
Abstract
Background:
Selenium supplementation may decrease circulating thyroid autoantibodies in patients with chronic autoimmune thyroiditis (AIT), but the available trials are heterogenous. This study expands and critically reappraises the knowledge on this topic.
Methods:
A literature search identified 3366 records. Controlled trials in adults (≥18 years of age) with AIT, comparing selenium with or without levothyroxine (LT4), versus placebo and/or LT4, were eligible. Assessed outcomes were serum thyroid peroxidase (TPOAb) and thyroglobulin (TgAb) autoantibody levels, and immunomodulatory effects. After screening and full-text assessment, 16 controlled trials were included in the systematic review. Random-effects meta-analyses in weighted mean difference (WMD) were performed for 3, 6, and 12 months of supplementation in two different populations: one receiving LT4 therapy and one newly diagnosed and LT4-untreated. Heterogeneity was estimated using I 2, and quality of evidence was assessed per outcome, using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) guidelines.
Results:
In LT4-treated populations, the selenium group had significantly lower TPOAb levels after three months (seven studies: WMD = –271 [confidence interval (CI) −366 to −175]; p < 0.0001; I 2 = 45.4%), which was consistent at six months (three studies) and 12 months (one study). TgAb decreased at 12 months, but not at three or six months. In LT4-untreated populations, the selenium group showed a decrease in TPOAb levels after three months (three studies: WMD = −512 [CI −626 to −398]; p < 0.0001, I 2 = 0.0%), but not after 6 or 12 months. TgAb decreased at 3 months, but not at 6 or 12 months. Quality of evidence was generally assessed as low. Study participants receiving selenium had a significantly higher risk than controls of reporting adverse effects (p = 0.036).
Conclusions:
Selenium supplementation reduced serum TPOAb levels after 3, 6, and 12 months in an LT4-treated AIT population, and after three months in an untreated AIT population. Whether these effects correlate with clinically relevant measures remains to be demonstrated.
Introduction
T
In humans, the essential trace element selenium exerts direct effects on thyroid hormone metabolism and redox processes (10). The thyroid gland critically depends on iodine and selenium for adequate functioning (11), and low selenium intake is associated with increased risk of thyroid disease (12).
Since 2002, several trials have investigated the effect of selenium supplementation on thyroid autoantibodies in AIT patients. A systematic review from 2010 (13) included four studies (14 –17) in their meta-analysis, showing significantly lower thyroid peroxidase autoantibody (TPOAb) levels after three months of selenium supplementation compared with placebo. A Cochrane Collaboration systematic review from 2013 (18) evaluated change in TPOAb levels following selenium supplementation, but no meta-analysis was performed due to considerable heterogeneity. A Chinese meta-analysis from 2014 (19), which searched three major Chinese databases in addition to Western databases, concluded that both 6 and 12 months of selenium supplementation resulted in a significant decrease in TPOAb as well as thyroglobulin autoantibody (TgAb) levels. However, the authors rated only one of nine included trials as having high quality.
The present study hypothesized that several trials of good quality had not been included in previous systematic reviews. In addition, none of the previous systematic reviews and meta-analyses differentiated between patients with a longer duration of disease from newly diagnosed disease. The objective of this study was to reappraise the available evidence of an effect of selenium supplementation on thyroid autoantibody levels in patients with AIT. The object was addressed both in an LT4-treated as well as in a newly diagnosed patient population not yet treated with LT4. To this end, an extensive literature search was performed in three Western and one Chinese database, with the aim of including all relevant trials in order to identify knowledge gaps and aid decision making.
Materials and Methods
Criteria for considering studies for this review
The inclusion criteria for considering studies for this review were controlled trials in adults (≥18 years of age) with AIT, comparing selenium alone or with LT4, versus placebo alone or combined with LT4 or no treatment. Outcomes of interest were changes in circulating thyroid autoantibody levels (TPOAb and TgAb) and immunomodulatory effects.
Literature search
The following databases were searched on September 23, 2015: Medline (from inception until September 23, 2015), EMBASE (from 1974 until September 22, 2015), and the Cochrane Central Register of Controlled Trials (CENTRAL; from inception until September 23, 2015). In addition, the Chinese database China National Knowledge Infrastructure (CNKI) was searched on September 23, 2015, using the search terms “selenium” AND “Hashimoto” and “selenium” AND “thyroiditis.”
