
Abstract
Background:
Hypothyroidism is referred to be a rare but possible cause of hyponatremia. However, there is only poor evidence supporting this association. Since hyponatremia and hypothyroidism are both common conditions themselves, co-occurrence does not have to be causal.
Methods:
To address a potential relationship, a retrospective analysis of data from the Division of Endocrinology of the Medical University of Vienna from April 2004 to February 2016 was performed. A total of 8053 hypothyroid patients (48 ± 18 years of age; 71% female) with thyrotropin >4.0 μIU/mL and available blood tests for free thyroxine and sodium (Na+) within maximal ± seven days were included and screened for hyponatremia. Patients' records were searched for concomitant disease and medication when Na+ concentration was <135 mmol/L.
Results:
Hyponatremia was present in 448/8053 (5.56%) patients. Analysis of medical history revealed potential alternative causes of hyponatremia in 442/448 (98.88%) patients (i.e., side effects of medication, concomitant underlying disease, or other endocrine disorders). This distribution did not differ between patients suffering from clinical or subclinical hypothyroidism. No case of clinically relevant hyponatremia (Na+ < 130 mmol/L), present in 111/448 (24.78%) patients could be attributed only to hypothyroidism. There was a very weak but statistically significant trend toward a positive association between thyroid function and serum Na+ levels (Na+/thyrotropin: R = 0.022, p = 0.046; Na+/free thyroxine: R = −0.047, p < 0.001).
Conclusion:
The results suggest that hypothyroid patients with moderate to severe hyponatremia often have other potential explanations for their low serum Na+ concentrations in routine care.
Introduction
R
In contrast to these data from exploratory experiments, cohort studies in real-life settings have failed to show an impact of hypothyroidism on serum sodium (Na+) concentration. Since hyponatremia and hypothyroidism are both common conditions in routine care, they are often observed to occur together in a single patient. In a cross-sectional analysis, there was no difference in distribution of Na+ concentrations in hypothyroid subjects compared to controls (6). Moreover, the proportion of patients with a serum Na+ concentration below the reference range was comparable between euthyroid and hypothyroid subjects (7,8).
However, the individual cause of decreased Na+ concentrations in hypothyroid patients has not yet been investigated. The question remains as to whether co-occurrence of hyponatremia and hypothyroidism is because of causality or coincidence.
Methods
To address this question, a retrospective, single center, cohort study was performed. Data of hypothyroid patients, defined by thyrotropin (TSH) >4 μIU/mL with an available serum Na+ concentration within maximal ± seven days of TSH measurement, treated at the Division of Endocrinology and Metabolism, Department of Internal Medicine III, Medical University of Vienna from April 2004 to February 2016 were used for analysis. If available, results of free thyroxine (fT4) concentration within maximal ± seven days of TSH measurement were also included. In patients suffering from hyponatremia (serum Na+ <135 mmol/L), patients' records were searched for possible other causes for decreased Na+ concentrations instead of hypothyroidism.
Potential differential diagnoses of hyponatremia were assigned into four different groups for a well-structured overview: group 1—other endocrine disorders: Addison crisis, syndrome of inappropriate antidiuretic hormone secretion (SIADH), blood glucose excursions in insufficiently controlled type 1 or 2 diabetes mellitus; group 2—disturbed volume status (hypo- and hypervolemia): advanced chronic kidney failure, advanced heart failure, decompensated liver cirrhosis, diarrhea, vomiting; group 3—drug side effects: drugs with hyponatremia listed in their adverse events profile; group 4—pregnancy.
Potential differential diagnoses were compiled from patients' charts when patients were treated only in an outpatients setting or from the medical discharge report when patients were hospitalized. Since there is no structured data assessment of comorbidities in the outpatient clinic, it was not possible to validate diagnoses in medical documents with other examinations or laboratory values in most of the patients.
