
Abstract
Background:
Oxidative stress, which occurs as a result of an imbalance between free-radical production and antioxidant defense mechanisms, has been implicated in the pathogenesis of several autoimmune disorders, including thyroid diseases. Importantly, it has been correlated to thyroid dysfunction. This study investigated the changes in oxidative balance in euthyroid Hashimoto's thyroiditis (HT) by means of specific serum tests, such as derived reactive oxygen metabolites (d-ROMs) and the biological antioxidant potential (BAP) test. In addition, advanced glycation end products (AGEs) and advanced oxidation protein products (AOPPs)—compounds formed by the transformation of proteins—were evaluated as potential new markers of oxidative stress in this disease.
Methods:
This study included 134 euthyroid subject: 71 newly diagnosed HT patients (63 females; M age = 38 ± 13 years) and 63 age and sex-matched healthy controls. None of them were on thyroxine therapy.
Results:
Serum d-ROMs were elevated, and BAP decreased in HT patients compared with controls (p < 0.001), and the two parameters were inversely correlated (r = −0.211; p = 0.027), clearly indicating an enhanced oxidative stress. Furthermore, AGE levels were higher in HT patients (M = 223.18 AU/g prot) than in controls (M = 189.636 AU/g prot; p = 0.020) and inversely correlated with BAP levels (r = −0.196; p = 0.037). In uni- and multivariate analysis, serum antithyroperoxidase antibodies were the main predictors for d-ROMs (p = 0.006), BAP (p < 0.001), and AGEs (p = 0.014), irrespective of thyrotropin and/or free thyroxine values. No differences in AOPPs levels were found between patients and controls (p = 0.923).
Conclusions:
Oxidants are increased and antioxidants decreased in euthyroid HT patients. As a result, the oxidative/antioxidative balance is shifted toward the oxidative side. Moreover, this study reports on a possible significant involvement of AGEs in HT, thus contributing to a better definition of the redox homoeostasis dysregulation in HT.
Introduction
R
In the field of AITD, however, the role of oxidative stress has mainly been evaluated in relation to thyroid dysfunction (9,10). In fact, thyroid hormones play a crucial role in regulating oxidative metabolism: on the one hand, they increase mitochondrial respiration and free-radical production, and on the other, they regulate the synthesis of enzymatic (superoxide dismutase, catalase, glutathione peroxidase, and reductase), and nonenzymatic antioxidants (11). Moreover, the thyroid itself is exposed to long-life oxidative stress, induced by the continuous production of H2O2 during the process of thyroid hormone synthesis (12). As a consequence, both hyperthyroidism and hypothyroidism have been reported to be associated with oxidative stress, sometimes with conflicting data (9 –11,13 –18). In contrast, our understanding of the role of the oxidative/antioxidative systems in the autoimmune process per se is limited, since few data on small cohorts of patients are available to date on oxidative status in patients with euthyroid AIDT (18,19). The present study aimed to investigate the changes in oxidative balance in euthyroid Hashimoto's thyroiditis (HT) by means of specific serum tests, such as derived reactive oxygen metabolites (d-ROMs) and biological antioxidant potential (BAP), which reflect the general status of the oxidative levels in the body. In addition, advanced glycation end products (AGEs) and advanced oxidation protein products (AOPPs), compounds formed by the transformation of proteins, recently reported as inflammatory markers in several diseases (20,21), were evaluated as potential new markers of oxidative stress in HT, since no data are available on this issue in the pertinent literature.
Materials and Methods
Subjects
A power analysis was used to guide in the choice of sample size; it allowed the minimum sample size required to accept the outcome of a statistical test to be calculated, with a confidence level of α = 0.050. It was established that the desired power level was 0.80, and consequently the sample size needed to ensure this specific power level was estimated. For the sample size calculation, an expected difference of 0.25 was considered between two groups (HT patients vs. healthy controls), and an expected residual standard deviation of about 0.5. Assuming α = 0.050, it was established that about 63 subjects per group would be needed to reach a power level of 0.80.