Selection of studies
Records were imported from Medline, EMBASE, and CENTRAL into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia;
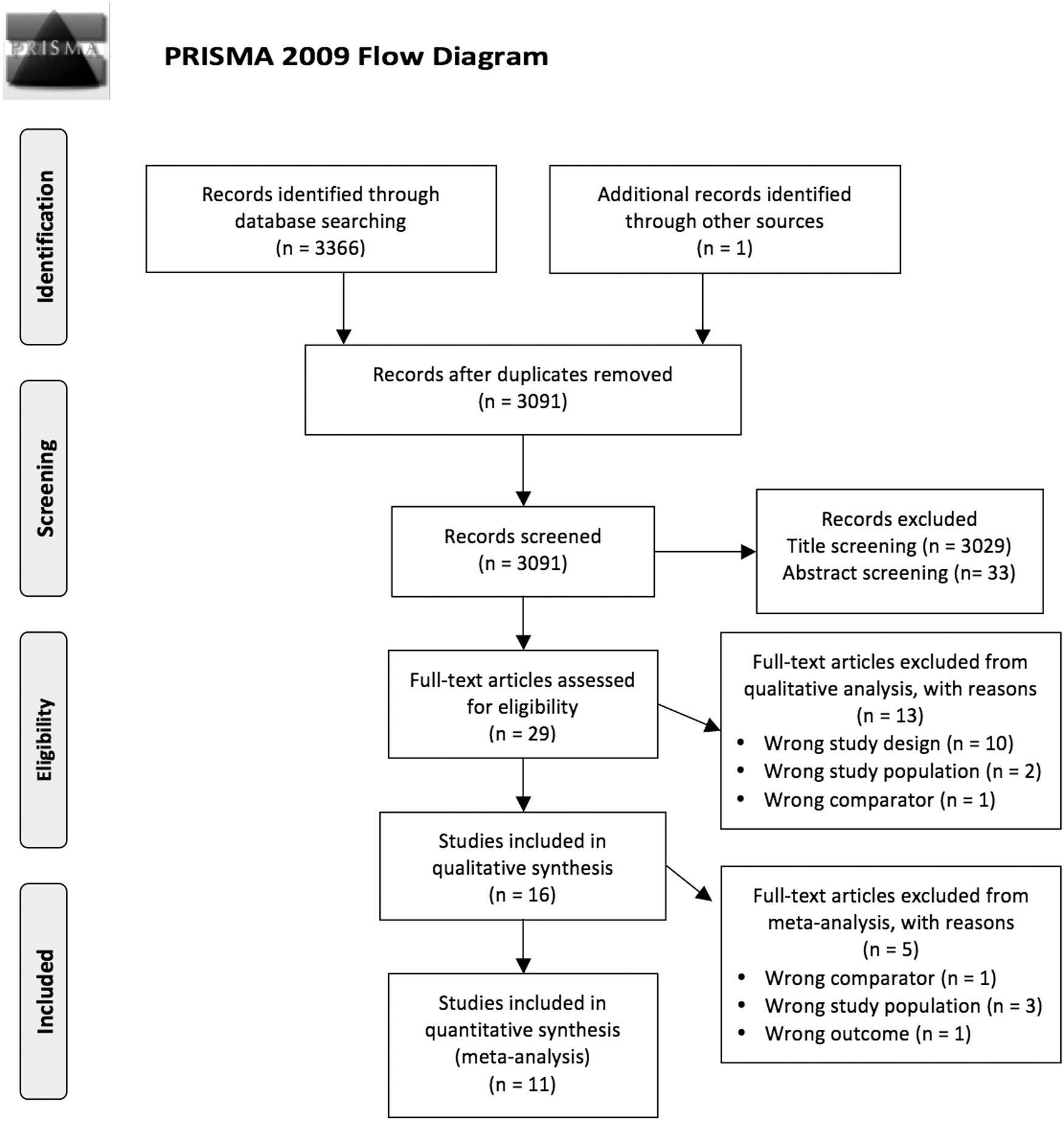
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart of the study selection process, with number of studies excluded at each step in the systematic review and meta-analysis.
Data extraction
For studies that fulfilled the inclusion criteria, two review authors (J.W. and K.W.) independently extracted relevant population and intervention characteristics onto a predesigned template. Where there were further questions regarding one or more of the included trials, an e-mail request was sent to the corresponding author of the study.
Quality of evidence
Quality of evidence was assessed per outcome, independently by two individuals (J.W. and a local consultant, A.A.), using the GRADE guidelines for rating the quality of evidence (20 –28).
Data synthesis
Levels of thyroid autoantibodies (TPOAb and TgAb) at 3, 6, and 12 months of follow-up were extracted as means with standard deviations (SD). Where data were presented as median with confidence interval (CI) (29), an SD was calculated using the formula [(HCI – LCI)/2/TINV(0.05; n – 1)*√(n)], where HCI is the highest value of the CI, LCI is the lowest value of the CI, and n is the sample size of the group (30). Where data were presented as median with interquartile range (IQR) (31), the median was used as the mean, and the SD was calculated by IQR/1.35 (30). One study (31) had two intervention groups (80 and 160 μg selenium), which were combined into a single intervention group (30). One article (32) presented data as cent change. Therefore, the author was contacted, who supplied a data sheet of raw data, which were used to calculate the means and SDs. Two trials by the same authors, using the same result measurements (33,34), had four arms (selenium vs. LT4 vs. selenium + LT4 vs. placebo). The four arms were divided into “Study A” (selenium vs. placebo) and “Study B” (selenium + LT4 vs. LT4) for the meta-analyses, where one was used in the analyses of the population receiving treatment (LT4), and the other in the LT4-untreated population. Meta-analyses in weighted mean difference (WMD) were performed using the follow-up scores at 3, 6, and 12 months in a random-effects model in STATA v13.1 (Stata Corp., College Station, TX).
Heterogeneity
The heterogeneity of the included studies was evaluated with the I2 statistic (35), where 0–40% might not be important, 30–60% may represent moderate heterogeneity, 50–90% may represent substantial heterogeneity, and 75–100% may represent considerable heterogeneity (30).
