
Abstract
Background:
Gallium-68 (Ga-68) DOTATATE is a radiolabeled peptide–imaging modality that targets the somatostatin receptor (SSTR), especially subtype 2 (SSTR2). Benign and malignant thyroid tumors have been observed to express SSTR. The aim of this study was to evaluate the frequency and clinical significance of incidental atypical thyroid uptake as detected by Ga-68 DOTATATE positron emission tomography/computed tomography (PET/CT).
Methods:
A retrospective analysis was conducted of a prospective study in which 237 patients underwent Ga-68 DOTATATE PET/CT as part of a work-up for metastatic and unknown primary neuroendocrine tumors. The types of uptake in the thyroid gland (focal/diffuse) and maximum standardized uptake value (SUVmax) levels were evaluated and compared with the background uptake in the liver and salivary glands.
Results:
Of 237 patients, 26 (11%) had atypical thyroid uptake as detected by Ga-68 DOTATATE PET/CT. There were no significant clinical or biochemical variables associated with atypical thyroid uptake. Fourteen (54%) patients had positive focal uptake, and 12 (46%) patients had diffuse uptake. Of the 14 patients with atypical focal uptake, 10 (71%) had thyroid nodules on the corresponding side, as detected by anatomic imaging. Three of 10 patients (21%) were found to have papillary thyroid cancer, and seven (70%) had adenomatoid nodules. Of the 12 patients with diffuse increased uptake, six (50%) had a history of hypothyroidism, five (42%) had chronic lymphocytic thyroiditis, and one (8%) had nontoxic multinodular goiter.
Conclusions:
Patients with an incidental focal abnormal thyroid uptake on Ga-68 DOTATATE PET/CT scan should have further clinical evaluation to exclude a diagnosis of thyroid cancer.
Introduction
T
Gallium-68 (Ga-68) DOTA peptide PET scanning is becoming the primary imaging modality for identifying neuroendocrine tumors (NETs) in Europe and, more recently, the United States. The sensitivity and specificity of detecting NETs has been reported to be as high as 96% and 100%, respectively (5,6). Several Ga-68 DOTA peptides (DOTATATE, DOTATOC, DOTANOC) have been used, with DOTATATE found to be the most accurate (5). While there is some published research on Ga-68 DOTATATE PET/computed tomography (CT) scanning in patients with medullary thyroid cancer and differentiated thyroid cancer to detect sites of persistent/recurrent or metastatic disease (7,8), the frequency and clinical significance of incidental uptake in the thyroid gland in patients without a history of thyroid cancer are unknown.
This study systematically characterized and quantitated thyroid uptake in a prospective cohort of patients undergoing Ga-68 DOTATATE PET/CT scanning to detect unknown primary or metastatic NETs.
Patients and Methods
The patients were enrolled in a clinical protocol (NCT01967537) after written informed consent was obtained. This prospective study was performed under an investigational new drug protocol approved by the United States Food and Drug Administration. The study was reviewed and approved by the National Cancer Institute review board and the National Institutes of Health Radiation Safety Committee.
A total of 237 patients participated in the study from October 2013 to September 2015. The demographic and clinical characteristics are summarized in Table 1. The laboratory work-ups included measurements of serum chromogranin A, the pancreatic polypeptide, vasoactive intestinal polypeptide, fasting serum gastrin, calcitonin, insulin, glucagon, dopamine, 24-hour urinary 5-hydroxyindoleacetic acid (5-HIAA), epinephrine, norepinephrine, fractionated metanephrine, normetanephrine, and total metanephrine. Anatomic imaging included a triple phase CT of the chest, abdomen, and pelvis with intravenous contrast, and magnetic resonance imaging in patients with renal insufficiency. Selected patients with abnormal thyroid uptake based on Ga-68 DOTATATE PET/CT underwent a thyroid US.
NET, neuroendocrine tumor; MEN1, multiple endocrine neoplasia type 1; VHL, von Hippel–Lindau.
