
Abstract
Background:
Calcitonin and carcinoembryonic antigen (CEA) are established markers of medullary thyroid cancer (MTC), used in the diagnosis and monitoring of disease and its progression. In clinical practice, various other tumor markers are utilized in the follow-up of different malignancies, although their utility has not been well described in MTC. CA 19-9 antigen, routinely used in the monitoring of pancreatic cancer, also has been detected in the tissue of approximately 6% of MTCs. However, its presence has never been reported in the serum of these patients. Elevation of CA 125 antigen, utilized as a tumor marker for ovarian cancer, has never been reported in MTC. We report a novel finding of metastatic MTC presenting with elevated CA 19-9 and CA 125 serum levels, with concurrent tissue staining for these antigens.
Summary:
A 56-year-old woman with multiple endocrine neoplasia 2B syndrome, post subtotal thyroidectomy for MTC in childhood, presented with extensive metastatic spread of MTC to the lungs and liver, 47 years after the original diagnosis. The patient's calcitonin level decreased from 2950 to 261 pg/mL (reference range: <20 pg/mL) over a 20-year period. The serum CEA level was elevated at 6800 ng/mL (reference range: <5.1 ng/mL). Because of a concern for an alternate malignancy, serum CA 19-9 and CA 125 tumor markers were measured and found to be significantly elevated, at 39,334 U/mL (reference range: <35.1 U/mL) and 96.2 U/mL (reference range: 7–41 U/mL), respectively. Immunostaining of the metastatic MTC tissue showed patchy staining for calcitonin, strongly positive staining for CEA and CA 19-9, and weakly positive staining for CA 125.
Conclusion:
Drawing from experience with CA 19-9 and CA 125 tumor markers in other malignancies, we propose that they may be associated with aggressive forms of MTC with significant metastatic potential.
Introduction
Patient Report
A 56-year-old woman presented with progressive dyspnea of a few weeks duration. At age 9, the patient was noted to have a thyroid mass and underwent a subtotal thyroidectomy. The initial pathological diagnosis was a benign thyroid lesion. Subsequently, multiple endocrine neoplasia 2B (MEN 2B) syndrome was described in the literature. This prompted reexamination of the original thyroid specimen, given the patient's classical facial features of MEN 2B. Upon reexamination of the specimen, a diagnosis of MTC and MEN 2B syndrome was made. At the time, the family and the patient decided not to complete the thyroidectomy. At age 35 the patient presented with malignant hypertension and was diagnosed with bilateral pheochromocytoma and megacolon. She underwent a bilateral adrenalectomy and partial colectomy. Her condition remained stable for a number of years, but she declined further medical or genetic evaluation. Her medications included levothyroxine 0.125 mg daily, fludrocortisone 0.1 mg daily, and hydrocortisone 20 mg in the morning and 10 mg in the evening. The patient had no known family history of MEN 2B.
On the current presentation to the hospital, the patient was found to be mildly hypotensive with BP 106/72, tachycardic with a pulse of 104, tachypneic with RR 40, and hypoxic, SpO2 86% on room air. Her physical examination was also significant for a long thin face, high arched palate, and widely spaced teeth. She had neuromas of the tongue, lips, and buccal mucosa. There was no palpable thyroid, lymphadenopathy, or neck masses. Her lung examination was normal. Her abdomen was distended and nontender, with hyperactive bowel sounds. There were no palpable abdominal masses. Review of her laboratory tests revealed that her serum calcitonin levels (Siemens Immulite 2000; Euro/DPC Ltd.) had progressively declined over a course of 20 years from 2950 to 261 pg/mL (reference range: <6 pg/mL) (Fig. 1). The serum CEA (Siemens Immulite 2000; Euro/DPC Ltd.) had increased from 21 to 6800 ng/mL (reference range: <5.1 ng/mL) over a period of 10 years (Fig. 1). Magnetic resonance imaging of the abdomen showed a right hepatic lobe with heterogeneous parenchyma, suggestive of an infiltrative process or metastases (Fig. 2A). These findings had not been present on a CT performed 1 year prior (Fig. 2B). Serum CA 19-9 (Beckman Access-2; Beckman Coulter, Inc.) and CA 125 (Siemens Immulite 2000; Euro/DPC Ltd.) were measured to evaluate the possibility of another malignancy and were 39,334 U/mL (reference range: <35.1 U/mL) and 96.2 U/mL (reference range: 7–41 U/mL), respectively. The plasma metanephrine was <25 pg/mL (reference range: <58 pg/mL) and plasma normetanephrine 427 pg/mL (reference range: <149 pg/mL), consistent with a history of bilateral adrenalectomy in a stressed patient. Genetic testing was performed and confirmed a diagnosis of MEN 2B syndrome, with a mutation localized to codon 918 (c.2753T>C) in the REarranged during Transcription (RET) proto-oncogene. The patient's family members declined genetic testing.
