
Abstract
Background:
Thyroid hormone (TH) is essential for the developing brain, and because the fetal thyroid develops relatively late in gestation, the maternal TH supply is critical for fetal brain development. However, if the mother has hypothyroidism during pregnancy, fetal brain and neuropsychological development may be compromised. Rodents experiencing maternal TH insufficiency show abnormal corpus callosum (CC) morphology, but it is not known if children born to women treated for hypothyroidism (HYPO) show similar effects. The purpose of the current study was to investigate HYPO for CC morphology and morphometry and to determine whether any specific CC abnormalities were associated aspects of maternal hypothyroidism and were correlated with reduced neuropsychological functioning in the children.
Methods:
ANALYZE software was used to trace CCs in archived magnetic resonance imaging scans from 22 HYPO and 22 matched controls. Areas of two sub-regions and six segments and different shape metrics (angles, lengths, ratios) were determined. CC parameters were correlated with maternal thyrotropin (TSH) values and number of hypothyroid trimesters as well as the child's neuropsychological test performance.
Results:
HYPO showed a smaller anterior CC and genu and larger posterior CC and splenium areas than controls as well as shape abnormalities in genu and splenium. Results were correlated with the duration of maternal hypothyroidism. Executive function skills were positively associated with genu size in HYPO, while verbal comprehension skills were negatively associated with splenium and overall posterior CC sizes.
Conclusions:
Maternal hypothyroidism contributes to CC abnormalities in the offspring, and effects differ for anterior versus posterior CC regions.
Introduction
T
In the human brain, the need for TH begins very early in gestation, as evidenced by the presence of TH and TH receptors in the first trimester (9,10). Since the fetal thyroid matures relatively late and does not achieve full function until near term, placentally transferred TH from the mother serves all fetal brain needs in early gestation and a supplementary role later. However, if the mother has hypothyroidism, hypothyroxinemia, or subclinical hypothyroidism, her TH contribution to the fetus will be insufficient and the child may have a suboptimal outcome. Indeed, studies of the offspring of these women show reduced IQs (11), memory and attention difficulties (12,13), behavioral and regulatory problems (14), and school underachievement (12). Recent magnetic resonance imaging (MRI) studies also indicate a smaller than normal hippocampus and abnormal cortical morphology (15,16), but their CC has not been studied.
