
Abstract
Background:
Molecular markers associated with thyroid malignancy are increasingly being used as differential diagnostic tools for thyroid nodules. However, little has been reported recently regarding the prevalence of these markers in benign lesions. The literature was systematically reviewed to examine studies that reported on the prevalence of these markers in benign thyroid lesions.
Methods:
Appropriate studies published between January 1, 2000, and April 30, 2015, and cataloged in PubMed, Embase, Cochrane, Scopus, and Web of Science databases were searched for by combining different keywords for “thyroid tumor” with both general and specific keywords for “molecular marker” by using “AND” as the Boolean operator. All studies meeting criteria that reported the prevalence of RAS mutations, and RET/PTC and PAX8/PPAR-gamma chromosomal rearrangements in benign thyroid lesions were included for study.
Results:
A total of 64 articles (including 8162 patients, of whom 42.5% had benign lesions) that met all the study criteria were systematically reviewed and abstracted. Among 35 studies examining RAS mutations, the reported prevalence of RAS mutation in benign lesions ranged from 0% to 48%. In 38 studies examining RET/PTC rearrangements, the prevalence in benign lesions ranged from 0% to 68%. PAX8/PPAR-gamma rearrangements were examined in 27 studies, with the prevalence in benign lesions ranging from 0% to 55%.
Conclusion:
The presence of these biomarkers and the tremendous variation in reports of their prevalence in benign lesions suggests the need for caution when including these markers in diagnostic decisions. Further understanding of the importance of these markers, as well as newly discovered markers of thyroid malignancy, may be required in order to avoid overtreatment of patients with benign thyroid tumors.
Introduction
T
As a result of recent advances in molecular genetics, measures of several molecular markers have been examined as possible tools to improve the accuracy of preoperative diagnosis of thyroid nodules. The examination of these markers has entered the practice of many physicians caring for patients with thyroid nodules, and an emerging market of molecular markers for thyroid cancer has evolved (1,8 –10). For example, somatic mutations in thyroid tumors include RAS mutations, and RET/PTC and PAX8/PPAR-gamma chromosomal rearrangements (11). Because these molecular markers appear frequently in patients with pathologically confirmed thyroid malignancy, somatic mutation panels have been widely studied as a means to detect malignant thyroid lesions, and their use has been widely implemented as an adjunct to FNA cytological diagnosis (12). Importantly, most studies examining relationships between these markers and malignancy in thyroid tumors have focused on examining the prevalence of these markers in malignant lesions, and have not examined the prevalence of these markers in benign lesions with the same intensity. However, numerous studies have reported that these same genetic mutations can also be found in benign lesions.
For example, Guerra et al. found RET/PTC rearrangements in 36% of malignant thyroid lesions compared with 13.3% of benign lesions, and concluded that this high prevalence in benign nodules must be taken into account to avoid false-positive diagnoses (13). Similarly, a high prevalence of RET/PTC rearrangements was reported by Elisei et al. (14). Rhoden et al. also found this mutation in up to 68% of patients with Hashimoto's thyroiditis (15). Cheung et al. found an even higher prevalence of PAX-8/PPAR-gamma translocations in follicular adenomas (FA) compared with follicular thyroid carcinomas (FTC; 55% vs. 35%) (16). Castro et al. also found RAS mutations in 26% of FAs in their study (17).
The substantial prevalence of the above markers in benign disease raises concerns about the ultimate value of using these biomarkers for treatment decisions. Because of these concerns and the implications of basing treatment on potentially inaccurate markers of benign versus malignant thyroid tumors, a systematic review was performed to examine and summarize the scientific literature regarding the prevalence of RAS mutation, and RET/PTC and PAX8/PPAR-gamma chromosomal rearrangements in benign thyroid lesions.
