
Abstract
Background:
Mild subclinical hypothyroidism (SCH) affects a large number of people and is known to be a risk factor for dyslipidemia. However, whether mild SCH patients should be treated with L-thyroxine to improve lipid profiles remains controversial. In addition, it is also unclear whether all mild SCH patients can benefit from L-thyroxine treatment, regardless of basal thyrotropin or lipid levels. This study aimed to assess the effects of L-thyroxine replacement therapy on the lipid profiles of mild SCH patients.
Methods:
This open-label randomized controlled trial was performed in Ningyang County, Shandong Province, China. A total of 378 mild SCH patients with diagnoses confirmed by two thyroid function tests were randomly assigned to either the intervention group (L-thyroxine replacement therapy) or the control group (no treatment). The primary outcome was a change in serum total cholesterol (TC) concentration.
Results:
In all, 369 participants completed the 15-month follow-up period. Reduced TC concentrations were more prominent in the intervention group than they were in the control group (–0.41 mmol/L vs. −0.17 mmol/L; p = 0.012), and changes in low-density lipoprotein cholesterol levels exhibited the same trend. Subgroup analyses were performed to assess the effects of L-thyroxine in patients with different thyrotropin or TC levels. When the study population was stratified according to basal thyrotropin concentration, all patients who had received L-thyroxine showed reduced TC levels (p < 0.001). The treatment was similarly beneficial for all patients, regardless of basal TC level. Even for subjects with TC levels <5.18 mmol/L, serum TC concentrations remained unchanged in the intervention group (p = 0.936) but increased by 0.35 mmol/L in the control group (p = 0.004).
Conclusions:
The findings suggest that mild SCH patients could benefit from L-thyroxine treatment to improve lipid profiles, regardless of basal thyrotropin or TC concentrations.
Introduction
A
Mild SCH is often concomitant with dyslipidemia and is also considered an independent risk factor for the development of cardiocerebrovascular disease (11 –14). For instance, a PreCIS database study clarified that all-cause mortality was 18% higher for mild SCH patients compared with that of euthyroid subjects (11). Similarly, the coronary heart disease mortality of mild SCH patients was 1.53 times higher than that of subjects with normal thyroid function in a large-scale meta-analysis (12). The authors’ previous studies demonstrated that even within the reference range, TSH was positively related to an atherogenic lipid profile independent of thyroid hormones (15,16). In addition, it has also been shown that TSH could directly regulate lipid metabolism in the liver (17 –19). Because observational studies have indicated that mild SCH is associated with dyslipidemia, it is essential to identify the extent to which L-thyroxine replacement therapy can benefit mild SCH patients by improving their lipid profiles. Previous studies examining the effects of L-thyroxine on serum lipids in mild SCH have generated inconsistent results (20 –23). Some studies have reported reduced lipid levels (20,21), whereas others have failed to find any beneficial effects (22,23). In addition, lipid improvements appear to occur primarily in a subset of mild SCH patients, for example subjects with a TSH close to 10.0 mIU/L or those who also exhibit hypercholesterolemia (24 –26). In fact, due to the relatively small sample sizes, most of the previous RCTs did not perform further subgroup analyses. Thus, it remains unclear whether all mild SCH patients should be treated to improve lipid profiles, regardless of the basal TSH or lipid concentrations before treatment.
Both the guidelines for hypothyroidism and reviews from leading endocrinologists have stated that more prospective RCTs are needed to assess the effects of L-thyroxine treatment in mild SCH patients (4,5,7,8,27). In this context, the present study was performed, and it was demonstrated that mild SCH patients could benefit from L-thyroxine replacement therapy via improved lipid profiles.
Materials and Methods
Study design and participants
This 15-month, open-label RCT was conducted in Ningyang County, Shandong Province of China. The primary screening for thyroid function began in July 2013. All registered Chinese residents aged ≥40 years who had lived in their current residence for at least five years were invited via telephone or door-to-door visits to undergo the screening examination at the recruitment site. Overall, 7405 participants provided a blood sample after having fasted overnight, underwent a medical examination, and were asked to complete a self-report questionnaire.
After the first thyroid function test, 802 subjects were diagnosed with mild SCH, that is, a normal fT4 and a mildly elevated TSH (range 4.2–10.0 mIU/L). After the second thyroid function test, which was completed three months after the first screening, 437 mild SCH patients were identified. Subjects were further excluded based on the following criteria: (i) pregnant or lactating women; (ii) complications or conditions that affect thyroid status or lipid metabolism, such as psychiatric disabilities, acute cardiovascular and cerebrovascular diseases, chronic respiratory diseases, familial hypercholesterolemia, malignant tumors, or severe dysfunction of the liver (alanine aminotransferase and/or aspartate aminotransferase levels >100 IU/L) or kidney (creatinine >105 μmol/L and evaluated glomerular filtration rate <60 mL/min per 1.73 m2, as calculated using the simplified Modification of Diet in Renal Disease equation); (3) taking any medicine in the previous three months that affects the thyroid or lipid metabolism, including statins, fibrates, thyroid hormone, antithyroid drugs, amiodarone, alemtuzumab, lithium, tyrosine kinase inhibitors, interferon, estrogens, androgens, glucocorticoids, nonsteroidal anti-inflammatory drugs, antiepileptic drugs, rifampicin, furosemide, heparin, or β-adrenoceptor blockers; and (4) obviously poor compliance. Ultimately, 378 mild SCH patients were enrolled in the trial.
The ethics committee of the Shandong Provincial Hospital approved the study, and procedures were conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from each participant prior to data collection.
