
Abstract
Background:
Thyroid cancer incidence in New York State has increased rapidly in recent years, particularly in New York City and its surrounding metropolitan area. In 2007 among white non-Hispanics, incidence rates were about 40% higher in the New York City metropolitan area than in the rest of the state. Here we explore the extent to which living in neighborhoods with a high percentage of highly observant Jews may be associated with this pattern.
Methods:
We identify neighborhoods with concentrations of highly observant Jewish persons based on the use of Yiddish among children and the location of Orthodox synagogues. Thyroid cancer risk is modeled as a function of living in such a neighborhood, adjusting for age, sex, and other factors. The model was repeated for small (<2 cm) and large (≥2 cm) tumors to assess the role of diagnostic improvements in driving the spatial-temporal patterns.
Results:
A moderate association with thyroid cancer was found among those living in Jewish neighborhoods and downstate New York. A lesser association was found among those who live in neighborhoods of high levels of people born in Russia, Belarus, or Ukraine. Similar elevated rate ratios were seen for small and large tumors in Jewish neighborhoods, providing evidence against differences in diagnostic practices in this group. Smaller tumors were more pronounced among women and persons diagnosed more recently.
Conclusions:
The associations found do not seem to be diagnostically driven, but rather due to environmental, genetic, or cultural factors in the highly observant population of New York State.
Introduction
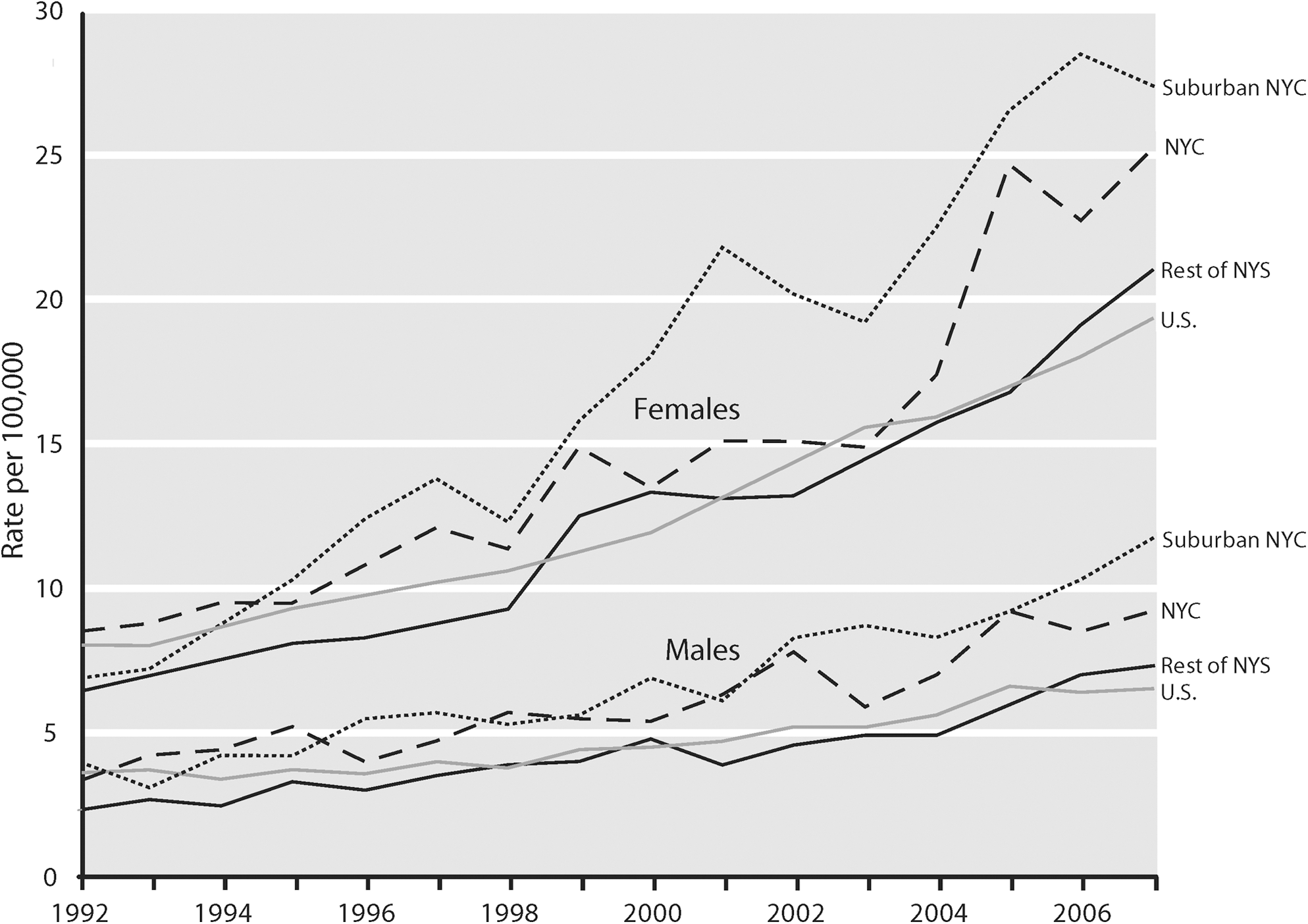
Thyroid cancer incidence rates by year of diagnosis for various regions of New York State and the United States, for males and females, age-adjusted to the U.S. 2000 standard population (7).
