
Abstract
Background:
BRAF mutations, the most common genetic alteration associated with papillary thyroid carcinoma (PTC), have never been associated with follicular thyroid carcinoma (FTC) except for one possible case, which, however, had some cellular features of the follicular variant of PTC. Here, we present a patient with a BRAF mutation within a FTC.
Summary:
A 78-year-old man presented with a nodular lesion 8 cm in size in the right thyroid lobe, coexisting with a goiter. Fine-needle aspiration samples were obtained for cytology, immunocytology, and molecular analysis. Immunoblot analysis on thyroid tissues was performed to evaluate the most important tumor activating pathways. Cytology was consistent with “follicular neoplasia” (negative for galectin-3 immunostaining); molecular analysis on the cytology sample detected a K601E mutation in the exon 15 of the BRAF gene. After total thyroidectomy with lymph-node dissection, the diagnosis of FTC was established by histopathological examination. The BRAF K601E mutation was confirmed in DNA obtained from different areas of the FTC. In addition, an activating mutation (E545A) in the PKI3CA oncogene was found in the FTC. As expected, immunoblot analysis showed activation of the PI3K/Akt pathway.
Conclusion:
This article describes what may be the first case of a classical FTC carrying a BRAF mutation. Unlike the most common BRAF mutation seen in PTC carcinoma (BRAF V600E), this patient's mutation was a BRAF K601E mutation that previously has been associated with some cases of the follicular variant of PTC. The BRAF K601E mutation should be included in the spectrum of genetic alterations in FTC.
Introduction
PTC has commonly been associated with BRAF mutations and, since this finding is almost always specific, a BRAF mutation is currently considered a suitable marker for PTC (3). BRAF mutations have almost never been reported in association with FTC, in which other genetic alterations (N-Ras, H-Ras, K-Ras point mutations and/or PAX8/PPARγ rearrangements, and/or PI3K/Akt pathway mutations) have been identified (4). Some of these molecular disarrangements are also rarely found in follicular variants of PTC (5). Here, we describe the first case of an FTC associated with the BRAF K601E mutation.