Randomization and masking
Eligible patients were randomly assigned (1.5:1) to the intervention group or the control group to receive either L-thyroxine replacement therapy or no treatment. The randomization was conducted using a computer-generated random sequence. Neither the patients nor the investigators involved in the study were blinded to the treatment allocation.
Procedures
The intervention group received L-thyroxine at an initial dose of 25 μg once daily (50 μg per tablet; Merck Serono, Darmstadt, Germany). Six weeks later, the thyroid function of all the patients in the intervention group was re-evaluated, and the administered doses were adjusted based on the re-evaluation results. Dose adjustment continued until euthyroidism was reached and the median L-thyroxine dose at the endpoint of the study was 50 μg per day (range 12.5–125 μg). The mild SCH patients in the control group were not given any treatment. All the mild SCH patients, in both the intervention group and the control group, were interviewed every three months either face-to-face or by telephone. All patient status updates were recorded, including any diseases, drugs, operations, and obvious life-style changes (e.g., vegetarian diet or intense exercise) that took place during the three months since the previous interview. The final serum lipid profile reevaluation was conducted 15 months after euthyroidism was reached in the intervention group.
Outcomes
The primary endpoint was a serum total cholesterol (TC) concentration change from the baseline level. The secondary endpoints were the changes in other serum lipid parameters during this period, including low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG).
Safety parameters were monitored throughout the study, including heart rate, blood pressure, and a review of systems (e.g., palpitations, chest tightness, dizziness, perspiration, lower back pain, and hunched back) (4,28,29). To address the possible occurrence of adverse effects, an emergency contact was provided. Endocrinologists offered professional consultations, and hospitalization could be arranged, if necessary. If subjects developed persistent symptoms during therapy, these participants were advised to withdraw from the trial.
Details about the blood sample analysis and physical examinations are provided in the Supplementary Methods (Supplementary Data are available online at
Statistical analysis
The target sample size was calculated based on differences in serum TC concentration between the intervention group and the control group. A target of 363 mild SCH patients was calculated with a mean difference of 0.30 mmol/L and a standard deviation of 1.00 mmol/L (30). This calculation assumed a two-tailed α-level of 0.05 and a power of 80% (31).
The data are presented as the mean (standard deviation), median (interquartile range), or number (percentage) based on whether the distribution was skewed, as determined by a histogram. Differences between the intervention group and the control group were compared using Student's t-test, Mann–Whitney U-test, or chi-square test. Differences between baseline and endpoint values were compared using the paired-samples t-test or Wilcoxon's signed-rank test. Two-tailed p-values of <0.05 were considered statistically significant. All statistical analyses were performed using PASW Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL).