The geographic pattern of the data also suggests that people of Jewish descent may be at higher risk of thyroid cancer. This association has previously been suggested in a limited number of studies in the United States and Israel going back several decades (5,8 –12), though at least one study found no such association (13). One study showed a further association with radiation treatment for childhood lymphoid hyperplasia (12). These studies used survey, hospital-collected, or cemetery-derived data on religion that were characterized by large proportions of missing data and small sample sizes. Consequently, the link between Jewish ethnicity and thyroid cancer cannot be considered well established. The objective of this article is to use high-quality, population-based surveillance data to reexamine this question.
New York State is an appropriate venue for this analysis as it contains the largest concentration of highly observant Jewish persons in the United States (14). “Highly observant” encompasses Orthodox Judaism and its various subdivisions and sects, including Hasidism. This population is growing rapidly, over 50% in a 6-year period in some areas (15), with an average family size of 9–11 people (16). Two of the largest population-growth areas in New York State over the last 5 years have been in Kiryas Joel, a Satmar Hasidic community in Orange County, and New Square, a Skverer Hasidic community in Rockland County (15). These and similar sects began to move into the Lower Hudson Valley from Brooklyn beginning in the 1950s to escape the influences of urban society (17). Brooklyn remains the focal point of the highly observant Jewish community, however. There are also significant numbers of highly observant Jews in the other boroughs of New York City and the western part of Long Island (Fig. 2). These communities tend to be less affluent and less educated than their nonhighly observant neighbors in the suburbs of New York City. Kiryas Joel, for example, has the highest rate of poverty of any area over 10,000 population in the country (18,19). This can be partially attributed to large family sizes, private school tuition for children, only one parent working, and few people leaving the community to attend college or obtain high-paying jobs (19), attributes it shares with most other Hasidic communities.
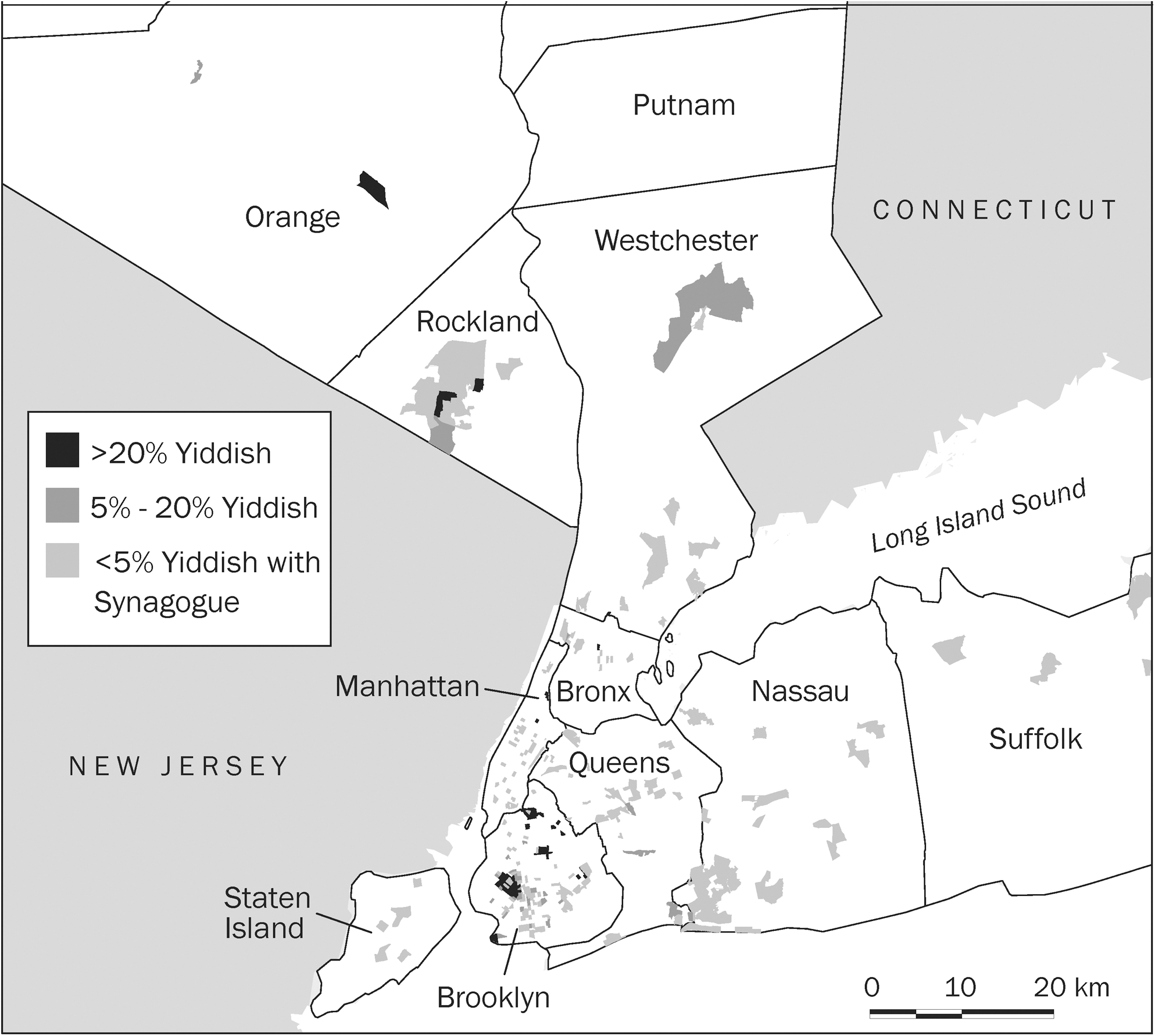
Areas with concentrations of highly observant Jewish persons in New York City and surrounding counties.
In this article we quantify the contributory role of living in a highly observant Jewish neighborhood on thyroid cancer incidence, accounting for demographic variables and tumor characteristics. We focus on the highly observant group, as opposed to Jewish persons generally, because they are easy to identify geographically by virtue of the compactness and insularity of their neighborhoods. As a more homogeneous group, both culturally and genetically than Jewish persons generally, any possible association with thyroid cancer may be easier to identify.