Patient
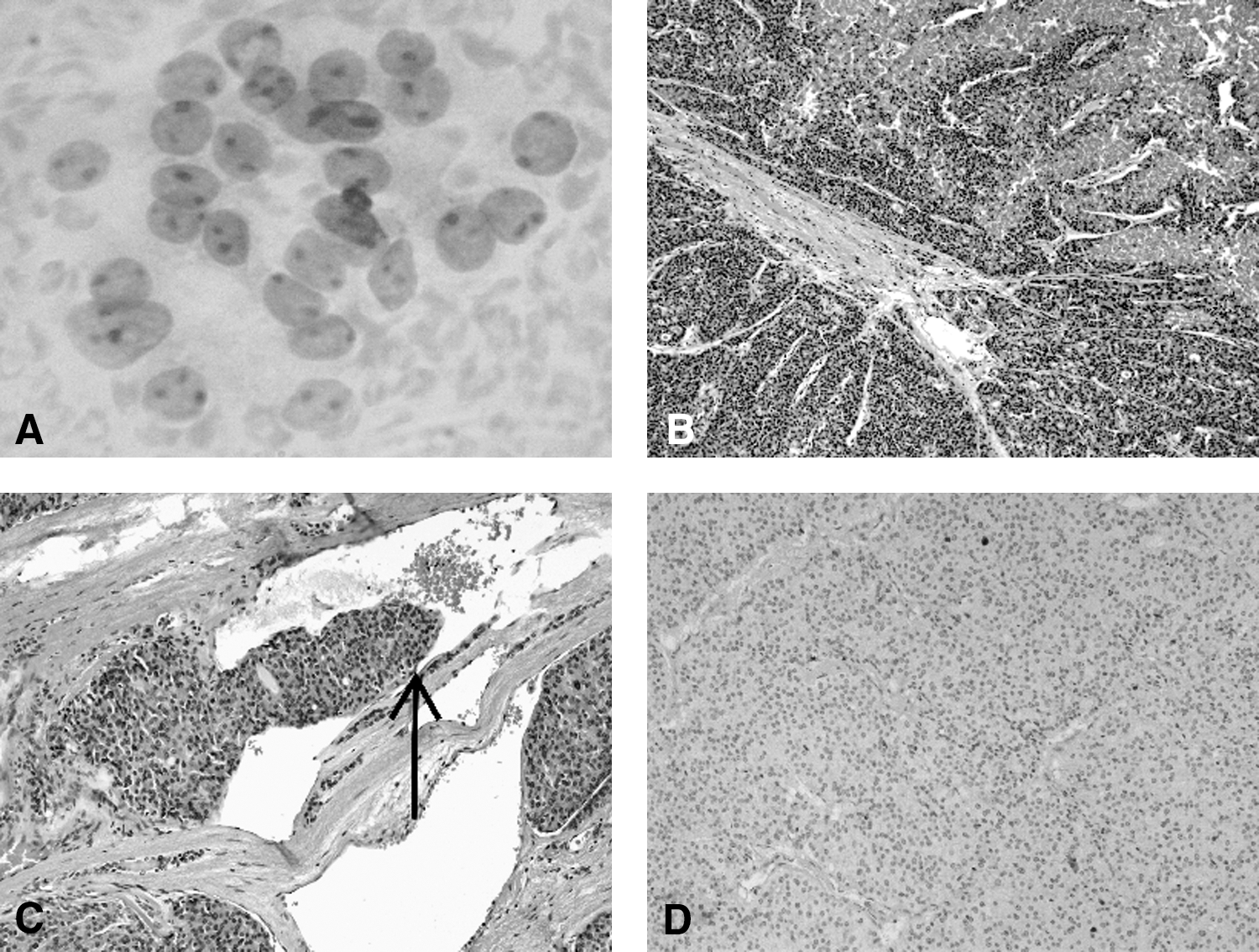
A 78-year-old Caucasian man with no significant medical history was referred to our Endocrinology Unit with a compressive nodular goiter. Physical examination revealed a nontender thyroid mass that moved on swallowing. Ultrasound showed a well-defined, hypoechoic nodule (8 cm in size) in the right thyroid lobe, with intranodular Doppler flow. No cervical lymphadenopathy was clinically detectable. Thyroid function tests were as follows: thyrotropin 1.56 mIU/L (normal range [n.r.] 0.27–4.20), free thyroxine 1.07 ng/dL (n.r. 0.93–1.7), free triiodothyronine 3.52 pg/mL (n.r. 2–4), calcitonin 6.1 pg/mL (n.r. 0–10), thyroglobulin >5000 ng/mL (n.r. 1.4–78), and negativity for anti-thyroglobulin antibodies. Cytological findings (on FNA biopsy) were consistent with “follicular neoplasia” with scattered cellular atypia (Thy 3) (Fig. 1A) (6).
A commercial anti-Galectin3 (Gal-3) antiserum was applied to the FNA sample (Galectin3 [9C4] Cell Marque). Using a biotin-free peroxidase complex technique, immunostaining was performed automatically with the Ventana ES secondary detection peroxidase/DAB kit (Ventana Benchmark XT system). The sections were then lightly counterstained with hematoxylin. An appropriate positive control was run concurrently, as previously reported (7). Gal-3 immunostaining was negative.
Genomic DNA was extracted from the FNA sample by using the DNeasy Blood and Tissue kit (Qiagen) according to the manufacturer's protocol. Analyses were performed for BRAF (exon 15), N-Ras (exons 2 and 3), K-Ras (exons 2 and 3), and H-Ras (exons 2 and 3) mutations by direct sequencing as described elsewhere (8,9). Molecular analysis revealed a BRAF point mutation in the exon 15, thus leading to a lysine-to-glutamate substitution at codon 601 (K601E) (Fig. 2A). No mutation was found in the H-Ras, K-Ras, or N-Ras genes (data not shown).
