
Abstract
Background:
Although 20–50% of papillary thyroid carcinoma (PTC) patients initially present with lymph node metastases, prognosis is excellent. Thus, the significance of lymph node metastasis in PTC remains controversial. In this study, we examined the impact of extranodal extension to surrounding organs (invasive extranodal extension) on the prognosis for PTC patients.
Methods:
Medical records of PTC patients who underwent surgery as their initial treatment at our institution between 1981 and 2008 were retrospectively reviewed. Patients with or without invasive extranodal extension were selected. Our therapeutic strategy for PTC with invasive extranodal extension included complete resection and functional reconstruction. Intergroup comparison was performed using Student's t-test or the chi-square test as appropriate. Survival curves determined by the Kaplan–Meier method were compared for statistical significance using the log-rank test. A Cox-hazard regression model with the forward stepwise method was used for multivariate analysis.
Results:
The study cohort included 60 (12.3%) patients with and 428 (87.7%) without invasive extranodal extension. The most common site of invasive extranodal extension in the central neck compartment was the recurrent laryngeal nerve, whereas the internal jugular vein was the most frequently invaded site in the lateral neck compartment. The locoregional recurrence rate did not differ significantly between patients with and without invasive extranodal extension, but the distant recurrence rate was higher for those with invasive extranodal extension. The 10-year disease-specific survival rate was significantly lower for patients with invasive extranodal extension than for those without invasive extranodal extension. Furthermore, multivariate analysis revealed that being aged ≥45 years, poor differentiation, and extrathyroidal extension were independent predictive factors for disease-specific death in PTC. Invasive extranodal extension had no effect on the survival of PTC patients.
Conclusions:
Invasive extranodal extension did not affect the survival of patients with PTC. Despite a negative impact on distant recurrence, invasive extranodal extension did not affect locoregional recurrence in PTC patients.
Introduction
D
Subsequent studies have identified several clinicopathologic indicators that might predict the prognosis and recurrence in patients with PTC. Overall, the presence of cervical LN metastases in PTC is considered to influence recurrence, but its impact on survival remains uncertain.
In this study, we investigated the impact of extranodal extension to the surrounding organs (invasive extranodal extension) on the prognosis of patients with PTC.
Materials and Methods
The charts of PTC patients who underwent surgical treatment at the Kyoto Medical Center and Kusatsu General Hospital between 1981 and 2008 were retrospectively reviewed. Patients with or without invasive extranodal extension were selected. Data on patient characteristics were collected for each group, and these were compared between groups. The invasive extranodal extension location was used to classify patients into two groups: the central compartment group and the lateral compartment group.
We examined the characteristics of the invaded organs in each group. The preoperative prognostic factors evaluated in this study included patient age, sex, the presence or absence of extrathyroidal extension and invasive extranodal extension, tumor differentiation, and the presence of distant metastasis prior to initial treatment.
Our therapeutic strategy for PTC with invasive extranodal extension was complete resection and functional reconstruction. Curative resection was performed with the aid of an operating microscope if necessary. Multiple margin samples were sent for frozen section analysis to pathologically confirm negativity during the operation. If the result was positive, additional resection was performed until negativity was achieved. Intraoperative cryosection analysis made it possible to preserve as much of the normal tissue adjacent to the tumor as possible and to improve functional outcomes. The surgical management for invasive extranodal extension is described in Table 1.
LN, lymph node; RLN, recurrent laryngeal nerve.
Invasive extranodal extension was defined as follows: intraoperative findings indicating that the organ had gross invasion by LN metastasis, or intraoperative cryosection analysis showing LN metastasis to the organ. Extrathyroidal extension was defined as invasion of the larynx, trachea, esophagus, recurrent laryngeal nerve (RLN), mediastinal vessels, or carotid artery from the thyroid primary tumor site, but not invasion of the sternothyroid or sternohyoid muscle.
The hospital review board approved this study. Patients' privacy was strictly maintained, and informed consent was obtained.