Materials and Methods
Study population
Incident cases of malignant thyroid cancer (SEER ICD-O-3 recode 32010) (7) diagnosed among non-Hispanic White New York State residents between 1998 and 2007 were identified from the New York State Cancer Registry (NYSCR) (n=15,367). Non-Hispanic Whites were selected as this describes nearly all Jewish persons.
Statistical analysis
A multilevel Poisson model was developed using SAS PROC GLIMMIX (SAS 9.2, Cary, NC) with cancer incidence as the outcome variable, the natural log of the population as the offset; age, sex, tumor size, time period of diagnosis, area poverty rate, residence in a highly observant Jewish neighborhood, and residence in a neighborhood with a high percentage of people born in Russia, Belarus, or Ukraine (hereafter called RBU neighborhood) as fixed effects; and region within the state (New York City, New York City suburbs, or upstate New York) as a random effect. Histology was considered, but the model was insensitive to this variable, as about 85% of the cases with known cell type are papillary and 12% follicular, with the remainder medullary or mixed types. Models stratified by tumor size were also developed to assess the contributory role of screening and incidental diagnosis from medical technology.
Independent variables
Since neither religion nor Jewish ancestry is collected by the NYSCR, highly observant communities were identified in two ways. First, the percentage of children under the age of 18 who speak Yiddish at home was obtained from Table P145I of the 2000 U.S. Census. Second, locations of Orthodox or Hasidic synagogues (shuln) were obtained from two sources: the Web site of the Chabad-Lubavitch sect of Hasidic Jews,
The RBU neighborhood variable was included to identify any independent thyroid cancer risk within this population resulting from radiation exposure from the Chernobyl nuclear reactor meltdown (20). Since birthplace information is incompletely collected by the NYSCR, Table QT-P15 of the 2000 Census was used. The 237 census tracts where at least 5% of the population were born in these countries were counted as RBU neighborhoods. Although only a proportion of the population born in Russia, Belarus, or Ukraine would have lived in areas with the highest exposure after the Chernobyl incident, the census data do not allow for a more refined definition of birthplace that would narrow in on the higher exposure areas. Census data also indicate that the majority of immigration from the former Soviet areas occurred after the Chernobyl incident, with immigration before World War II accounting for a minimal percent of residents in these neighborhoods (18).
