
Abstract
Background:
Sorafenib has shown promise in the treatment of patients with advanced or metastatic thyroid carcinoma. However, its therapeutic effect has not been assessed in patients with brain metastases from follicular thyroid carcinoma (FTC). Here, we report a patient in whom this treatment was employed with a relatively favorable response.
Patient and Methods:
A 56-year-old woman had a thyroidectomy 8 years previously for FTC. She subsequently developed lung metastases, for which she received seven courses of radioiodine (131I) therapy. She developed right hemiplegia and other symptoms and was found to have a ∼5-cm lesion in the left parietal lobe. Radiosurgery with a total dose of 28 Gy (7 Gy/day, for 4 days) to treat her brain metastatic lesion was ineffective, and she was referred to us. We treated her with sorafenib, 200 mg orally, on a twice-daily basis. The effect of this intervention was assessed clinically and radiographically using Response Evaluation Criteria in Solid Tumors (RECIST).
Summary:
Symptoms and signs improved dramatically and continuously after initiation of sorafenib treatment. Partial response (PR) in the brain metastasis and stable disease (SD) in lung metastatic lesions were verified by consecutive imaging findings for more than one year. Despite alopecia, other treatment-related adverse events did not occur.
Conclusions:
Targeted therapy such as with sorafenib could be an effective alternative therapeutic strategy in the treatment of progressive brain metastasis from differentiated thyroid carcinoma (DTC) when surgery, external beam radiation, and 131I are not suitable or give poor outcomes. A paradigm of sustained low dose of sorafenib (200 mg,twice a day) may be well-tolerated without compromising maintenance of the therapeutic effect.
Introduction
Because of limited experience, management of thyroid carcinoma with brain metastases is often problematic. At present, management decisions are usually made based on case reports, retrospective series, and the standard of care for brain metastases from other types of tumors. Surgery is recommended for patients with accessible lesions, especially for a single lesion. For those patients with more aggressive tumors and multiple lesions, however, the role of surgery is less well established. The roles of external beam radiation therapy, gamma knife radiosurgery, and 131I therapy also are unclear (4).
Recently, a growing understanding of molecular oncology has allowed the development of targeted agents in different types of advanced thyroid carcinoma, offering great hope (5). Sorafenib is an oral, small-molecule tyrosine kinase inhibitor targeting vascular endothelial growth-factor receptors, RET/PTCs, and BRAF-mediated events (6). We have established a low dose of 200 mg twice daily in Chinese patients with 131I-refractory PTC, which has an overall clinical benefit rate of 77% with a mean progression-free survival of 42 weeks, and a more acceptable safety profile (7). In addition, experience from M.D. Anderson Hospital has demonstrated that both PTC and FTC had similar responses to this targeted therapy (8). To date, however, there is only one case in which sorafenib was used to treat brain metastases, and this was from PTC. This patient had a short-term stable disease (SD) response to sorafenib, probably because the drug was administered for only 16 weeks (9). We treated a patient with progressive FTC metastases to brain and lungs with sorafenib. The drug was administered for more than one year, since the patient was not amenable to surgery, and radiosurgery had a poor response.
Patient and Methods
A 56-year-old woman was admitted to our hospital in March 2010 complaining of progressive dizziness, impairment of recent and remote memory, slow response, lisp, vomiting, and right hemiplegia. She had undergone thyroidectomy for FTC (T2N1M1, Stage IVC) 8 years previously, followed by seven courses of 131I treatment for lung metastases with a total activity of 1050 mCi (38.85 GBq). By January 2010, the accumulation of 131I in both lungs had gradually decreased to faint visualization as compared to the image after the initial course of 131I therapy. No other iodine-avid lesion outside the chest was found (Fig. 1). She developed progressive dyspnea and debilitation of right arm and leg. Chest computed tomography (CT) showed multiple nodular lesions in both lungs with a predominant increasing mass measuring 11 cm×9 cm×20 cm in the left upper lobe (Fig. 2A). Brain magnetic resonance imaging (MRI) revealed a 5.0 cm×3.9 cm×5.2-cm-sized lesion in the left parietal lobe, which was hypo- and hyperintense on T1WI (not shown) and T2WI with marked perilesional edema (Fig. 3A). The serum thyroid-stimulating hormone (TSH), thyroglobulin, and antithyroglobulin antibody were <0.005 mIU/L, >50,000 ng/mL, and 637.5 IU/mL, respectively. Other biochemical parameters were within normal limits. The patient received radiosurgery with a total dose of 28 Gy (7 Gy/day, for 4 days) to treat her brain metastatic lesion. Two months after radiosurgery, however, she was referred to our clinic because of disease progression.
