
Abstract
Background:
Worldwide, iodine prophylaxis measures have improved iodine status in populations. Several studies have reported an increase in thyrotropin (TSH) levels coinciding with this prophylaxis. Whether this implies an increased risk for hypothyroidism or simply reflects a physiologic TSH adaptation mechanism is not clear.
Methods:
Data on iodine and thyroid status of 6–17 year old children and adolescents (n=9175), collected between 2003 and 2006 in the German-wide Health Interview and Examination Survey for Children and Adolescents (KiGGS) Study, provided the basis for the analyses of mutual relationships of urinary iodine status (assessed by iodine/creatinine ratio in spot urines), serum TSH levels, and thyroid volume (determined by ultrasound). For data analyses (multivariable linear regression analysis), only those children were included for whom none of the available parameters (including free triiodothyronine [fT3], free thyroxine [fT4], and thyroperoxidase antibody [TPO-Ab] measurements) indicated a potential pathophysiologic thyroid status (n=6101).
Results:
In this population-based sample of thyroid-healthy children, higher urinary iodine excretion was associated with higher TSH levels (p<0.05), adjusted for sex, age, body surface area, body mass index, fT3/fT4 ratio, and time of blood sampling. Higher TSH levels were not associated with a higher prevalence of TPO-Ab but with lower thyroid volume (p<0.001, fully adjusted). For the present study sample, one-time spot measurements of urinary iodine excretion were not related to thyroid volume, the long-term marker of iodine status.
Conclusion:
Our findings show for the first time in thyroid-healthy children that smaller thyroid volume is associated with higher normal TSH levels. A decreased thyroid cell mass and cell amount, as induced by an improved iodine status, does presumably require a higher TSH signal to maintain a constant thyroid hormone production, suggesting an underlying physiologic adaptation. Correspondingly, an increased TSH level should not be used as the single criterion to evaluate the prevalence of hypothyroidism, and the repeatedly observed parallel increases of iodine supply and TSH levels should not readily be interpreted as evidence for an increased hypothyroidism risk. These insights, contradicting conventional interpretations, may contribute to dispel uncertainties about the safety of iodine prophylaxis measures.
Introduction
O
According to the guidelines of the American Thyroid Association (2012), “serum thyrotropin (TSH) is the single best screening test for primary thyroid dysfunction for the vast majority of outpatient clinical situations” (7). Different studies that compared TSH levels between conditions of low and high iodine intake (e.g., cross-sectionally between different populations or prospectively after introduction of iodine prophylaxis measures) observed increased TSH levels with higher iodine intake (3,8 –11). From these observations, some of the authors concluded that an improved iodine status could cause a higher risk for hypothyroidism (8,11).
It has already been described that the distribution of TSH levels is shifted to higher levels in iodine sufficient populations, whereas it is skewed to lower levels in iodine deficiency (10). Different possible reasons for this observation are discussed, including thyroid autoimmunity (6) or thyroid autonomy (particularly in populations with previous iodine deficiency) (10), but the underlying mechanism is so far not clear. Whether an iodine-dependent TSH increase could rather be a normal adaptive phenomenon, secondary to some kind of “downregulation” of the thyroid (6), has not yet been examined in this context. In older studies in rats (12), it was shown that there is an increased sensitivity to TSH in iodine deficiency. The response of the cAMP pathway to TSH is under negative control of iodine (13). Therefore, it can be hypothesized that under iodine repletion, the TSH signal should increase to maintain normal thyroid hormone release.
Based on the extensive and detailed data collection in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) on iodine excretion, thyroid hormones, thyroid volume, and autoantibodies, we aimed to investigate two hypotheses: (a) in thyroid-healthy children and adolescents, a better urinary iodine status is (physiologically) associated with higher TSH levels; and (b) this finding is associated with a smaller thyroid volume (induced by better iodine supply) requiring a higher TSH signal to maintain a constant thyroid hormone output.