Census-tract level poverty rate was also obtained from the 2000 census, Table P88, and grouped into four categories. A small number of census tracts consisting mainly of persons living in group quarters with no associated poverty rates were excluded from the analysis. These tracts comprised 0.1% of the population and zero thyroid cancer cases. Census-tract level education measures were also considered but excluded as they had no impact on the model outcomes.
The region variable was included to reflect the observation that thyroid cancer rates in the New York City metropolitan area are elevated generally compared to New York State, not just in highly observant neighborhoods. The suburban region was defined as six counties surrounding New York City to the east (Nassau, Suffolk) and north (Rockland, Westchester, Orange, and Putnam) (Fig. 2). The remainder of New York State comprised all counties north of Orange and Putnam. County-level cancer rates and percent Jewish populations for the counties within these regions are given in Table 1. Each of the suburban counties has elevated rates for both males and females, even those with low Jewish populations.
Taken from Religious Congregations and Membership, 2000 (21).
Taken from 2000 U.S. Census for NHW (18).
Rate is per 100,000 people, age-adjusted to the 2000 U.S. standard population.
CI, confidence interval; NHW, non-Hispanic White; NYS, New York State.
Populations for non-Hispanic Whites were obtained from the 2000 U.S. Census and 2005 population estimates published by Claritas, Inc. These were applied to the 1998–2002 and 2003–2007 time periods, respectively. All variables not otherwise described above were obtained from the NYSCR.
Results
After adjustment for demographic and tumor characteristics (Table 2), persons living in high Yiddish-speaking census tracts show a significantly elevated risk of thyroid cancer of ∼40%. Those living in tracts with Orthodox or Hasidic synagogues, but without a high proportion of Yiddish-speaking children, also show a significantly elevated risk. Most of the difference between the unadjusted and adjusted results is a consequence of age-adjustment. The age distribution of the highly observant Jewish community is much younger than that of New York State generally: 37% of the population in the census tracts where over 20% of the children speak Yiddish is under age 15, versus 17% in the referent population. The other geographic variables in the model also show significant differences in risk after adjustment. Residence in New York City, its suburbs, or an RBU neighborhood is associated with higher risk of thyroid cancer, whereas poverty rate shows an inverse association.
All variables in model fully adjusted for all other variables.
High=20% or more children under the age of 18 speak Yiddish at home; moderate=5–20% of children under the age of 18 speak Yiddish at home; synagogue only ≤5% of children under the age of 18 speak Yiddish at home and there is an Orthodox synagogue in the census tract; low/no ≤5% of children under the age of 18 speak Yiddish at home and there is no Orthodox synagogue in the census tract.
Yes=5% or more of the population in the census tract was born in RBU.
Includes Orange, Rockland, Putnam, Westchester, Nassau, and Suffolk Counties.
RBU, Russia, Belarus, or Ukraine.
Stratification by tumor size (Table 3) shows that smaller tumors are much more likely to have been diagnosed during the more recent time period and among women. There was no difference in the likelihood of detecting smaller tumors when compared to larger tumors by poverty group. Among high Yiddish-speaking census tracts and RBU neighborhoods, smaller tumors were not more likely to be diagnosed.
All variables in model fully adjusted for all other variables.
High=20% or more children under the age of 18 speak Yiddish at home; Moderate=5%–20% of children under the age of 18 speak Yiddish at home; Synagogue only ≤5% of children under the age of 18 speak Yiddish at home and there is an Orthodox synagogue in the census tract; low/no ≤5% of children under the age of 18 speak Yiddish at home and there is no Orthodox synagogue in the census tract.
Yes=5% or more of the population in the census tract was born in RBU.
Includes Orange, Rockland, Putnam, Westchester, Nassau, and Suffolk Counties.
Discussion
Our results suggest that thyroid cancer rates in highly observant Jewish neighborhoods are elevated relative to the rest of New York State, with an increased risk of about 40% (adjusted rate ratio [ARR] 1.41, 95% confidence interval [CI] 1.21–1.64) in census tracts with high levels of Yiddish spoken among children. Significantly elevated risk is also seen in census tracts containing Orthodox or Hasidic synagogues. This increased risk is not driven by a disproportionate share of smaller tumors, as would be expected if heightened screening or incidental diagnosis related to medical imaging were major contributory factors. While information on cancer screening is not collected by the NYSCR, we would not expect unusually high screening levels in these groups owing to their cultural insularity. There have been well-publicized efforts to increase thyroid examinations among emigrants from Russia, Belarus, or Ukraine who were exposed to radiation from Chernobyl (a group that also includes many highly observant Jews) (20,22,23), but this group does not show a trend toward smaller tumors either.