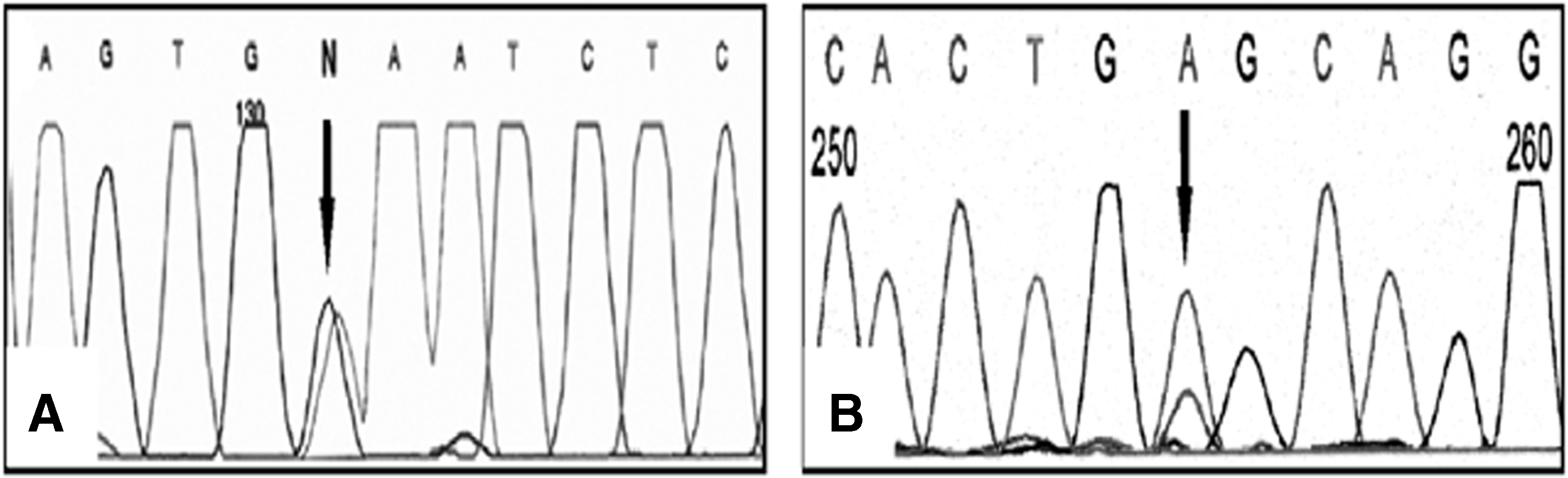
Electropherograms of
The patient subsequently underwent total thyroidectomy with central compartment lymph node dissection. The thyroid weighed 122 g and contained a subcapsular 80×56×53 mm firm, grayish-white intra-thyroid neoplasm with a thick capsule (with no infiltration of the resection margins). The five dissected lymph nodes (diameters ranging from 2 to 6 mm) had a grossly normal appearance.
The histological diagnosis of angio-invasive FTC with poorly differentiated component (Stage III, according to the 7th TNM classification) (10) was made by the local thyro-pathologist (G.P.). It was subsequently confirmed by blinded evaluations of two expert thyroid oncology pathologists (G.B. and S.A; see Acknowledgments). The neoplasia had a combined architectural pattern including well-formed follicles, solid/trabecular areas, and small necrotic foci (Fig. 1B). The neoplasia focally invaded the fibrous neoplastic capsule, where multiple (>4) angio-invasions were detected (Fig. 1C). No extra-thyroid spread was identified in any of the serial histology sections. The cell population included a well-differentiated (and even oxyphilic) component, coexisting with clusters of small and uniform poorly-differentiated cells. Nuclei were round/hyperchromatic and focally vesicular. No diagnostic feature of PTC was present. Mitotic activity was restricted to the poorly-differentiated cell population. Gal-3 immunostaining was consistently negative in histological sections of the cancer (Fig. 1D).
Genomic analysis was also performed on multiple tissue samples obtained from four different (follicular, oxiphil, insular, and trabecular) areas of the cancer. All tissue samples consistently harbored the same K601E mutation as was detected in the presurgical cytological sample. Analysis for PAX8/PPARγ rearrangements was also performed by reverse-transcription polymerase chain reaction as described in Nikiforova et al. (11) with negative results (data not shown). In addition, direct sequencing of the PIK3CA (exons 9 and 20) and PTEN (exons 5, 7, and 8) genes was carried out. One mutation was found in the exon 9, codon 545 of PIK3CA (GAG-GCG, E545A), which resulted in a glutamic acid to alanine substitution (12) (Fig. 2B).