Materials and Methods
Study population
The data for the present examination were taken from the KiGGS Study, conducted from May 2003 to May 2006 by the German Robert Koch Institute (RKI), Berlin. The aim of this nationwide survey was to obtain for the first time comprehensive and representative data on the health status of German children and adolescents aged 0–17 years. A total of 17,641 children and adolescents (8656 girls and 8985 boys) from 167 towns and municipalities representative of the nation as a whole participated in the study. Details on the study protocol have been published elsewhere (14). The parents of all participants gave informed written consent.
For the present study, we included all 6–17 year old children for whom measurements on urinary iodine and creatinine excretion, TSH, free triiodothyronine (fT3) and free thyroxine (fT4) serum levels, and thyroid volume were available (n=9175; Fig. 1). To maintain a thyroid-healthy study population, additional exclusion criteria were applied, finally resulting in a subsample of the KiGGS Study of 6101 children (Fig. 1).
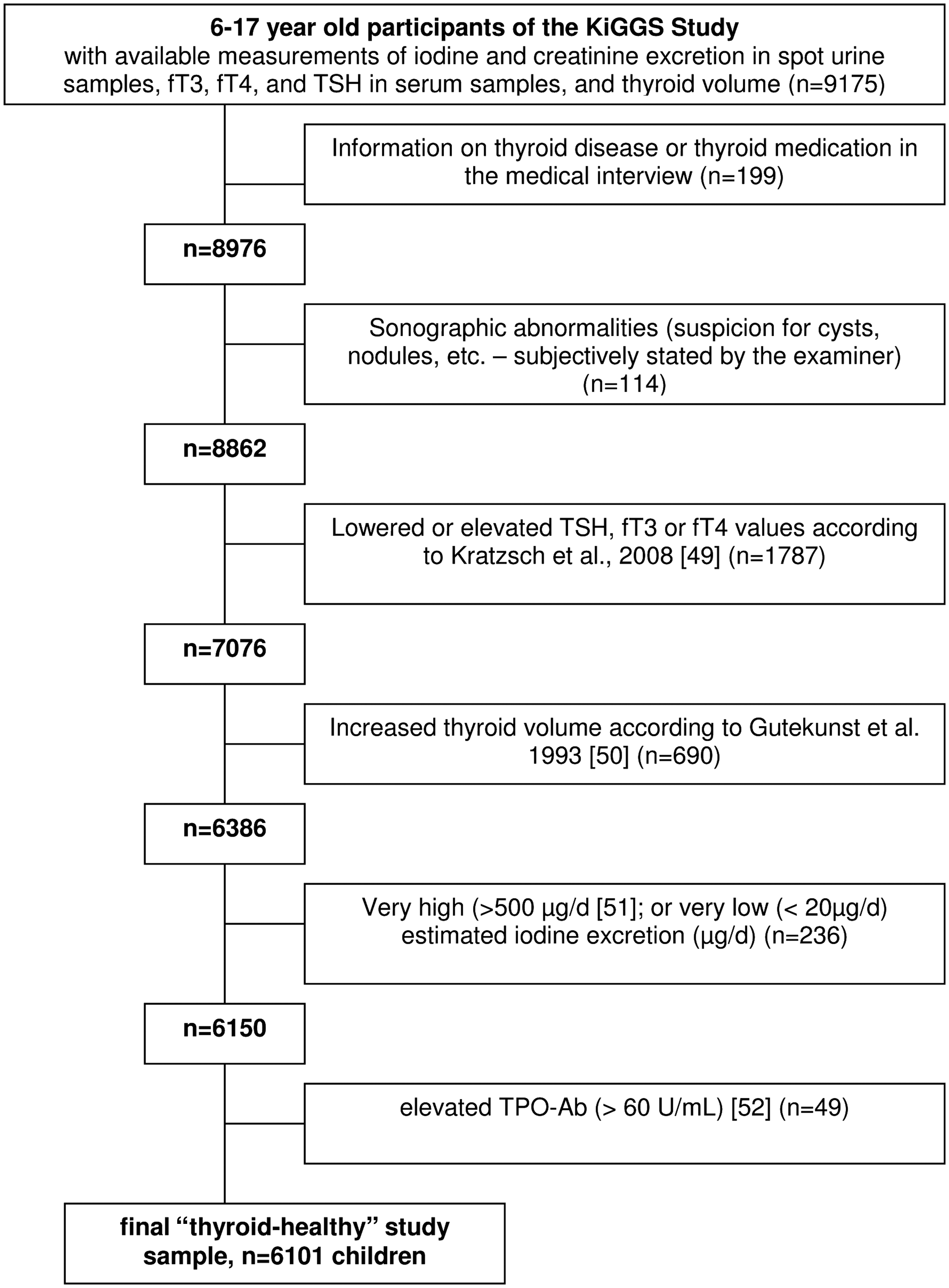
Selection criteria for the “thyroid-healthy” subpopulation of the German-wide Health Interview and Examination Survey for Children and Adolescents (KiGGS) Study.