The human CC is comprised of six segments (see Fig. 1), each with a distinct developmental trajectory that begins in early gestation (17). Anterior CC regions, which include the genu and anterior and posterior midbodies and connect with the superior frontal, supplementary premotor, and primary motor cortices, respectively, start to develop at 14–16 weeks of gestation (17). Next to develop at about 18–19 weeks of gestation are the posterior CC sub-regions, namely the isthmus and splenium, which connect sensory cortex and parietal, temporal, and occipital cortical regions (18,19). The rostrum, which is inferior to the genu and connects corresponding regions of the orbitofrontal lobes, forms last around midgestation (17). Notably, these times are when the fetal brain is under maternal TH control.
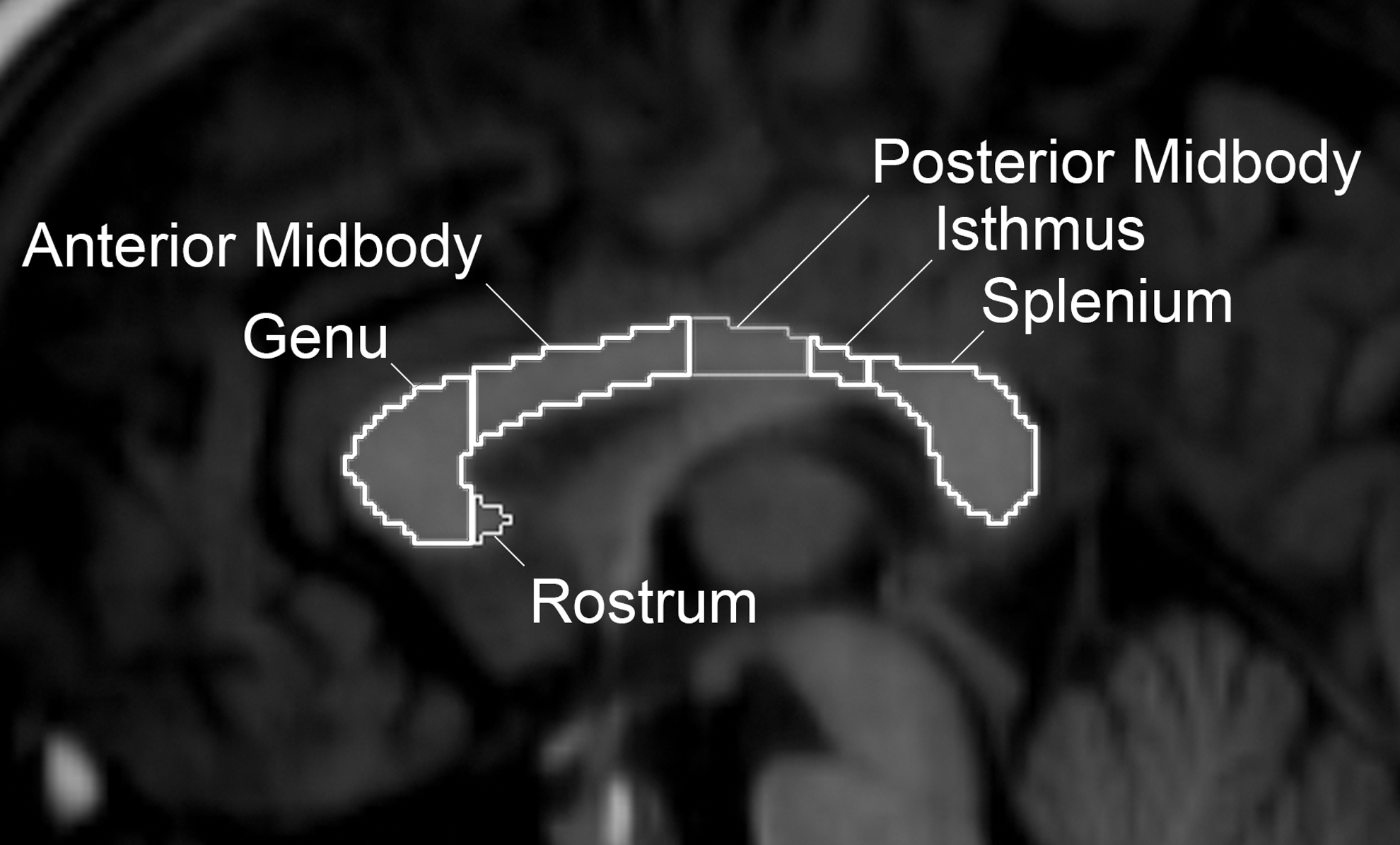
Corpus callosum (CC) segments on the mid-sagittal magnetic resonance imaging (MRI) view.
In light of recent studies showing CC abnormalities in pediatric conditions such as autism (19) and ADHD (20), which are both coincidentally increased in children exposed to maternal hypothyroidism (14,21), the current study investigated (a) whether CC morphology is abnormal in children born to women treated for hypothyroidism during pregnancy (HYPO); (b) if this reflects the severity and duration of their mothers' hypothyroidism; and (c) whether, in HYPO, CC abnormalities and specific neuropsychological weaknesses are linked.
Methods
Participants
Participants were 44 individuals aged 9–14 years (M=10.6 years; SD=0.78 years; 68.2% male) derived from a cohort born between 1996 and 2001 and followed since infancy. The current sample represents approximately one third of subjects from the original cohort and did not differ from non-participants in maternal or other background factors.
The HYPO group included 22 children whose mothers were diagnosed de novo during pregnancy (17%) and so underwent a brief period of hypothyroidism or who were treated for hypothyroidism that predated pregnancy but had not had an increment in thyroxine dosage during pregnancy (83%). All women were recruited during or right after pregnancy by local endocrinologists and obstetricians or from the Motherisk program at The Hospital for Sick Children (SickKids), an antenatal counseling service for prenatal medication exposures including L-thyroxine (L-T4). Table 1, which presents trimester-specific thyrotropin (TSH) values, shows a broad range of values. Six women (27.3%) were hypothyroid for one trimester only, 10 (45.5%) for two trimesters, and four (18.2%) for all three trimesters, while two (9.1%) on L-T4 had normal TH levels throughout pregnancy. In these women, the mean daily pregnancy dose of L-T4 was 105±39 μg (range 50–200 μg).
TSH upper normal values were 2.5 mIU/L for the first trimester, 3.0 mIU/L for the second trimester, and 3.5 mIU/L for the third trimester.