Immunoblot analysis was performed on thyroid tissues (pathological and normal thyroid samples) by using different antibodies against Erk1/2, phospho-Erk1/2 (Thr202/Tyr204), MEK, phospho-MEK (Ser221), p70S6 kinase, and phospho-p70S6 kinase (Thr389). Cell proteins were isolated in lysis buffer containing a protease inhibitor. Proteins were separated by sodium dodecyl sulfate polyacrylamide gel electrophoresis, electroblotted onto nitrocellolose membranes and saturated in 5% milk. Membranes were incubated overnight at 4°C with primary antibodies and then incubated with horseradish peroxidase-labeled goat anti-mouse or anti-rabbit secondary antibodies for 1 h. Immunoreactivity was detected with a chemiluminescent substrate.
We found activated expression of phosphorylated p70S6 kinase, a downstream mediator of mammalian target of rapamycin (mTOR) in the PI3K/Akt pathway, in our specimen. Total p70S6 kinase was scarcely expressed and was comparable to a nonpathological sample (Fig. 3B, C).
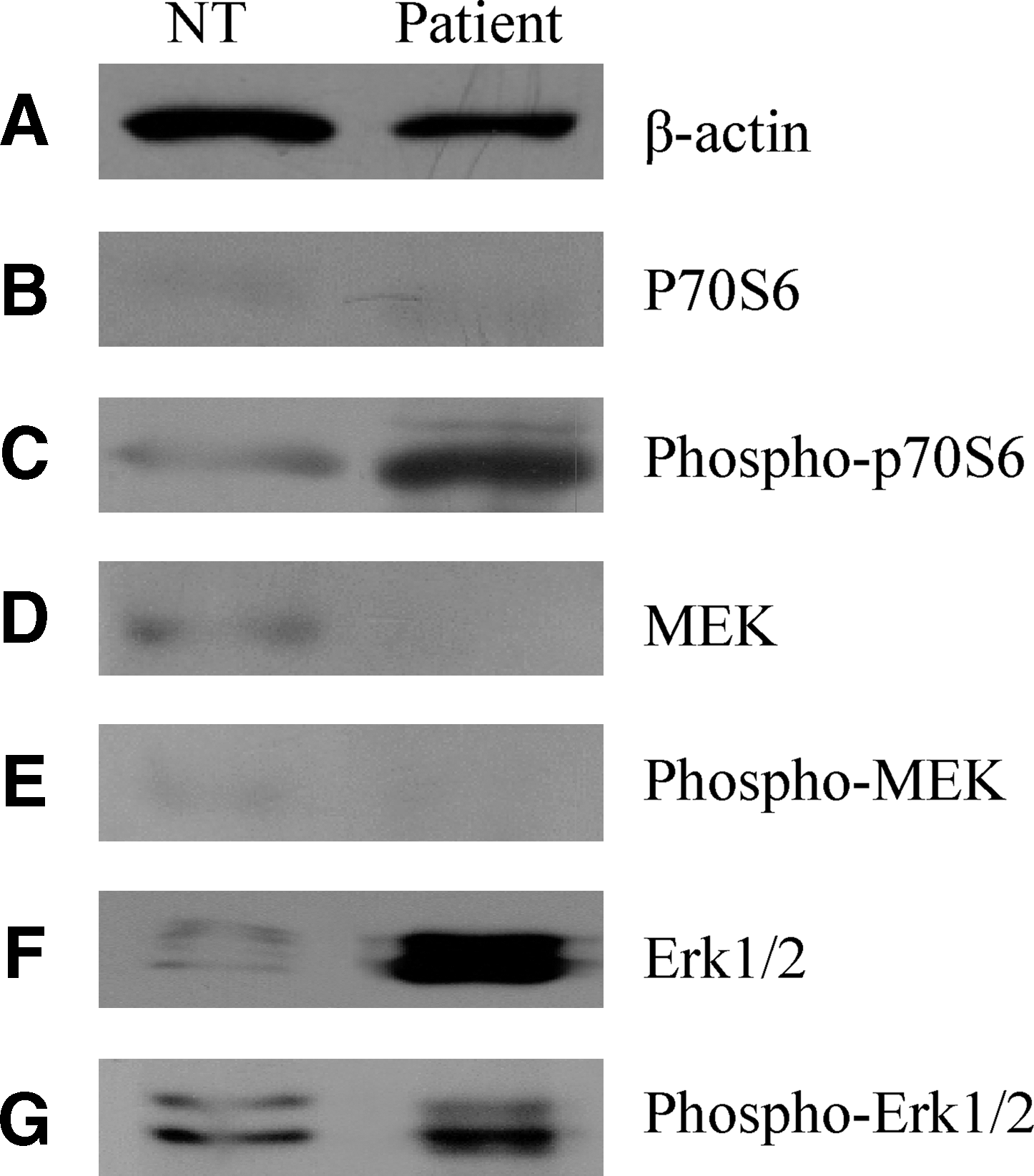
Immunoblot analysis of PI3K/Akt pathway
The MAP kinase (MAPK) pathway was investigated for Erk1/2 and MEK expression. By comparison with normal thyroid, we demonstrated a strong reaction for total Erk1/2 in a cancer specimen, whereas phosphorylated Erk1/2 was slightly increased. Total and phosphorylated MEK expressions were negative (Fig. 3D–G).