Groups were compared using Student's t-test or chi-square test as appropriate. A p-value of <0.05 was considered significant.
Survival curves, determined using the Kaplan–Meier method, were compared for statistical significance using the log-rank test, and a Cox-hazard regression model with the forward stepwise method was used for multivariate analysis. A p-value of <0.05 was considered statistically significant. Commercially available software (Ekuseru-Toukei 2012; SSRI Co., Ltd., Tokyo, Japan) was used for all statistical analyses.
Results
During the study period, 488 PTC patients underwent primary thyroid surgery. The study cohort included 114 men (23.4%) and 374 women (76.6%). Their mean age at the initial treatment was 51 years (range 9–92 years). The mean±standard deviation (SD) follow-up period after surgery for surviving patients was 10.5±7.1 years.
Sixty (12.3%) patients with and 428 (87.7%) without invasive extranodal extension were enrolled. The patients with invasive extranodal extension were older than those without invasive extranodal extension (p=0.0368) and had a higher frequency of LN metastases in the lateral neck (N1b; p<0.0001). There were no significant differences in other parameters, as shown in Table 2.
p=0.0368; ** p<0.0001.
SD, standard deviation.
The invaded organs were classified according to their location in the central neck compartment or lateral neck compartment. In the central neck compartment, the RLN was most frequently infiltrated by invasive extranodal extension, followed by the trachea and esophagus. In the lateral neck compartment, the internal jugular vein was the most frequently invaded of the cervical veins, followed by the subclavian and brachiocephalic veins, which were partially resected and treated with angioplasty. Of the cervical arteries, six common carotid arteries and one vertebral artery were invaded. The former were all preserved by resecting the adventitia with LN metastasis, while the vertebral artery was transected and reconstructed using an artificial vessel. Of the cervical nerves, the vagal nerve was the most frequently invaded, followed by the spinal accessory nerve. Both these nerves were invaded in the level II node compartment (Table 3).
IJV, internal jugular vein; SAN, spinal accessory nerve.
Preoperative RLN paralysis by invasive extranodal extension was detected in 12 nerves (40%), whereas RLN paralysis by extrathyroidal extension was detected in 60 nerves (63.2%). The difference in preoperative RLN paralysis between the two groups was significant (p=0.0253; Table 4).
A significant difference was observed between the two groups (p=0.0253).
The locoregional recurrence rates for patients with and without invasive extranodal extension were 8.3% and 6.5% respectively, although this difference was not significant. However, the distant recurrence rate for patients with invasive extranodal extension was higher than that for patients without invasive extranodal extension (Table 5).
p=0.0147; # p=0.808.
A comparison of the prognosis for patients with and without invasive extranodal extension indicated that the 10-year disease-specific survival was shorter for patients with invasive extranodal extension than for those without, and this difference was significant (p=0.0201; Fig. 1).