Accordingly, 134 subjects >18 years of age, consecutively referred to the authors' outpatient clinics over a six-month period, were enrolled in the study. Seventy-one newly diagnosed HT patients (63 females; M age = 37.8 ± 13.42 years) formed the patient group. HT was diagnosed by the currently accepted laboratory and ultrasonographic criteria (serum antithyroid antibodies positivity and/or heterogeneous echo-structure with diffuse or patchy hypoechogenicity at ultrasound) (22,23). All patients were euthyroid and were not taking levothyroxine therapy or drugs affecting thyroid function at the time of sampling. Sixty-three age- and sex-matched healthy subjects (57 females; M age = 34.12 ± 12.33 years) served as the control group, after taking a history to rule out current and past thyroid illness, as well as any autoimmune-related disease.
Exclusion criteria for both groups were diabetes mellitus or kidney failure, history of neoplastic disease, and the existence of any comorbid cardiovascular, autoimmune, infectious, or inflammatory disease, as well as smoking, alcohol consumption, and taking of any form of antioxidant agents, vitamin supplements, and lipid-lowering or antihypertensive drugs. Each subject received a careful medical evaluation, including recording of the past medical history, and physical examination.
The study was approved by the local Ethics Committee. Informed consent was obtained from each subject.
Biochemical analysis
Blood samples were collected from the cubital vein after overnight fasting. Venous blood was centrifuged at 1450 g at 4°C for 10 min. Glucose, insulin, lipids, liver enzymes, and homocystenine were immediately measured; aliquots for other assays were stored at −20°C. Overall, determination of the study parameters occurred within two months of sera collection.
Serum fasting insulin, glucose, triglycerides, total cholesterol, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, glutamic oxaloacetic transaminase and glutamic pyruvic transaminase, and homocysteine were measured using commercial kits with routine methods.
Serum thyrotropin (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) concentrations, as well as antithyroglobulin (TgAb) and antithyroperoxidase (TPOAb) antibodies, were measured by electrochemiluminescence immunoassay (ECLIA), using commercial kits for Elecsys 1010/2010 e modular analytics E170 supplied by Roche Diagnostics. Reference ranges in the authors' laboratory are: TSH 0.27–4.2 mIU/L; fT3 2.0–4.4 pg/mL; fT4 12.0–22.0 pmol/L; TgAb 0–4 IU/mL; TPOAb 0–10 IU/mL.
All samples were processed centrally in the laboratory of the University Hospital of Messina. For all assays, the intra- and inter-assay CV were <5 and <10%, respectively.
Assays for oxidant and antioxidant parameters
The ROMs were measured by the d-ROMs kit from Diacron. The assay measures the concentration of hydroperoxide that is present in the serum sample. The method is based on the principle that in an acidic solution (pH 4.8), iron is released from transferrin and is available to catalyze the reaction of hydroperoxides to alkoxyl and peroxyl radicals, which further react with chromogen N,N-diethyl-pphenylenediamine. Upon oxidation, the chromogen is transformed in red colored cation, which is measured at 505 nm. The results of the test are expressed in CARR U (Carratelli Units). Each CARR U corresponds to 0.08 mg H2O2/100 mL sample.
To measure the BAP, a kit from Diacron was used. The assay is based on the decrease in absorption when Fe3+ ions that bind to a thiocyanate-derived substrate are reduced to Fe2+. The absorbance was measured at 505 nm, and the amount of reduced ferric ions can be calculated. The results are expressed in μmol/L of vitamin C used as an iron-reducing agent.
Determination of AGEs was based on the spectrofluorimetric detection, as previously reported (24). Briefly, blood serum was diluted 1:50 with phosphate-buffered saline (PBS) pH 7.4, and fluorescence intensity was recorded at the emission maximum (∼440 nm) upon excitation at 350 nm (spectrofluorimeter Shimadzu). The serum concentration of AGEs was normalized to the total protein amount determined by the Bradford assay and expressed in arbitrary units (AU) per gram of protein (AU/g prot).
Determination of AOPPs was based on spectrophotometric detection, as previously described (24). Blood serum (100 μL) or the same volume of chloramin T (0–100 μmol/L) for calibration were diluted 1:5 with PBS pH 7.4. Subsequently, 25 μL of 1.16 M KI and 50 μL of acetic acid were added to the diluted solutions, and absorbance was measured immediately at 340 nm (spectrophotometer Shimatzu). Concentration of AOPP is expressed in chloramine T units (μmol eq Cl T/L).