Meta-analyses
Two meta-analyses were performed for TPOAb and two for TgAb levels, in LT4-untreated populations and in populations receiving LT4, respectively. All forest plots were performed by months of intervention.
Meta-regression analyses
Four meta-regression analyses were performed where the WMD of TPOAb levels at three months was plotted against (i) baseline TPOAb levels (seven studies), (ii) baseline selenium levels (five studies), (iii) baseline age of participants (six studies), and (iv) percentage of females in the population (seven studies). Meta-regression analysis of effect plotted against duration of disease as well as meta-regression analyses of TgAb were planned, but neither could be performed due to insufficient data.
Subgroup analyses of selenium formulation type
Subgroup analysis of TPOAb at three months in an LT4-treated population was performed comparing the effect of 200 μg of selenomethionine (five studies) against the effect of 200 μg sodium selenite (two studies).
Sensitivity analysis
Meta-analysis of TPOAb and TgAb in an untreated population was performed both including and excluding the study by Pilli et al. (31) in order to test if the calculation of a SD from IQR influenced the results. Meta-analyses of TgAb in treated populations including and excluding the studies by Turker et al. (15) and Gärtner et al. (16) were performed, since they had stratified the randomization of the participants according to baseline TPOAb levels, and baseline TgAb levels were therefore not comparable at baseline.
Relative changes of thyroid autoantibodies
The relative changes in TPOAb levels following selenium supplementation for three months in LT4-treated patients were calculated in percent for each study. Selenium groups were compared to control groups across the seven trials using the Wilcoxon signed rank sum test.
Relative risk analysis of adverse effects
Relative risk (RR) was calculated as the probability of an event (adverse effect), occurring in an exposed group (receiving selenium supplementation) compared to an unexposed group (receiving placebo or no treatment).
Registration of systematic review
The systematic review was registered at PROSPERO on August 25, 2015 (
Results
Search results
A total of 3366 records were identified in the Medline, EMBASE, and CENTRAL databases. One article was identified by one of the authors as being from another source (31). All records were imported into the Covidence software platform, and 276 duplicates were removed. Two reviewers (J.W. and K.W.) independently screened the remaining 3091 records, and of these, 3029 records were excluded following title screening, leaving 62 records to be screened by abstract. Of these 62 records, 33 were excluded after abstract screening, leaving 29 articles for full-text assessment. Two articles were ordered from the Medical Research Library at the University of Southern Denmark (14,36). Full-text evaluation was carried out independently by two reviewers (J.W. and K.W.), except for one record, written in Hungarian (36), which was translated by a colleague. Conference abstracts (37 –41), studies among pregnant women (42,43), one study with the wrong comparator (44), and four records with the wrong study design (13,18,19,45) were excluded, with difference of opinion resolved by discussion and consensus. Finally, 16 studies were included in the systematic review. In the meta-analyses, three studies with the wrong study population (46 –48), one with the wrong comparator (49), and one with the wrong outcome (33) were excluded. The screening is presented as a PRISMA flow chart (Fig. 1).
In the search in CNKI, only abstracts could be accessed in English. In the first search, using the search terms “Hashimoto” AND “selenium,” there were 17 hits. In the second search, using the search terms “thyroiditis” AND “selenium,” there were 43 hits. One Chinese article with an abstract in English was identified in the Medline search (50), which was analyzed together with the abstracts found in the CNKI search. None of these abstracts contained sufficient data to be included in a meta-analysis. Therefore, the results, as given in the abstracts, were analyzed qualitatively.
Systematic review
Summary of included studies
The 16 studies included from the search in Medline, EMBASE, and CENTRAL were published between 2002 and 2015, and reported data on 1494 patients with AIT. The main data are summarized in Table 1. All trials were conducted in Europe, except for one in India (48) and one in Brazil (51). One trial was not randomized (49), and two trials did not state whether patients were randomized (47,48). All trials used placebo as a control, except two (29,49) that used no treatment. Six studies were double-blinded (31,33,34,36,51,52), four were described as “blinded” without specification (15 –17,48), two studies were open label (32,46), and four studies did not state whether they were blinded (14,29,47,49). Two studies had two intervention groups and two control groups (33,34), respectively, and one study had two intervention groups and one control group (31). Of the 11 studies included in the meta-analyses, seven used chemiluminescence assays (16,17,29,31,32,36,52), three used radioimmunoassays (14,15,34), and one used fluorometry (51).
Int./con., intervention group/control group; LT4-treated, receiving levothyroxine treatment; Seme, selenomethionine; NaSe, sodium selenite; Se, selenium; TSH, thyrotropin; T3, triiodothyronine; T4, thyroxine; TT3, total T3; TT4, total T4; fT3, free T3; fT4, free T4; TPOAb, thyroid peroxidase autoantibodies; TgAb, thyroglobulin autoantibodies; CXCL-9, −10, and −11, chemokine (C-X-C motif) ligand 9, 10, and 11; TNF-α, tumor necrosis factor alpha; IL-1β, interleukin-1 beta; IL-6, interleukin-6; MCP-1, monocyte chemoattractant protein-1; IL-2, interleukin 2; IL-10, interleukin 10; IL-13, interleukin 13; IFN-γ, interferon gamma.