10 individuals were missing values for first and second trimesters, and 13 were missing values for the third trimester.
HYPO, hypothyroidism; TSH, thyrotropin; fT4, free thyroxine.
Controls were 22 normally developing children also followed since infancy. Their mothers were recruited via posters displayed in offices of local endocrinologists and obstetricians or from the Motherisk database of women with no known teratogenic exposure. A small subset of women was also recruited directly by one obstetrician who measured her patients' TH levels at the first prenatal visit and determined these women were euthyroid. Even though TH levels in pregnancy were unavailable for the remaining women, all reported never being treated for hypothyroidism throughout the course of their child's follow-up. The current sample of controls was selected from a larger group and matched for age (within six months), sex, and socioeconomic status (SES) with individual HYPO cases.
Procedures
Data were acquired from a larger study of TH and memory (15). In this study, children on day 1 received a four-hour test battery assessing intelligence, reading, memory, attention, and aspects of executive functioning, and on day 2, approximately one week later, they underwent MRI scanning. Parents, while their children were being tested, concurrently completed questionnaires. The SickKids Research Ethics Board approved all procedures.
Neuropsychological tests
Intelligence was assessed using the Vocabulary and Matrix Reasoning subtests of the Wechsler Abbreviated Scale of Intelligence (WASI), and reading was assessed with the Wide Range Achievement Test-3 (WRAT-3) Reading subtest. The complete Test of Memory and Learning (TOMAL), copy and delayed recall conditions of the Rey–Osterrieth Complex Figure task (ROCF), and Dot Locations and Stories subtests of the Children's Memory Scale (CMS) were used to assess memory. Attention and executive functioning were assessed with the Map Mission and Score DT subtests of the Test of Everyday Attention for Children (TEACh), and Rapid Visual Information, Spatial Working Memory, and Stockings of Cambridge subtests of the CANTAB.
Parent questionnaires included: (a) a demographic history checklist on the child's birth and developmental history, current health, school status, family history, and family background (for computing SES); (b) the Behavioral Rating Inventory of Executive Function (BRIEF), an 86-item questionnaire evaluating eight aspects of executive function (e.g., shift, inhibit, working memory, planning); and (c) the Everyday Memory Questionnaire (EMQ), a 28-item rating scale of children's everyday memory difficulties.
Image acquisition, preprocessing, and morphological analysis of CC
Structural images were obtained on a 1.5 Tesla GE Signa scanner using a 3D-FSPGR (IR prep Zip X2) T1-weighted series in the axial plane (TR=10.37 ms, TE=4.26 ms, TI=400 ms, flip angle=20°, field of view=240 mm, slice thickness=1.50 mm, no gap). Preprocessing involved extracting brain from skull and cerebral spinal fluid and then normalizing the extracted brain in standard space using anterior and posterior commissure alignment, as is standard in neuroimaging analyses.
Scans were examined in ANALYZE 9.0, and a subtle increase in contrast was used to facilitate white-matter recognition. The following landmarks were identified in the mid-sagittal slice: aqueduct of sylvius, third ventricle, and interhemispheric fissure. ANALYZE's Region of Interest (ROI) tool was used to manually trace the CC in the sagittal view; coronal and axial views were used for confirmation. The intracranial area (ICA), defined as the cross-sectional area of the brain in the mid-sagittal slice excluding the cerebellum and brainstem, was also measured.
The morphometric analysis was based on a modification of Hofer and Frahm's system (18), originally derived from their diffusion tensor imaging (DTI) fiber tractography findings (Fig. 2A). This system identifies five CC segments that project to distinct cortical areas; the current modification involved also including the rostrum. Initially, a horizontal line was extended between vertical tangents at anterior-most and posterior-most ends, and the resulting region was partitioned into halves, thirds, and quarters (Fig. 2B). Within the posterior half, the posterior-most quarter signified the splenium, while the region within the posterior-most third minus the splenium signified the isthmus; the remaining region after removing both splenium and isthmus was the posterior midbody. Within the anterior half, a vertical line drawn at the anterior border of the septum pellucidum (SP, ∼1/6 CC) served to designate the genu as the part anterior to the line and the rostrum as the part posterior to the line and inferior to the SP; the anterior midbody was the remainder posterior to the line and superior to the SP. Based on knowledge about the developmental timing of different CC segments (22), the genu, anterior midbody, and posterior midbody were assigned to the anterior CC subregion, and the isthmus and splenium to the posterior CC subregion; the rostrum was not included in this designation. Areas of the six individual segments and the anterior/posterior sub-regions were measured within ANALYZE. A second individual also performed tracings on a subset of scans and obtained an inter-rater reliability of 0.97 with the main analyst. Both analysts were masked to subject group, age, and sex.