Ultrasonography evaluation
Subjects were examined by the same trained ultrasonographer (R.C.) using a real-time 2D apparatus with a 7.5 MHz linear transducer. An abnormal sonographic appearance of the thyroid, characterized by diffuse areas of decreased echogenicity, was considered an important criterion for the sonographic diagnosis of HT. The volume of thyroid lobes was calculated with the ellipsoid formula (π/6 × height × width × depth, each diameter being expressed in cm). The carotid intima-media thickness (IMT), an early marker of atherosclerosis, was assessed at the far wall as the distance between the interface of the lumen and intima (first echogenic line) and the interface between the media and adventitia (second echogenic line). Both the left and right carotid arteries were scanned at four sites, as described elsewhere (25). The mean of the IMT values was used for analysis.
Statistical analysis
The numerical data are expressed as mean, median, and range, and the categorical variables as number and percentage. The examined variables were not normally distributed, as verified by a Kolmogorov–Smirnov test. Consequently, the nonparametric approach was used. In order to assess any significant differences between HT cases and controls, the Mann–Whitney U-test was applied for all examined numerical parameters, and the chi-square test for categorical variables. For BAP, d-ROMs, AGEs, and AOPPs, some univariate linear regression models were estimated in order to assess the dependence of each oxidative stress marker by potentially explicative variables such as age, sex, BMI, waist–hip ratio, metabolic parameters, pressure values, IMT, hepatic enzymes, thyroid functionality indexes, and antithyroid antibodies. Subsequently, for each oxidative stress marker, a multivariate linear regression model was estimated inserting only the covariates that were statistically significant with a univariate approach. The Spearman correlation test was applied to assess the interdependence relationship between the studied oxidative stress markers (BAP, d-ROMS, AGEs, and AOPPs).
Statistical analyses were performed using SPSS Statistics for Window v17.0. A p-value of <0.050 was considered to be statistically significant.
Results
A total of 134 subjects (71 HT and 63 controls) were included in the study. Demographic, clinical, and biochemical features of the study population are summarized in Table 1. The two groups of HT patients and healthy controls, who were age- and sex-matched, did not differ significantly regarding the main anthropometric and metabolic parameters. All subjects were euthyroid at the time of sampling, but serum TSH levels were significantly higher in HT patients compared with controls (p < 0.001).
Data are shown as M ± SD (range), except TgAb and TPOAb, which are median (range). Normal values are specified in the Materials and Methods. Statistically significant values are shown in bold.
The BMI was calculated by dividing the body weight (kg) by the square of height in meters.
WC measured midway between lower costal margin and iliac crest at the end of normal expiration; WHR calculated by the formula: waist circumference (cm)/hip circumference (cm).
Insulin resistance was estimated by the homeostatic model assessment index (HOMA).
Thyroid volume and IMT were evaluated by ultrasound as described in the Materials and Methods.
BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; GOT, glutamic oxaloacetic transaminase; GPT, glutamic pyruvic transaminase; HDL, high-density lipoprotein; HT, Hashimoto's thyroiditis; IMT, intima-media thickness; LDL, low-density lipoprotein; TgAb, thyroglobulin antibodies; TPOAb, antithyroperoxidase antibodies; TSH, thyrotropin; WC, waist circumference; WHR, waist–hip ratio.
The serum levels of the oxidative stress parameters evaluated are presented in Table 2. Serum d-ROMs were significantly increased in HT patients compared with controls (M = 339.24 vs. 267.34 CARR U; p = 0.0002), while BAP were decreased (M = 2496.48 vs. 3380.31 μmol/L; p < 0.0001; Fig. 1). Accordingly, the two parameters were inversely correlated (r = −0.211; p = 0.027; Fig. 2, top), clearly indicating an imbalance between endogenous production of free radicals and antioxidant defense systems in HT patients.

Serum levels of the four oxidative stress parameters under study in patients with Hashimoto's thyroiditis (HT) and healthy subjects (controls): reactive oxygen metabolites (d-ROMs), biological antioxidant potential (BAP), advanced glycation end products (AGEs), and advanced oxidation protein products (AOPPs). The lines represent mean and range.