The 10 Chinese studies from the CNKI search were published between 2012 and 2014, and included a total of 978 participants with AIT. Only one of the abstracts stated that the study was blinded (50), and seven stated that the participants were “randomized” or “randomly divided.” Follow-up periods ranged from 3 to 12 months, and two abstracts did not specify the follow-up time. Eight abstracts reported that the participants were treated with LT4, and two did not (Supplementary Table S1; Supplementary Data are available online at
Immunomodulatory effects
Three of the included trials investigated immunological effects of selenium supplementation beyond autoantibody levels. One trial (17) found no significant differences in the cytokine pattern of helper (CD4+) or cytotoxic (CD8+) T cells following three months of 200 μg of sodium selenite supplementation. Another study (31) found a significant reduction of serum chemokine ligand 9 (CXCL-9) and CXCL-10 in the two groups receiving 80 μg and 160 μg of selenomethionine, respectively, at both 6 and 12 months, and a transient decrease of CXCL-11, tumor necrosis factor alpha (TNF-α), and interferon gamma (INF-γ) at six months in both groups, but a return to nearly the basal level at 12 months. Another study (33) found that LT4 and selenomethionine both have a systemic anti-inflammatory effect but target different cells. LT4 reduced monocyte release of TNF-α, interleukin 1 beta (IL-1β), IL-6 and monocyte chemoattractant protein-1 (MCP-1), while selenomethionine inhibited lymphocyte release of IL-2, INF-γ, and TNF-α. All effects were most prominent by the end of study, after six months of intervention, and seemed to accumulate in a group receiving both interventions. Quality of evidence was assessed as moderate (Tables 2 and 3).
RCTs, randomized controlled trials; CI, confidence interval.
+, low risk of bias; ?, unclear risk of bias; –, high risk of bias.
Meta-analyses
Change in TPOAb levels
