
Abstract
Background:
The aim of this study was to evaluate the role of core-needle biopsy (CNB) as a first-line diagnostic tool for initially detected thyroid nodules.
Methods:
This observational study evaluated 632 initially detected thyroid nodules in 632 consecutive patients who underwent CNB between October 2008 and December 2011. CNB results were categorized into the six categories of the Bethesda System. A final diagnosis of malignancy was based on surgery or CNB, whereas a final diagnosis of benign nodules was based on surgery, two benign biopsy results, or benign cytology of stable size after one year. The rates of Bethesda category 1 and inconclusive results, diagnostic performance, unnecessary surgery, and complications were evaluated. Subgroup analysis based on nodule size was performed. Risk factors for inconclusive results were evaluated by multivariate logistic regression analysis.
Results:
The rates of Bethesda category 1 and inconclusive results by CNB were 1.3% and 5.9%, respectively. The diagnostic accuracy, sensitivity, specificity, positive predictive value, and negative predictive value for the diagnosis of malignancy were 97.6%, 90.0%, 100%, 100%, and 92.3%, respectively. The rate of unnecessary surgery was 0.5%, and the complications rate was 0.2%. Based on subgroup analysis, the diagnostic performance was not significantly associated with nodule size. There were no independent risk factors associated with inconclusive results.
Conclusion:
CNB showed low rates of Bethesda category 1 and inconclusive results and a high diagnostic accuracy. CNB also minimized unnecessary surgery. CNB seems to be a promising diagnostic tool for patients with initially detected thyroid nodules.
Introduction
U
Core-needle biopsy (CNB) may be a good alternative to FNA, since it is safe, well tolerated, and associated with a low incidence of complications (4,9 –13). Several recent studies have demonstrated that CNB can effectively reduce the rate of inconclusive results (4,14 –16) and minimize unnecessary and/or diagnostic surgery (4,13,14) for patients with thyroid nodules initially showing Bethesda category 1 or 3 by FNA. Although the role of CNB for initially detected thyroid nodules has not yet been determined, a recent pilot study involving 31 patients reported that first-line CNB was diagnostic for thyroid nodules with suspicious features seen on US, thus suggesting that CNB could reduce the rates of Bethesda category 1 and inconclusive results, even in initially detected thyroid nodules (17). Therefore, the effectiveness and safety of CNB for initially detected thyroid nodules have not yet been fully documented. CNB may be a good first-line diagnostic tool for initially detected thyroid nodules if it shows high diagnostic performance and prevents unnecessary surgery. This study therefore evaluated the diagnostic yield, rate of unnecessary surgery, and complications of CNB in a large population of patients with initially detected thyroid nodules.
Materials and Methods
Study population
The protocol of this observational study was approved by the Institutional Review Board of the authors' medical institution, a tertiary referral center, and it waived the requirement for written informed consent for use of these data. However, all patients provided written informed consent for CNB.
The CNB registry and medical records at the authors' institution were searched for patients who underwent CNB for initially detected thyroid nodules between October 2008 and December 2011 and who had not previously undergone FNA for these nodules. Figure 1 shows the flow chart for patient enrollment. Of the 1295 thyroid nodules in 1273 consecutive patients who underwent CNB, 663 nodules from 641 patients were excluded because they had undergone prior FNA. The final study population included 632 initially detected thyroid nodules from 632 consecutive patients. These patients included 136 men and 496 women with a M age ± SD of 50.8 ± 12.8 years (range 13–92 years). Of these patients, 145 underwent CNB because their nodules had suspicious features seen on US, 118 had heavily calcified nodules, 88 had vascular nodules, and three had predominantly cystic nodules. The remaining 278 patients underwent CNB due to their referring physician's preference.