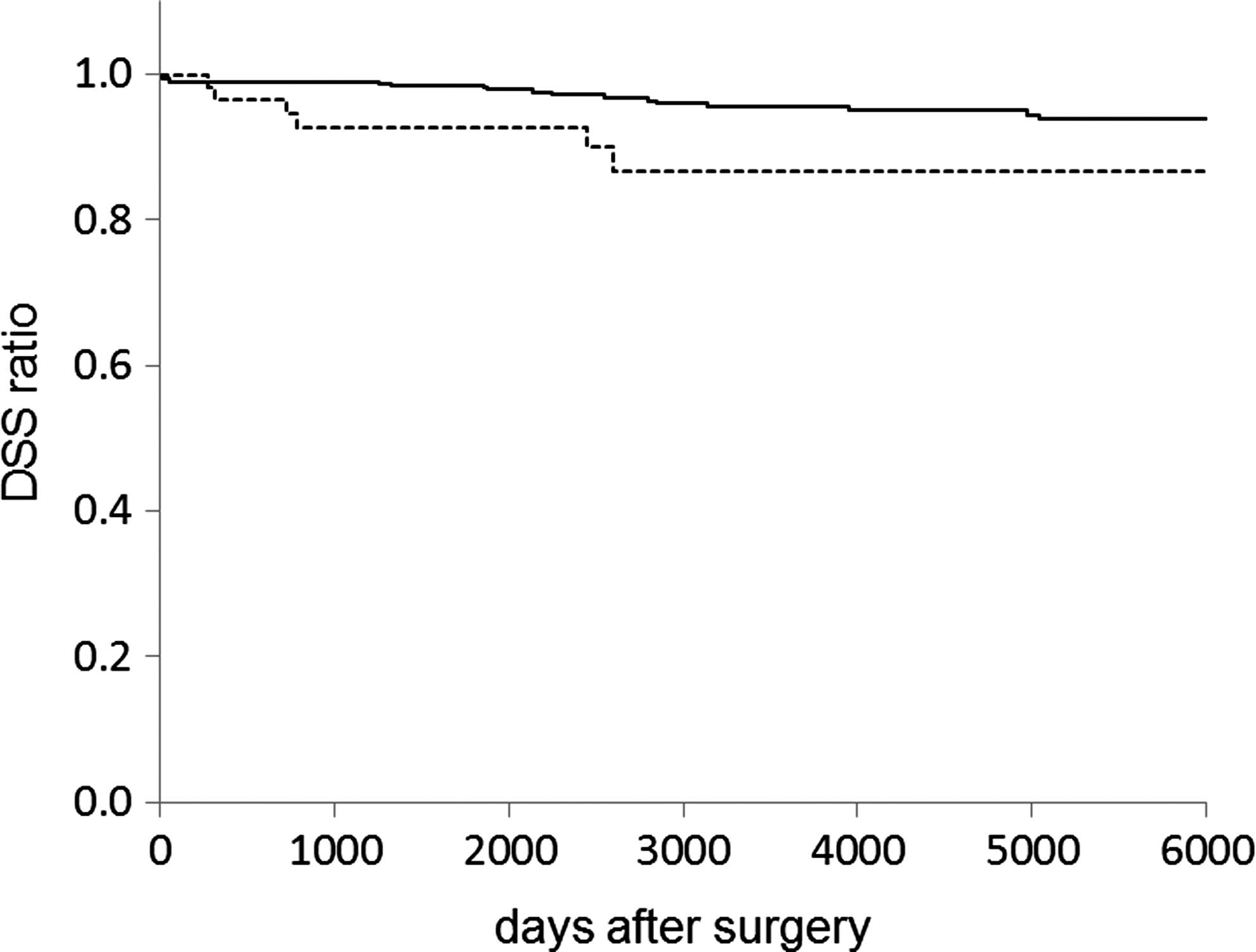
Comparison of disease-specific survival (DSS) rates between patients with or without invasive extranodal extension. The 10-year DSS rates for patients with (solid line; n=60) and without (dotted line; n=428) invasive extranodal extension were 86.8% and 95.6% respectively, as determined using the Kaplan–Meier method (p=0.0201).
For all 488 PTC patients who underwent primary thyroid surgery, being aged ≥45 years, poor differentiation, and extrathyroidal extension other than invasive extranodal extension were significantly associated with reduced disease-specific survival.
Multivariate analysis was performed for the preoperative prognostic factors that were deemed significant by univariate analysis (Table 6). The results indicate that being aged ≥45 years, poor differentiation, and extrathyroidal extension were independent predictive factors for disease-specific death due to PTC, but invasive extranodal extension had no impact on the survival of patients with PTC.
CI, confidence interval.
Discussion
In this study, we found that invasive extranodal extension did not affect the survival of patients with PTC. Despite a negative impact on distant recurrence, invasive extranodal extension did not affect locoregional recurrence in PTC patients. Although LN metastases are common in PTC patients, they appear to have little influence on survival according to traditional prognostic schemas. Subsequent studies on the impact of LN metastasis on the survival of PTC patients indicated that large nodal metastases (≥3 cm) in older patients (≥50 years of age), extranodal invasion, LN involvement in patients ≥45 years of age, LN metastases (N1 status) with T1–T3 status, N1b status with a carcinoma of ≤3.0 cm, a ratio of metastatic LNs to total LNs of ≥0.42, and lateral/mediastinal cervical involvement in patients ≥45 years of age were associated with a poor prognosis (2,3,7 –11).