In LT4-treated populations (Fig. 2), patients assigned to receive selenium demonstrated significantly lower TPOAb levels after three months (seven studies: WMD = −271 [CI −366 to −175]; p < 0.0001; I 2 = 45.4%), six months (three studies: WMD = −469 [CI −617 to −322]; p < 0.001, I 2 = 52.4%), and 12 months (one study: WMD = −423 [CI −450 to −396]; p < 0.0001). Quality of evidence was assessed as moderate at three and six months, and low at 12 months (Tables 2 and 3). In newly diagnosed populations not yet treated with LT4 (Fig. 3), the selenium group demonstrated significantly lower TPOAb levels after three months (three studies: WMD = −512 [CI −626 to −398]; p < 0.0001; I = 0.0%), but not after 6 or 12 months. Quality of evidence was assessed as moderate at three months, very low at six months and low at 12 months (Tables 2 and 3).
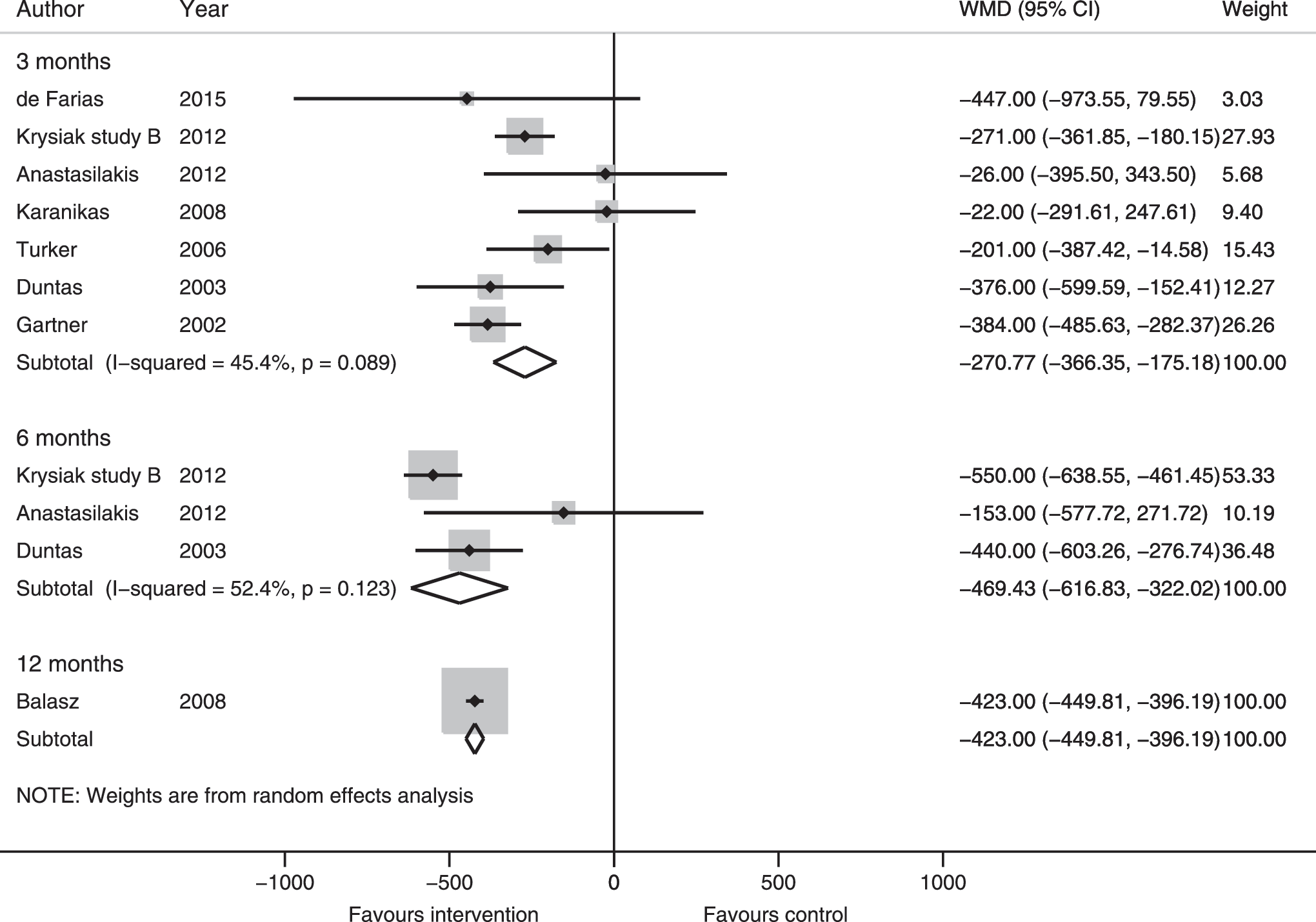
Meta-analysis of the effect of selenium supplementation on serum thyroid peroxidase autoantibody (TPOAb) levels in levothyroxine (LT4)-treated populations of chronic autoimmune thyroiditis (AIT) patients. Weighted mean difference (WMD) in serum TPOAb levels after 3, 6, and 12 months of selenium supplementation or placebo in LT4-treated populations is shown. Boxes represent mean values of the outcomes in a study, horizontal lines the confidence intervals, and the box area is proportional to the weight of the individual study (as seen in “Weight”). Diamonds represent the overall summary estimate, with confidence interval given by its width. I 2 shows the heterogeneity among studies and with p-value.
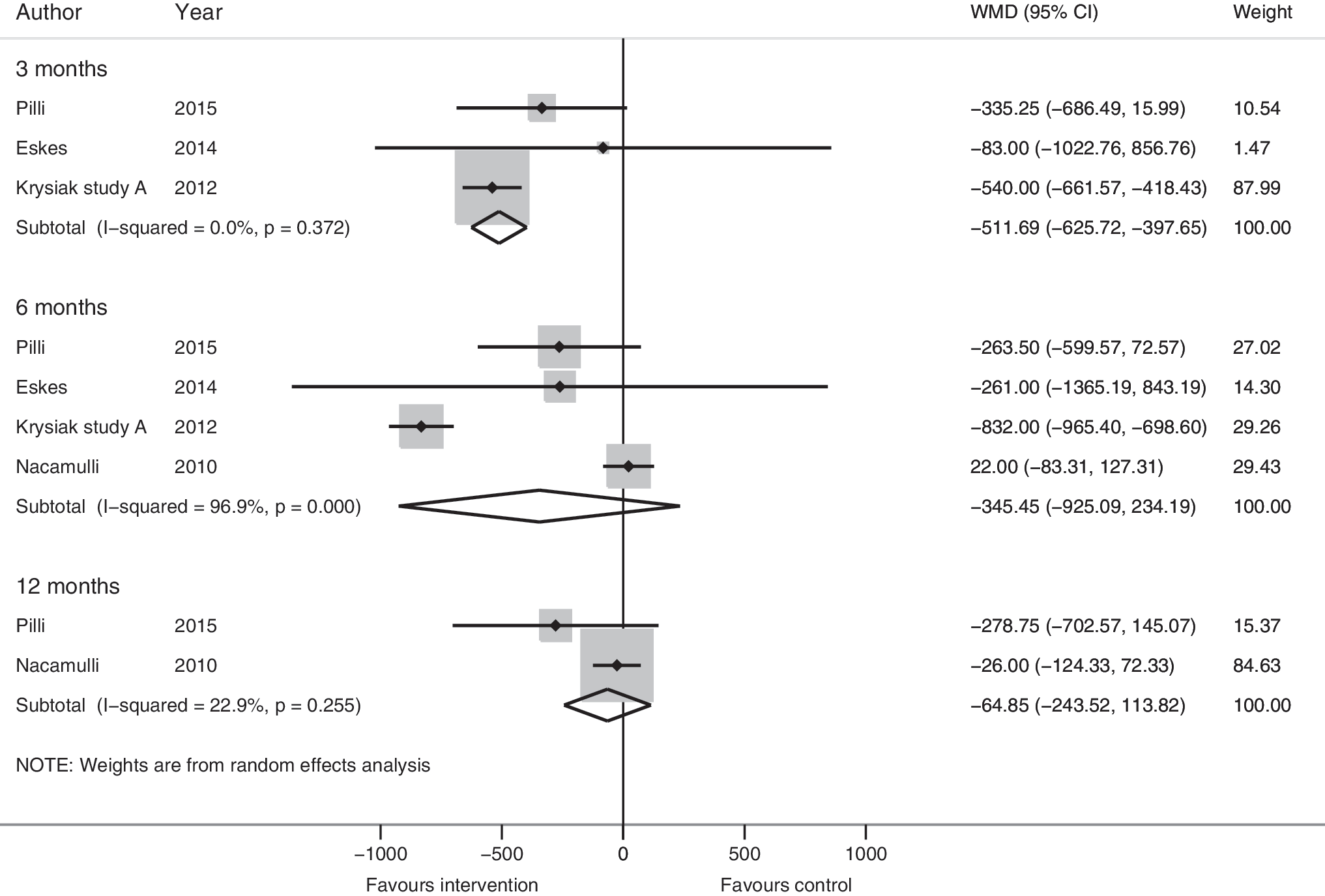
Meta-analysis of the effect of selenium supplementation on serum TPOAb levels in newly diagnosed, not yet LT4-treated populations of chronic AIT patients. WMD in serum TPOAb levels after 3, 6, and 12 months of selenium supplementation or placebo in LT4-untreated populations is shown. For further explanation, see legend for Figure 2.