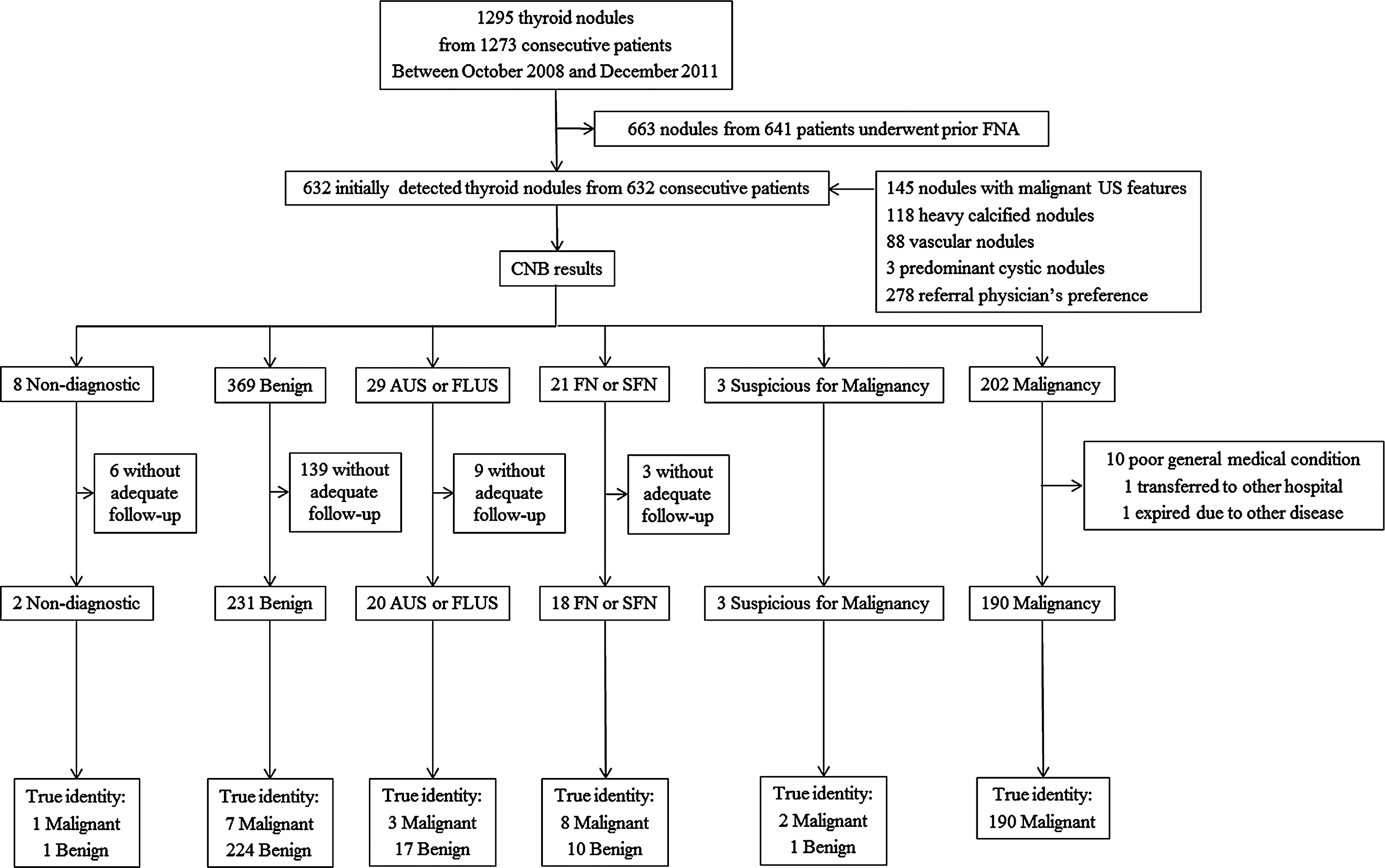
Patient flow and study outcomes in the study patients. Numbers represent the number of thyroid nodules. CNB, core-needle biopsy; AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; FN, follicular neoplasm; SFN, suspicious for a follicular neoplasm; US, ultrasound.