Assessments
Body height was measured to the nearest 0.1 cm using calibrated stadiometers (Holtain Ltd., Crosswell, United Kingdom). Electronic scales (SECA Ltd., Hamburg, Germany) were used to measure body weight to the nearest 0.1 kg. From these measurements, body mass index (BMI) was calculated as weight (kg)/height (m)2. Body surface area (BSA) was calculated according to the formula of Du Bois and Du Bois (15).
Iodine concentration in spot urine samples was determined after pretreatment with ammonium persulfate by the principle of the Sandell–Kolthoff reaction on the Analyzer system Cobas Mira plus (Roche, Basel, Switzerland). The procedure was validated by inductively coupled plasma mass spectrometry (ICP-MS) and conventional manual Sandell–Kolthoff photometry. The Spearman correlation coefficients each amount to 0.97 (p<0.01). Creatinine concentration was measured in spot urine samples by the Jaffé method without deproteinization on the Hitachi 917-Analyzer (Roche).
Blood samples were drawn with evacuated serum gel tubes between 09:00 and 19:00 h and processed within 45 min according to a highly standardized protocol (16). TSH, fT3, and fT4 were measured with electrochemiluminescence assay on an Elecsys 2010 immunoanalyzer (Roche Diagnostics, Mannheim, Germany). Intra- and inter-assay CVs (%) were <8.6 and <8.7 for TSH (concentrations 0.034, 0.91, 3.96 U/mL); <2.2 and <2.9 for fT3 (concentrations 2.90, 3.83, 19.4 pmol/L), and <2.9 and <6.6 for fT4 (concentrations 8.7, 21.1, 50.8 pmol/L), respectively. Sensitivity was 0.005 U/mL for TSH, 0.4 pmol/L for fT3, and 0.3 pmol/L for fT4. Thyroperoxidase antibodies (TPO-Ab) were measured on Thyroid Peroxidase ImmunoCAP (Phadia, Uppsala, Sweden) with intra- and inter-assay CVs (%) <4.7 and <7.2 respectively (concentrations 182, 494, 2015 U/mL).
In all children aged 6–17 years, thyroid volume was determined by ultrasonography. Thyroid-lobe height, width, and depth were measured, and thyroid-lobe volume was determined by the formula of Brunn: 0.479×depth×width×height (17).
Statistical analysis
All calculations were performed with SAS v9.1.3 (SAS Institute, Cary, NC). Significance was defined as p<0.05.
Iodine status of the study sample was estimated by three different parameters: iodine concentration (μg/L), iodine/creatinine ratio (μg/g), and estimated daily iodine excretion (μg/day). Urinary iodine concentration (μg/L) is the parameter recommended by the World Health Organization (WHO) to estimate iodine status of a population (18). However, due to known possible hydration-status dependent constraints of iodine concentration (19), additionally absolute daily iodine excretion (μg/day) was estimated to correct for the actual dilution of the urine sample. The latter was calculated from the iodine/creatinine ratios measured in the spot urine samples according to a standardized calculation procedure by means of age- and sex-specific 24 hour creatinine excretion reference values (20).