Evaluation and analysis of thyroid uptake as detected by Ga-68 DOTATATE PET/CT
The Ga-68 DOTATATE scans were performed as previously described (9,10). Five mCi of Ga-68 DOTATATE was administered through a peripheral vein. After approximately 60 minutes, the patient was placed in a supine position in a PET/CT scanner (Siemens Medical Solutions USA, Inc., Malvern, PA), and images from the upper thighs to mid-skull (including pituitary gland) were obtained. A low-dose, non-contrast CT was used for attenuation correction and anatomic localization. Maximum standardized uptake value (SUVmax) levels were measured based on patient total body weight.
Two providers independently reviewed all of the Ga-68 DOTATATE PET/CT scans and classified the thyroid uptake status. The blinded reads were compared, and a board-certified nuclear medicine physician (C.M.) provided validation of all imaging assessments. Thyroid uptake was classified as diffuse or focal. Normal thyroid uptake was defined as having a SUVmax that was below that of the liver and salivary glands. Abnormally increased uptake was defined as focal and diffuse uptake, with SUVmax levels greater than those of the liver or salivary glands.
Data analysis
The Ga-68 DOTATATE PET/CT uptake status was analyzed by patient demographic, clinical characteristics, familial versus sporadic NETs, history of thyroid disease or neoplasm, and biochemical laboratory data. Spearman's correlation coefficient, Student's t-test, and chi-square tests were used to test for associations between variables and abnormal Ga-68 DOTATATE PET/CT SUV. A p-value of <0.05 was considered statistically significant. IBM SPSS Statistics Data Editor (Armonk, NY) and Microsoft Excel (Redmond, WA) were used for statistical analysis.
Results
Of the 237 patients enrolled, 26 (11%) had an abnormal uptake, as detected by Ga-68 DOTATATE PET/CT: 14 patients had focal uptake (53.8%), and 12 patients had diffuse uptake (46.2%). Of the 14 patients with focal uptake, as detected by Ga-68 DOTATATE PET/CT scan, 10 underwent an US of the thyroid gland (Fig. 1). Of these 10 patients, three were found to have differentiated thyroid cancer (average SUVmax 10.3, range 6.1–14.7). Of the remaining seven patients with benign thyroid tumors (average SUVmax 10.3, range 5.8–22.4), six underwent FNA biopsy, and two of six patients underwent a hemithyroidectomy. In all six patients, the diagnosis was consistent with benign adenomatous nodules based on cytology or histology. The remaining patient was found to have an inhomogeneous thyroid gland on US, and no biopsy was recommended because the thyroid nodules were <1 cm and or had no US suspicious features for thyroid cancer. One of the three patients with papillary thyroid cancer (PTC), who had focal uptake, had bilateral focal uptake, with a SUVmax of 12.3 in the left thyroid lobe and a SUVmax of 10.2 in the right. The patient underwent an FNA biopsy of the bilateral thyroid nodules and was found to have PTC in the right thyroid lobe. The patient underwent a total thyroidectomy, and pathology showed a 1.1 cm PTC in the right thyroid lobe and a papillary microcarcinoma (2 mm) in the left thyroid lobe. The second patient was a 38-year-old woman with von Hippel–Lindau disease who was found to have a left thyroid nodule, with a SUVmax of 18.7, based on 18F-FDG PET. Ga-68 DOTATATE PET/CT showed focal uptake in the left thyroid lobe, with a SUVmax of 8.18, and an isthmus nodule, with a SUVmax of 14.7. She underwent an FNA biopsy of the left thyroid nodule, which was suspicious for PTC. Total thyroidectomy was performed, and the patient was found to have multicentric PTC and chronic lymphocytic thyroiditis. The third patient was a 64-year-old woman with an incidentally found right thyroid nodule, with a SUVmax of 6.1, as detected by Ga-68 DOTATATE PET/CT. The FNA biopsy showed PTC, and the patient underwent a total thyroidectomy, with pathology showing a follicular variant of PTC.
