
Abstract

In a recent prospective paper carried out at our institutions (1), we reported frequent occurrence of hypothyroidism and thyroid autoimmunity in metastatic sunitinib-treated carcinoma patients followed for 18 months. While it is well known that sunitinib-induced adverse events mainly occur during the first year (2,3) and then decrease in frequency, scant data are available for long-term effects of sunitinib on thyroid function (4). Thus, we extended the study of sunitinib-induced thyroid dysfunction to 30 months of sunitinib administration.
We enrolled 28 consecutive patients aged 51–77 years (median age = 57.7 years), 27 with metastatic renal cell carcinoma and one with gastrointestinal stromal tumor with comparable tumor stage of the metastatic disease, normal thyroid parameters (thyroid function and autoimmunity), and thyroid ultrasound. Blood samples were collected before and at the end of the period of sunitinib administration, at monthly intervals up to 30 months (median 16.5 months; range 2–30 months). Thyrotropin (TSH; reference range 0.4–4.0 mIU/L), free triiodothyronine (1.8–4.2 pg/mL), free thyroxine (0.9–1.9 ng/dL), and antithyroglobulin (0–20 IU/mL) and antithyroid peroxidase autoantibodies (TPOAb; 0–35 IU/mL) were measured by an ultrasensitive chemiluminescent assay (Immulite 2000; Siemens). Non-parametric tests (Mann–Whitney test) were used to compare different groups. The hazard ratio and confidence interval were estimated by stratified Cox proportional-hazards regression. Statistical significance was considered at p < 0.05.
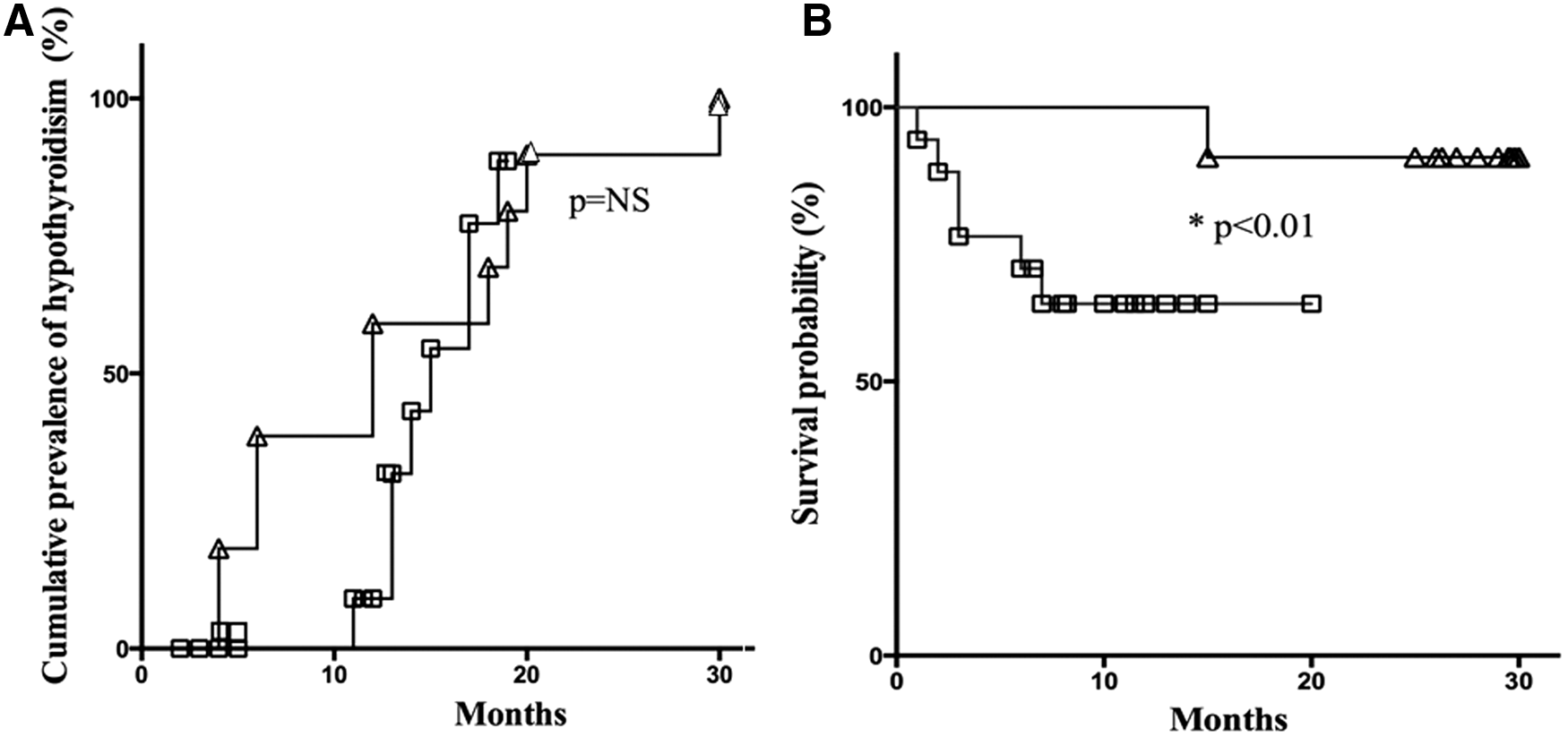
Of the 28 patients, six (21%) patients died after two to five months of treatment, with no evidence of thyroid dysfunction and thyroid autoimmunity; 20 (74%) patients developed variable degree of primary hypothyroidism (TSH 7–114 mIU/L) requiring levothyroxine (LT4) therapy; and 11 (39%) patients developed mild to elevated TPOAb titers (86–3000 IU/mL), which persisted over all follow-up periods independently from LT4 therapy. As previously reported, TPOAb-positive patients developed more profound hypothyroidism (median TSH at diagnosis: 14.1 mIU/L, range 7.0–114 mIU/L vs. 8.8 mIU/L, range 6.5–19.2 mIU/L, in TPOAb-negative hypothyroid patients; p < 0.01, Mann–Whitney test). As shown in Figure 1A, hypothyroidism appeared earlier in TPOAb-positive compared with TPOAb-negative patients, but the cumulative prevalence of thyroid failure was similar in the two groups of patients (100% in TPOAb-positive and 81% in TPOAb-negative patients; p = n.s.) at the end of the follow-up period. As shown in Figure 1B, the survival probability of TPOAb-positive patients was significantly higher when compared with TPOAb-negative patients (p < 0.01).
(
In conclusion, our observation with a follow-up of up to 30 months confirmed that sunitinib is able to trigger persistent thyroid autoimmunity, which may contribute to thyroid damage and concur with the drug toxicity to exacerbate hypothyroidism. In addition, this extended follow-up period showed that the appearance of hypothyroidism was earlier in TPOAb-positive than it was in TPOAb-negative patients, but the cumulative prevalence was similar, provided that sufficient time has elapsed. More importantly, we confirm and extend our preliminary observation that development of thyroid autoimmunity and more severe thyroid dysfunction is associated with longer survival, and may therefore represent a biomarker of oncological response.
Footnotes
Acknowledgments
This work was partially supported by funds of the University of Cagliari (Contributo di Ateneo della Ricerca) to S.M.
Author Disclosure Statement
The authors have nothing to disclose.