As a reference standard, malignant nodules with specific pathologic results, including lymphoma, metastasis from other sites, or thyroid malignancy with metastasis, were diagnosed after surgery or after biopsy. Benign nodules were diagnosed after surgery, after at least two sets of benign findings on FNA and/or CNB on different occasions, or after benign cytology findings on CNB with the nodule size remaining stable after one year.
US-guided CNB procedures
US examinations were performed using one of three US systems: an iU22, a HDI-5000 unit (Philips Healthcare, Bothell, WA), or a EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan). Each was equipped with a linear, high-frequency probe (5–14 MHz). All US examinations and US-guided CNBs were performed by two faculty radiologists (J.H.B. and J.H.L., with 18 and 13 years of clinical experience, respectively, in performing and evaluating thyroid US) and three neuroradiology fellows and one resident supervised by two faculty radiologists.
US-guided CNBs were performed under local anesthesia with 1% lidocaine using a disposable 1.1- or 1.6-cm excursion, 18-gauge, double-action, spring-activated needle (TSK Ace-cut; Create Medic, Yokohama, Japan) (4,14,15). Before insertion of the core needle, the vessels along its approach route were evaluated by power Doppler US in order to prevent hemorrhage. Using a freehand technique, the core needle was advanced from the isthmus of the thyroid toward the nodule. After the tip of the needle had been advanced to the edge of the nodule, the distance of fire (1.1 or 1.6 cm) was measured before sequential firing of the stylet and cutting cannula of the needle (Fig. 2).