To investigate the effects of L-thyroxine on serum TC concentration in patients with various TSH or TC concentrations further, all the mild SCH patients, including those in both the intervention and control groups, were divided into three subgroups according to their baseline TSH or TC concentrations. The serum TSH concentration thresholds were 5.0 mIU/L, 7.0 mIU/L, and 10.0 mIU/L; for serum TC levels, the three subgroups were defined by TC levels <5.18 mmol/L (normal), between 5.18 and 6.20 mmol/L (marginally elevated), or >6.20 mmol/L (elevated) (1). This study is registered with
Results
Baseline clinical characteristics of the study population
From July to December of 2013, 7405 subjects were screened, and 378 mild SCH patients were randomly assigned to either the intervention group or the control group to receive L-thyroxine (n = 215) or no treatment (n = 163), respectively. A total of 369 participants completed the follow-up period and were included in the final analyses (210 patients in the intervention group and 159 patients in the control group); the total dropout rate was 2.38%. Figure 1 illustrates the trial profile. The baseline clinical characteristics of the two groups were similar (Table 1).
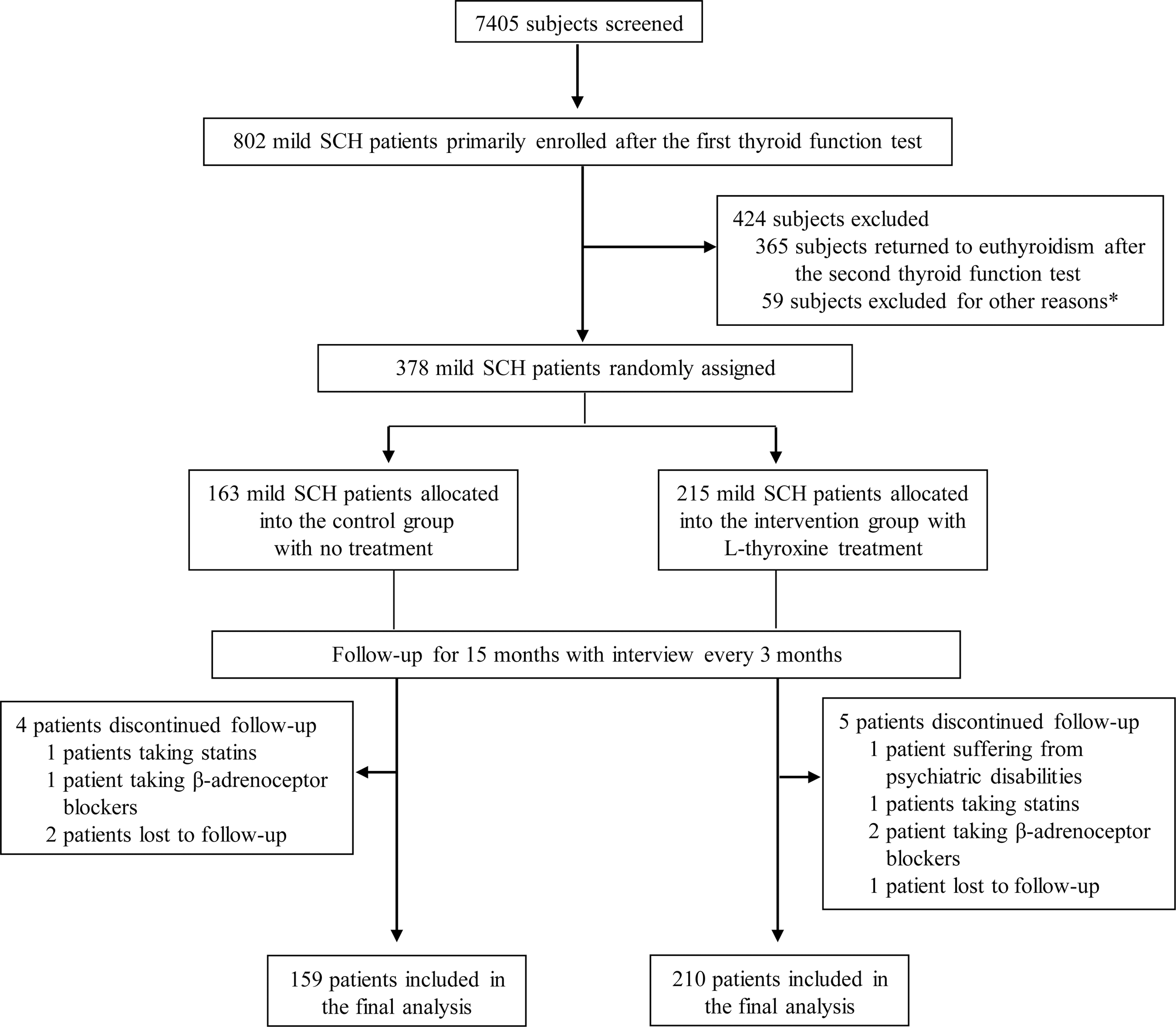
Trial profile. *Reasons for exclusion are given in the Methods section.
p-Values <0.05 were considered significant.
Continuous variables were compared by using Student's t-test or the Mann–Whitney test, and categorical variables by using the chi-square test.
SCH, subclinical hypothyroidism; SD, standard deviation; TC, total cholesterol; TG, triglyceride; IQR, interquartile range; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Cr, creatinine.
Changes in thyroid function and thyroperoxidase antibodies on L-thyroxine replacement therapy
At baseline, the thyroid function of the control group was similar to that of the intervention group (p = 0.378, 0.999, 0.188, and 0.859, respectively, for free triiodothyronine [fT3], fT4, TSH, and thyroperoxidase antibodies [TPOAb]). As shown in Table 2, at the time of the follow-up examination, TSH levels in the control group had naturally slightly decreased, whereas fT3 and fT4 levels had not changed. In the intervention group, L-thyroxine treatment resulted in increased fT4 levels and decreased TSH levels, whereas fT3 levels remained similar to the baseline values. Regarding thyroid autoimmunity, TPOAb levels increased in the control group but remained unchanged in the intervention group. These results suggest that the L-thyroxine replacement therapy seemed to ameliorate thyroid autoimmunity effectively in addition to improving thyroid function. These results are consistent with those of previous studies (32 –34).
p-Values <0.05 were considered significant.
fT3 and fT4 levels were compared by using the paired-samples t-test; TSH and TPOAb levels were compared by using the Wilcoxon signed-rank test.
fT3, free triiodothyronine; fT4, free thyroxine; TSH, thyrotropin; TPOAb, thyroperoxidase antibody.
Serum lipid profiles changes on L-thyroxine replacement therapy
Changes in serum TC concentration were first investigated at the 15-month follow-up. As shown in Figure 2A, serum TC levels had decreased from 5.74 mmol/L to 5.57 mmol/L (p = 0.019) in the control group, whereas serum TC levels in the intervention group decreased from 5.83 mmol/L to 5.42 mmol/L (p < 0.001). The decline in the control group was significantly less than that in the intervention group (–0.17 mmol/L vs. −0.41 mmol/L; p = 0.012; Fig. 2B).