Material and Methods
The systematic review was designed based on the Cochrane Handbook for Interventional Systematic Reviews (18), and was written according to the guidelines proposed by the Preferred Reporting Items for Systematic review and Meta-analyses (PRISMA) statement (19). With the assistance of an expert librarian and informationist, appropriate studies published between January 1, 2000, and April 30, 2015, on PubMed, Embase, Cochrane, Scopus, and Web of Science databases were searched for by combining different keywords for “thyroid tumor” with both general and specific keywords for “molecular marker” by using “AND” as the Boolean operator (see Supplementary Data for details of search terms; Supplementary Data are available online at
After removing duplicates using Mendeley reference manager software, 5278 studies were imported into a FileMaker Pro v13 database. Each title and abstract was reviewed and screened twice by five independent reviewers (A.N., S.N., F.A., C.A., and G.T.). Studies on tissues other than the thyroid, those that did not examine any of the molecular markers of interest, those that studied only malignant lesions, those that did not have final diagnoses based on histopathology, that that included only animal studies, studies on cell lines, non-original articles (review articles, case reports, conference abstracts and letters to editors), and non-English articles were excluded.
Citations of relevant articles were also assessed to identify any additional eligible studies. During the entire selection process, studies with discrepancies or uncertainty were marked in the database and were discussed with the other reviewers to reach a final decision on whether these should be included. Upon identification of the final group of eligible studies, full-text publications were reviewed, and data on study population, number of cases with benign thyroid lesions, prevalence of each of the molecular markers (RAS mutation, and RET/PTC and PAX8/PPAR-gamma chromosomal rearrangements) and theirs subtypes (H-RAS, K-RAS, and N-RAS; RET/PTC-1, RET/PTC-2, and RET/PTC-3), and study criteria were extracted.
Results
The flow of the study search is described in Figure 1. Using a broad search with multiple databases, 10,592 articles were identified. After removal of 5315 duplicates, 5277 articles were screened by title and abstract. After exclusion of 4970 studies that did not meet the study criteria based upon a review of the abstract, the remaining 307 full-text articles were reviewed, and finally, after eliminating an additional 243 articles that did not fulfill