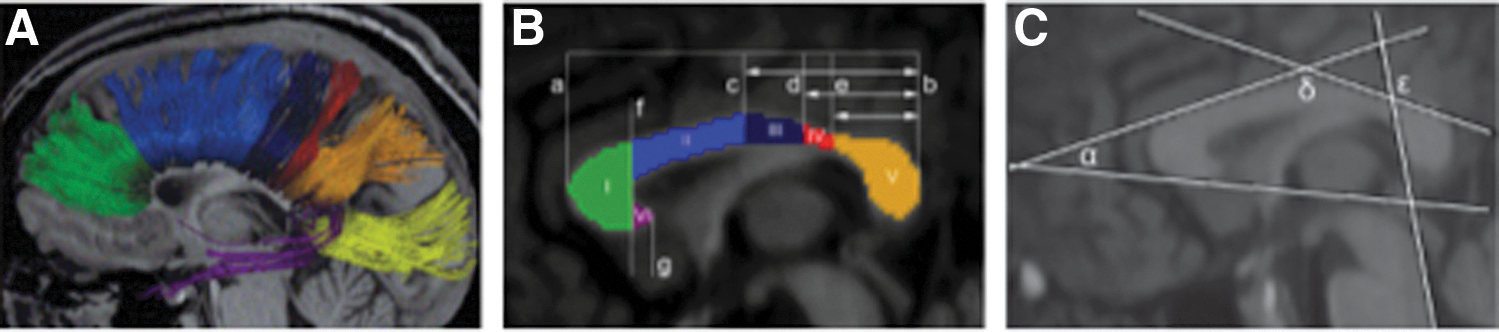
CC connections and measurement methods. (
The method of Gabrielli et al. (23) was used to characterize aspects of CC shape. First, four tangent lines were drawn (Fig. 2C): one from the anteroinferior surface of the genu through the anterior commissure; a second at the anterosuperior surface of the anterior midbody; a third at the posterosuperior surface of the isthmus; and a fourth along the floor of the fourth ventricle. Different line pairs were connected to form the following three angles: (a) “α” between the first two lines reflecting genu bulbosity; (b) “δ” between the second and third lines reflecting CC curvature; and (c) “ɛ” between the third and fourth lines reflecting splenium orientation. Genu and splenium plumpness/skinniness were also determined by computing the ratios between their respective heights (lengths) and widths.
Statistical analysis
All data were analyzed using IBM SPSS Statistics for Windows v21 (IBM Corp., Armonk, NY). t-Tests and chi-square tests were used to compare groups for demographics and intracranial and total CC areas. Separate multivariate analyses of covariance (MANCOVA) with ICA as the covariate were used to examine group differences in areas of CC subregions or segments as well as linear measurements and angles. Proportional CC areas determined by calculating ratios between segment area and total CC area were analyzed via multivariate analyses of variance (MANOVA). Similarly, neuropsychological test data were analyzed by separate MANOVAs for each test. For MANCOVA and MANOVA, both omnibus (across all effects) and univariate results are reported. Effect sizes (η2) were determined for each analysis. Only cases whose mothers had at least one abnormal TSH value in pregnancy were included in this set of analyses, since the two women who were euthyroid throughout gestation despite no increase in treatment were not technically hypothyroid in pregnancy.
Within the HYPO group, trimester-specific maternal TSH values were correlated with CC measures. The entire HYPO sample was included in these analyses (including those with normal TSH throughout pregnancy) in order to examine the full range of effects. To assess duration of hypothyroidism, the HYPO group was subclassified by the number of trimesters involving an elevated maternal TSH level based on trimester-specific reference ranges; for example, mothers first diagnosed in the second trimester of this pregnancy were considered to have two trimesters with TSH elevations, and mothers who were euthyroid throughout pregnancy were assigned a score of zero. These values were entered into linear regression analyses to predict size of each CC sub-region and segment. To determine structure–function relationships, correlations were performed (within the HYPO group only) between specific sub-region or segment ratio values and neuropsychological test scores.
