
Abstract
Background:
Thyroid paraganglioma (TP) is a very rare neoplasm that can be misdiagnosed. We evaluated the clinical and pathologic characteristics of three patients with TP.
Patient Findings:
The records of all patients from 1981 to 2008 who had thyroidectomy with a final histologic diagnosis of TP were retrieved, and histology was reviewed by a single pathologist. Head and neck paragangliomas arising outside of the thyroid were excluded. TP accounted for 3 of all 6782 (0.04%) patients undergoing thyroidectomy during three decades. One patient has been previously reported and will not be discussed. In the remaining two patients and a surgical pathology consult case that we also describe herein, the mean age at diagnosis was 56 years (40–67) and two patients were men. Presenting features were indicative of advanced local invasion, including stridor, tracheal invasion, compression of the great vessels, and hemoptysis. The diagnosis of TP was not suspected preoperatively; in two patients, fine-needle aspiration (FNA) cytology was inadequate for diagnosis because of excessive blood. Intraoperative frozen section analysis suggested medullary thyroid cancer in two patients and oncocytic (Hurthle) cell carcinoma in one patient. Local invasion was common, requiring concurrent tracheal resection in two of three patients, and present histologically in all three patients. In all three cases, immunohistochemical analysis was negative for cytokeratin AE1/3, calcitonin, and thyroglobulin but positive for S100, highlighting sustentacular cells. After resection of a large TP with tracheal and vascular invasion, a 67-year-old woman experienced a 7-year disease-free interval.
Conclusions:
Primary TP is indeed rare. It does occur in men, frequently presents with compressive symptoms, and is typically locally aggressive, but does not appear to cause symptoms suggestive of catecholamine excess. Despite invasion of adjacent structures, aggressive resection can achieve a long disease-free interval.
Introduction
TP may arise from misplaced inferior laryngeal paraganglia (18,32). Morphologically, TP is difficult to distinguish from medullary thyroid cancer (MTC) and thus correct diagnosis by either preoperative fine-needle aspiration (FNA) biopsy or intraoperative frozen section is reportedly rare. Because TP arises from embryonic neural crest cells, positive immunohistochemical tissue staining for neuroendocrine markers such as chromogranin A and synaptophysin in addition to negative staining for cytokeratin helps to determine the histologic diagnosis in patients with these interesting tumors. Although local invasion is often seen at the time of initial presentation, surgical resection can result in durable cure, and to date, there have been no reported cases of disease recurrence. We present here the clinical and pathologic characteristics of three patients (two men and one woman) with TP, all three of whom had locally invasive tumors.
Methods
Clinical data were retrospectively reviewed under a protocol approved by the Institutional Review Board of the University of Pittsburgh. During the 27-year period studied (1981–2008), 6782 patients underwent thyroidectomy at our institution. All patients with a final histologic diagnosis of TP were identified and histology was reviewed by a single pathologist (S.I.C.). Head and neck paragangliomas arising outside of the thyroid were excluded. A total of three patients were diagnosed with TP, which gives an approximate primary TP prevalence of 3 of 6782 (0.04%) among patients requiring thyroidectomy. One of our three TP patients has been previously reported and thus will not be discussed further (12). In each case, the extent of thyroidectomy was determined by the intraoperative findings and the ability to resect with clear margins. Additionally, a pathology consult case reviewed by the same pathologist is described. The mean age at diagnosis of these three cases was 56 years (range, 40–67).