The postulated associations between urinary iodine status, TSH levels, and thyroid volume were tested by three different linear regression models (Association 1: urinary iodine status and TSH; Association 2: urinary iodine status and thyroid volume; Association 3: thyroid volume and TSH). Since usual transformations (log, square root) did not improve the fit of the TSH and thyroid volume data to normal distribution, and the results of analyses using transformed data were similar to those using untransformed data, raw values were used. To test whether thyroid volume constitutes a potential mediator for the association of urinary iodine status and TSH, in a fourth regression model, both urinary iodine status and thyroid volume were included as determinants of TSH as the dependent variable. Each regression model was basically adjusted for sex, age group, and BSA. The following potential confounders were additionally selected: smoking (yes/no, only for children aged >11 years), socioeconomic status (lower SES, middle SES, upper SES) (21), BMI categories (according to age-specific percentiles of (22), P<3, P3–10, P10–90, P90–97, P>97), migrant (yes/no), geographical location (north/middle/south), region (rural, mid-sized cities, urban), time of blood sampling, time-lag of blood sampling to the last meal, and fT3/fT4 ratio. Variables changing the main predictor estimate (iodine status or thyroid volume) or associated significantly with the dependent variable (TSH or thyroid volume) were retained in the models.
All fully adjusted models were tested for potential sex or age-group interactions and, in case of an indication for a relevant interaction (p<0.1), calculations were stratified. To check further whether the investigated associations are of physiological nature and are not representing emerging autoimmune processes, we finally analyzed the distribution of TPO-Ab-positive children in quartiles of TSH levels, iodine excretion, and thyroid volume. For this special purpose, those children from the original KiGGS sample with TPO-Ab >60 U/mL (but with no other abnormalities regarding thyroid health) were again included in this specific study sample (n=6150, compare Fig. 1). We tested for linear associations between TPO-Ab and sex- and age-adjusted quartiles of TSH, iodine excretion, or thyroid volume (BSA-adjusted) by using the Mantel–Haenszel chi-square test.
Results
General characteristics of the study population are presented in Table 1. Due to the selection criteria, all thyroid parameters (fT4, fT3, TSH, and volume) were in the reference range (Fig. 1). According to the WHO parameter median iodine concentration (μg/L), the sample had adequate iodine nutrition (>100 μg/L). However, when comparing estimated iodine excretion per day (μg/day; calculated from the iodine/creatinine concentration ratio) to the estimated average requirements (EAR) (23), after considering 15% nonurinary iodine losses, >25% did not meet the recommended iodine intake values.
All values are medians (25th, 75th percentile). All comparisons of means between age groups were significant (p<0.0001, Wilcoxon Rank Sum Test).
Significantly different from the median of boys in the respective age-group (Wilcoxon Rank Sum Test).
For comparison of the EAR values with daily iodine excretion (μg/day), 15% nonrenal iodine losses were considered. Corresponding translated EAR values: 4–8 years, 55 μg/day; 9–13 years, 62 μg/day; 14–18 years, 81 μg/day.
n (%), here children are also included with TPO-Ab>60 U/mL (n=6150).
KiGGS, German Health Interview and Examination Survey for Children and Adolescents; BMI, body mass index; BSA, body surface area; EAR, estimated average requirement; fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin; TPO-Ab, thyroperoxidase antibodies.
Children with higher estimated daily iodine excretion (μg/day) had higher TSH serum levels than children with lower iodine excretion (Fig. 2). This observation was confirmed by the fully adjusted regression model showing a significantly positive association between iodine excretion and TSH levels (Table 2, Association 1). Interestingly, only urinary iodine status parameters that were corrected for creatinine excretion (i.e., μg/g and μg/day) to minimize variation due to hydration status showed this association.