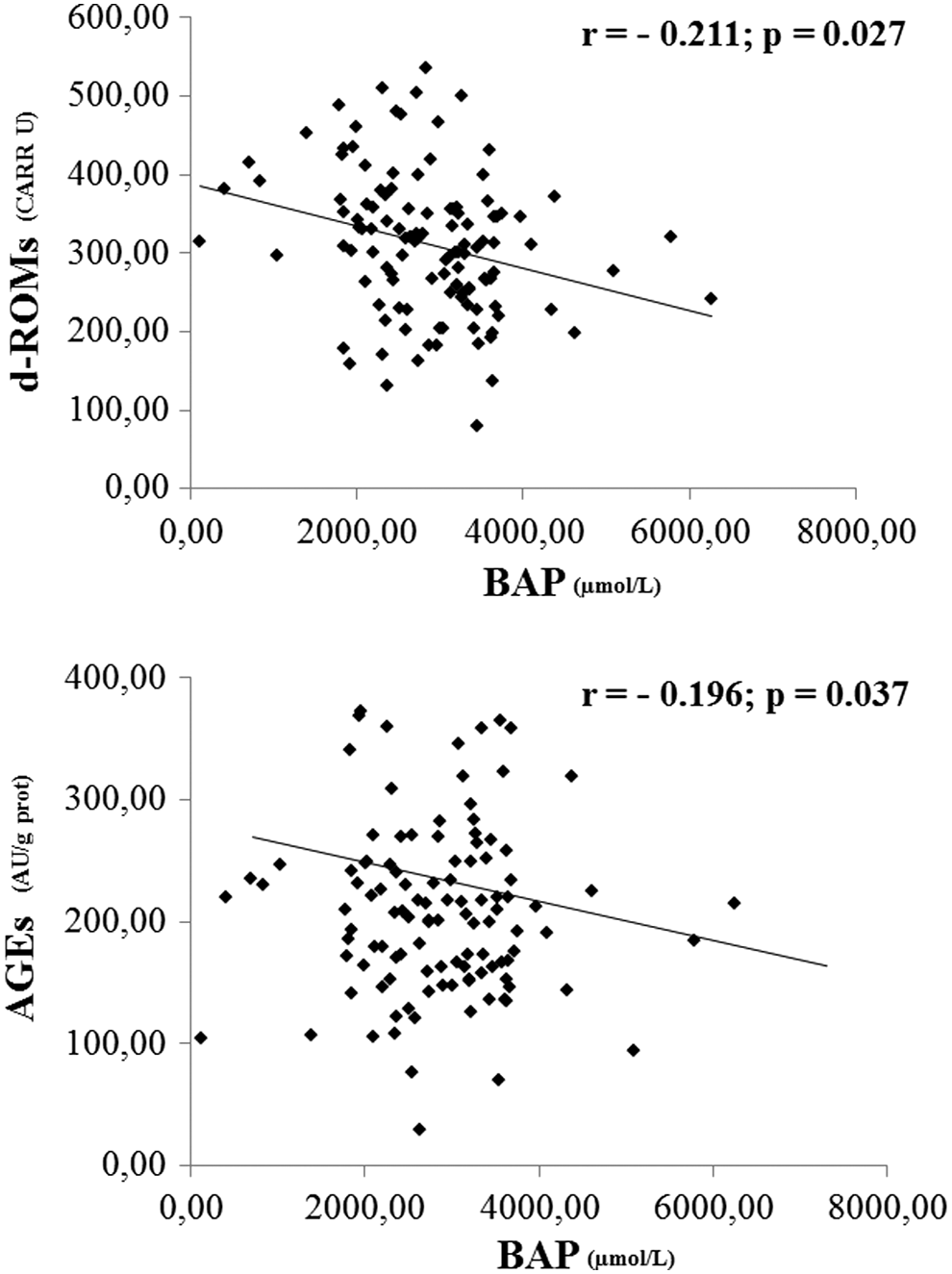
Relationship between serum levels of BAP and of d-ROMs (top) and AGEs (bottom).
Data are shown as mean (range). Comparison was made using the Mann–Whitney U-test. Statistically significant values are shown in bold (p ≤ 0.05).
AGEs, advanced glycation end products; AOPPs, advanced oxidation protein products; AU/g prot: arbitrary units (AU) per gram of protein; BAP, biological antioxidant potential; CARR U, Carratelli units; d-ROMs, derived reactive oxygen metabolites.
In addition, serum AGEs levels were higher in HT patients than they were in controls (223.18 vs. 189.636 AU/g prot; p = 0.020), and inversely correlated with BAP levels (r = −0.196; p = 0.037; Table 2 and Fig. 2, bottom). Instead, the AOPPs levels were similar between the HT patients and controls (p = 0.923; Table 2), and did not correlate with the other oxidative stress markers (p > 0.05).