Patient 1
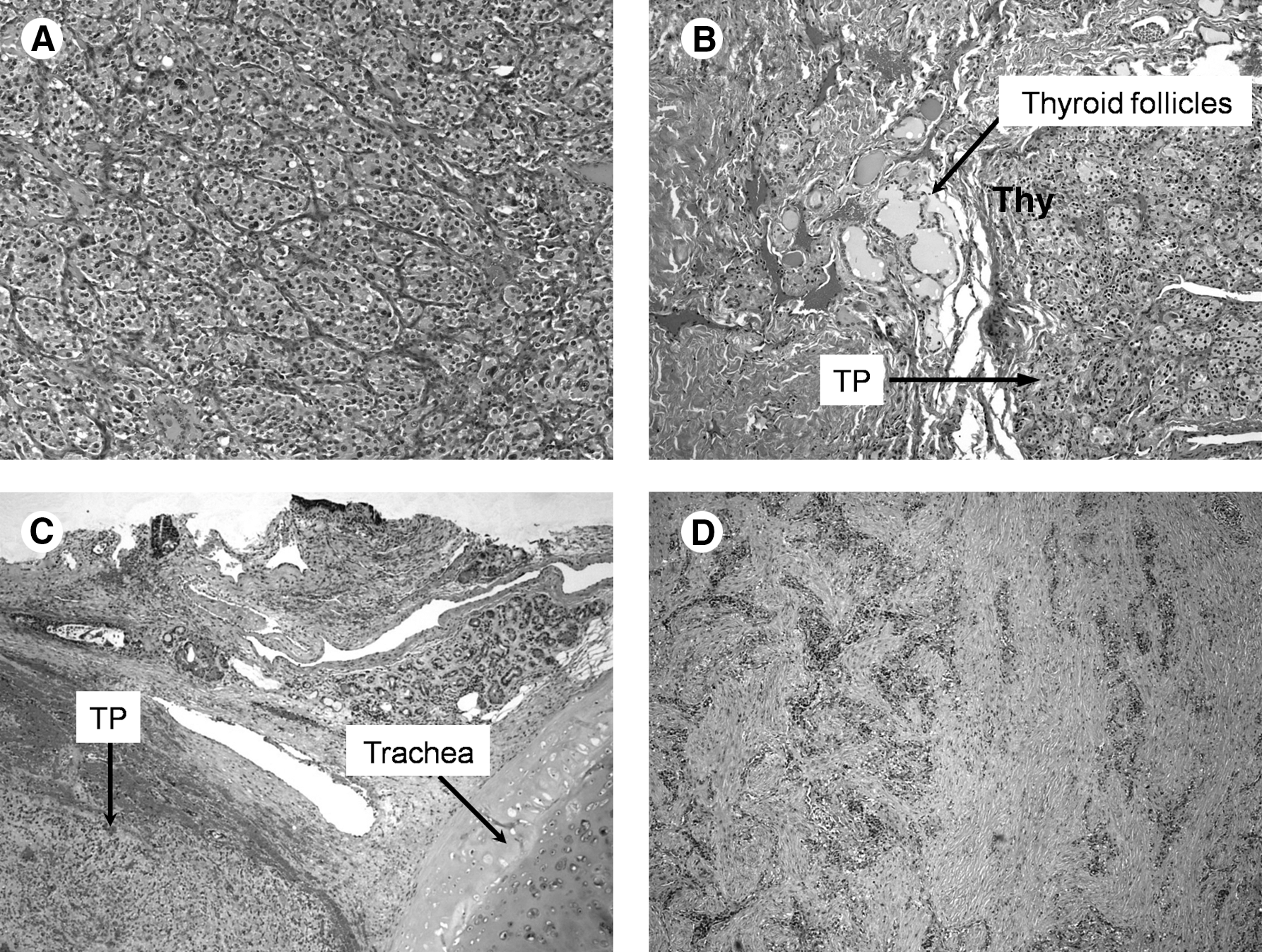
A 67-year-old woman presented with a large thyroid mass that had been of concern for at least 3 years, but surgical referral was delayed because of cardiac concerns. She had a history of total colectomy for ulcerative colitis at 44 years prior. When she developed dysphagia, dyspnea, stridor, and hemoptysis, neck computed tomography (CT) revealed a 9-cm mass of the left thyroid lobe causing severe tracheal compression at the thoracic inlet and extending caudally to the innominate vein. Preoperative FNA was read as nondiagnostic because of excessive blood. Intraoperatively, the airway was managed with jet ventilation, and a rigid bronchoscopy confirmed endotracheal invasion; tumor compression of the cervical esophagus was associated with large esophageal varices to the cricopharyngeus. In a combined resection performed by the thoracic and endocrine surgery teams in 1993, the tumor was exposed by cervicotomy and median sternotomy and was found to be extremely friable and vascular, extending caudally to the innominate vein. Although frozen section analysis suggested possible MTC, because of concern about the integrity of the left recurrent laryngeal nerve, the patient underwent anatomic left thyroid lobectomy and isthmusectomy, concurrent tracheal resection of rings 3–6 with negative margins, and immediate reconstruction. She did well postoperatively. Histologically, multiple encapsulated nodules up to 3.5 cm were found within the tumor and electron microscopy revealed mitochondria-rich endocrine epithelial cells with neurosecretory granules and the characteristic sustentacular cells of TP. The immunohistochemistry findings supported the diagnosis of TP with negative cytokeratin AE1/3, calcitonin, thyroglobulin, and carcinoembryonic antigen staining but positive chromogranin, serotonin, synaptophysin, S100 (in sustentacular cells), and neuron-specific enolase staining (Fig. 2). Interestingly, TP tumor so completely replaced the entire left thyroid lobe that the original pathologist disputed that anatomic lobectomy had been performed; thus, postoperative 123I thyroid imaging was done and confirmed that anatomic left lobectomy had indeed occurred. In chronic postoperative surveillance, cervical ultrasonography, chest CT, and 24-hour urine catecholamine levels remained normal with no evidence of distant metastases. Four years after TP surgery, she developed a bleeding polyp at her ileostomy site that proved to be adenocarcinoma in situ and later manifested metastatic adenocarcinoma to the liver, to which she succumbed at age 74, almost 8 years after TP resection.