The p-value was set at 0.05 for group comparisons and at 0.01 for correlations with TSH levels. Because of the large number of neuropsychological test indices, the critical p-value for these correlations was set at 0.001. Given the exploratory nature of the study, a few near-significant trends are also mentioned (e.g., p<0.10 for group comparisons and p<0.05 for correlations).
Results
Table 2 presents the groups' demographic data. They did not differ in age, sex, SES, handedness, IQ, or ICA.
Results expressed as mean±standard deviation; groups do not differ on any variable.
Table 3 provides area and ratio measurements for CC subregions and segments. These data were analyzed via MANCOVAs (area measurements) and MANOVAs (ratio measurements). Although groups did not differ in ICA, this was included as a covariate in the MANCOVA given its strong correlation with total CC area (p=0.004). Although HYPO and control groups did not differ in their area values, it was found that when ratio data were used, significant differences were seen for both sub-regions and segment values. For sub-regions, a near-significant omnibus group effect (p=0.059, η2=0.135) reflected significantly smaller anterior (p=0.019, η2=0.130) and larger posterior sub-regions (p=0.018, η2=0.132) in HYPO. For individual CC segments, a significantly larger splenium ratio was observed (p=0.045, η2=0.097) in HYPO who also had a smaller genu, at a trend level (p=0.059, η2=0.086), than controls. Groups did not differ in size of the other segments or in their linear or angle measurements (Table 4).
Does not include the two cases whose mothers had normal TSH values throughout pregnancy.
Adjusted for total CC area.
CC, corpus callosum.
Does not include the two cases whose mothers had normal TSH values throughout pregnancy.
No significant correlations were obtained between CC indices and trimester-specific maternal TSH values. However, when children were classified by the number of trimesters (zero to three) in which their mothers' TSH levels were elevated, results revealed an effect for the genu (b=−0.45, t(22)=−2.26, p=0.035), with TSH explaining 20% of variance in its area. This suggests that for mothers with a longer period of TH insufficiency, their children's genua were smaller. Within the entire anterior sub-region, the number of hypothyroid trimesters also significantly predicted its reduced size (b=−0.44, t(18)=6.53, p=0.054) accounting for 44% of variance in its area (Table 5). Although no effects were observed for shape indices, children exposed to more hypothyroid trimesters tended to have more bulbous genua (α-angle; p=0.07).
CI, confidence interval.
For the different neuropsychological tests, separate MANOVAs indicated significant between-group differences on the BRIEF Emotional Control subscale (p=0.03) and on the EMQ (p=0.007) and at a trend level (p=0.07) on the BRIEF Working Memory scale. These results reflected the higher scores (i.e., more problems) by HYPO than controls. HYPO also tended to have poorer reading ability than controls (p=0.07; Table 6).
Does not include the two cases whose mothers had normal TSH values throughout pregnancy.
T-score: mean=50, standard deviation=10; standard score: mean=100, standard deviation=15.
Score represents the square root of the sum across all ratings.
Table 7 shows the significant correlations between CC sub-region and segment values and neuropsychological test results for the HYPO group. Those with larger genua had fewer problems on the BRIEF Shift subscale, while those children with plumper genua (larger width:height ratios) scored higher on Rey-O Delay and TOMAL Object Recall, Paired Recall, and Verbal Memory Index. Children with smaller splenium ratios scored higher on the WASI Vocabulary subtest, while children with wider and shorter splenia scored higher on TOMAL Digits Forward and Backward, Paired Recall, and Abstract Visual Memory. Further, those with smaller ɛ-angles (i.e., more upright splenia) performed less well on the TOMAL Visual Sequential Memory subtest. Finally, those with a larger posterior midbody showed more initiative (lower BRIEF Initiate scores) and better narrative recall (higher CMS Delayed Story Recall scores).
Higher scores on BRIEF test indicate more problems in the corresponding subtest category.
Higher scores Rey, WASI, TOMAL, and CMS indicate better performance in the corresponding subtest category.
Discussion
The present study found that insufficient maternal TH during pregnancy affects the development of specific CC sub-regions in the offspring. Relative to children born to women with normal thyroid function throughout pregnancy, it was found that children whose mothers underwent a period of TH deficiency in pregnancy due to de novo diagnosis or to inadequately treated pre-existing hypothyroidism had smaller anterior and larger posterior CCs. These changes consist of a smaller genu and a larger splenium size. The CC shape was generally unaffected. Although CC morphometry and morphology indices were not correlated with average maternal TSH levels within a single trimester, an association was observed between the duration of the maternal hypothyroidism and CC morphometry. Specifically, children from women who were hypothyroid for more than one trimester had smaller genua and anterior CCs and larger splenia than did children whose mothers were hypothyroid for a shorter duration. Also within the HYPO group, genu and splenium size and certain shape features were correlated with a number of the neuropsychological test indices.