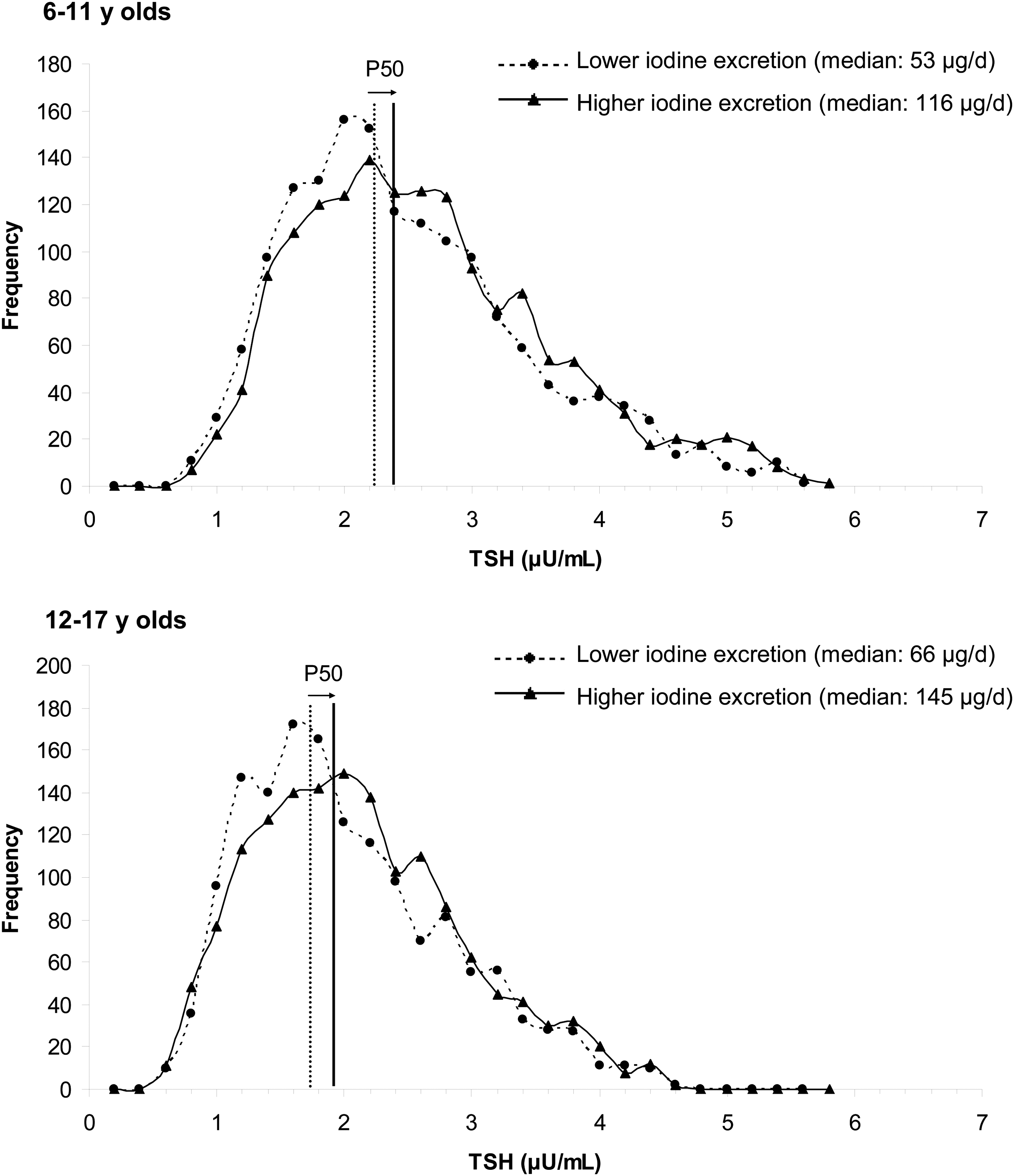
Distribution of thyrotropin (TSH) serum levels in terms of iodine status. Dotted lines: lower daily iodine excretion (<50th percentile of the population); solid lines: higher daily iodine excretion (>50th percentile).