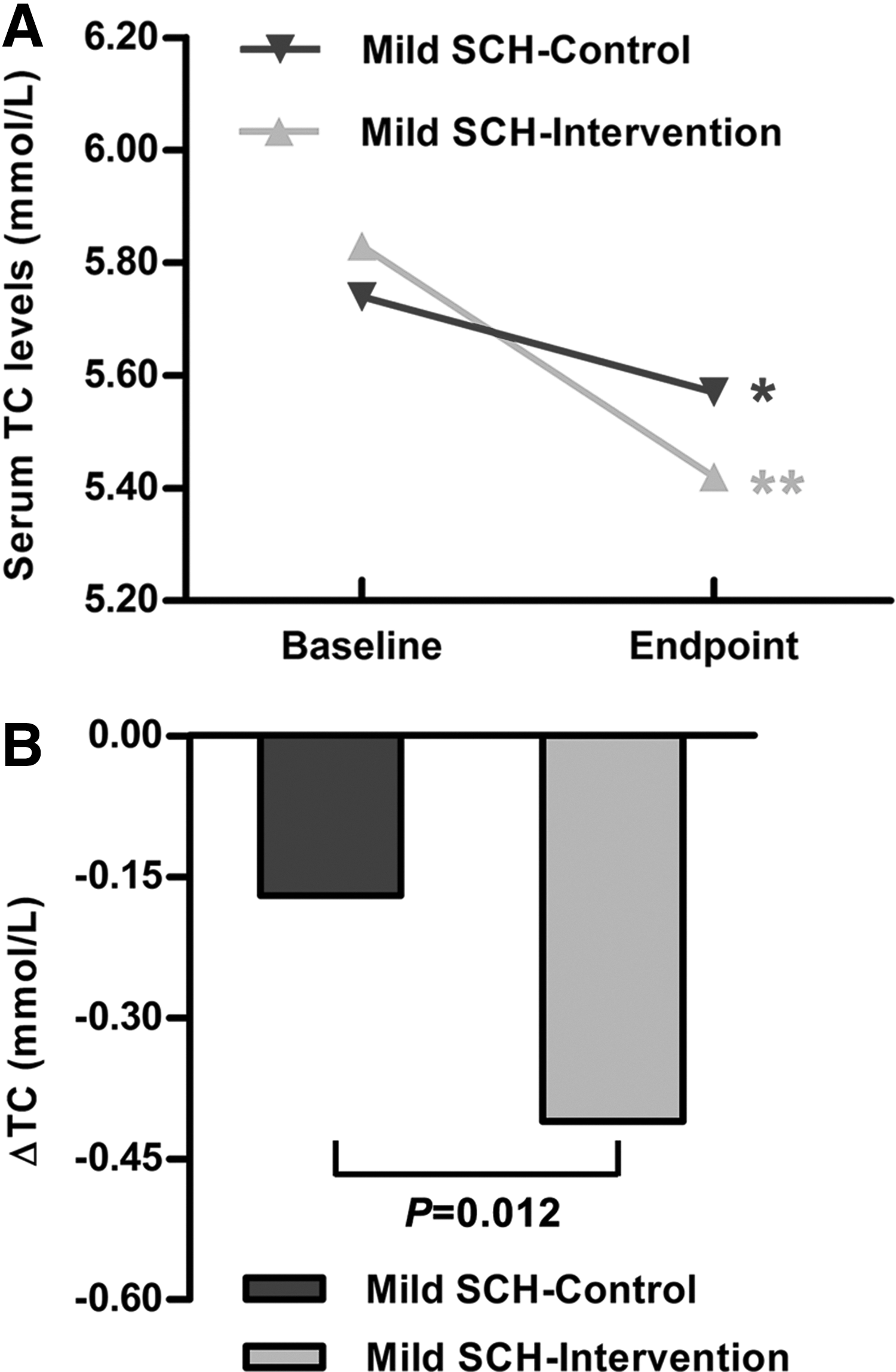
The changes in serum total cholesterol (TC) concentrations in mild subclinical hypothyroidism (SCH) patients. (
Changes in other lipid parameters were also investigated, including LDL-C, HDL-C, and TG. The variation trend of serum LDL-C levels was similar to that of TC levels (Fig. 3A). In the control group, the decline in serum LDL-C levels was not statistically significant (3.31 mmol/L at baseline vs. 3.21 mmol/L at endpoint; p = 0.072), whereas in the intervention group, serum LDL-C levels had decreased significantly (3.34 mmol/L at baseline vs. 3.25 mmol/L at endpoint; p = 0.023). The HDL-C levels had increased in the control group (1.41 mmol/L at baseline vs. 1.48 mmol/L at endpoint; p = 0.001) but had decreased in the intervention group (1.41 mmol/L at baseline vs. 1.36 mmol/L at endpoint; p = 0.001; Fig. 3B). As shown in Figure 3C, serum TG levels had declined in both the control group (1.39 mmol/L at baseline vs. 1.28 mmol/L at endpoint; p < 0.001) and the intervention group (1.32 mmol/L at baseline vs. 1.15 mmol/L at endpoint; p < 0.001). Furthermore, the magnitude of serum TG level change did not differ between the control and intervention groups (–0.11 mmol/L vs. −0.17 mmol/L; p = 0.406).
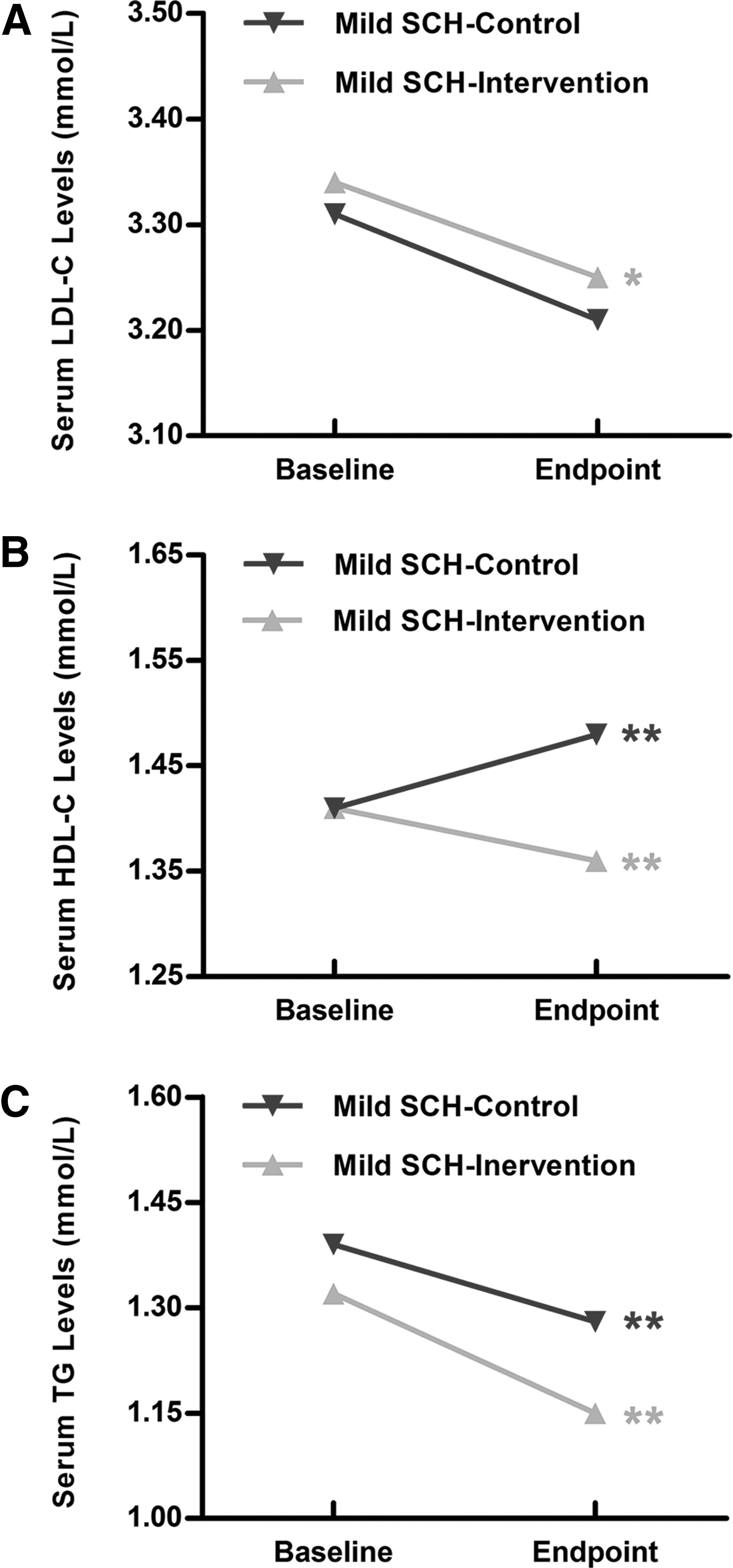
The changes in other lipid parameters, including low-density lipoprotein cholesterol (LDL-C) (
These findings indicate that serum cholesterol levels, including TC, LDL-C, and HDL-C, decreased on L-thyroxine replacement therapy in mild SCH patients, whereas the effects on serum TG levels appeared to be minimal.
Effects of L-thyroxine replacement therapy on serum TC concentration in mild SCH patients with different baseline TSH levels
To explore the effects of L-thyroxine replacement therapy further in mild SCH patients with different baseline TSH levels, TSH levels were stratified into three subgroups (i.e., 4.2 mIU/L < TSH ≤5.0 mIU/L, 5.0 mIU/L < TSH ≤7.0 mIU/L, 7.0 mIU/L < TSH <10.0 mIU/L), and serum TC level changes were compared between the control and intervention groups within each TSH subgroup. As shown in Figure 4, little change in serum TC level was observed in the control group. However, after the L-thyroxine replacement therapy, serum TC levels decreased by 0.41 mmol/L, 0.41 mmol/L, and 0.42 mmol/L (p < 0.001), respectively, in the three intervention subgroups defined above. These results show that the effect of L-thyroxine on serum TC level was similar, regardless of the baseline TSH level.