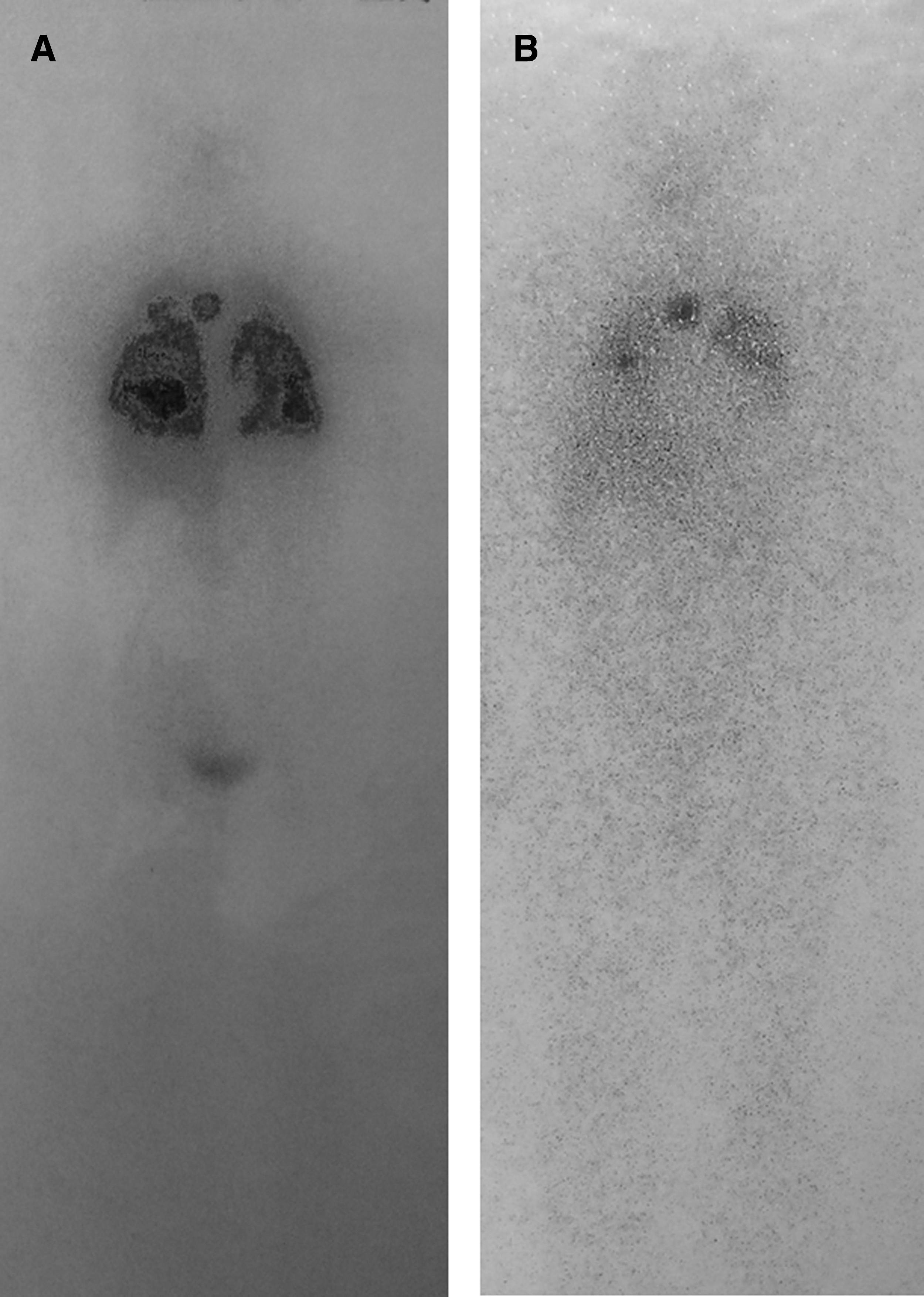
Whole-body planar scan (anterior view) on day 5 postradioiodine therapy (150 mCi) showing intense uptake in both lungs and mediastinum during the first treatment

Computed tomography scan of the chest (axial view) showing a mass measuring 11 cm×9 cm×0 cm in the left upper lobe before sorafenib treatment, indicating a contraindication of surgery for brain metastasis
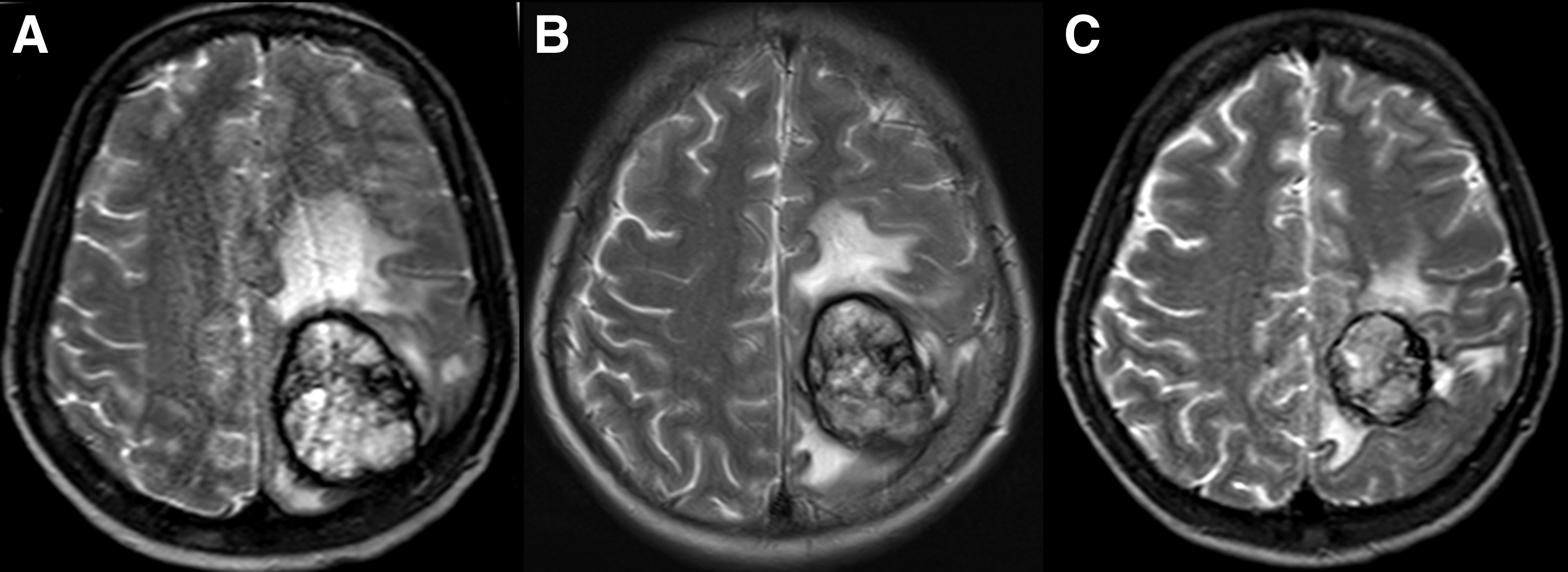
Magnetic resonance imaging (T2-weighted imaging [T2WI], axial view) showing a 5.0 cm×3.9 cm×5.2-cm-sized hyper- and hypointense lesion with perilesional edema in the left parietal lobe before sorafenib treatment, in accordance with a metastatic lesion accompanied by chronic and acute hemorrhage
At our clinic, we made a diagnosis of advanced multiple metastases from FTC to the lungs and the brain, which was refractory to 131I therapy and radiosurgery. Sorafenib was then administered orally at a dose of 200 mg twice a day as reported previously (7). The objective response was evaluated by medical imaging modalities using Response Evaluation Criteria in Solid Tumors (RECIST). Adverse events were assessed at each visit with an interval of a treatment cycle (4 weeks) using Common Terminology Criteria for Adverse Events (version 3.0).
Results
Four weeks after the start of sorafenib treatment her dizziness and headache improved. Three months later, incontinence of urine and stool resolved, and the patient could stand and walk with help. During the follow-up at 6 months and one year after the beginning of sorafenib treatment, she continued to be able to stand up and walk by herself and was able to talk without a lisp. Her recent and remote memory as well as judgment and emotional function improved significantly. Responses of SD in lung metastases and partial response (PR) in brain metastasis were achieved, which were confirmed by CT (Fig. 2) and MRI (Fig. 3), respectively. Expect alopecia, she did not experience hand–foot skin reaction, weight loss, or diarrhea. Sorafenib was continued at the dose of 200 mg twice daily for additional 2 months. The total duration of sorafenib treatment was at least 14 months, and at the time of this writing the patient was still taking sorafenib.