Change in TgAb levels
In LT4-treated populations, there was a significant decrease in TgAb levels in the selenium-treated group at 12 months (one study: WMD = −176 [CI −199 to −153]; p < 0.0001), but not at three months (six studies: WMD = 26 [CI −251 to 304]; p = 0.85; I 2 = 91.7%) or six months (three studies: WMD = −111 [CI −252 to 30]; p = 0.12; I 2 = 0.0%; Supplementary Fig. S1). Quality of evidence was assessed as very low at three months, and low at 6 and 12 months (Tables 2 and 3). In LT4-untreated populations, the selenium group demonstrated a significant decrease at three months (two studies: WMD = −215 [CI −407 to −24]; p = 0.027; I 2 = 25.5%), but not at six months (three studies: WMD = −164 [CI −425 to 97]; p = 0.218; I 2 = 91.2%) or at 12 months (two studies: WMD = −50 [CI −123 to 22]; p = 0.174; I 2 = 0.0%; Supplementary Fig. S2). Quality of evidence was assessed as moderate at three months, very low at six months, and low at 12 months (Tables 2 and 3).
Meta-regression analyses
No correlation was found between WMD of TPOAb levels at three months and baseline TPOAb (seven studies: p = 0.29; Fig. 4), baseline selenium levels (five studies: p = 0.40, data not shown), age of participants (six studies: p = 0.44, data not shown), or percentage of females in the population (seven studies: p = 0.79, data not shown). In the analysis of percentage of females, four studies included only females, and the remaining three studies included 91%, 86%, and 62% females, respectively. In absolute numbers, the total sample size was 470 participants, and only 44 were males.
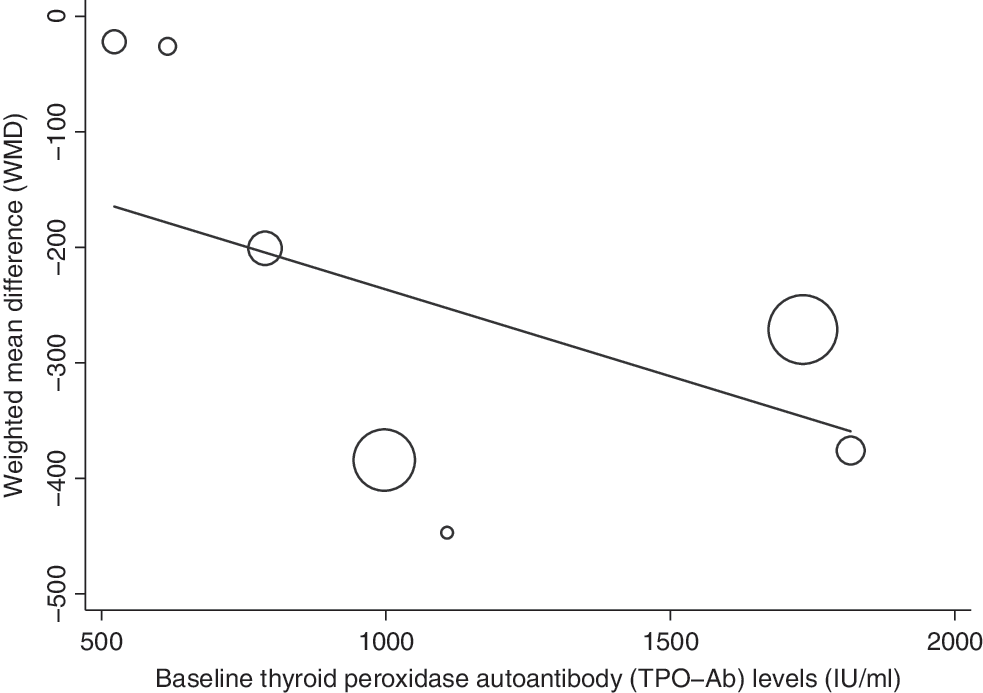
Meta-regression analysis of WMD in serum TPOAb levels after three months of selenium supplementation in LT4-treated populations of chronic AIT patients, correlated by baseline TPOAb level in IU/mL of participants. Circles represent individual studies, and the size of the circles represents the weight of the study in the meta-analysis.