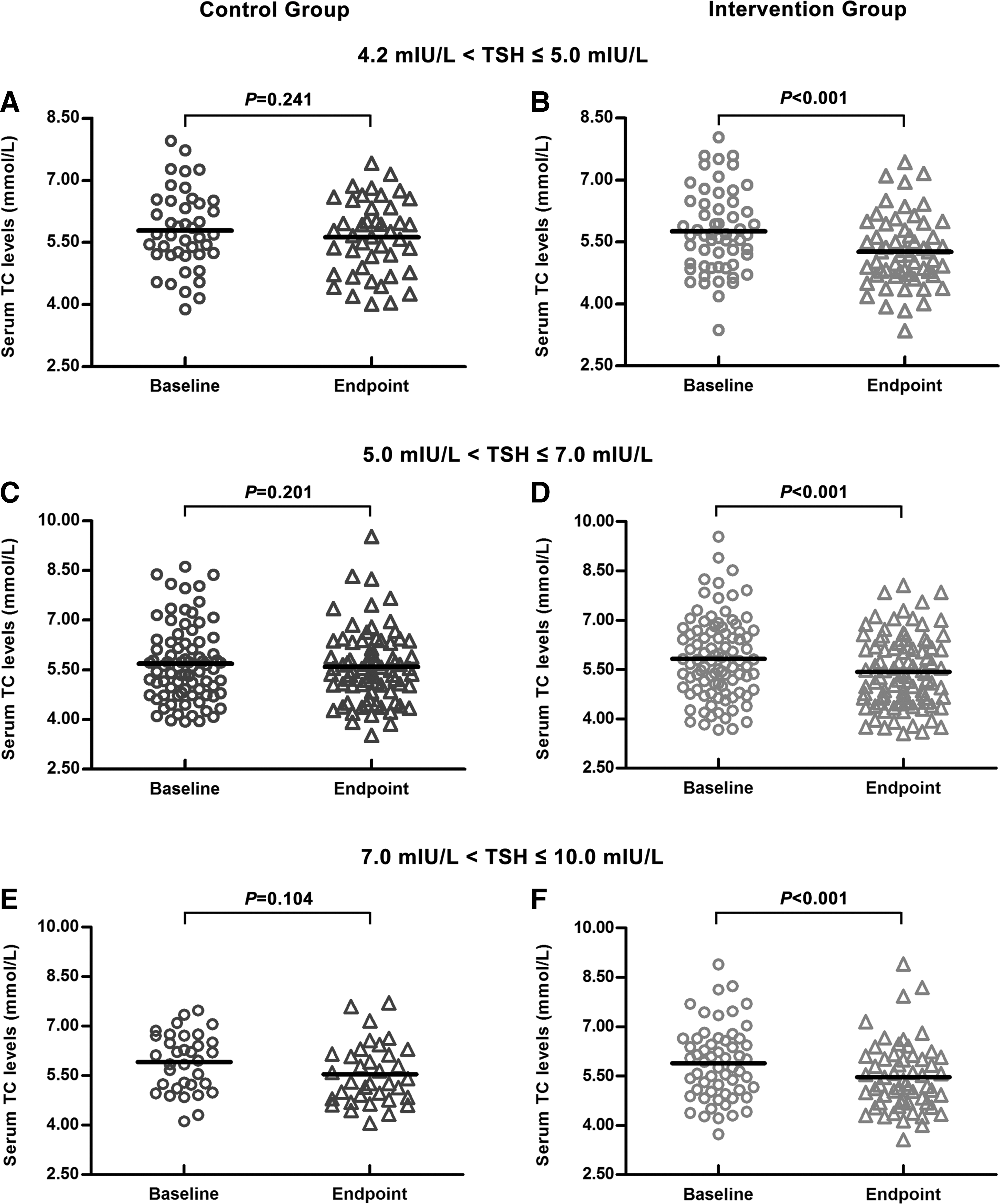
Serum TC concentrations at baseline and at endpoint in thyrotropin <5.0 mIU/L subgroup (
Effects of L-thyroxine replacement therapy on serum TC concentration in mild SCH patients with different baseline TC levels
Serum TC level changes within each TC subgroup were also investigated (i.e., TC <5.18 mmol/L, 5.18 mmol/L ≤ TC <6.20 mmol/L, TC ≥6.20 mmol/L). As shown in Figure 5A and B, in those patients with absolutely normal baseline TC levels (TC <5.18 mmol/L), serum TC levels increased in the control group (4.57 mmol/L at baseline vs. 4.92 mmol/L at endpoint; p = 0.004). However, in the intervention group, serum TC levels remained virtually unchanged (4.57 mmol/L at both baseline and endpoint; p = 0.936). In those patients with marginally elevated baseline TC levels (5.18 mmol/L ≤ TC <6.20 mmol/L), no significant differences were observed in the control group (5.63 mmol/L at baseline vs. 5.48 mmol/L at endpoint; p = 0.088; Fig. 5C), but L-thyroxine decreased serum TC levels in the intervention group (5.67 mmol/L at baseline vs. 5.37 mmol/L at endpoint; p < 0.001; Fig. 5D). Finally, serum TC levels decreased in both the control group and the intervention group (p < 0.001) in those patients with absolutely increased baseline TC levels (TC ≥6.20 mmol/L; Fig. 5E and F). Although the decline in the control group appeared to be less obvious than that in the intervention group, the difference in decline between the two groups was not statistically significant (–0.70 mmol/L vs. −0.88 mmol/L; p = 0.322). These results suggest that mild SCH patients with absolutely normal or marginally elevated TC levels could benefit from L-thyroxine replacement therapy for the prevention or reduction of hypercholesterolemia. Similarly, in the subgroup with elevated TC that received therapy, the changes in serum TC levels appeared to be obvious, though the reduction in the intervention group was not significantly different from that observed in the control group.
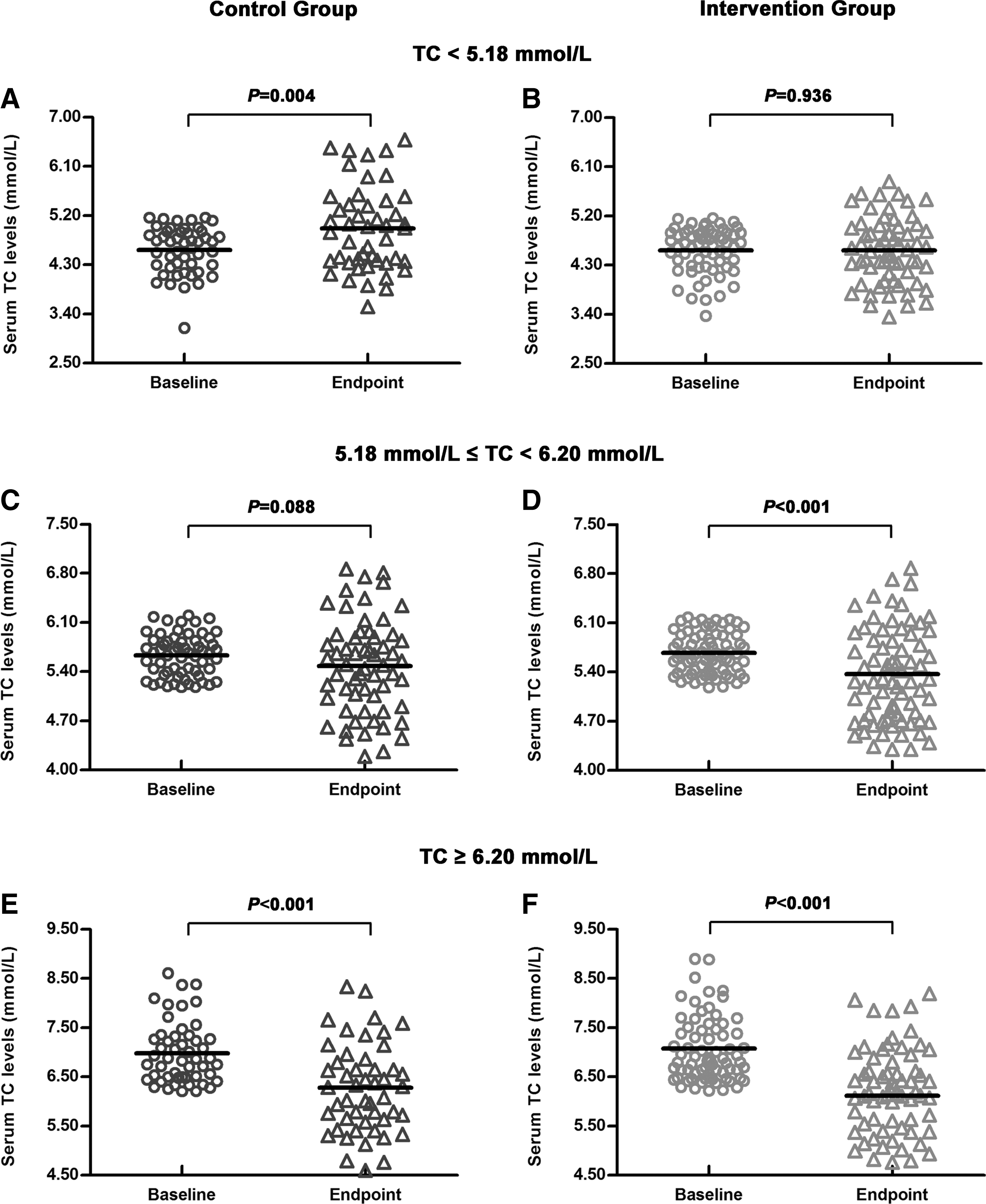
Serum TC concentrations at baseline and at endpoint in TC <5.18 mmol/L subgroup (