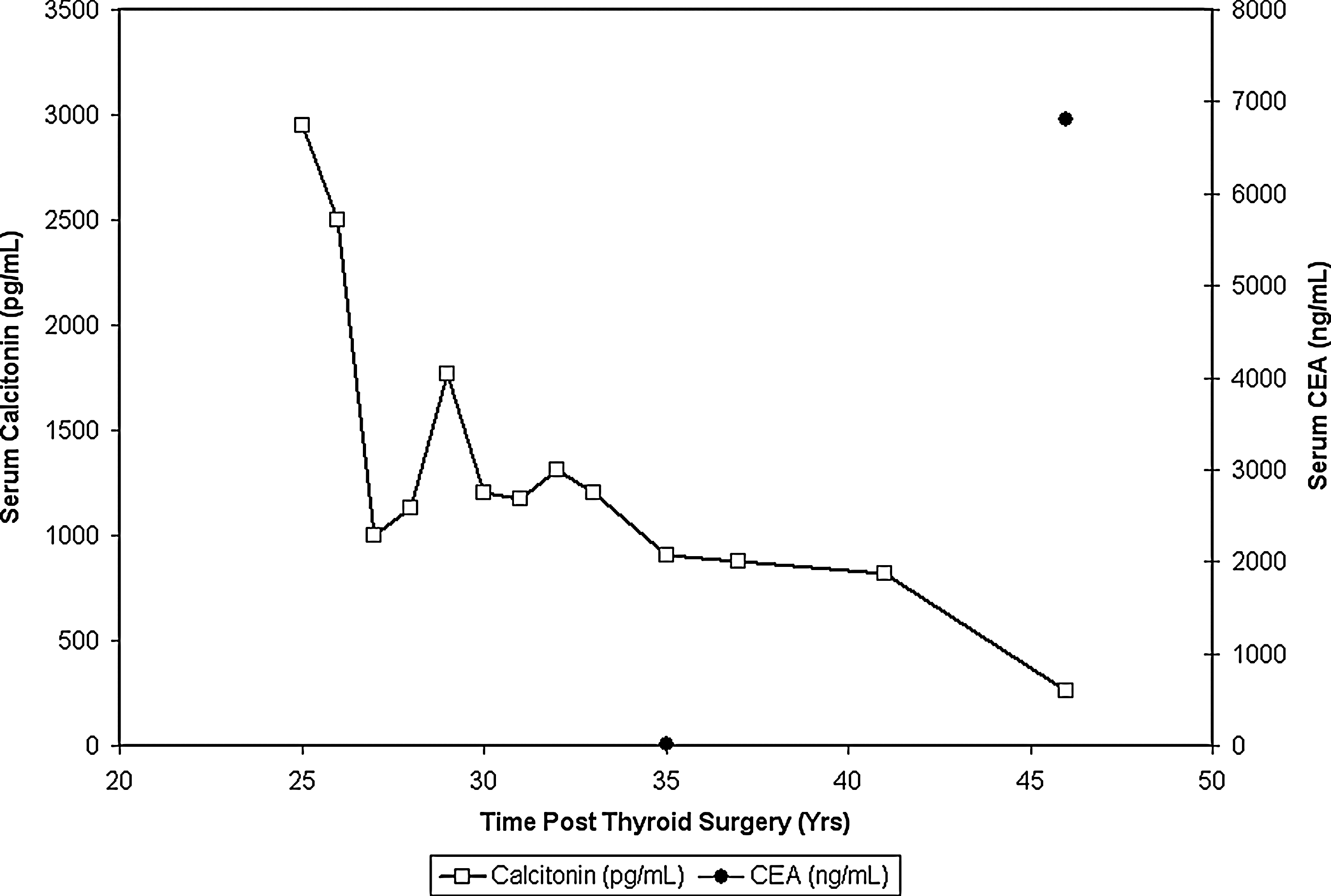
Patient's calcitonin and CEA levels. CEA, carcinoembryonic antigen.