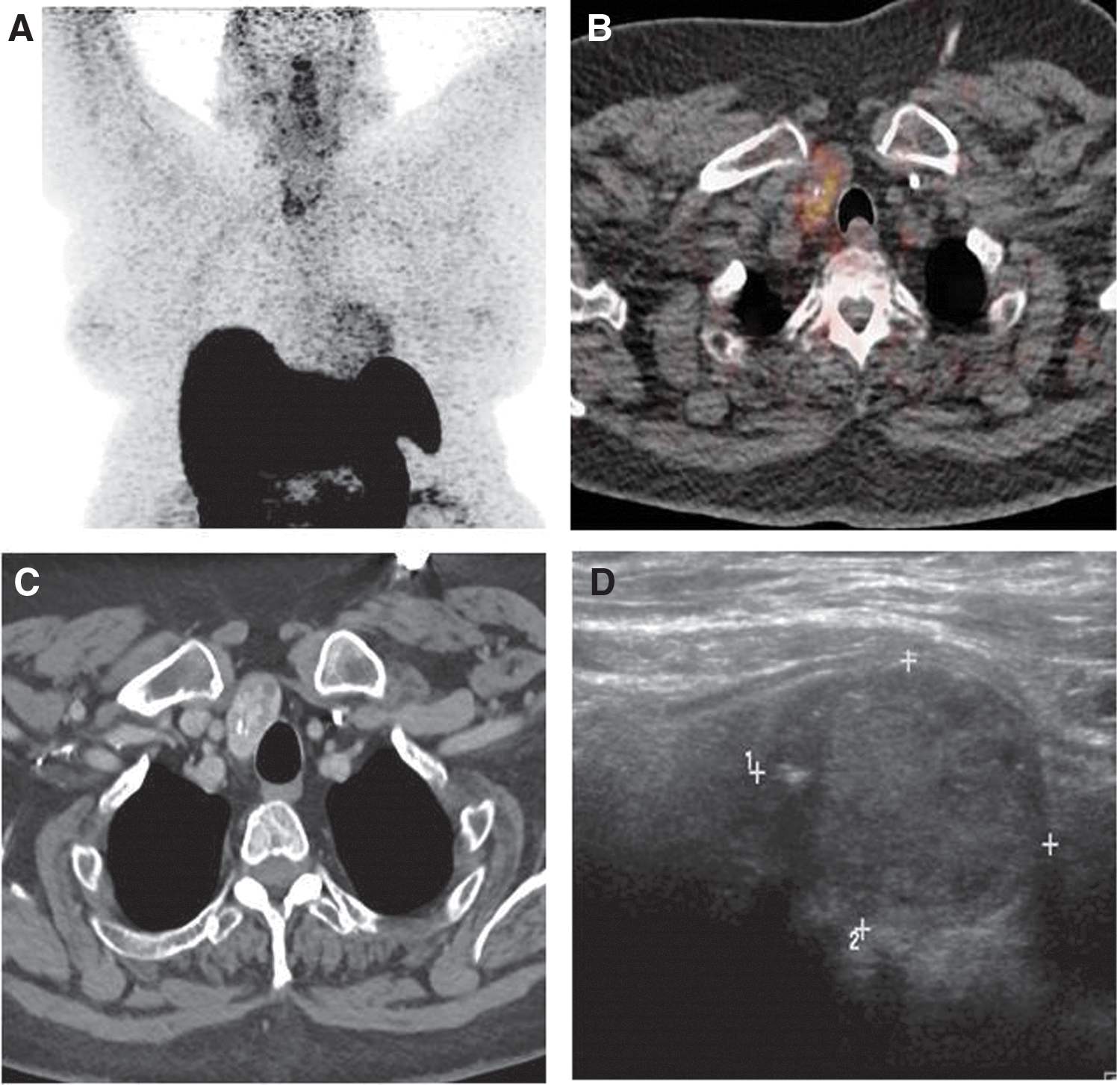
Representative image of a right incidentally detected thyroid nodule. (
Of the 12 patients with diffuse abnormal uptake, six had anatomic imaging with thyroid US, and four were found to have multinodular goiters. Two of the patients underwent FNA biopsies that showed adenomatous nodules, and the thyroid nodules in the rest of the patients were too small to warrant FNA biopsies. Five of 12 patients with diffuse abnormal uptake had a history of hypothyroidism.
Ga-68 DOTATATE PET/CT scanning showed no statistically significant difference in the average SUVmax levels between benign and malignant thyroid nodules based on histology and/or cytology. In addition, no significant association was found of Ga-68 DOTATATE PET/CT focal or diffuse thyroid uptake status associated with patient demographics, clinical characteristics, or biochemical profiles.