In the univariate analysis, the variables that were significantly associated with the three altered markers of oxidative stress were serum TSH values and the presence of TgAb and/or TPOAb, as well as serum total and LDL or HDL cholesterol levels, and age (Table 3). In the multivariate analysis adjusted for age, serum TSH, presence/absence of TgAb/TPOAb, and serum cholesterol values, serum TPOAb positivity was found to be the main independent predictor that affects the levels of d-ROMs, BAP, and AGEs, irrespective of TSH levels (Table 3). Furthermore, age and HDL cholesterol were an independent predictor for BAP levels, and LDL cholesterol for AGEs levels.
Statistically significant values are shown in bold. Borderline significant values (p ≤ 0.10 but ≥0.05) are shown in italic.
Multivariate linear regression model for each parameter was estimated inserting only the covariates that resulted statistically significant in univariate approach.
In the regression model, AOPPs were not significantly associated with thyroid function and autoimmunity indexes, as expected, since AOPPs levels were similar in HT patients and controls. However, in the univariate analysis, AOPP levels were associated with the following metabolic parameters: fasting glucose and insulin, HOMA index, total cholesterol, LDL and HDL cholesterol, triglycerides, glutamic pyruvic transaminase, blood pressure values, and IMT. In multivariate analysis adjusted for the above-mentioned variables, only fasting glucose was an independent predictor for AOPPs levels (Table 3).
Discussion
The present study assessed the oxidant/antioxidant status in euthyroid patients affected by HT in comparison with healthy subjects, and found that d-ROMs were significantly higher and the antioxidant potential (BAP) significantly lower in HT patients than in controls. In HT, then, the balance between serum antioxidants and oxidants has been shown to be shifted in favor of the latter, suggesting that oxidative stress may be a key event in the pathophysiology of HT, irrespective of thyroid function.
This is the first study evaluating the changes of oxidative balance in a large series of euthyroid HT patients. Most of the studies encountered in the literature in recent years have evaluated oxidative stress in AIDT patients with thyroid dysfunction (9,10). Both hyperthyroidism and hypothyroidism have been found to be associated with enhanced oxidative stress, since the former has been shown to increase free radicals and oxidants production (6,7,9,10,15,17) and the latter to reduce the antioxidant defense systems (9,10,14,16,18). On this basis, antioxidant supplementations have been proposed in Graves' hyperthyroidism and orbitopathy as useful therapeutic tools (17,26 –28), and their role in HT is debated (29,30).
To date, only two studies had evaluated the oxidative status in euthyroid HT patients, demonstrating a significant increase of oxidants without changes in antioxidant defenses in one study (18) and increased oxidative stress resulting from both oxidant increase and antioxidant decrease in another study (19). These two studies included a small number of both euthyroid patients and controls (31 and 35 subjects for each group, respectively) and provided conflicting data concerning levels of antioxidant defenses in such patients (18,19). In line with the data from Baser et al. (19), the current study found both higher oxidant parameters and lower antioxidant parameters in euthyroid HT patients than in controls, and TPOAb presence was the main independent predictor affecting both parameters. In the univariate analysis, TSH levels were significantly associated with the markers of oxidative stress, but in multivariate models, TSH was not shown to be an independent risk factor for developing oxidative stress, confirming the main role of TPOAb, namely of autoimmunity. In addition to the thyroid functional status, the 134 subjects enrolled in the present study were also similar with regard to age, sex, and the main metabolic and anthropometric parameters that may affect the oxidant/antioxidant balance, thyroid autoantibodies being the only significant difference. Therefore, enhanced oxidative stress seems to be mainly related to the chronic autoimmune inflammation rather than to variations of thyroid hormone levels, although discrete alterations of intracellular thyroid hormone concentrations cannot be ruled out in such patients.