the study requirements, a total of 64 articles that met all the study criteria were systematically reviewed and abstracted. A summary of the final 64 studies is listed in Table 1 (1,13 –17,20 –77). These studies include a total of 8162 patients with a median of 88 (interquartile range [IQR] 56–139) patients, of whom 3474 (42.5%) had benign lesions. The median number of patients with benign pathology was 30 (IQR 16–53). The earliest and latest studies that were reviewed were published in 2000 (23,42,64) and 2015 (56,76), respectively. The largest single study population was 513 patients, and the largest number of patients with benign lesions in a single study was 392 (38). Three studies included ≤20 fewer total cases (29,63,76), and 10 studies had <10 patients with benign lesions (23,29,32,42,54,63,66,68,70,76). Four studies included patients with a history of radiation exposure (14,21,30,37).
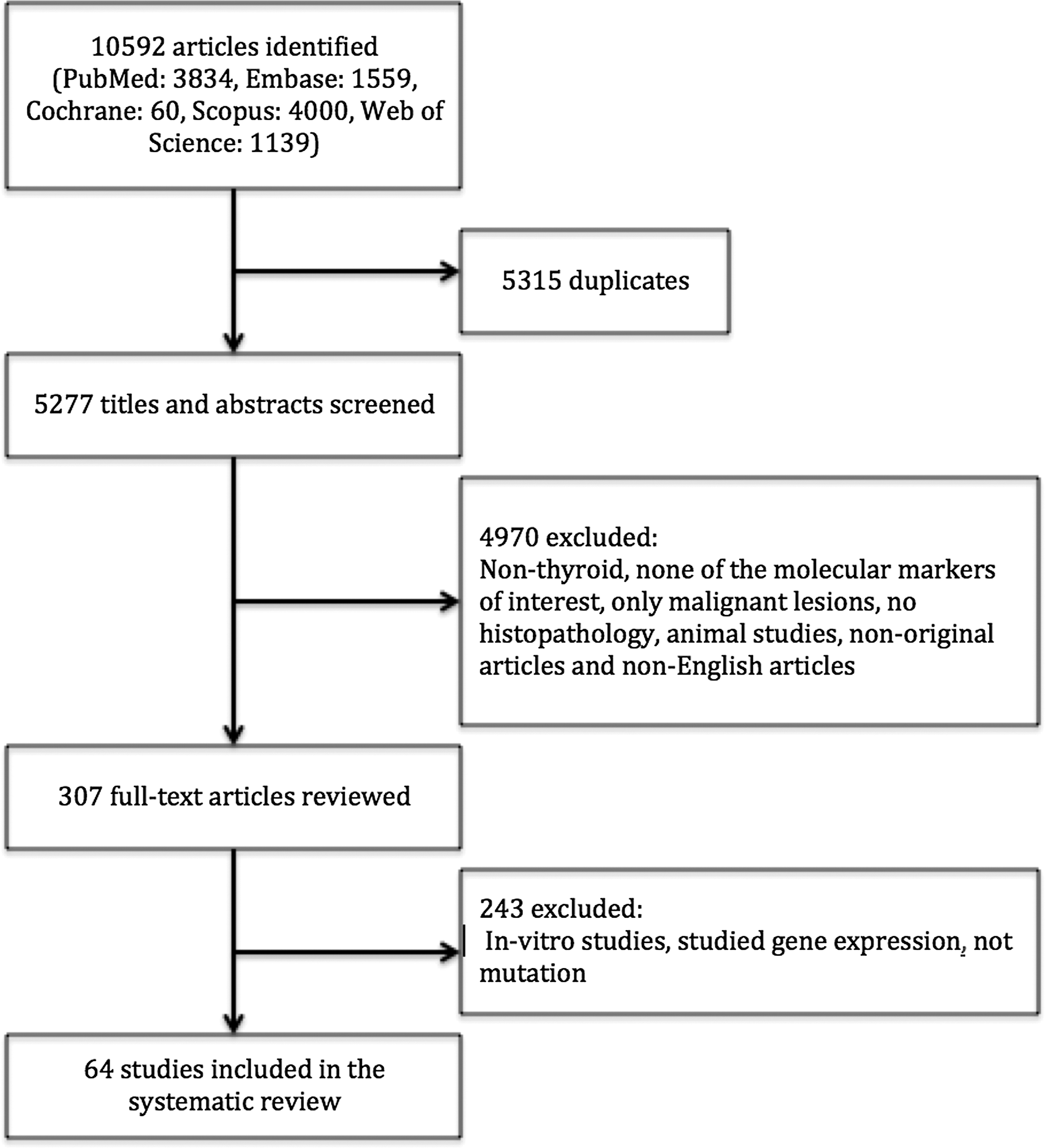
Study flow chart: algorithm for identification of eligible studies with inclusion and exclusion criteria.
N and n represent the number of samples for which both final diagnosis and mutation analysis were available.
Only included BRAF-negative samples. Of the total of 155 cases, histology was available for 19 cases.
Initially included 232 benign cases, but PCR failed in 39 cases.
Studied children and adolescents with hot nodules.
Initially included 42 benign lesions, but RAS mutation was checked only in 34 cases.
N, total number; n, number of benign cases; Pyroseq, pyrosequencing; qPCR, quantitative PCR; HRM, high-resolution melting; PCR, polymerase chain reaction; RT-PCR, reverse transcription PCR; FISH, fluorescence in situ hybridization; IHC, immunohistochemistry; LC-PCR, LightCycler® RT-PCR; FMCA, fluorometric microculture cytotoxicity assay.
RAS mutations
Thirty-five (55%) studies investigated RAS mutation in 2574 benign lesions (1,17,20 24,27,29,31 –35,38,42 –45,48,50,51,54 56 –59,63,66 –69,72,74 –76). The prevalence of RAS mutation in benign thyroid lesions ranged from a low of 0% to a high of 48%. There was substantial variability in the proportion of patients with RAS mutation across studies: nine studies found RAS mutations in >20% of benign lesions (25–48%; Table 2) (20,32,35,42,48,50,52,67,68); and 21 studies detected RAS mutations in 1–20% of the benign lesions (1,17,20,24,27,31,33,38,43 –45,51,54,56 –59,69,72,74,75). However, five studies on a total of 56 benign lesions did not find any mutations in benign thyroid lesions (29,34,49,63,66).
n, number of benign lesions in each study; N, total number of cases in each study.