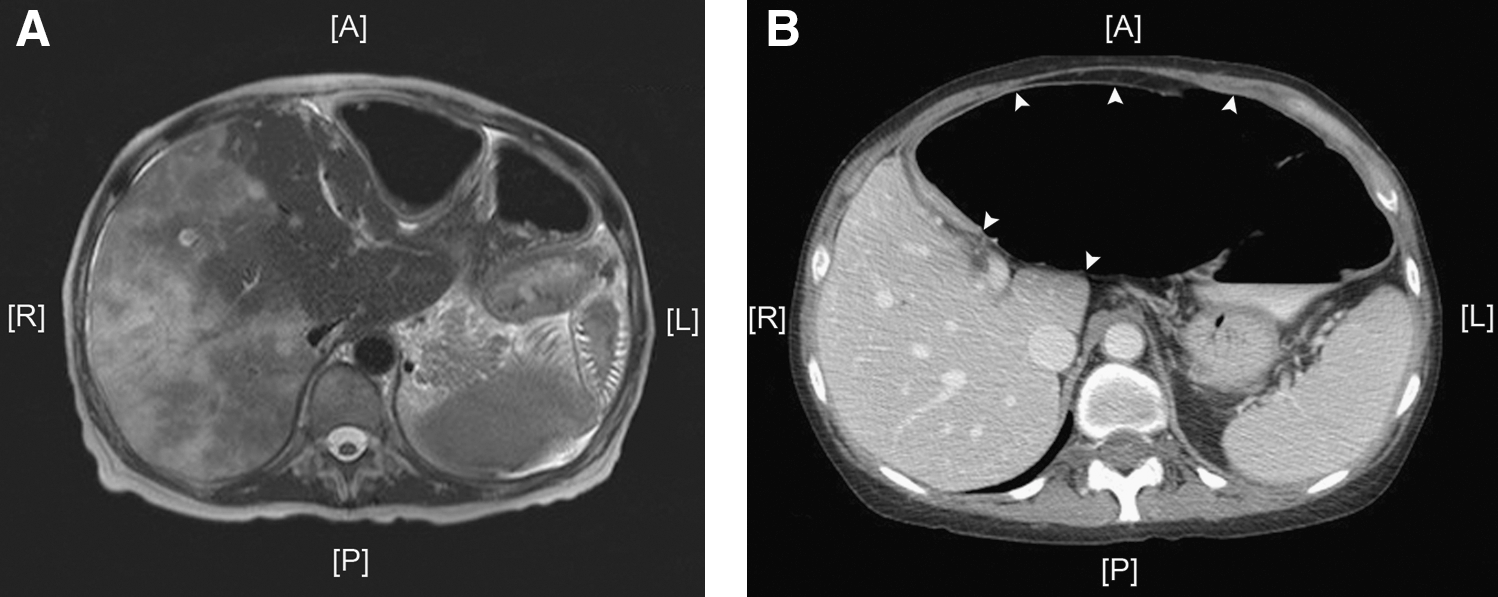
Abdominal imaging.
The patient's condition deteriorated and she expired. An autopsy was performed, which revealed metastatic carcinoma involving the lungs and liver. Atrophic thyroid tissue, without evidence of MTC, was present. The tumor was submitted for histopathologic evaluation.
Five-micrometer-thick sections of formalin-fixed paraffin-embedded tissue were stained with hematoxylin and eosin. The slides for immunohistochemical analysis, utilizing the antibodies described by the following paragraph, were stained with an automatic slide stainer (Dako LV-1 Autostainer/Dako universal staining system) for 30 minutes at room temperature followed by the secondary antibody. 3,3′-Diaminobenzidine was used as the chromogen. The slides were counterstained with hematoxylin. Appropriate negative controls were included.
The hematoxylin and eosin–stained slides demonstrated a malignant population of uniform, polygonal- to spindle-shaped cells with finely granular eosinophilic cytoplasm and central nuclei, identified in metastatic foci in the liver and lung, compatible with metastatic MTC (Fig. 3A). Immunohistochemical staining for calcitonin (Dako Denmark) showed patchy positively stained tumor cells (Fig. 3B) and neuroendocrine markers (chromogranin and synaptophysin; Dako Denmark) were positive (Fig. 3C, D), confirming the diagnosis of MTC. The immunostaining of the MTC was diffusely strong for CEA (Dako Denmark) and rare focally positive cell staining was demonstrated for CA 125 (Novocastra Laboratories Ltd.) (Fig. 3E, F). Diffuse strong staining was identified with CA 19-9 (Dako North America, Inc.) (Fig. 3G).