Patient 2
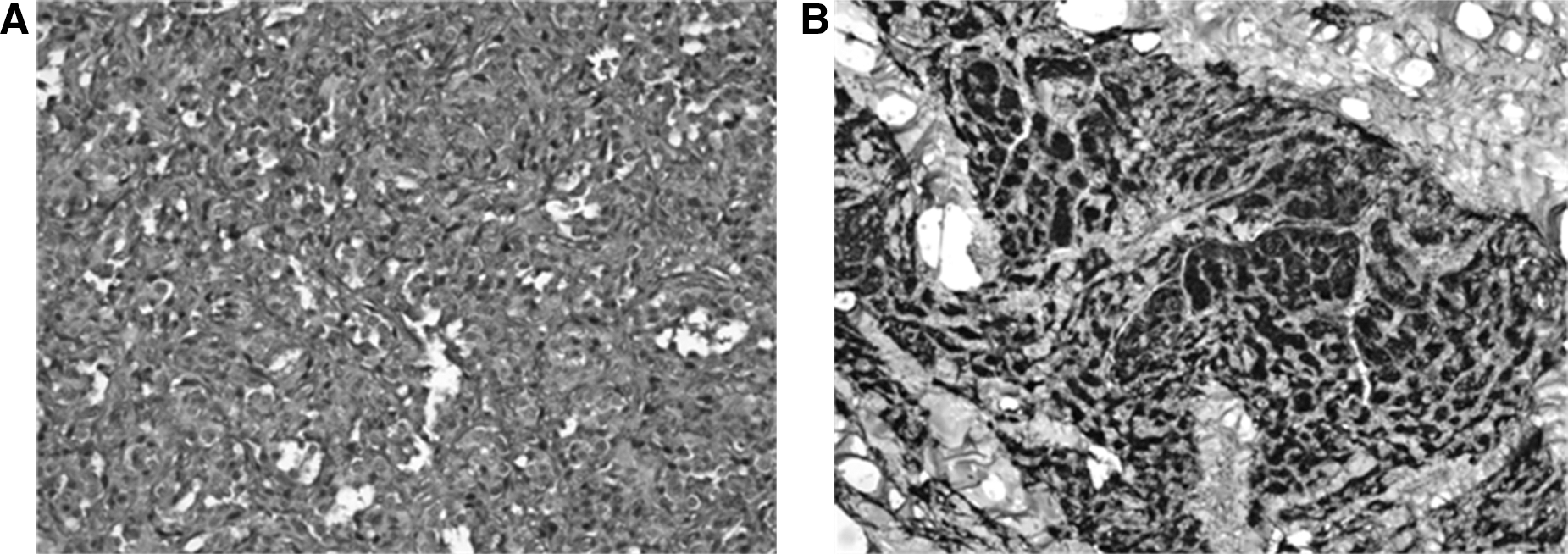
A 40-year-old man presented with a 2-year history of a large thyroid mass associated with dyspnea on exertion and progressing to stridor. He had no evidence of hypertension. Neck CT showed a 5.0-cm left thyroid mass with tracheal invasion. At surgery in 1997, no esophageal invasion was present on esophagoscopy, but rigid bronchoscopy showed a polypoid mass within the trachea, causing 50% airway obstruction. At left thyroid lobectomy, frozen section evaluation was positive for Hurthle cell carcinoma, and total thyroidectomy with tracheal resection, negative margins, and primary tracheal reconstruction was performed. Histologic examination showed a tumor composed of eosinophilic cells with focally pleomorphic nucleoli-forming cellular nests (Zellballen arrangements) lined by fine fibrous septae with extensive thin-walled vasculature characteristic of TP (Fig. 1). The diagnosis of TP was confirmed by negative immunohistochemistry (IHC) staining for carcino-embryonic antigen (CEA), calcitonin, thyroglobulin, and pancytokeratin but positive staining for S-100 and synaptophysin. Neck and chest CT scans were absent of metastases. Clinical follow-up was unavailable, but the patient lived another 14 years.
Patient 3
A 60-year-old man was evaluated as a pathology consult. The patient had presented with a 3.2-cm right thyroid mass and underwent total thyroidectomy in 2008, because an intraoperative frozen section suggested malignant medullary thyroid carcinoma with vascular invasion. On final pathology, a primary TP with vascular invasion was diagnosed and confirmed with negative IHC staining for CEA, calcitonin, thyroglobulin, cytokeratin AE1/3, TTF1, and Pax8, but positive staining for S-100, synaptophysin, and chromogranin. Clinical follow-up including the presence or absence of metastasis was unavailable.
In summary, locally invasive tumors were seen in all three cases of TP requiring aggressive surgical resection to achieve negative margins. The histologic findings by light microscopy are characteristic and include highly vascularized tumors with distinctive cell nests (Zellballen architecture) surrounded by sustentacular cells and separated by fibrovascular stroma (Fig. 1). Confirmatory IHC findings included positive staining for S-100 and synaptophysin in all three cases and chromogranin in two of three cases. Durable cure was achieved after primary surgical therapy, which should be the first treatment modality for these rare primary thyroid tumors.