Since all patients included in this study suffered from hypothyroidism, diagnosis of SIADH was provisional, since thyroid function was not used as one of the diagnostic criteria. Drug side effects were classified for prescribed medication only. Follow-up data of patients omitting medication potentially being the cause of hyponatremia was incomplete, and could not be used for confirmation of the diagnosis. Only one patient suffering from hyponatremia in the cohort was hospitalized because of hypothyroidism and showed laboratory findings consistent with polyglandular autoimmune syndrome, including adrenal insufficiency, in the further work-up. Hyponatremia was classified as mild (Na+ >130 and <135 mmol/L), moderate (Na+ >120 and ≤130 mmol/L), and severe (Na+ ≤120 mmol/L). The local ethics committee of the Medical University of Vienna, Vienna, Austria, approved the conduct of this study.
Exploratory statistical analysis was performed using IBM SPSS Statistics for Windows v24 (IBM Corp., Armonk, NY). Data are given as means ± standard deviation. Comparison between groups was performed by unpaired Student's t-test. For correlation analysis, Pearson's correlation coefficient was used. Level of statistical significance was set at p < 0.05.
Results
In total, 8053 patients were included in this study for analysis (M age = 48 ± 18 years; 71% female). Hyponatremia was present in 448/8053 (5.56%) patients, and 111/448 (24.78%) patients suffered from moderate to severe hyponatremia.
In all but 6/448 (98.88%) patients a possible alternative cause for decreased serum Na+ concentrations could be found. All six patients suffered only from mild hyponatremia. All patients with moderate to severe hyponatremia could be assigned to one or more other underlying causes for electrolyte disturbances. Additionally, no difference in the cause of hyponatremia between patients suffering from latent and manifest hypothyroidism could be observed (see Table 1).
All hypothyroid patients diagnosed with hyponatremia were assigned to groups of potentially causal differential diagnosis for hyponatremia based on their medical history. (i) Endocrine: other underlying endocrine disorders such as Addison crisis, syndrome of inappropriate antidiuretic hormone secretion, blood glucose excursions in insufficiently controlled type 1 or 2 diabetes mellitus. (ii) Volume status: hypo- and hypervolemia: advanced chronic kidney failure, advanced heart failure, decompensated liver cirrhosis, diarrhea, vomiting. (iii) Drug side effects. (iv) Pregnancy. (v) Combined: more than one possible differential diagnosis. (vi) None: only hypothyroidism.
When patients with a TSH ≥20 μIU/mL were investigated separately, 43/764 (5.62%) patients had hyponatremia. No potential alternative causes of hyponatremia could be identified in only three (0.39%) of these patients. In these patients, serum Na+ concentrations were 134 mmol/L or 133 mmol/L, respectively. Additionally, when only patients with a TSH ≥100 μIU/mL were investigated, 2/138 patients had decreased Na+ concentrations (i.e. 134 mmol/L and 132 mmol/L), and a potential alternative diagnosis for hyponatremia could be identified for both of them.
In two patients with a TSH ≥20 μIU/mL, no other cause but furosemide could be found as an explanation for hyponatremia. One patient was 81 years of age, had a serum Na+ of 121 mmol/L, and was hospitalized for dizziness. In this patient, serum Na+ immediately recovered after fluid replacement and cessation of furosemide, independently of changes in thyroid function. The other patient had only a slightly decreased Na+ level of 134 mmol/L.
A detailed list of all differential diagnoses in patients suffering from hyponatremia is given in the Supplementary Data (Supplementary Data are available online at
Interestingly, in correlation analysis, there was a very mild but significantly positive relation between serum Na+ levels and concentrations of TSH (R = 0.022; p = 0.046) and a significant negative impact of serum Na+ levels on concentrations of fT4 (R = −0.047; p < 0.001) in the whole cohort. No difference could be found between patients suffering from mild or severe hypothyroidism (see Fig. 1). The relationship between Na+, fT4, and TSH levels was present in all patients with hyponatremia (R = −0.227; p < 0.001), as well as in patients suffering from moderate to severe hyponatremia (R = −0.121; p < 0.001).