Changes in body mass index, heart rate, and blood pressure with L-thyroxine replacement therapy
Details are presented in the Supplementary Data.
Adverse effects during follow-up
The subjects were monitored for potential adverse effects throughout the follow-up period. As shown in Supplementary Table S1, no differences at the endpoint were observed between the two groups in heart rate, blood pressure, or any adverse symptoms (4,28,29,35). No participant attempted to visit a physician or withdraw from the trial due to adverse effects.
Discussion
This study demonstrates that in mild SCH patients, serum TC and LDL-C levels, which are important predictors of cardiocerebrovascular disease, both decreased with the L-thyroxine replacement therapy, though a similar effect on TG concentration was less obvious. Subgroup analyses illustrate that when the study population was stratified according to basal TSH concentration, the L-thyroxine treatment reduced the TC level in each subgroup. Similarly, L-thyroxine was also beneficial for all patients, regardless of the basal TC level. This study suggests that mild SCH patients could benefit from L-thyroxine replacement therapy via improved lipid profiles.
As of yet, this study has the largest sample size of all RCTs investigating the effects of L-thyroxine on serum lipids. Although several clinical studies have been performed to address this problem, the common limitation has been a relatively small sample size (i.e., ≤100 participants) (20 –23). With an insufficient number of participants, these studies might be not representative of the general population, and the results might not be reliable. Furthermore, the conclusions of the above studies have been inconsistent. For instance, Meier et al. observed a decrease in both TC and LDL-C levels after L-thyroxine treatment, which was similar to the present results (20). However, in another study from Brazil, no differences in lipid parameters were observed in the thyroxine group (22). Relatively small sample sizes and inconsistent conclusions might be reasons why these studies did not provide sufficiently powerful evidence to guide clinical practice. Therefore, a large-scale RCT was still necessary. With 369 participants completing a 15-month follow-up, the present study demonstrates a reduction in both TC and LDL-C concentrations after L-thyroxine treatment. These findings may help to improve the management guidelines for mild SCH patients, who form the majority of people with hypothyroidism but to date have not been offered definite therapeutic recommendations.