Histopathology and immunostaining of medullary thyroid cancer hepatic metastases.
Discussion
MTC is a rare malignancy accounting for 4% of all thyroid carcinomas in the United States (5). It originates from the calcitonin-secreting parafollicular C cells of the thyroid gland and was first histopathologically described in 1959 (6). About 25% of MTCs are attributed to autosomal dominant inheritance and include familial MTC and MEN 2A and MEN 2B syndromes (7,8). Our patient was not initially recognized to have MTC, likely because it was a newly described entity at the time. MTC resulting from a germline mutation in the RET 918 codon, as in this patient, can develop in those as young as 9 months of age, and most hereditary MTCs have a tendency to metastasize early in the course of disease (9). Despite early metastases, the disease may remain dormant for many years and patients may experience prolonged survival (8,10). The fact that the patient did not have a family history of MEN 2B is not unusual either, as about 50% of mutations in the RET proto-oncogene resulting in MEN 2B are attributed to de novo germline mutations on the paternal allele (11).
Calcitonin and CEA tumor markers have a well-established role in monitoring the progression of MTC (1,2,12). An inverse relationship has been reported between calcitonin and CEA expression in some metastatic MTCs (3). In these tumors, as the cancer metastasized, cellular calcitonin declined and CEA increased. In the current case, calcitonin levels declined over a 20-year period as the CEA level rose, while the MTC aggressively metastasized. This may represent dedifferentiation of MTC, with CEA being a marker of early epithelial differentiation and calcitonin a marker of later terminal epithelial differentiation (3).
The “hook effect” in calcitonin immunometric assay should also be considered when the calcitonin levels measure lower than would be predicted based on the MTC burden (13). Although we did not confirm the calcitonin levels with a different assay or serial serum dilutions in order to rule out the “hook effect,” our findings of declining calcitonin levels are unlikely to be due to this phenomenon. Our results are confirmed by the presence of only a small number of cells in the metastatic MTC that stained positive for calcitonin by immunohistochemistry, supportive of declining serum calcitonin levels.
Weak staining for CA 19-9 has been reported in 6% of 48 MTCs previously studied (4). However, no medical history for these patients or serum CA 19-9 levels were reported by the authors, making it difficult to apply these results to clinical practice. In this case, the patient had a very elevated serum CA 19-9 level, which initially raised concern for an additional malignancy to MTC. However, the fact that the serum CA 19-9 level correlated with the immunohistochemical staining for CA 19-9 in the metastatic MTC tissue, and that no other malignancy was identified, eliminated that possibility.
CA 19-9, a carbohydrate Lewis blood group antigen, is secreted by or found on the surface of cancer cells and is detected by monoclonal antibodies. It is a nonspecific tumor marker routinely used for monitoring the response to therapy and disease progression in patients with pancreatic malignancy (14). It is important to note that patients who do not express Lewis blood group antigens routinely test negative for CA 19-9, despite the presence of malignancy. CA 125, a glycoprotein antigen, is a marker frequently used to monitor ovarian cancer progression (15). It has never been previously reported in MTC. In our case, CA 125 was detected both in the patient's serum and in tissue staining of the metastatic MTC lesion. The significance of CA 19-9 and CA 125 expression in the pathogenesis of MTC is presently unknown.
The patient we described had a stable course of MTC for over 40 years and then quickly deteriorated, as evidenced by the development of extensive hepatic metastases within a 1-year period. During this time, the calcitonin level decreased, after remaining stable for at least 15 years. Over the same period, the CEA level rose dramatically. We hypothesize that the tumor underwent a transformation late in the course of the disease, which rendered it capable of expressing CEA, CA 19-9, and CA 125, thus allowing it to grow and metastasize more aggressively. It remains to be seen whether these markers can be confirmed in other patients as predictors of very aggressive disease.
Footnotes
Acknowledgments
The authors thank Dr. Monica Smiddy for her assistance in procuring the pathological specimens and Dr. Martin I. Surks for providing the patient's historical records.
Disclosure Statement
The authors disclose that no competing financial interests exist.