Discussion
The incidence of thyroid cancer has increased throughout the world in the past two decades with PTC being more common than FTC (10). Although the incidence of cervical lymph metastases at the time of diagnosis of differentiated thyroid carcinoma (DTC) is 45%, this is not always associated with a poor prognosis. The most common cause of death from thyroid carcinoma is neck recurrence, followed by lung, mediastinal, and rarely brain metastasis (11). The presence of distant metastases in extracranial sites, per se, is a risk factor for the development of brain metastases, as shown in the series by McConahey et al. in PTC patients from the Mayo Clinic, in which 15% of the patients with metastatic papillary carcinoma developed brain metastasis at some point during their disease course (12).
Brain metastases typically occur in older patients with more advanced disease and are associated with a worse prognosis (2). The lesions can become asymptomatic and may be associated with chronic or acute hemorrhage. These are characterized, respectively, by hypo- or hyperintense images on MRI (Fig. 3). Since brain lesions can cause acute life-threatening complications, early recognition and appropriate management are crucial. However, treatment varies, and there are no clearly defined guidelines. Surgical resection and external beam radiotherapy traditionally have been the mainstays of therapy (2,13). There are few data showing efficacy of 131I for treatment of brain metastases from DTCs, and since most of them do not have avidity for 131I, this treatment is usually not very effective. For the same reason, the suggestion has been made that 18FDG-PET/CT be used to evaluate such lesions (14). In these patients with no radioiodine uptake and disease progression, new therapeutic modalities need to be considered.
Sorafenib is a multikinase inhibitor that targets several molecular signals believed to be involved in the pathogenesis of DTC. As a novel therapeutic strategy, sorafenib has been successfully used in the treatment of advanced or metastatic 131I-refractory DTC, especially when there are pulmonary metastases (7,8,15,16). However, it has been rarely used in the treatment of brain metastases from DTC. Krajewska et al. treated a 55-year-old male with brain metastases from PTC for 16 weeks with sorafenib (800 mg/day) because of cancer progression despite thyroidectomy, 131I therapy, increasing doses of thalidomide, neurosurgical metastasectomy, and palliative central nervous system and vertebra radiotherapy. A response of SD was noted about 2 months after the beginning of sorafenib treatment according to radiological examination. However, further progression was observed 2 months after sorafenib withdrawal, indicating the therapeutic effect may be rapidly compromised by drug withdrawal (9). The reason for discontinuing sorafenib in that patient was not clear.
To our knowledge, this is the first report showing PR of more than one year for FTC with brain metastases. Our patient had progressive metastatic lesions in brain and lungs after surgery, TSH suppression therapy, 131I therapy, and radiosurgery, indicating an advanced and serious situation needing new therapeutic strategies. Although and perhaps because we gave the patient a relatively low dose of sorafenib, we were able to sustain the treatment for more than one year. This was much longer than that reported by Krajewska et al. (9). As demonstrated by improvement of clinical features and radiologic findings, a favorable response for brain and lung metastases was achieved in our patient, suggesting that drug maintenance is necessary to obtain sustained control of lesions.
In cancer therapy, reliable assessment of treatment response is essential, because response parameters often represent surrogate markers for improved survival. This is why RECIST was developed and became the main evaluation system used in current oncologic investigations. However, RECIST is not capable of assessing all the therapy-induced changes in tumor lesions. In this case, although shrinkage of pulmonary lesions could not be noted, marked cavitation of pulmonary lesions was found in the follow-up CT examination, which was performed 12 months after the initiation of the targeted therapy (Fig. 3C), suggesting tumor necrosis induced by an antiangiogenesis effect of sorafenib. It is our opinion that response assessment of targeted therapy is likely to be improved by adjusting volume measurements to take account of marked cavitation and attenuation as assessed by contrast enhancement imaging of pulmonary lesions. We favor this approach for studies of DTC patients, determining tumor responses to therapy with the multikinase inhibitor sorafenib.
Conclusions
Although multidisciplinary treatments have been used solely or in combination, there is no a clearly defined treatment protocol for brain metastases from DTC. Optimal treatment for individual patients may differ depending on the aggressiveness of the tumor and other factors. Sorafenib could be a valid treatment in patients with progressive brain metastasis from DTC when surgery, external beam radiation, and 131I are not suitable or ineffective. Sustained low dose of sorafenib (200 mg,twice daily) is usually well tolerated, allowing prolonged therapy with this agent and the possible employment of other treatment modalities.
Footnotes
Acknowledgments
This study was sponsored by the National Natural Science Foundation of China (30700187), Shanghai Rising-Star Program (08QA14040), and the Public Health Bureau of Shanghai Municipality (2006Y34).
Disclosure Statement
The authors declare that no competing financial interests exist.