The subgroup analyses found that serum TC levels could be reduced in all mild SCH patients with L-thyroxine, regardless of basal TSH concentration. This has rarely been reported in previous RCTs. As some other observational studies have indicated, a positive association between SCH and the risk for atherosclerotic disease was observed only in subjects with relatively high TSH levels (e.g., >7.0 mIU/L) (36,37). Based on these results, it was reasonable to assume that the L-thyroxine treatment might benefit only those patients with TSH concentrations close to 10.0 mIU/L. However, the present findings suggest that even patients with slightly elevated TSH concentrations (e.g., 4.2–5.0 mIU/L) could benefit from L-thyroxine replacement therapy.
Another important finding from the subgroup analyses was that L-thyroxine was beneficial for mild SCH patients with basal TC levels <6.20 mmol/L, which has also not been previously demonstrated. However, in the mild SCH patients with hypercholesterolemia (basal TC ≥6.20 mmol/L), the effect of L-thyroxine appeared to be less obvious; that is, a TC level reduction was also observed in the control group, and the decline was not statistically lower than that in the intervention group. There are two potential reasons for the TC decrease in the control group. First, subjects with elevated TC concentrations might pay more attention to ameliorating their hypercholesterolemia by changing their life-style. Second, SCH is naturally reversible in some patients (5), and serum TC levels would decrease following a decrease in TSH concentration. However, this is not to suggest that patients should forgo treatment and wait for natural improvement. Short-term hypercholesterolemia has been identified to induce inflammatory cell dysfunction, impaired endothelium-dependent vasorelaxation, and increased plaque area in the aorta (38,39). Therefore, mild SCH patients with hypercholesterolemia should be treated with L-thyroxine to normalize lipid profiles as soon as possible, thereby reducing the risk for future atherosclerosis.