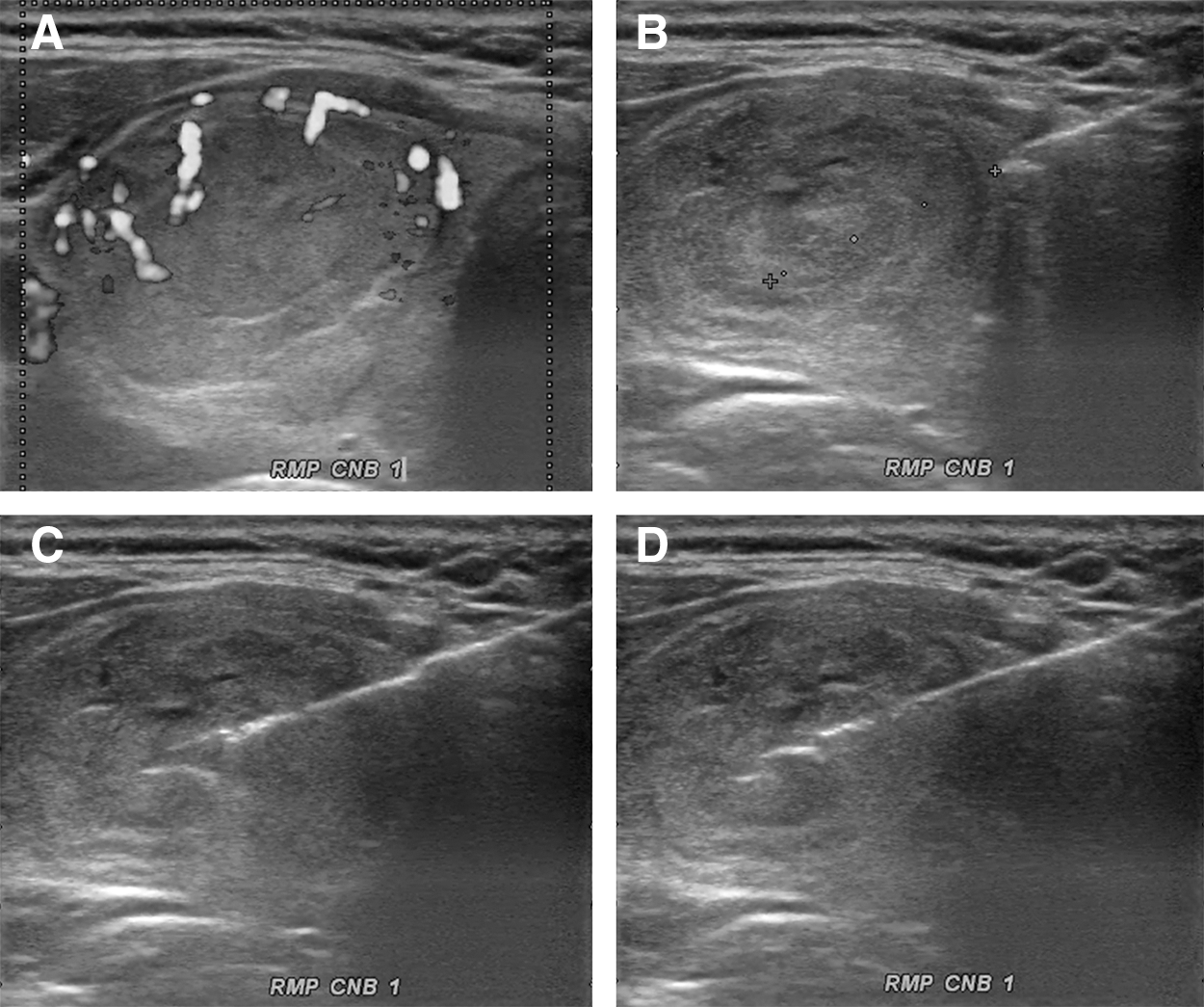
US images of a 48-year-old female with a thyroid nodule evaluated by CNB. (
The adequacy of the procedure was monitored by real-time US, and the adequacy of the tissue core was assessed by visual inspection (Fig. 3). An additional CNB was performed when targeting of the lesion was considered inaccurate. Each patient was observed after firm local compression of the biopsy site for 10–20 minutes following the biopsy. If patients complained of pain or neck swelling, a repeat US examination was performed in order to evaluate possible complications.
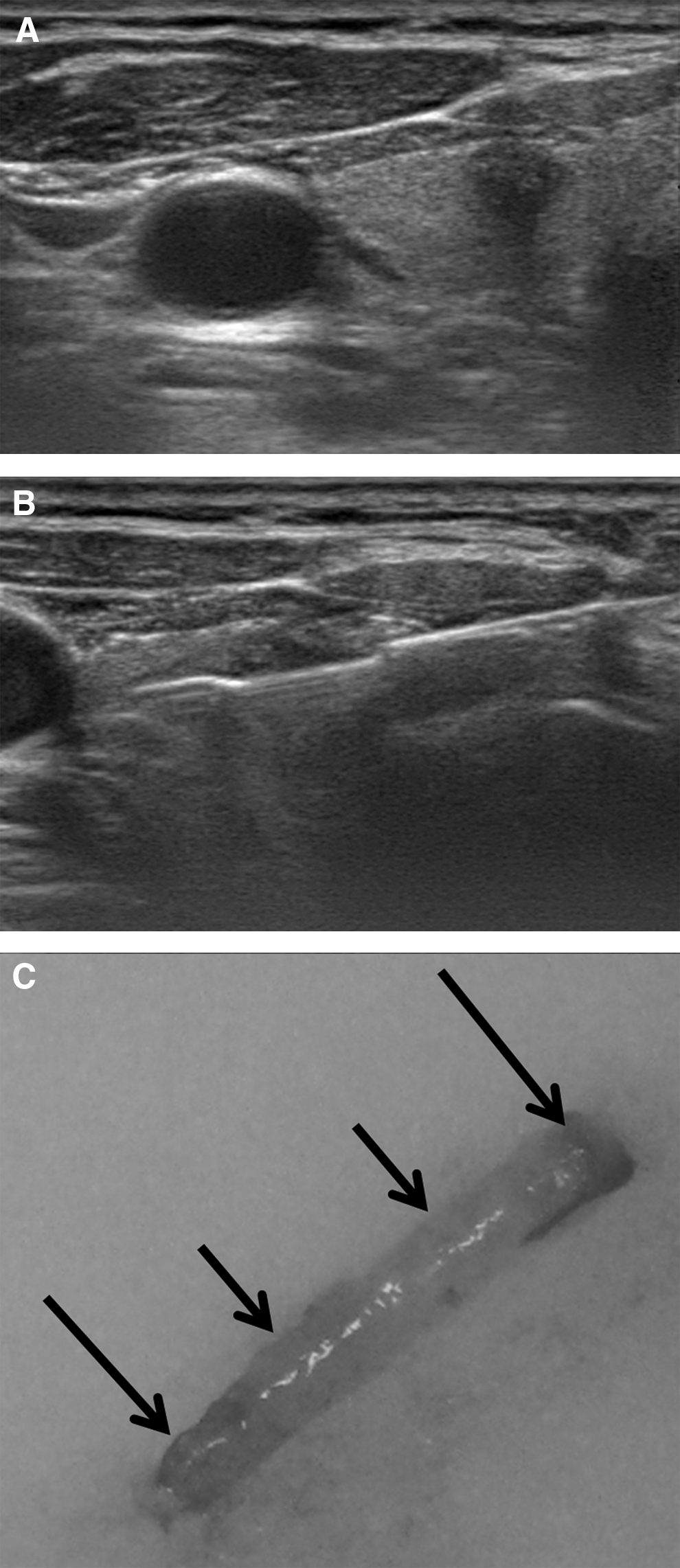
Visual assessment of a CNB specimen from a 56-year-old female with a right thyroid nodule. (
Analysis of US findings
The US images were reviewed independently by two radiologists (J.H.B. and C.H.S). Neither had any information regarding the patient's clinical history, previous imaging results, or histologic results. Discrepancies between the US findings of the two investigators were resolved by consensus.
The US findings for the nodules were evaluated for the following features (18 –21): internal composition (solid, predominantly solid, predominantly cystic, or cystic), shapes (ovoid to round, taller than wide, or irregular), margins (smooth, spiculated, or ill-defined), echogenicity (isoechoic, hypoechoic, markedly hypoechoic, or hyperechoic), and the presence of microcalcifications, macrocalcifications, or rim calcifications. The suspicious features seen on US were a taller-than-wide shape, spiculated margin, marked hypoechogenicity, and the presence of micro- or macrocalcification (18 –20,22).