RET/PTC rearrangements
RET/PTC rearrangements were examined in 38 (59%) studies including 2239 benign thyroid lesions (1,13 –15,21 –23,25 –27,29 –31,33,34,36,39 –41,43,44,49,51,55 –57,59,60,62 –66,68,69,71 –73). The prevalence of RET/PTC rearrangements in benign thyroid lesions ranged from 0% to 68%. Three of these studies included patients who had been exposed to radiation (14,21,30). Six studies detected RET/PTC rearrangements in >20% of the lesions (14,15,22,30,63,65) (Table 3); eight studies found RET/PTC rearrangements in ≤20% of the benign lesions (13,21,41,51,55,62,64,73); 24 studies on 1708 benign lesions did not find any RET/PTC rearrangements (1,23,25 –27,29,31,33,34,36,39,40,43,44,49,56,57,59,60,66,68,69,71,72).
These studies included patients with radiation exposure.
n, number of benign lesions in each study; N, total number of cases in each study.
PAX8/PPAR-gamma rearrangements
PAX8/PPAR-gamma rearrangements were studied in 27 (42%) articles with 1874 benign lesions (1,16,28,31,33 –35,37,46,47,51,53 –59,61,63,66,67,69,70,72,74,77). The prevalence of PAX8/PPAR-gamma rearrangements in benign thyroid lesions ranged from 0% to 55%. One study included patients with radiation exposure (37). The highest prevalence of PAX8/PPAR-gamma rearrangements in benign lesions was observed in two other studies: Castro et al. (67) studied 12 benign lesions and detected PAX8/PPAR-gamma rearrangements in 25% of benign lesions. Cheung et al. (16) examined a total 11 benign lesion and found PAX8/PPAR-gamma rearrangements in six (55%) benign lesions. Thirteen studies found PAX8/PPAR-gamma rearrangements in up to 15% of the benign lesions (2–15%) (28,35,37,46,47,51,54,55,59,61,72,74,77). However, no PAX8/PPAR-gamma rearrangements were found in 1073 benign lesions of 12 studies (1,31,33,34,53,56 –58,63,66,69,70).
Discussion
This study systematically reviewed studies reporting the prevalence of RAS mutations, and RET/PTC and PAX8/PPAR-gamma chromosomal rearrangements in benign thyroid lesions. While associations between the markers of interest and malignancy form the bulk of reporting on potential prognostic biomarkers to aid decision making in the treatment of thyroid tumors, this systematic review found that these markers are quite prevalent in benign thyroid nodules, with up to 48% of them harboring RAS mutations, up to 68% RET/PTC rearrangements, and up to 55% PAX/PPAR-gamma rearrangements.
RAS mutations are known to be the second most common genetic alteration in thyroid malignancy (78), but despite their high prevalence in FTC and follicular variant of papillary thyroid carcinoma (FVPTC), their role in the clinical behavior of thyroid tumors remains unclear (42,78). RAS mutations are also common in benign follicular lesions, including FA, which is the most common thyroid tumor reported in final pathology when a FNA sample is classified in the indeterminate cytology category (79).
According to this systematic review, only 5/35 (14%) studies examining RAS mutations did not find any of these mutations in benign lesions. Furthermore, 9/35 (26%) studies found RAS mutations in >20–50% of benign thyroid lesions (20,32,35,42,48,50,52,67,68). On the other hand, the prevalence of RAS mutations in malignant lesions in these 35 studies ranged from 10% to 93%. Although the prevalence of RAS mutations was significantly higher in malignant lesions in most studies, relying upon the presence of RAS mutation to drive the clinical decision process toward surgery for an indeterminate thyroid nodule without any other obvious indication for surgical intervention might result in overtreatment of a RAS-positive FA that otherwise could have been safely followed. Recent studies suggest that benign thyroid nodules harboring RAS mutations have excellent prognosis with conservative treatment in the long term (80). In addition, a recent study by Medici et al. demonstrated that the majority of RAS-positive malignant thyroid lesions have a low-risk phenotype, and also reported that cytologically benign lesions with a positive RAS mutation tend to have an indolent course. Therefore, they concluded that the presence of a RAS mutation should not affect the clinical decision-making process (81).