Thus, increased oxidative stress may play a pathogenic role in thyroid autoimmunity. First, autoimmune-related inflammation may promote excess ROS production and enhanced oxidative stress in thyroid tissue via activation of T and B lymphocytes infiltrating the gland. In fact, it has been demonstrated that Th1 cytokines released by activated lymphocytes (and HT is a Th1-related disorder) induce ROS production by thyrocytes (31,32). Moreover, activated lymphocytes produce excess ROS (33,34). Independent of the origin of the ROS, their accumulation causes oxidative damage of the cells, thereby leading to increased rates of apoptosis, necrosis, and parenchymal destruction, as occurs in other autoimmune diseases (4,5,35,36). Moreover, the antioxidant system is not sufficient to counteract ROS overproduction, since the antioxidant potential is reduced in HT, even in euthyroid patients (see Baser et al. (19) and the present study).
Second, oxidative stress may play a role in the onset of autoimmune disease. Excess ROS may cause oxidative modifications of proteins, lipids and DNA, which become highly immunogenic and may act as neo-antigens, leading to loss of self-tolerance in genetically predisposed individuals (37,38). As demonstrated in vitiligo (39), oxidative stress imbalance may also represent a pathogenetic link between environmental agents and autoimmune disease in HT: increased ROS production due to environmental agents (i.e., iodine excess, radiation, drugs, pollutants) could induce a modification of tissue proteins, or might dysregulate the immune system, influencing the expression of the autoimmune disorder.
Finally, the present study evaluated the serum levels of AGEs and AOPPs as potential new markers of oxidative stress in HT, since no data are available in the literature. To date, studies evaluating oxidative stress in thyroid diseases had studied different parameters of oxidative stress mainly related to lipid peroxidation, and have yielded conflicting results (8,9,13,14,18,19). Searching for new markers of oxidative stress is an area of growing interest, and novel molecules, such as ischemia modified albumin, have been recently proposed (19,40 –42).
AGEs and AOPPs, compounds formed by the transformation of proteins, share similar formation mechanisms and biological effects, and are considered to have a role in inflammatory processes and immune dysregulation (20,21,24). AGEs are composed of a heterogeneous group of bioactive compounds (e.g., pentosidine, carboxymethyl lysine, and imidazolone) that are formed by nonenzymatic glycation of macromolecules (20). AGEs are involved in the pathogenesis of diabetic complications, since their formation is markedly increased in hyperglycemia (43). However, there is increasing evidence that AGEs also play a role in the pathogenesis of other diseases involving oxidative stress and inflammation, including autoimmune diseases (24,44 –46). Moreover, increased serum levels of the soluble AGEs receptor were found in obese children and correlated with TSH levels, suggesting that oxidative stress may be involved in the development of obesity and thyroid dysfunction, at least in children (47). AOPPs are proteins (predominantly albumin and its aggregates) that are damaged by oxidative stress. They contain abundant dityrosines, which enable cross-linking, disulfide bridges, and carbonyl groups and are mainly formed by chlorinated oxidants (hypochlorous acid and chloramines) resulting from myeloperoxidase activity (21,24). AOPPs and AGEs are relatively stable molecules that can be measured by fast and inexpensive techniques, which makes them suitable markers to monitor oxidative stress (20,21,24,43 –46).
This study found higher serum levels of AGEs in HT patients than in healthy controls, although the serum levels of AOPPs in patients were similar to those of controls. The different behavior observed for these two biomarkers is very likely due to the activation of specific biochemical pathways (e.g., the myeloperoxidase pathway) associated with the disorder under study. In HT patients, AGEs serum levels were inversely correlated with serum antioxidant potential, and in multivariate analysis, they were significantly associated with TPOAb positivity. To the authors' knowledge, this is the first study showing the possible involvement of AGEs in HT. These results suggest that AGEs are potentially valuable markers to monitor the level of oxidative stress in HT because their determination is simple, fast, and inexpensive, and the analysis can be performed routinely in the laboratory.
In conclusion, oxidants are increased and antioxidants decreased in euthyroid HT. As a result, the oxidative/antioxidative balance is shifted toward the oxidative side. Moreover, this study reports for the first time on increased serum levels of AGEs in HT, thus contributing to a better definition of the redox homoeostasis dysregulation in this autoimmune disorder. AGE levels could be used as new reliable biomarkers of oxidative stress in HT. Finally, the present data suggest that antioxidant supplementation may be helpful in providing protection from HT. However, other studies are needed to monitor oxidative stress parameters during treatment and to support further the therapeutic use of antioxidants, whose role in HT patients remains open to debate.
Footnotes
Author Disclosure Statement
There is no potential conflict of interest, and the authors have nothing to disclose.