Histopathologic analysis of CNB specimens
All CNB specimens were reviewed by a thyroid cytopathologist with 10 years of clinical experience (D.E.S.). In as much as the diagnostic criteria for CNB of thyroid nodules had not been standardized during the study period, the histologic results of CNB were categorized into the six categories of the Bethesda System (2,4,14,15). Bethesda category 1 (non-diagnostic) include (i) the absence of any identifiable follicular thyroid tissue; (ii) the presence of follicular cells, but which are regarded as normal thyroid tissue only (3); and (iii) tissue containing only few follicular cells insufficient for diagnosis. Bethesda category 2 (benign) include colloid nodules, nodular hyperplasia, and lymphocytic thyroiditis. Bethesda category 3 (atypia of undetermined significance and follicular lesion of undetermined significance) include findings in which some atypical cells are present, but they are not diagnostic of “suspicious malignancy” or “malignancy,” and include cellular follicular cytologies that do not fulfill the criteria for “follicular neoplasm/suspicious for follicular neoplasm.” Nodules with histologic features favoring follicular neoplasm were categorized as Bethesda category 4 (follicular neoplasm or suspicious for a follicular neoplasm). Nodules were categorized as Bethesda category 5 (suspicious for malignancy) if the specimen exhibited atypia, although there was insufficient evidence for a definite diagnosis of malignancy. Specimens exhibiting unequivocal features of cancer were categorized as Bethesda category 6 (malignancy).