Since the advent of MRI for research and use of advanced analytical procedures, much interest has been garnered for studying the CC, possibly because this is the most detectable structure within the brain and it can be severely malformed or even missing in certain pediatric populations (24). Furthermore, there is a substantial literature showing that adults with callosal transections have distinct cognitive, social, and emotional deficits (25). Importantly also, findings from animal, histological, and recent MRI studies show that the CC undergoes major development in a non-uniform (17,24) and bidirectional (26) fashion during pregnancy. In animals, callosal development involves a period of exuberant axonal growth followed by axonal pruning in late gestation and myelination of axons postnatally (22). Indeed, this period of exuberant connections is thought to play a significant role in cortical evolution (27). Furthermore, in primates, the axonal properties underlying the complex system of intercommunication with specific regions of the cortex has been found to reflect the specific geometries of the callosal and cortical regions with which they connect (28). Also, populations suffering from psychiatric disorders show CC shape abnormalities (29,30), while preterm infants and children with traumatic brain injury or autism show increased or decreased CC size overall or within selective regions (31,32). The present findings indicating that offspring of hypothyroid women had smaller than normal genua and larger than normal splenia are novel and suggest that the human CC is indeed vulnerable to TH insufficiency during pregnancy.
Rodents with early TH deficiencies exhibit CC abnormalities that reflect atypical topography of callosal projections (7), reduced number and abnormal maturation and myelination of axons (6 –8), and malformations of the CC itself (33). The present findings of CC abnormalities in humans, particularly children who experienced longer periods of gestational TH deficiency, suggest TH insufficiency is the likely culprit. However, it was not possible to pinpoint when within individual trimesters the specific effects occurred, since most women were receiving some (albeit inadequate) treatment or were treated soon after experiencing symptoms (in de novo cases). Nevertheless, the observation of strongest effects in children exposed to TH insufficiency during the third trimester suggests (based on animal evidence) that this may be due to reduced callosal sprouting in the genu and reduced pruning in the splenium (34). Furthermore, the findings also suggest that to exert an effect, the impact of TH loss may be cumulative, since correlations were not shown with averaged TSH values for each trimester.
The present findings also indicate a plumper genu in HYPO than controls, while observed genu abnormalities were correlated with increased difficulties in shifting attention. Since the genu contains fibers connecting homologous frontal lobe regions that play a role in aspects of executive functioning, particularly attention, the current findings offer a mechanism as to why HYPO have specific executive function difficulties. Interestingly, research from the Generation R study shows children exposed to maternal hypothyroxinemia have an increased risk of autism, which may reflect specific executive-function difficulties (14).
The larger than normal splenium in the HYPO group may reflect an abnormality in the pruning process that typically follows exuberant axonal growth (35) and is disrupted by exposure to hypothyroidism in rodents (34). Splenium size was also observed to be inversely correlated with WASI Vocabulary performance, signifying maternal TH insufficiency may have a negative impact on language comprehension and expression. Since the splenium has crossing fibers from occipital, parietal, and temporal lobes, some of which are involved in the formation and storage of language information (e.g., Wernicke's area), the present findings suggest this may be a possible neural substrate for the observed verbal weaknesses in HYPO (36). Furthermore, given that splenium enlargement is observed in obsessive-compulsive disorder and familial major depression disorder (37,38), HYPO may be at risk for these problems as well.
It is not readily clear why the genu and the splenium were the most affected CC sub-regions. However, this may reflect the exact timing of TH deficiency in relation to the stage of each segment's development as well as to the severity of the hypothyroidism. Other factors may include TH availability from iodine deficiency or exposure to environmental TH disruptors (39). Although the genu and splenium differ in number of myelinated axons (fewer in the splenium), this is an unlikely explanation given that CC myelination only starts after birth (22), which was not when the present sample was TH deficient. Furthermore, TH deficiency may indirectly alter callosal projections by disrupting cortical microarchitecture (40,41), given that manifestations in different cortical areas can influence the integrity of callosal projections (35).