Adjusted for sex, age group, and BSA.
Additionally adjusted for BMI categories, fT3/fT4 ratio, and time of blood sampling.
The basic linear regression model indicated a trend (p<0.1) for an inverse association between urinary iodine status (μg/L, μg/day) and thyroid volume (Table 2, Association 2; adjusted for sex, age group, and BSA). This association disappeared in the fully adjusted model (p>0.3).
The association between thyroid volume and TSH was more distinct, according to the fully adjusted regression model; a thyroid volume about 5 mL lower in 6–11 (12 –17) year old children was associated with a 0.4 (0.25) μU/mL higher TSH level (Table 3). The model was age-group stratified due to thyroid volume-by-age-group interactions.
Adjusted for sex BSA.
Additionally adjusted for age group, BMI categories, fT3/fT4 ratio, and time of blood sampling.
In the fourth linear regression model, where both urinary iodine excretion (μg/day) and thyroid volume were included as predictors for TSH, both showed significance and similar β values as in the single models (iodine excretion β=0.0005, p=0.009; thyroid volume β=−0.05, p<0.0001; data not shown).
In Table 4, the number of children (12–17 year old girls) with elevated TPO-Ab in quartiles of TSH, thyroid volume, and iodine excretion (μg/day) respectively are presented. For boys and younger girls, the number of children with elevated TPO-Ab was not sufficient to allow for a statistically reasonable analysis. In 12–17 year old girls, neither iodine excretion (μg/day) nor TSH levels were significantly associated with elevated antibody levels. Similar results have been found for iodine concentration (μg/L) and iodine/creatinine ratio (μg/g; data not shown). Significantly higher percentages of girls with elevated TPO-Ab found only for higher thyroid volumes.
Only the results for 12–17 year old girls are presented, as only in this group was the number of elevated TPO-Ab sufficient to allow a statistically reasonable analysis.
Percentage values are related to the respective total number of children in each quartile.
Quartiles of TSH and iodine excretion were calculated by age (6 years, 7 years, 8 years,…). To calculate the quartiles of thyroid volume, BSA corrected values were used. The presented medians are absolute values.
Differences between quartiles were tested with the Mantel Haenszel chi square test.
Children with TPO-Ab >60 were again included for this sub-analysis. However, they showed no other abnormalities regarding thyroid heath.
Discussion
As an integral part of the hypothalamic–pituitary feedback system, TSH is the most sensitive parameter indicating changes of thyroid function. The physiologic logarithmic relationship between TSH and fT4 explains the diagnostic power of TSH, as even a small change in fT4 (even in its reference range) will lead to an amplified change in TSH (24). The introduction of the term “subclinical hypothyroidism” (abnormal TSH, but fT3 and fT4 values still in the reference range) has led to the common practice, especially in epidemiological studies, of using TSH (above or below a certain cut-off) as the decisive parameter for the characterization of the thyroid functional state of subjects or populations (25). Accordingly, a shift in the TSH distribution of a population toward higher levels is widely considered as the first sign of underactive function of the thyroid gland. In contrast to this conventional doctrine, with the results of the present study in thyroid-healthy children, we provide a physiologic explanation for the repeatedly observed positive association between iodine intake and TSH levels. A better iodine status, which is known to be accompanied by a smaller thyroid volume (26), is dependent on a higher TSH level (within the normal range) to maintain the required thyroid hormone production.