Statistical analysis
Study outcomes included the rates of Bethesda category 1, inconclusive and conclusive results, and malignancy, diagnostic performance, unnecessary surgery, and complications. Nodules classified as inconclusive included those that were Bethesda category 1 on CNB, those with atypia of undetermined significance, and those with follicular lesion of undetermined significance. Nodules classified as conclusive included those found on CNB to be benign, follicular neoplasm or suspicious for follicular neoplasm, suspicious for malignancy, and malignant. The diagnostic criteria for malignancy were defined as Bethesda category 6 (malignancy). The diagnostic performance of CNB included its diagnostic accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for a diagnosis of malignancy. Unnecessary surgery included nodules reported as malignant on CNB that were confirmed as being benign after surgery and nodules reported as follicular neoplasms on CNB confirmed as being adenomatous hyperplasia after surgery (23). Major and minor complications were those defined by the Society of Interventional Radiology (24,25). A major complication was defined as one that if left untreated might be life-threatening, lead to substantial morbidity or disability, or result in a lengthened hospital stay. All other complications were considered as minor.
Subgroup analyses were performed according to nodule size (<1 cm or ≥1 cm) and suspicious features seen on US. Results after surgery were compared with those after CNB. Independent risk factors related to inconclusive results were identified by dividing the 632 CNB results into those that were inconclusive and conclusive. The parameters of the two groups were compared using univariate analysis, with Student's t-tests used for numerical values and the chi-square test or Fisher's exact test for categorical values. The level of significance was defined as p < 0.05. All statistical analyses were performed using SPSS Statistics for Windows v21.0 (IBM Corp., Armonk, NY).
Results
All patients tolerated the core biopsy procedures. The mean size of the 632 nodules was 2.0 ± 1.6 cm (range 3–130 mm), with 409 nodules (64.7%) being ≥1 cm. CNB was performed on all nodules, even the 223 nodules <1 cm in size, in order to evaluate the nodules with suspicious features seen on US (n = 166), as well as those with indeterminate features seen on US (n = 57), in order to determine the extent of the surgery for multiple thyroid nodules or to evaluate primary malignancy when cervical lymph nodes were diagnosed as metastatic.
Sample adequacy
The results of CNB (n = 634) and the final diagnoses (n = 465) are summarized in Table 1. CNB was Bethesda category 1 in 8/634 biopsies (1.3%). Of the eight Bethesda category 1 CNB specimens, three showed the presence of fibromuscular tissue because the biopsy was targeted incorrectly, four showed no or only a few cells because the biopsy was of a cystic or necrotic portion of the mass, and one yielded insufficient tissue for diagnosis.
Data are number of nodules, with percentages in parentheses. Percentages do not add up to 100% because of rounding.
AUS, atypia of undetermined significance; CNB, core-needle biopsy; FLUS, follicular lesion of undetermined significance; FN, follicular neoplasm; SFN, suspicious for a follicular neoplasm.
Final diagnosis
Final diagnoses were obtained for 465 nodules (73.3%), and they were included in the outcome analyses. In contrast, 169/632 patients (26.7%) were not adequately followed up to confirm the diagnosis of their initially detected thyroid nodule. Of the 211 malignant nodules, 196 (92.9%) were diagnosed after surgery, and 15 (7.1%) after biopsy yielded specific pathologic results, including eight diagnosed as lymphoma, five as metastases from other sites, and two as thyroid cancers with metastases. Of the 254 benign nodules, 25 (9.8%) were diagnosed after surgery, 51 (20.1%) after FNA and/or CNB yielded benign findings at least twice, and 178 (70.1%) after CNB yielded benign findings with the nodule size remaining stable after one year. The mean patient follow-up period was 30.7 ± 10.7 months.
Study outcomes
The outcomes of CNB for initially detected thyroid nodules are summarized in Figure 1 and Table 2. CNB yielded conclusive results for 595/632 nodules (94.2%), and inconclusive results for the other 37 (5.9%). CNB diagnosed 190/632 nodules as malignant (30.1%). The diagnostic accuracy, sensitivity, specificity, PPV, and NPV of CNB for diagnosing malignancy were 97.6%, 90.0%, 100%, 100%, and 92.3%, respectively.