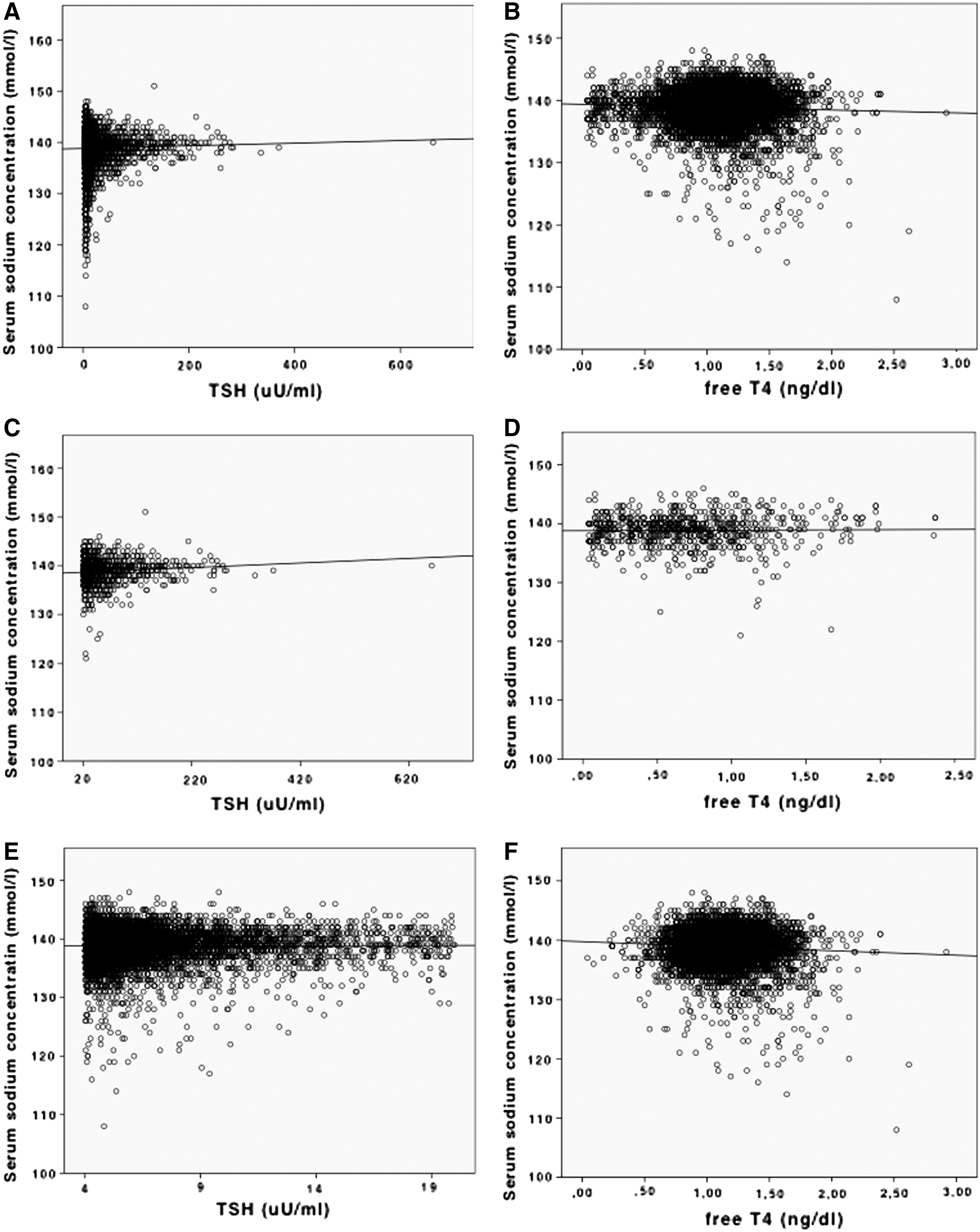
Correlation analysis of thyroid function and serum sodium (Na+) concentration. In all patients included for analysis, there was a significantly positive association between thyrotropin (TSH) and Na+ (R = 0.022; p = 0.046) (
Moreover, in patients with hyponatremia, the TSH concentration was significantly lower (10.57 vs. 12.46 μIU/mL; p = 0.011) and fT4 concentration was significantly higher (1.09 vs. 1.20 ng/dL; p < 0.001) compared with patients with normonatremia.