The fact that a higher iodine intake (measured by urinary iodine excretion) is associated with a shift in TSH toward higher levels has already been observed in several epidemiological studies in adults (3,8,10,11,27,28). The underlying mechanism is so far not clear. One suggested explanation is an inhibitory effect of a higher iodine intake on different cellular thyroidal processes involved in thyroid hormone synthesis and secretion. Accordingly, it has been observed that iodine decreases the cAMP response to TSH (13). Therefore, higher TSH levels are necessary to maintain normal thyroid hormone synthesis. Another possible explanation can be deduced from an experimental study in adults in the early 1990s that investigated the short-term effects of altered iodine intake on thyroid function (29). After four weeks of iodine administration (200 μg/day) followed by four weeks of iodine depletion (3×300 mg perchlorate/day), TSH and fT4 levels were significantly diminished, whereas thyroglobulin was increased and thyroid volume was not altered. The authors suggested that the decrease in TSH serum levels was a very early sign of adaptation of the thyroid to reduced iodine levels. In line with this hypothesis, initially put forward by Studer et al. (30)—which specifically suggests a heterogeneous sensitivity of thyrocytes to TSH in euthyroidism—it is conceivable that iodine deficiency “recruits” previously (i.e., in iodine sufficiency) insensitive thyrocytes to become TSH-responding cells. That is, if iodine supply diminishes, a greater number of thyrocytes participating in thyroid function will reduce the requirement of pituitary TSH stimulation (29), or the opposite way around, a smaller number of thyrocytes in iodine sufficiency increases the requirement of TSH. Accordingly, we found a significantly positive association between urinary iodine status and TSH levels. Furthermore, an independent, inverse association between thyroid volume and TSH levels was observable in the mostly iodine sufficient KiGGS children (mediator regression, fourth model). This suggests that the thyroid gland is physiologically dependent on a higher TSH-stimulus to maintain a constant thyroid hormone output not only in the short term (i.e., indicated by higher iodine excretion), but also in the long term (i.e. with a smaller thyroid volume) (26).
It is important to highlight that we observed the positive association between iodine status and TSH levels in particularly selected thyroid-healthy children (i.e. TSH, fT3, and fT4 in the reference range; no elevated TPO-Ab; and normal thyroid volume and sonography). This fact supports the hypothesis that in this population with a median urinary iodine excretion of 88.7 μg/day, the positive association between iodine status and TSH levels mirrors a physiologic phenomenon. In addition, in this specifically selected healthy subpopulation, no relationship between TPO-Ab and serum TSH was detected. To the contrary, we found a significant association between higher thyroid volume (indicating lower iodine status) and elevated TPO-Ab. Such an association had already been observed in other epidemiologic studies (31,32). However, due to the very low prevalence of detectable TPO-Ab in children and the known fact that, at least in adults, no elevated thyroid antibodies can be measured despite cytological evidence of lymphocytic infiltration in up to 20% of individuals (33,34), our findings on TPO-Ab should be interpreted with caution.
Remarkably, the association between iodine excretion and TSH was only observable for those iodine excretion parameters that were corrected for individual creatinine excretion, that is, for all except iodine concentration. Median iodine concentration is the parameter recommended by the WHO to estimate iodine status of a population (18). Here again, some doubts arise whether the simple concentration data of iodine in urine samples not corrected for the actual dilution (urine volume, hydration status) (19,26) are really appropriate to investigate physiologic interrelations of iodine status with other thyroid-related characteristics. This probable limitation of urinary iodine concentration was indirectly confirmed by the results of the present analyses.
Thyroid size and urinary iodine excretion are the two most widely used measures for the characterization of iodine status (26). The fact that there was no explicit association between urinary iodine excretion and thyroid volume (only a trend of an inverse association in the basic regression model) has already been observed in former studies (35 –37). Because of the large day-to-day variability in iodine excretion (38) measured in spot urines, one single urine sample is rather a measure of short-term than of individual long-term iodine status. Therefore, as just recently stated by Zimmermann et al. (39), even if an individual's average daily iodine intake is adequate, on the day of the spot urine collection, iodine concentration may be below the applied cutoff. To prevent an overestimation of the prevalence of inadequate iodine intake when only considering spot urine samples (especially in populations with large variations in iodine intake), different methodologic approaches have to be applied, for example adjustment of the distribution of iodine concentration for intra-individual variation (cf. “EAR cutpoint approach”) (39). Single measurements of iodine concentration obviously do not provide direct information on thyroid function. Biomarkers more functionally related to thyroid health, such as thyroid volume, may reflect a more stable long-term indicator of iodine supply.