Subgroup analysis according to the nodule size
Subgroup analysis showed that the malignancy rate was significantly higher for nodules <1 cm in size (44.8%) than for nodules ≥1 cm in size (22.0%). The sensitivity of CNB was also significantly higher for nodules <1 cm (96.2%) than for nodules ≥1 cm (84.1%). Most malignant nodules <1 cm were found to be papillary thyroid carcinomas (99.0%), whereas other types of cancer (26.2%), including follicular, medullary, and anaplastic carcinoma, were more common in nodules ≥1 cm. Other study outcomes did not differ significantly according to nodule size.
Subgroup analysis according to suspicious features seen on US
Of the 632 nodules, 280 (44.3%) had at least one suspicious feature seen on US. CNB was Bethesda category 1 in 3/280 biopsies (1.1%). CNB yielded conclusive results for 318/325 nodules (96.1%), and there were inconclusive results for the other 11 (3.9%). CNB diagnosed 154/280 nodules as malignant (55.0%). Final diagnoses were obtained for 223 nodules (79.6%). The sensitivity, specificity, PPV, and NPV of CNB for the diagnosis of malignancy were 94.2%, 100%, 100%, and 88.2%, respectively.
Risk factors associated with inconclusive results
Univariate analysis showed that nodule size, shape, and margin were significantly associated with inconclusive results on CNB (Table 3). Multivariate logistic regression analysis, however, failed to identify any independent risk factors associated with inconclusive results (Supplementary Table S1; Supplementary Data are available online at
Correlation of CNB results with surgery
Of the 465 nodules with a final diagnosis, 254 (54.6%) were benign and 211 (45.4%) were malignant. Of the 221 (47.5%) nodules removed surgically, 196 were malignant and 25 were benign (Supplementary Table S2).
Of the 176 nodules diagnosed as malignant after CNB, all 176 were confirmed as malignant after surgery. Among the 13 nodules diagnosed as follicular neoplasms after CNB, seven were confirmed as being malignant, four were follicular adenomas, one was a Hürthle cell adenoma, and one was confirmed as adenomatous hyperplasia. Therefore, the rate of unnecessary surgery was 0.5%.
Of the 23 nodules found to be benign on CNB and which were surgically removed, 12 were because of image-pathology discordance (benign on CNB but suspicious for malignancy on US), five due to FNA showing a metastatic cervical lymph node, two due to malignancy on secondary CNB, and four for cosmetic reasons. Of the 12 nodules with image-pathology discordance, three were found to be malignant (i.e., two follicular carcinomas and one papillary carcinoma). Of these 23 nodules with benign findings after CNB, seven were confirmed as being malignant after surgery. Failure of CNB to diagnose malignancy was likely due to mistargeting of the lesion when performing CNB.
Complications
None of the included patients experienced any major complications associated with intervention or hospitalization. Only one patient developed a hematoma after the procedure, thus resulting in a complication rate of 0.2%. The hematoma resolved following compression and rest for one hour. There was also no incidence of needle-tract seeding associated with CNB.
Discussion
This study found that CNB for initially detected thyroid nodules had a Bethesda category 1 rate of 1.3% and an inconclusive rate of 5.9%. These findings indicate that CNB could provide conclusive results for a substantial majority of these patients (94.2%) and that further unnecessary biopsies or diagnostic surgery are not required. CNB also showed a high diagnostic accuracy for malignancy (97.6%), with low rates of complications (0.2%) and unnecessary surgery (0.5%). Taken together, these findings suggest that CNB is a safe method for the diagnosis of initially detected thyroid nodules. Subgroup analyses show that the diagnostic performance of CNB and its rates of Bethesda category 1 and inconclusive results were similar for nodules <1 cm and ≥1 cm in size. Multivariate logistic regression analysis failed to identify any independent risk factors associated with the inconclusive results.
