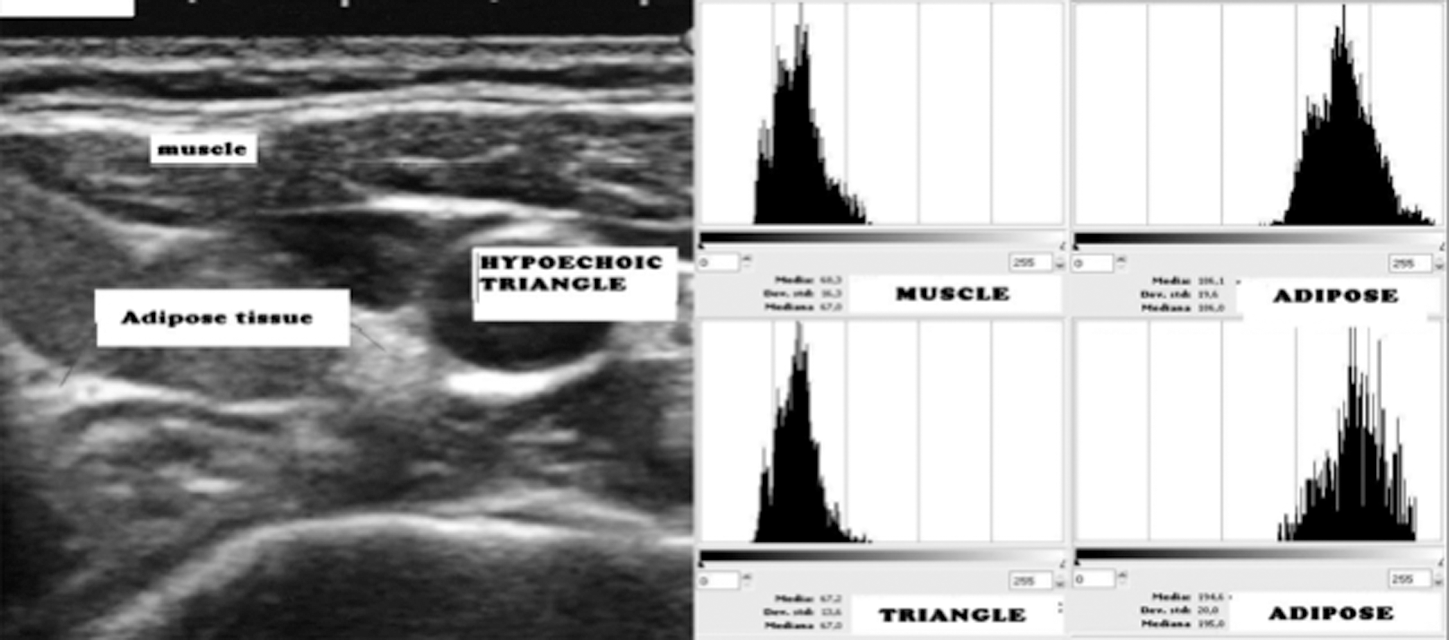
Gray-scale evaluation demonstrates a near complete overlap between the hypoechoic triangle zone and the muscle tissue while a clear difference was present between the hypoechoic triangle and the adipose tissue.
Serum levels of TSH (normal range: 0.2–4.0 mcIU/mL), FT3 (normal range: 2.2–5.0 pg/mL), FT4 (normal range: 8.0–18.5 pg/mL), antithyroglobulin antibodies (TgAb, normal range: 0.0–70.0 IU/mL), and antithyroid peroxidase antibodies (TPOAb, normal range: 0.0–70.0 IU/mL) were determined with commercially available chemiluminescent assay kits (Radim, Pomezia, Italy).
The diagnosis of AT was based on the presence of positive tests for antithyroid antibodies, whether or not there were US features consistent with autoimmune thyroid disease (5). The US pattern considered consistent with AT was diffuse hypoechogenicity and hypervascularization and a fine inhomogeneous pattern. Patients were classified as euthyroid if their serum TSH, FT3, and FT4 were normal or having subclinical hypothyroidism if their serum TSH was mildly elevated (4–10 mcIU/mL) and their serum FT3 and FT4 levels were normal. They were considered to be clinically hypothyroid if their serum TSH was elevated and their serum FT4 was subnormal.
Statistical analysis
Data collection and statistical evaluation were blindly performed by R.G., I.M., and L.P. Data are expressed as mean ± standard deviation. χ 2 analyses was used for categorical variables and the Student's t-test was used for continuous variables in the univariate analyses. Linear regression was used within the same group to assess a possible correlation between continuous variables. The statistical package used was SPSS (version 12.0; Chicago, IL) and p < 0.05 was accepted as significant.