The reason why we focused on lipid profile changes in the present study is that dyslipidemia plays a crucial role in the development of atherosclerotic disease. As Nakamura et al. suggested, even a moderate decrease in TC concentration (<0.6 mmol/L) is associated with an approximately 30% reduction in the incidence of coronary heart disease (40). Two cohort studies investigating the relationship between SCH and cardiocerebrovascular disease also demonstrated the importance of the lipid profile. The Whickham survey illustrated that SCH patients had an increased incidence of ischemic heart disease and mortality over a 20-year follow-up (41). However, in a 10-year cohort analysis from the Cardiovascular Health Study, no differences between SCH participants and euthyroidism subjects were observed with regard to the incidence of coronary heart disease, heart failure, or cardiovascular death (42). Notably, basal cholesterol concentration was one of the most important differences between the two studies. In the Whickham survey, SCH patients had higher basal TC levels than did euthyroidism subjects. However, in the Cardiovascular Health Study, the baseline LDL-C concentrations were similar between the two groups. It is plausible that different baseline cholesterol concentrations caused the different outcomes in the two studies. This phenomenon indicates that dyslipidemia is an important intermediate link between SCH and cardiocerebrovascular disease. Therefore, amelioration of dyslipidemia followed by thyroid dysfunction at an early stage might contribute to the primary prevention of cardiocerebrovascular disease.
In addition to dyslipidemia, SCH facilitates atherosclerosis in many aspects. In a series of previous studies, it was found that TSH could regulate lipid metabolism in the liver (17 –19), induce the secretion of brain natriuretic peptide in the ventricle (43), and promote inflammation responses in macrophages (data not shown). Additionally, the authors’ clinical studies clarified that SCH might not only worsen the effects of aging on serum lipid profiles but also result in an abnormal, atherogenic circulating microRNA expression profile (44,45). Together with the results of the present study, it is suggested that normalizing thyroid function with L-thyroxine might prevent atherosclerotic disease in SCH patients.
According to the diagnostic recommendations from hypothyroidism management guidelines and previous studies (7,20,22), mild SCH patients were recruited based on two consecutive thyroid function tests. It was found that only approximately 55% (437/802) of the initial group of mild SCH patients were again diagnosed with mild SCH on the second test. This percentage was similar to those of the other clinical trials (46,47). It is speculated that there might be two reasons for the “remission” of SCH. First, some subjects might not be “true” mild SCH patients, with TSH levels around the upper limit of the reference range. At the first test, their TSH levels might have been determined to be slightly above the limit, and the TSH concentrations might have fallen back into the reference range by the time of the second test. Second, as Cooper and Biondi demonstrated, SCH is naturally reversible in some patients (5). Therefore, serum TSH levels might have been transiently elevated in these patients at the time of the initial test but have returned to normal by the time of the second test. This is precisely the reason why we performed two tests during the recruitment stage.
The present results demonstrate that mild SCH patients could benefit from L-thyroxine replacement therapy by improving dyslipidemia, especially hypercholesterolemia, which is a key risk factor for cardiocerebrovascular disease (1,2,40). However, this is just the first step. The trial, with more medical centers involved and sample sizes enlarged, will go on to observe the effects of L-thyroxine on other crucial markers for atherosclerosis, and finally identify whether treatment could decrease the incidence and mortality of cardiocerebrovascular disease in mild SCH patients. Only once further data are available, will it be possible to make more definitive recommendations about whether mild SCH patients should be given long-term therapy or when the treatment should be stopped after a limited intervention. The absent evidence from RCTs (i.e. large-scale, multicenter, long-term, prospective, taking cardiocerebrovascular disease as the primary endpoint) might be the reason why no definite recommendations could be established for mild SCH patients in currently available guidelines for hypothyroidism (4,7,8).
One of the most important strengths of this study is the relatively large sample size, which helped the differences between the intervention group and the control group to be discovered (48). The relatively large number of participants also made it possible to perform subgroup analyses to explore the effects of L-thyroxine in subjects with different baseline TSH or TC levels. Certain potential limitations also exist in this study. The endpoint was a change in lipid concentration, which is an intermediate step in atherosclerosis development. However, as discussed above, dyslipidemia is a significant cardiocerebrovascular risk factor (1,2), and reducing hypercholesterolemia is a key aspect of the prevention of atherosclerotic disease (40). Therefore, it is essential to observe the effects of L-thyroxine on lipid profiles. A long-term, prospective RCT with cardiocerebrovascular events as the primary endpoint is currently being performed, and the results will help to provide more definitive recommendations for mild SCH patients.
In summary, this study illustrates that L-thyroxine treatment results in significantly decreased serum TC and LDL-C levels in mild SCH patients. These results might provide reliable and important data for evidence-based medicine to help clinicians offer effective treatment advice to mild SCH patients. A long-term, prospective RCT is necessary to investigate the effects of L-thyroxine replacement therapy on cardiocerebrovascular events (49,50).
Footnotes
Acknowledgments
This research was supported in part by grants from the National Natural Science Foundation (81230018, 81270869, 81370891 and 30901461), Wu Jieping Medical Foundation, International Scientific and Technologic Cooperation Program of Shandong Province (2011), Scientific and Technologic Development Program of Shandong Province (2012GSF11824), and Self-Independent Innovation Program for Colleges, Universities and Scientific Research Institutes in Jinan City (201202030).
Author Disclosure Statement
No competing financial interests exist.