Discussion
BRAF mutations occur in about 45% of adult PTC cases (in both the “classic” and the “tall cell” variants), and they have also been identified in poorly-differentiated carcinoma arising from PTC. (13). The most prevalent mutation is a thymine-to-adenosine transversion in the exon 15 (nucleotide 1799), resulting in a valine-to-glutamate substitution in position 600 (V600E). Less frequently, the BRAF gene harbors a mutation resulting in a lysine-to-glutamate substitution at 601 (K601E) position; this event is detected in about 7% of cases of follicular variants of PTC and has also been reported in a unique case of follicular adenoma (14).
Kebebew et al. described a case of FTC harboring a BRAF V600E mutation. However, the tumor features were not completely consistent with classical FTC, as “some of the tumor cells showed intranuclear pseudoinclusions and nuclear grooves” (15). Apart from this “histologically unusual” case, no other cases of BRAF-mutated FTCs have been reported. In the present case, a true follicular histology was accompanied, at molecular level, by both an activating mutation of the PIK3CA gene and a “PTC-type” BRAF-status. Clinically, the patient's age, the constant lack of typical PTC nuclear features, and the absence of any lymph node implants (coexisting with an advanced thyroid tumor) support the diagnosis of a poorly-differentiated FTC.
Aberrant stimulation of the PI3K/Akt signaling pathway, by activating mutations in PIK3CA, is found in around 10%–15% of FTC and ATC and to a lesser extent in PTC, where it plays an important role in thyroid tumorigenesis and cancer progression to less-differentiated phenotypes (16). As expected by the presence of an activating mutation in PIK3CA (E545A), we demonstrated an up-regulation of p70S6 kinase, a downstream protein effector of activated Akt and mTOR (17,18).
As concerns the mutated BRAF genotype in this patient, this was consistently demonstrated in all the tissue samples of the tumor obtained both at FNA and in the thyroidectomy specimen, thus supporting the monoclonal origin of such thyroid cancer. In addition, we observed an increased level of phospho-Erk1/2 in our specimen, accompanied by a concurrent rise of basal Erk1/2, by comparison with in normal tissue, so that we could not demonstrate a constitutive activation of the MAPK pathway, as would be expected with BRAF mutations. Furthermore, we cannot exclude that the simultaneous presence of the two mutations (in the BRAF and PIK3CA oncogenes) could promote a cross-talk between the PI3K/Akt pathway and other pathways. Currently, we cannot define a reciprocal or synergistic role of BRAF or PIK3CA mutations in the pathogenesis of thyroid cancer in our patient. Further research is needed to address this question.
The molecular analysis of nodular thyroid lesions, including determining the status of BRAF, has recently been employed to improve diagnostic accuracy for cases where cytological findings are doubtful (19). The present demonstration of a BRAF mutation in a follicular cancer somewhat lowers the 100% reliability of aberrant BRAF status as a marker of PTC. In summary, this is the first report of a BRAF K601E mutation in FTC.
Footnotes
Acknowledgments
This work was supported by a grant from the Ministero dell'Istruzione, dell'Università e della Ricerca (No. 200734RMKE_002 to C.M.).
The authors are grateful to Professor Gianni Bussolati and Dr. Sofia Asioli of the Department of Biomedical Sciences & Human Oncology at the University of Turin for their kind review of the case. They also thank Dr. Davide Nacamulli, Mrs. Laura Zambonin, and Mr. Vanni Lazzarin for their excellent technical assistance. They are grateful to Professor J.M. Bidart for kindly donating positive controls for PAX8-PPAR gamma rearrangement for their experiments.
Disclosure Statement
The author declares that no competing financial interests exist.