With regard to the effect of LN metastasis on recurrence, extracapsular spread, lymphovascular invasion, and nodal involvement in older patients aged ≥45 years, a high LN ratio (>0.4) and the presence of macrometastases (>0.2 cm), node metastases of >3 cm, an elevated total ratio of positive to total nodes, an elevated central LN ratio, and the presence of three or more metastatic nodes are reported to be associated with recurrence (12 –18).
In the central compartment, the RLN was the most frequently infiltrated organ by invasive extranodal extension, and it was characterized by a lower frequency of RLN paralysis than that associated with extrathyroidal extension. It can be difficult to identify many cases of RLN infiltration by invasive extranodal extension because of the low frequency of RLN paralysis and the low sensitivity of ultrasonography and computed tomography in cases of central neck compartment involvement (19 –23). Recently, intraoperative nerve monitoring (IONM) data have proved useful for prognosticating postoperative RLN function. Additionally, intraoperative electrophysiological activity is thought to provide information on RLN viability and persistent function of RLN invaded by thyroid malignancy (24). Thus, IONM for RLN invasion, especially in cases of RLN invasion by invasive extranodal extension, might help improve vocal cord function.
In the lateral neck compartment, the mean size of LNs with invasive extranodal extension was 35 mm. It has previously been reported that large LN metastases (≥3 cm) affect disease prognosis and recurrence. However, in other studies, the relationship between large LN metastasis and extranodal extension has not been confirmed (9,18). Although these later studies examined prognosis or recurrence according to the size of the metastatic LN, the LN size in the previous investigation was approximately equal to that in our study, in which we examined the correlation between invasive extranodal extension and prognosis or recurrence. However, in our study, invasive extranodal extension did not affect the prognosis or recurrence of patients with PTC.
In patients with pathologically proven cervical LN metastases (pathological N1 disease), the median risk of locoregional LN recurrence is reported to vary markedly according to the initial clinical staging, with recurrence rates of 2% (range 0–9%) for patients with clinical N0 disease compared with 22% (range 10–42%) for those with clinical N1 disease. In addition, the presence of extranodal extension is reported to be associated with a median risk recurrence of 24% (range 15–32%). The presence of extranodal extension thus resulted in an increased risk of recurrence (25).
On the basis of previous reports, we hypothesized that invasive extranodal extension would strongly affect the survival or recurrence of patients with PTC. However, our study did not identify invasive extranodal extension as a poor prognostic factor for PTC. Most fatalities were attributable to distant metastasis, while locoregional recurrence did not account for any of the fatalities. The locoregional recurrence rates with or without invasive extranodal extension were similar in our study. The locoregional recurrence rate with invasive extranodal extension in our study was lower than that in previous studies. We attribute the low rate of locoregional recurrence in our patients to the surgical approach adopted, wherein pathologically negative margins were confirmed by frozen section analysis, which reduces the risk of incomplete resection, while attempts were made to preserve as much adjacent healthy tissue as possible. For successful resection therefore, intraoperative cryosection analysis should be liberally used to confirm margin negativity.
External beam radiation therapy was not administered for patients after surgery for invasive extranodal extension. Unfortunately, distant metastasis frequently occurred, even in patients with good locoregional control, and became a leading cause of death. As such, we suggest that preventive radioiodine ablation therapy should be considered in patents with invasive extranodal extension.
In conclusion, invasive extranodal extension did not affect the survival of patients with PTC in this study. Despite a negative impact on distant recurrence, invasive extranodal extension did not affect locoregional recurrence in PTC patients.
Footnotes
Author Disclosure Statement
The author declares that no competing financial interests exist.