Subgroup analyses of selenium formulations
The seven studies investigating TPOAb at three months in LT4-treated populations found a significant decrease of TPOAb in the group receiving 200 μg of selenomethionine (five studies: WMD = −267.99 [CI −341.97 to −194.01]; p < 0.0001; I 2 = 0.0%), but no significant decrease in TPOAb in the group receiving 200 μg of sodium selenite (two studies: WMD = −225 [CI −577 to 127]; p = 0.21; I 2 = 83.5%, data not shown).
Sensitivity analysis
Meta-analyses, first including and then excluding the study by Pilli et al. (31), were performed for TPOAb and TgAb in LT4-untreated populations. Likewise, meta-analyses of TgAb in LT4-treated populations were performed both including and excluding the studies by Turker et al. (15) and Gärtner et al. (16). None of the results changed following the sensitivity analyses (data not shown).
Relative changes of thyroid autoantibodies
The relative changes in thyroid autoantibodies were analyzed in the largest meta-analysis for LT4-treated patients following three months of selenium supplementation. Across the seven studies, TPOAb decreased 24% (range −48% to −1%) in the selenium groups and 6% (range −31% to +17%) in the control groups. The difference in relative changes between selenium and controls was statistically significant (p = 0.02).
Adverse effects
Analysis of the reported adverse effects in the included studies showed a RR of 4.96 ([CI 1.12–22.21], p = 0.036). Gastric discomfort was the adverse effect most commonly reported (seven patients in the selenium-treated groups). Other adverse effects were headache (selenium group), hair loss (equally in selenium and placebo groups), and skin rash (selenium group). There were no reports of serious adverse effects or signs of acute toxicity or hospitalizations. Quality of evidence was assessed as high.
Quality of evidence assessment
Quality of evidence was assessed per outcome (Tables 2 and 3) using the GRADE guidelines (20 –28). One outcome was not evaluated in a meta-analysis (immunomodulatory effects). Inconsistency was therefore assessed by comparing the findings of the trials. All outcomes were downgraded for indirectness, since they dealt with surrogate markers of clinical efficacy (21). Publication bias could not be assessed by a funnel plot with Egger's test, since none of the meta-analyses contained ≥10 studies (30). Instead, included trials were divided into groups by sample size (>100, 70–100, and <70 participants), and assessed if smaller trials to a larger extent reported positive results than the larger ones did. Using this method, no sign of publication bias was found in this meta-analysis.
Discussion
This systematic review and meta-analyses show that selenium supplementation effectively reduces TPOAb levels at 3, 6, and 12 months and TgAb at 12 months in LT4-treated populations. In populations not receiving thyroid hormone, there was a decrease in TPOAb and TgAb levels after 3 months, but not after 6 or 12 months of supplementation. Two trials in LT4-treated populations (17,32) found no effect of selenium supplementation on TPOAb levels after three months. These had the lowest baseline TPOAb levels (522 IU/mL and 616 IU/mL, respectively). It was hypothesized that the higher the TPOAb levels at baseline, the larger the decrease, but in a meta-regression analysis, a significant correlation could not be demonstrated between the decrease in WMD at three months and the baseline TPOAb levels. Since the studies used different assays for TPOAb, this might influence any potential trend in such a relationship. Further, meta-regression analyses did not demonstrate any significant correlation between baseline selenium status and decrease in TPOAb in LT4-treated patients. Of note, four of the five trials measuring selenium at baseline reported levels in the range of 70–85 μg/L (14,16,17,32), while the fifth was carried out in a population of more marked selenium deficiency, with a baseline serum selenium level of 37 μg/L (51). The decrease in TPOAb did not depend on sex, but the number of male participants was generally low in all included trials, which reflects the female predominance in AIT.
In a subgroup meta-analysis of the decrease in TPOAb in an LT4-treated population, five studies using 200 μg of selenomethionine were compared with two studies using 200 μg of sodium selenite. Results showed a significant drop in TPOAb at three months in the subgroup receiving selenomethionine but not in the one receiving sodium selenite. Absorption of selenite is approximately two-thirds of the absorption of selenomethionine (53), meaning that 200 μg of sodium selenite would correspond to approximately 133 μg of selenomethionine, and this implies that the effects might simply be dose dependent. However, compared with five studies using selenomethionine, only two studies assessed the effect of sodium selenite, and the explanation may therefore lie elsewhere. The trial by Karanikas et al. (17), using 200 μg of sodium selenite, was the first to report no effect on TPOAb. Further, the authors found no effects on T-cell cytokine patterns, sparking debate about the immunological benefit of selenium supplementation in AIT patients. Rather than focusing on formulations, the authors of previous trials noted that the biggest potential might lie in newly diagnosed patients (54,55). Two subsequent trials corroborated this concept, finding reduced lymphocyte release of IFN-γ after six months (31,33) in patients not yet receiving LT4. However, the effect attenuated in one of the trials after 12 months of intervention (31).
The present findings regarding TPOAb in LT4-treated populations are consistent with the meta-analyses of Toulis et al. (13). Further, in a subgroup analysis, Toulis et al. (13) also found a decrease in TPOAb levels following three months of selenomethionine but not sodium selenite. It was not possible to include the studies found in the CNKI search in the meta-analyses due to linguistic obstacles. However, qualitative analysis showed accordance with the present data, suggesting that if the Chinese studies had been incorporated in the meta-analyses, this would most likely not have affected the robustness of the results. However, it may explain the discrepancy between the present results and those obtained by Fan et al. (19), who included several Chinese studies in their study.