We also identified an elevated risk of ∼30% (ARR 1.29, 95% CI 1.04–1.59) in New York City and over 40% (ARR 1.43, 95% CI 1.16–1.76) in its suburban counties, compared to the rest of New York State, that is unrelated to tumor size. We are unaware of any compelling explanations for this pattern, which deserves further analysis and continuing surveillance. Activists have cited the presence of the Indian Point nuclear reactor located in Buchanan, Westchester County, as a causal factor (24), but historic releases of 131I from this facility have been negligible. Specifically, cumulative 131I releases from Indian Point have been ∼50,000 times lower than releases from the nuclear weapons plant in Hanford, Washington, between 1944 and 1957. The Hanford Thyroid Disease Study, one of the largest and most complex epidemiologic studies of the relation between environmental exposures and 131I and thyroid disease, has found no conclusive elevated risk of thyroid cancer from these exposures (25 –27).
The association between thyroid cancer and highly observant Jewish populations could plausibly have either a genetic or environmental basis. A number of cancers and cancer-related conditions have been found to be in excess in Jewish populations, including ovarian, pancreatic, endometrial, colon, and stomach cancers, non-Hodgkin's lymphoma, hairy cell leukemia, classic Kaposi's sarcoma, Bloom's syndrome, polycythemia vera, Gaucher's disease, Crohn's disease, ulcerative colitis, Fanconi's anemia, and ataxia telangiectasia (28). Cancer-related genetic mutations in excess in Jewish populations include the BRCA1, BRCA2, MSH2 1906C-G Ashkenazi, and APCI1307K Ashkenazi founder mutations (8,28 –30). These mutations concentrate in the population as a result of the tradition of intra-religion and intra-community marriage (31).
It could also be the case that Jewish persons receive disproportionate exposure to environmental radiation, particularly radioactive iodine, during fetal development and childhood. Ionizing radiation in the environment is the most well-established risk factor for thyroid cancer (32), and people with iodine deficiencies are more likely to take up atmospheric iodine. As Europe and the Eastern Mediterranean area have the lowest usage of iodized salt in the world (with Kosher salt and Sea salt not being iodized), it is plausible that Jewish emigrants from these areas and their descendents (33) suffer disproportionately from iodine deficiencies and therefore take up more radioactive iodine from their surroundings. Even if environmental exposures are not meaningfully different between Jewish and non-Jewish populations, gene–environment interactions could still play a role. For example, carriers of the ataxia-telangiectasia mutation have been hypothesized to be at increased risk of sensitivity to radiation (34). Additionally, the highly observant Jewish population is likely to have differences from the general population with respect to other environmental factors that have been hypothesized to be associated with thyroid cancer, including reproductive history and diet (35,36).
Our analysis was subject to a number of limitations. The identification of individuals as being highly observant Jews because of their residence in areas identified as highly observant was ecologic and subject to misclassification. Specifically, some non-Hispanic White people living in the census tracts identified as highly observant may be of Jewish descent, but not involved in a highly observant sect, or may not be Jewish at all. The converse is also true; there may be highly observant Jews in areas that are not considered highly observant in our analysis. The same reasoning applies to areas categorized as RBU neighborhoods or by poverty rate. Census tracts were chosen as the spatial unit to associate with synagogues because of their congruence with urban neighborhoods, but synagogues may draw population from several adjacent census tracts or an area smaller than a single tract. Together, these factors would tend to make it more likely that we underestimated the effect sizes for these variables. In addition, tumor size was not reported for ∼15% of the cases. Tumor size is more likely to be missing in earlier years and from smaller reporting facilities and thus could exert a small bias on the results.
In conclusion, the substantially elevated thyroid cancer incidence in areas of New York State with high levels of highly observant Jewish persons does not seem to be diagnostically driven, but rather is due to some other factor, or combination of factors, as yet unknown. An independent elevation of similar magnitude is seen among those who live in the suburbs of New York City and in New York City itself. Further research, such as a case–control study using a more sophisticated study design, needs to be done to examine this relationship and determine if causes of the higher incidence of thyroid cancer in this population can be established.
Footnotes
Acknowledgment
The authors of this article were supported in part by the Centers for Disease Control and Prevention's Cooperative Agreement U58/DP000783, awarded to the New York State Department of Health through the National Program of Cancer Registries.
Disclosure Statement
All authors declare that no competing financial interests exist.