Results
A second US examination was performed in all patients. The presence of the HET sign was confirmed in all Group 1 patients. In most patients, the HET sign was present on one side only (46.0% patients on the right and 54.0% patients on the left). In three patients (11.5%), the HET sign was bilateral. The greatest diameter of the HET ranged from 8 to 15 mm (median: 12 mm). Seventeen of the 26 patients in Group 1 (65.4%) were taking thyroid hormone as
The patients enrolled in Group 2 originally had a US examination because their antithyroid antibody tests were positive. In all cases, except one, the repeat US examination had a pattern consistent with AT. No patient in Group 2 had the HET sign on either the original or repeat US examination. At enrollment, 9 of the 71 patients (12.7%) in Group 2 had a borderline elevation of serum TSH. All of the remaining patients were euthyroid. No patient in Group 3 had an HET sign or US features suggestive of AT on US examination. Consistent with the selection criteria for Group 3, all subjects in this group were euthyroid and did not have positive serum antithyroid antibodies.
TSH values were significantly higher (p < 0.01) in Group 1 than in Groups 2 and 3 (3.6 ± 1.3 vs. 2.18 ± 1.4 and 1.9 ± 1.1 mIU/L, respectively), even though 65.4% of Group 1 subjects were taking
No correlation was found between TSH level and thyroid volume in Group 1 (r 2 = 0.01) and in Group 2 (r 2 = 0.02), whereas there was a weak but significant correlation in Group 3 (p = 0.04, r 2 = 0.03). The prevalence of severe hypoechoic patterns was significantly higher (p < 0.001) in Group 1 (21/26; 80.8%) than in Group 2 (9/71; 13%) and Group 3 (10/154; 6%).
Color- and power-Doppler evaluation failed to demonstrate the presence of vascular images in the area of the HET sign in Group 1 patients.
In three patients in Group 1, 3D US demonstrated a well-defined hypoechoic area, extended craniocaudally in the neck, and placed along the posterior and lateral margin of one of the lobes of the thyroid gland (Fig. 3). Gray-scale evaluation demonstrated an incomplete overlap between the hypoechoic triangle zone and the surrounding muscle tissue, with intermediate values between muscle and fat.
Discussion
An increasing number of patients with AT are diagnosed on the basis of incidental US findings obtained using either color-Doppler for carotid artery examination or neck US for evaluation of palpable thyroid nodules or goiters. Reduced thyroid echogenicity on US evaluation of the thyroid gland in AT patients is a strong predictor of hypothyroidism (6,7,16 –18). Patients with a recent diagnosis of AT are likely to be different from patients with a protracted history of AT not only in terms of the rate and severity of hypothyroidism but also for their degree of hypoechogenicity and inhomogeneous sonographic pattern.
It has been proposed that computerized gray-scale sonography gives quantitative determination of thyroid echogenicity (19 –21) and mean tissue density and is therefore used as a quantitative parameter of echogenicity. Quantitative echogenicity assessment is a useful tool but is time consuming and not widely used. Moreover, in the end stage of AT, mean tissue density assessment may be misleading because the US image is due to a combination of the hyperechoic and hypoechoic signals present in the zone selected for examination.
We now describe a new US finding, the HET sign, which can be easily detected. In the present series of cases, the HET sign was usually associated with overt hypothyroidism or subclinical hypothyroidism. Importantly, in our series, no euthyroid patient with AT had the HET sign. In most cases, the HET sign was present on one side of the neck only.
On the basis of color-Doppler, 3D US examination, and gray-scale examination, the area where the HET sign is seen seems to be secondary to the formation of a free space interposed among the neck structures and filled with fibrous and muscle tissue. This anatomic change in the neck structures could be the consequence of thyroid gland fibrosis and the subsequent shrinkage of thyroid parenchyma.
It is important to note that our study design provides data regarding the specificity of the HET sign for thyroid failure in AT but not the sensitivity of the HET sign for thyroid failure in AT. This is because we did not study a consecutive group of patients with AT and thyroid failure to see what percentage had the HET sign. Even the overall specificity of the HET sign for AT is not known as there needs to be a study of a host of diseases to see if it occurs in them.
In conclusion, if a sonographic evaluation of the neck, performed for thyroid disease or other clinical reasons, shows a combination of small thyroid volume and the HET sign, there should be prompt evaluation for concomitant hypothyroidism. This information could be clinically relevant in subjects with conditions that could be adversely influenced by a previously unidentified hypothyroidism, such as pregnant women and patients with cardiovascular disease or severe dyslipidemia. In patients with AT, the US finding of the HET sign is suggestive for clinically significant hypothyroidism. Further controlled studies on a large number of patients affected by AT are needed to confirm this preliminary observation, to define the sensitivity of the HET sign for thyroid failure in AT, and to find out whether the HET sign is seen in patients with other forms of thyroid disease.
Footnotes
Disclosure Statement
The authors declare that no competing financial interest exists.