Since the CC is the brain's primary interconnecting fiber bundle, abnormalities in its structural and anatomical organization can affect multiple mental functions in different ways that reflect the specific structure of the CC and the nature of the projections to the cortex such as axonal diameter and temporal delays (42). Previous studies have shown an association between CC surface area and social deficits in children with traumatic brain injury (32) and between CC length and executive function abilities in normal preschoolers (21). Similarly, the present findings suggest a functional impact of reduction in area and plumpness of genu on emotion regulation, as observed in newborns whose mothers were hypothyroxinemic (43). Conversely, callosal enlargement seen in children with neurofibromatosis-1 has been associated with nonverbal learning disability and impaired visuospatial and visuomotor skills (17). Although overgrowth in the present HYPO sample may contribute to similar deficits, the current study did not examine these particular abilities. However, Pop et al. have shown that children exposed gestationally to hypothyroxinemia had weak perceptuomotor skills, and this became more prominent as the number of hypothyroxinemic trimesters increased (11).
A strength of the current research includes our having one of the largest and longest-followed samples of well-characterized offspring born to women treated for hypothyroidism during pregnancy and similarly followed controls, all recruited originally as infants and now studied in peri-adolescence. Likewise, use of MRI and manually tracing the CC in children whose CC maturity is near complete is novel. Additionally, the CC segmentation approach was superior to traditional arbitrary sectioning methods in most CC research (44), since that used in our study was derived from known functional projections to the cortex.
However, this study does have some limitations. Regarding hormonal data, TSH values were averaged within trimesters, and in a few cases, group averages were used if data were missing in a particular trimester. Also, there was insufficient T4 data to perform these correlations. Further, the study did not record when symptoms first appeared in women diagnosed de novo in pregnancy, and it was assumed that this occurred at the onset of pregnancy when in fact it may not have appeared until the second trimester. Two women had normal TSH levels throughout pregnancy, and in only a few cases, mothers were hypothyroid in the third trimester, which is when CC sprouting occurs. Second, there was a lack of hormonal data on the full set of controls, and thus some of these women may have had subclinical if not clinical hypothyroidism during their pregnancy. However, it should be noted that in the subset that was tested, none were hypothyroid, and all mothers of control children verbally reported not being hypothyroid in pregnancy and at every assessment period when their children were seen. A third limitation is that the small sample size represents only about a third of the original cohort given the five- to seven-year gap between the current assessment and one previously at age five. Fourth, some children may have been exposed to factors other than maternal hypothyroidism such as poor nutrition or enrichment that could negatively or positively impact subsequent CC morphology. Fifth, the test battery was limited mostly to memory measures given that this was the main focus of the project for which scans were originally derived. Thus, abilities such as visuospatial skills could not be examined that may more accurately reflect the observed CC abnormalities. Six, the study did not initially set out to analyze sex differences in CC metrics. However, in light of research showing a larger overall CC area in males and a larger splenium in females (45), a supplementary analysis was performed examining for sex differences and none were found. Finally, effects on CC microstructure were not investigated that would determine how the degree of maternal TH insufficiency directly affects myelination and number, size, and integrity of callosal fibers. Therefore, future studies need to use DTI and DTI tractography techniques to evaluate the CC and other white-matter structures better.
In conclusion, the present study shows that maternal TH is necessary for early CC development and, when deficient, leads to abnormalities in size and shape of the genu and splenium. These abnormalities reflect primarily the duration of maternal TH insufficiency and are associated with suboptimal neuropsychological test performance and behavioral problems, particularly poor emotion regulation. Nevertheless, in order to understand the role of TH better on the many facets of CC development, future research needs to examine other conditions involving insufficient TH at different times during pregnancy or the postpartum, such as iodine deficiency and congenital hypothyroidism.
Footnotes
Acknowledgments
The authors would like to thank Anishka Greene, Dragana Ostojic, Erin Sheard, Michelle Vitti, and Karen Willoughby for their assistance in data collection; Garry Detzler, Tammy Rayner, and Ruth Weiss for obtaining MR scans; Susan Blaser for reading neuroradiological scans; Hayyah Clairman for her assistance in editing the article; and Charles Raybaud for enlightening us on corpus callosum development. Our extreme gratitude goes to the children and families whose dedication to this research and willingness to participate have made these findings possible. Funding for this research was through a Canadian Institute of Health Research operating grant (MOP 49488) and an SSuRe Summer Student Scholarship, while funding to ascertain the original sample was through the American Thyroid Association and March of Dimes.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.