Discussion
This study found that 11% of patients who underwent Ga-68 DOTATATE PET/CT scanning had abnormal uptake in the thyroid gland. In patients who had further clinical evaluation of focal abnormal thyroid uptake, 3/14 (21%) had thyroid cancer and 7/14 (50%) had benign thyroid tumors or lymphocytic thyroiditis. In patients who had diffuse abnormal thyroid uptake, 42% had a history of hypothyroidism. These findings suggest that patients with an incidental focal abnormal thyroid uptake as determined by Ga-68 DOTATATE PET/CT scan should have further clinical evaluation to exclude a diagnosis of thyroid cancer.
The physiologic Ga-68 DOTA peptide biodistribution, in contrast to 18F-FDG, involves diffuse thyroid gland uptake because SSTR is expressed in normal thyroid tissue (6). In the authors’ experience, the thyroid activity is equal to or is below the salivary glands uptake and/or the liver uptake. Atypical patterns of uptake observed in the current population were: (i) diffusely increased homogeneous or heterogeneous uptake above the salivary glands and liver, and (ii) focal increased uptake within a homogeneous thyroid background. These two patterns of uptake described above were considered as abnormal.
Organs such as the small and large intestines, kidneys, the spleen, the liver, adrenal glands, or salivary glands, and an uncinate process of the pancreas are known to have physiological uptake as determined by Ga-68 DOTATATE PET/CT. The SUVs in these organs can be variable. Ga-68 DOTATATE has a high affinity to the somatostatin receptor 2 (SSTR2), which is commonly expressed in NETs (6). Both benign and malignant thyroid tissues also express high levels of SSTR2 (11). Atkinson et al. found high SSTR2 expression in differentiated thyroid cancer cells and benign thyroid disease based on immunohistochemistry analysis (11). Druckenthaner et al. also found predominant expression of SSTR2 in differentiated thyroid cancer based on reverse transcription polymerase chain reaction, which correlated with immunostaining results in 13/16 cases (6). Thus, it is not surprising to find abnormal uptake of Ga-68 DOTATATE in patients who were found to have benign and malignant thyroid neoplasms.
To the authors’ knowledge, there has been no prospective study evaluating incidental uptake of Ga-68 DOTATATE PET/CT in the thyroid gland. Kunikowska et al., in a retrospective study, analyzed the rate of incidental thyroid abnormal uptake as detected by Ga-68 DOTATATE PET/CT, and found that 4.1% of 1150 patients had abnormal uptake. Abnormal uptake in that study was more common in women, but no such sex difference was found in the present study. The investigators found PTC in only 1/147 patients with abnormal focal uptake, which is lower than the 21% of patients with focal uptake found to have PTC in the present cohort. The differences between the current study findings and those of Kunikowska et al. may be due to several reasons. In the present study, all patients were evaluated prospectively, and the imaging results were analyzed in a blinded fashion, with defined parameters for what we called abnormal thyroid uptake, given that there is normal physiological uptake in the thyroid tissue. Lastly, not all patients with abnormal thyroid uptake on Ga-68 DOTATATE PET/CT scanning underwent clinical evaluations and work-ups to ascertain the true rate of thyroid cancer in those patients with abnormal focal uptake (12).
This study has several limitations. The study cohort represents patients with a history of NETs, so the findings would not be generalizable to the general population. However, patients with NETs are the patient population likely to undergo Ga-68 DOTATATE PET/CT scanning. Another limitation is the relatively small sample size, which may not have allowed small statistically significant differences in demographic and clinical characteristics, and/or biochemical profiles that may be associated with abnormal thyroid uptake on Ga-68 DOTATATE PET/CT scanning to be detected. Lastly, not every patient with abnormal uptake in the thyroid gland as detected by Ga-68 DOTATATE PET/CT scanning underwent a clinical evaluation to determine the cause of the abnormal uptake. However, these evaluations would likely lead to an even higher rate of thyroid cancer detected.
In summary, focal abnormal thyroid uptake as detected by Ga-68 DOTATATE PET/CT scanning should be further evaluated with thyroid US, and FNA biopsy if there are suspicious features for malignancy on US examination.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.