CNB was found to be Bethesda category 1 on 0–7.2% of thyroid nodules previously found to be Bethesda category 1 on FNA (4,9,11,13,15,26). Moreover, comparisons of CNB and repeat FNA on thyroid nodules previously found to be Bethesda category 1 on FNA showed that Bethesda category 1 rates were lower for CNB (0–7.2%) than they were for repeat FNA (28.1–40%) (13,15,26), and that repeat FNA was significantly associated with a repeat Bethesda category 1 (13). Current guidelines recommend CNB rather than repeat FNA when the initial FNA is Bethesda category 1 (5,12), thus suggesting that CNB can be a management tool for thyroid nodules with Bethesda category 1 on a previous FNA.
A small population study assessed CNB as a first-line diagnostic tool for initially detected thyroid nodules and found that the Bethesda category 1 rate was low (3.2%; 1/31) and the diagnostic accuracy rate was high (96.8%; 30/31) (17). The results reported in this study validate CNB as a first-line diagnostic procedure for thyroid nodules with suspicious features seen on US, and with low Bethesda category 1 (1.1%), and inconclusive result (3.9%) rates and high sensitivity (94.2%) and specificity (100%). These results suggest that CNB may be considered as an effective diagnostic tool for initially detected thyroid nodules.
Since thyroid malignancies <1 cm are often considered clinically insignificant, the role of CNB for these small nodules has not yet been established. However, biopsy remains necessary, even for these small nodules, in order to evaluate the nodules with suspicious features seen on US and indeterminate features seen on US in order to determine the extent of surgery for multiple thyroid nodules or to identify the primary malignancy when cervical lymph nodes have been found to harbor metastatic cancer. The present study found that the Bethesda category 1, the inconclusive result rate, and the diagnostic performance of CNB did not differ for nodules <1 cm and ≥1 cm in size. These findings indicate that CNB is an effective method, even for small thyroid nodules.
Several factors have been correlated with Bethesda category 1 or inconclusive results on FNA, including operator skill, processing errors, and the intrinsic characteristics of the nodules, that is, cystic component, small size, macro/rim calcifications, and vascularity (8,27,28). Although inconclusive results on CNB were not associated with US characteristics (29), the risk factors associated with Bethesda category 1 or inconclusive results on CNB have not yet been determined. Multivariate logistic regression analysis of the large study population also failed to identify any independent risk factors associated with inconclusive results on CNB. These results indicate that the high rates of conclusive results on CNB are not influenced by patient characteristics, operator experience, the number of procedures (number of passes), or nodule characteristics. Moreover, these findings may have been possible due to the advantages of CNB, including large tissue samples, less operator dependence, and the ability to assess histologic architecture (15). Nevertheless, operator experience might be important because the risks of CNB may be higher and the accuracy may be lower in less clinically experienced hands.
A PPV of 100% was observed of CNB for a diagnosis of malignancy, similar to previous findings (4,14 –17,30,31) (Table 4). This high PPV may prevent repeat biopsy to confirm thyroid cancer and thus minimize unnecessary surgery. Indeed, the unnecessary surgery rate in this study was only 0.5%. CNB was reported to prevent unnecessary diagnostic surgery in 96% of the patients with repeated Bethesda category 1 FNA results (4), thus suggesting that CNB provides diagnostic confidence for managing these patients to perform surgery.
PPV, positive predictive value.
This study has several limitations, including its observational design and the lack of a control group. Direct comparisons between CNB and FNA are necessary in order to verify the results of the study. Second, although diagnostic categories have not been standardized for CNB results during the study period, a recent article suggested a pathology reporting system for thyroid CNB (3). Further comparative studies of CNB and FNA using the pathology reporting of thyroid CNB will be required. Finally, there may be potential biases in the inclusion criteria for CNB because of its retrospective nature.
In conclusion, this study demonstrates that evaluation using CNB resulted in low rates of Bethesda category 1 and inconclusive results and a high diagnostic accuracy in patients with initially detected thyroid nodules. CNB had a PPV of 100%, thus minimizing unnecessary surgery. There were no independent risk factors associated with inconclusive results. These findings indicate that CNB may be a promising diagnostic tool for patients with initially detected thyroid nodules.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.