Discussion
TP is a very rare tumor. Our findings indicate an approximate prevalence of 0.04% among patients requiring thyroidectomy. In brief reports of 1–3 patients, a total of 32 cases of TP have been previously described. Moreover, only two previous cases were in men. We here describe an additional three cases of TP, including two in men. We thus can conclude that while TP is more prevalent in women, male gender does not preclude the diagnosis.
In the current series, there were several clinical findings that were unique to TP. TP in all cases presented with a locally aggressive growth pattern involving tracheal compression and direct tracheal invasion (two of three patients). The common types of thyroid neoplasia typically have either a much more indolent rate of growth (papillary, follicular, and MTC) or a more rapid rate of growth (anaplastic thyroid cancer and primary thyroid lymphoma). We thus suggest that a clinically intermediate rate of growth, such as expansion over 2–3 years as we observed in two of the patients described here, can be a clue to the presence of this rare tumor. Further, in non-TP thyroid cancer, the rate of local invasion is <5% (20,33).
The available data on the clinical presentation of the world's cases of TP are given in Table 1. TP was primarily diagnosed as a thyroid mass (22/32) or cold nodule (6/32), and pain was also reported in only three patients. FNA was performed sporadically and was nondiagnostic in 4 of 19 (as in our series), misdiagnosed as MTC in 6 of 19 cases, and indicative of TP in only 1 of 19 cases who had FNA. At surgery, a full 9 of 32 patients were noted intraoperatively to have thyroid capsule adherence or tumor extension to adjacent structures. However, even with local invasion into the trachea or esophagus, aggressive surgical resection of TP to achieve negative margins can result in durable cure, as seen for Patient 1 described here, who underwent major resection and lived 7 years with no indication of recurrence in careful surveillance, to succumb to another disease entirely. Although synchronous and metachronous tumors can occur (4,5,14), local tumor recurrence of TP has not been reported, which further emphasizes the importance of primary surgical treatment of these locally aggressive tumors.