More than half (55.6%) of studies examining PAX8/PPAR-gamma rearrangements in this systematic review found this translocation in benign thyroid lesions, including two studies that found this mutation in up to half of the begin lesions studied (16,67). Although originally believed to occur only in malignant thyroid lesions, PAX8/PPAR-gamma rearrangements are frequently detected in benign thyroid lesions, clearly indicating that PAX8/PPAR-gamma rearrangements are not restricted to malignant thyroid lesions only (61). Therefore, the value of this marker as a test to differentiate benign from malignant thyroid lesions is unclear.
The other commonly studied molecular markers in thyroid malignancies are RET/PTC rearrangements, which appear to be more common in PTCs. However, these rearrangements were also reported in benign thyroid lesions and can be associated with radiation exposure (82 –84). This systematic review revealed that although RET/PTC rearrangements were absent in the benign lesions in 24/38 (63.2%) studies, between 26% and 68% of benign lesions were positive for RET/PTC rearrangements in the remaining six studies (14,15,22,30,63,65). Although the expectation was to see higher prevalence of RET/PTC rearrangements in patients with a history of radiation, the prevalence of RET/PTC rearrangements in benign lesions with radiation exposure was <26% (14) and 46% (30) compared with 33–68% in those without a history of radiation (15,22,63,65). This might be attributed to the differences in demographics of the study population or study design.
In addition to the high prevalence of these markers in benign thyroid lesions, there is new nomenclature for encapsulated FVPTC, now considered as non-invasive neoplasms (non-invasive follicular thyroid neoplasms with papillary-like nuclear features) with a very low risk of adverse outcome (85). This further challenges the literature with regard to these molecular markers, with some of the past tumors catalogued as malignant now considered benign.
In addition, the recent The Cancer Genome Atlas has identified even more markers of thyroid malignancy (86). Given the present findings, their prevalence rates in benign thyroid lesions also to be examined in the future.
There are several important factors that might bias the findings of studies on molecular markers in thyroid lesions, and results of these studies should be interpreted in the context of these limitations. First, the relatively small number of benign lesions examined in these studies might have limited power to detect the actual prevalence of these markers in benign lesions. Since the majority of studies assume that these markers are associated with thyroid malignancy, the studies generally focus on malignant thyroid lesions and do not examine benign lesions or just examine a small number of benign lesions as controls. The median number of benign lesions in studies that were included in this systematic review was 28 (IQR 16–53), whereas the median number of total lesions was 88 (IQR 56–139). Another possible reason for the small number of benign lesions examined in these studies is that the majority of patients with thyroid lesions found to be benign on FNA opt to follow up, and therefore these lesions are much less likely to be resected and cannot be included in molecular marker studies. The majority of benign lesions that are examined in such studies represent those with indeterminate or suspicious cytology that were ultimately found to be benign on histopathology.
Another important limiting factor involves differences in the methods used to detect genetic alterations by different studies. For instance, real-time polymerase chain reaction is known to be more sensitive than pyrosequencing (32). Therefore, some studies that rely primarily on pyrosequencing may lack sufficient sensitivity at the molecular level to detect mutations, which could bias estimates of the prevalence of these markers in thyroid lesions (Table 4).
Also, geographical factors and variability in radiation exposure might be associated with these mutations and account for some proportion of the wide range in the prevalence of these markers across different studies (87). Further limitations of this systematic review are driven by variability in measuring and reporting of variability in predictor and outcome variables across studies and time, and it is possible that our screening methods for the review might have led to some additional studies that might have provided some relevant information being missed or excluded. A final limitation of this study is that because of the nature of a systematic review, data are not captured at the level of the individual across studies, and no population-level estimates can be calculated.
In conclusion, it is clear that molecular markers found in some proportion of malignant thyroid tumors are also found in some proportion of benign thyroid tumors. Substantial further work is required to understand the relationships between the prevalence of these markers, their impact on thyroid tumors, and their actual clinical application. Assigning too much weight to the presence of these markers that are prevalent in both malignant and benign thyroid lesions may mislead the decision-making process and might lead to resection of benign thyroid tumors, and the risks associated with surgical intervention, in patients who would have had excellent results with conservative management.
Footnotes
Acknowledgments
We are grateful to Stella Seal for her expert assistance in searching the databases, and to Sruthi Murali for her help with the abstract screening process.
Author Disclosure Statement
All authors have nothing to disclose.