The evidence from previous studies has been updated by including new trials, and for the first time, an LT4-treated population has been differentiated from a newly diagnosed population not yet treated, and baseline selenium and antibody status has also been taken into account. Looking at newly diagnosed individuals at risk of developing hypothyroidism, an attempt was made to limit the confounder of disease duration, which was not reported in the majority of the studies. It could be a preconditioning factor for response to selenium supplementation because thyroid autoantibodies typically, but not invariably (56), decrease during LT4 therapy (57,58). Further, this population could be similar to community-dwelling individuals carrying the autoantibodies where the disease has not yet developed. However, it is virtually impossible to establish when a patient becomes positive for TPOAb, since this is a slowly developing process in most individuals, with no or subtle impact on the health, at least in the initial phase. In this meta-analysis, a significant autoantibody decrease was found at 3 months, but not after 6 or 12 months. One possible explanation could be the small sample size, with only four studies in an LT4-untreated population, and a total sample size of only 270 participants.
Because the aim was to include all available trials in the area for a broad critical reappraisal of the evidence, a strict exclusion process of trials depending on how they reported their methodology was not pursued, but rather trials were included that were controlled (placebo or no treatment) and investigated selenium supplementation in different selenium formulations and doses in AIT patients. Then the risk of bias was assessed in each study using the GRADE guidelines, as presented in Table 3, showing that the risk of bias was unclear in studies published before 2010 compared with later studies, perhaps owing to the launch of the 2010 Consolidated Standards of Reporting Trials (CONSORT) statement (59).
A limitation to this study is that the Chinese trials identified in the search in CNKI could not be included. Further, when performing the meta-analyses, one study presented data as medians with IQR (31), which may be unreliable for calculating a mean and a SD for the meta-analysis (30). Two studies (15,16) stratified the randomization according to baseline TPOAb levels, resulting in different baseline TgAb levels in the intervention and control groups. However, sensitivity analyses revealed that the results would not have changed if the studies had been excluded. The Cochrane Handbook of Systematic Reviews recommends that at least 10 studies be included in meta-regression analysis, implying that the present results regarding the relevance of baseline TPOAb and selenium status should be interpreted with caution. Finally, an important limitation to this meta-analysis, being performed in absolute numbers using the WMD, is that the included studies used different assays for measuring thyroid autoantibody levels. Tests that measure antibodies will measure a mixture of different serum molecules, depending on the assay (60). Analyzing the relative changes could limit the significance of this shortcoming, and was done in the largest meta-analysis, for LT4-treated individuals following three months selenium supplementation. As mentioned in the results section, the results were unchanged with this approach, which has other drawbacks, such as loss of statistical power. Therefore, these analyses were only carried out in the largest meta-analysis. The difficulty of standardizing antibody measurements across studies, and lack of information on TPOAb recognition patterns (61), questions whether this outcome can be the basis for clinical decision making.
Summarizing the evidence of this study and previous systematic reviews and meta-analyses, selenium supplementation may decrease TPOAb levels in AIT patients. However, TPOAb is rated as a non-important outcome for patients and decision makers according to GRADE (21). Rather, it is a surrogate marker of disease activity, rendering it suboptimal when investigating the clinical efficacy of selenium supplementation in this patient group. In ongoing trials, such as CATALYST (62), attempts are made to shift the focus to more clinically relevant outcomes. The importance of this is emphasized by recent reports questioning the safety of current upper tolerable intake limits, which may be lower than hitherto recommended (63). On the other hand, there is circumstantial evidence for low selenium status being associated with a number of health issues (10), including a higher risk of developing thyroid disease (12).
In conclusion, the present results do not provide the evidence to warrant routine use of selenium supplementation in the treatment of patients with AIT because a decrease in circulating thyroid autoantibodies per se should not be the foundation of clinical decision making. The emerging use of selenium in AIT (64), without adequate evidence of clinical relevance, should thus be discouraged (65). However, correction of selenium deficiency seems rational in order to avoid negative health effects due to shortage of this important element. Future well-powered randomized controlled trials with long-term follow-up, reporting baseline selenium status and disease stage, will help clarify efficacy.
Footnotes
Acknowledgments
We would like to thank associate professor Carsten Bogh Juhl for extensive help and support in performing the statistical analyses, and Dr. Abdellatif Aharaz for all the work involved in assessment of the quality of evidence together with the first author. Dr. Judit Kolovics is acknowledged for being so kind to translate the article in Hungarian so we could include it in our study, and we wish to thank Dr. Lars Folkestad for expert guidance in connection with the statistical analyses. We are indebted to Dr. Athanasios Anastasilakis for sending us a data sheet of raw data from his clinical trial for analyses, and to Dr. Tania Pilli for supplementary data for inclusion in our analyses, as well as supplementary information for our quality of evidence assessment.
This study was supported by funding from the Agnes and Knut Mørk Foundation, Odense University Hospital, and the Faculty of Health Sciences, University of Southern Denmark.
Author Disclosure Statement
No competing financial interests exist.