Discussion
The data clearly demonstrate that co-occurrence of hyponatremia and hypothyroidism in routine care is not likely to be causal and that there are more common causes of hyponatremia in hypothyroid patients diagnosed with hyponatremia than impaired thyroid function. Especially in patients with clinically relevant electrolyte disturbances and serum Na+ levels <130 mmol/L, no case of hyponatremia could be only assigned to impaired thyroid function.
Hyponatremia is the most common electrolyte disorder in patients hospitalized for acute or chronic illnesses, with an estimated prevalence of 4–35%, and it is therefore frequently observed in clinical practice. It is clearly associated with increased mortality and adverse prognostic outcomes (9,10).
The etiology of hyponatremia is diverse (11,12). In the present cohort, drug side effects were the most common cause of hyponatremia, which is in line with previous reports (13). Increased extracellular volume in heart failure, nephrotic syndrome, or liver cirrhosis, as well as decreased extracellular volume due to diarrhea and vomiting and endocrine diseases such as adrenal crisis and SIADH, are common causes of hyponatremia (1,2). In addition, in pregnancy, a decrease in serum osmolality and mild hyponatremia is observed in the second and third trimesters (14). Due to these various reasons, a clear assignment to one specific cause of electrolyte disturbances can be difficult in clinical practice.
In particular, severe forms of hypothyroidism have been reported to be associated with a decrease in serum Na+ concentration (15,16). This has been explained by a decrease in renal function and impaired cardiac output due to lower heart rate and reduced stroke volume, which are reversible by thyroid hormone substitution therapy (17). However, despite reports of selective cases of critically ill patients in myxedema coma (15), prospective studies failed to show an impact of thyroid function on the prevalence of hyponatremia, even in severely hypothyroid patients with TSH concentrations from 140 to 192 μIU/mL (18,19).
In this study, the prevalence of hyponatremia in the whole group of patients with subclinical and clinical hypothyroidism was only 5.58%, which is lower than the commonly reported prevalence in the literature in the general population (1). This might be explained by the selected cohort of patients, the majority of whom were treated in an outpatient setting and did not suffer from acute illness. Furthermore, the proportion of patients diagnosed with an endocrine disorder known to decrease serum Na+ concentrations was high in this population, which is explained by the study design, since all data stem from a department specialized in endocrinology.
Interestingly, a very weak but significant positive association between levels of TSH and serum Na+ and also a very weak but significant negative association between levels of fT4 and serum Na+ could be observed independently of the severity of hyponatremia. Of note, these trends were independent of the severity of hypothyroidism, since no difference was observed between patients with a TSH ≥20 μIU/mL and a TSH <20 μIU/mL (see Fig. 1). This unexpected finding stands in sharp contrast to the assumed relationship between hypothyroidism and hyponatremia. While statistically significant, these week associations are clearly of no clinical relevance.
The major limitation of this study is the retrospective design, with its well-known disadvantages. Since there was no well-structured data assessment of comorbidities in most of the patients, alternative diagnoses of hyponatremia were assigned from patients' records and prescribed medication but could not be validated by other laboratory values.
The results highlight the importance of careful examination of medical history, comorbidities, and drug history in every patient suffering from hypothyroidism and hyponatremia. Although impaired thyroid function alone can occasionally cause very mild hyponatremia, hypothyroid patients with hyponatremia may have other potential explanations for their low serum Na+ concentrations, and these patients should be evaluated carefully to identify the underlying etiology.
Footnotes
Acknowledgments
This study was in part funded by an unrestricted science grant of the Austrian Association of Endocrinology and Metabolism (ÖGES) to P.W.
Author Disclosure Statement
The authors have nothing to declare.