A, alive; adher, adherence; bilat, bilateral; BP, blood pressure; compress, compression; differ, differentiated; epith, epithelial; esoph, esophagous; exten, extension; foll, follicular; HTN, hypertension; hyperthy, hyperthyroidism; hypervasc, hypervascular; invas, invasion; jug, jugular; L, left; malig, malignant; metach, metachronous; MTC, medullary thyroid cancer; mut, mutation; NA, not available; neo, neoplasm; para, paraganglioma; poss, possible; pt, patient; R, right; RAI, radioiodine ablation; rsxn, resection; susp, suspicious; synch, synchronous; thy, thyroidectomy; trach, trachea; TT, total thyroidectomy; W, well; w/, with.
TPs are a subset of the head and neck paraganglioma, which arise from the parasympathetic system and are usually nonfunctional (3,34). However, a recent study found that when systematic evaluation included 24-hour urine dopamine and 2-methoxytyramine, up to 29% of head and neck paraganglioma had detectable active catecholamine synthesis (35). To our knowledge, no study has yet specifically examined TP biochemical function or described surgical complications due to TP catecholamine secretion. One historical case did show postoperative improvement of hypertensive symptoms (20). None of our patients had symptoms of catecholamine excess uncovered preoperatively or intraoperatively, and although mild hypertension has been reported in 8 of the 32 historical TP patients (4,11,15,18,20,22,23,28), we suspect that this may reflect its incidence in the population at large. Preoperative medical blockade of TP could thus be imperative for a safe surgical outcome in the modern era with a method of accurate preoperative diagnosis available for this rare tumor.
We and others have observed that TPs are often misdiagnosed by both FNA and frozen section analysis (27,36). MTC is the most common differential diagnosis. In our three patients, the intraoperative frozen section analysis suggested MTC in two patients and Hurthle cell carcinoma in one patient. In addition to MTC, the appearance can suggest metastatic renal cell carcinoma (18), metastatic carcinoid (15), poorly differentiated thyroid cancer (15,18), or even follicular thyroid cancer (26). IHC is confirmatory for TP and includes positive staining for S-100 in the sustentacular cells with negative staining for cytokeratin, calcitonin, and CEA (Fig. 2).
Immunohistochemical analysis: all were negative for cytokeratin AE1/3, calcitonin, and thyroglobulin but positive for S100
As with most endocrine neoplasms, there are no standardized histological criteria for differentiating benign and malignant TP. Thus, long-term clinical follow-up is required to evaluate for distant metastases that would indicate malignancy. Of our three patients, two had CT scans that were negative for metastasis and were considered benign. Our third patient did not have sufficient available data to allow us to assess the malignant potential of his disease. Overall, benign head and neck paragangliomas have a 5-year survival of 95%, while malignant paragangliomas are estimated to have a 5-year survival rate of 43.3%; however, the paucity of data makes this difficult to ascertain and outcomes are likely more associated to the disease stage at diagnosis (37). The malignant potential of TP is unknown, but to date there have been no reports of locoregional recurrence or distant metastasis. TPs have been predominantly considered benign, including two of our cases that had frank regional invasion. Yet, with initial aggressive resection, to our knowledge, none have recurred. Ongoing surveillance is also needed to monitor for the development of metachronous tumors, which has been previously reported (14). Further, consideration of SDHB or SDHD mutation testing should be discussed and the appropriate genetic counseling should be provided for first-degree relatives.
In conclusion, primary TP is indeed very rare and does occur in men. TP frequently presents with a clinically intermediate and locally aggressive growth pattern involving compression of thoracic outlet structures. Tracheal invasion and vascular invasion are common. FNA and frozen section analysis are typically hypervascular and nondiagnostic. Despite direct tracheal invasion, aggressive surgical resection of primary TP can achieve a long disease-free interval.
Footnotes
Disclosures Statement
No competing financial interests exist.