The interpretation of the results of epidemiologic studies investigating the impact of iodine intake on thyroid health is a very complex issue. To our knowledge, only one relevant study investigated the longitudinal association of introduction of iodized salt on thyroid health in a population (11-year follow-up) (27). After improved iodine intake, TSH levels, as well as fT4 values and TPO-Ab, were found to be increased. However, longitudinal and trend studies covering a long study period often have to face the problem that the analytical methods change and more sensitive methods for analysis of the more current samples are used. For example, the change from microsomal Ab to TPO-Ab during the second half of the 1990s (40) seemingly increased the prevalence of TPO-Ab also in populations with constant iodine supply such as Japan (41,42). Another example is a prospective study conducted in Denmark (28), in which the authors state that it cannot be excluded that part of the observed increase in incidence of hypothyroidism after increased iodine intake is caused by a higher diagnostic alertness.
One study in China compared the development of thyroid health with a 5-year follow-up between three regions with different iodine intakes: mildly iodine deficient, more than adequate iodine intake, and excessive iodine intake (8). Although they only found an increased cumulative incidence of subclinical but not overt hypothyroidism (i.e., simply more cases with higher TSH, above a fixed, not iodine-adjusted upper TSH reference value) in the population with the highest iodine intake, the authors concluded that more than adequate iodine intake may lead to hypothyroidism. When comparing the initial mean TSH levels in these three different populations (1.15, 1.28, and 1.93 mU/L respectively; p=0.000) (43) already notable differences appeared. Therefore, the use of the same fixed TSH reference range to determine hypothyroidism in the three studied populations seems inappropriate, especially in the light of the known inverse linear correlation of log TSH and fT4 (24). The use of TSH as single criterion to determine hypothyroidism is also questioned by a study in Moroccan school children, showing 18% of children having total T4 values below 65 nmol/L despite a mean TSH of <1 mU/L (44). The comparability of TSH levels between different populations (10,11,45) is finally hampered by the strong dependency of TSH distribution on several factors that are independent of current iodine status such as age, body fatness, preceding iodine nutrition, iron or selenium status (46,47), use of thyroid hormone, or sensitivity of TSH assays (48). Moreover, the TSH adaptation to changed iodine intake seems to occur with some delay. Accordingly, in the Moroccan study in school children (44), TSH was not altered during the year following introduction of iodized salt, despite a significant increase in total T4. For conclusions on the effects of higher iodine intakes on thyroid health, there is a need for more evidence-based analyses.
In conclusion, according to our results, the repeatedly observed shift of the TSH-distribution toward higher levels following improved iodine supply (27)—and therefore a higher number of subjects above a fixed upper TSH reference value—should not readily be interpreted as a higher risk for (subclinical) hypothyroidism. Better iodine nutrition obviously requires higher normal TSH levels to maintain a certain thyroid hormone secretion—because of the smaller thyroid volume and the decreased sensitivity of the gland to TSH. Therefore, an adequate estimation of the prevalence of hypothyroidism (subclinical or manifest) is only possible when the applied TSH reference values are adapted to the populations' iodine status and further parameters of thyroid function (thyroid hormones, thyroid autoantibodies, thyroid ultrasound) are carefully examined. The present results therefore shed some light on the ongoing and quite complex discussion on the effects of iodine nutrition on thyroid health and may help to eliminate doubts about the safety of WHO-based iodine fortification measures.
Footnotes
Acknowledgments
The present examination was financially supported by the German Federal Ministry of Food, Agriculture and Consumer Protection (BMELV) through the Federal Office for Agriculture and Food (BLE), grant number 2812HS014.
Author Disclosure Statement
No competing financial interests exist.