
Abstract
Background:
Previous research has suggested an increased risk of death and cardiovascular disease in patients treated for hyperthyroidism. However, studies on this subject are heterogeneous, often based on old data, or have not considered the impact that treatment for hyperthyroidism might have on cardiovascular risk. It is also unclear whether long-term prognosis differs between Graves' disease and toxic nodular goiter. The aim of this study was to use a very large cohort built on recent data to assess whether improvements in cardiovascular care might have changed the prognosis over time. The study also investigated the impact of different etiologies of hyperthyroidism.
Methods:
This was an observational register study for the period 1976–2012, with subjects followed for a median period of 18.4 years. Study patients were Stockholm residents treated for Graves' disease or toxic nodular goiter with either radioactive iodine or surgery (N = 12,239). This group was compared to Stockholm residents treated for nontoxic goiter (N = 3685), with adjustments made for age, sex, comorbidities, and time of treatment. Comparisons were also made to the general population of Stockholm. Outcomes were assessed in terms of all-cause and cardiovascular mortality as well as cardiovascular morbidity.
Results:
The hazard ratios (HR) for all-cause mortality and for cardiovascular mortality were 1.27 [confidence interval (CI) 1.20–1.35] and 1.29 [CI 1.17–1.42], respectively, for hyperthyroid patients compared to those with nontoxic goiter. For cardiovascular morbidity, the HR was 1.12 [CI 1.06–1.18]. Patients aged ≥45 years who were treated for toxic nodular goiter were generally at greater risk than others, and those included from the year 1990 and onwards were at greater risk than those included earlier. Increased all-cause mortality, as well as cardiovascular mortality and morbidity, were also seen in comparisons with the general population.
Conclusions:
This is the first large study to indicate that the long-term risk of death and cardiovascular disease in hyperthyroid subjects is due to the hyperthyroidism itself and not an effect of confounding introduced by its treatment. Much of the excess risk is confined to individuals treated for toxic nodular goiter. Despite advances in cardiovascular care during recent decades, hyperthyroidism is still a diagnosis associated with increased cardiovascular morbidity and mortality.
Introduction
I
Most previous research has compared hyperthyroid subjects to the general population or to randomly selected age- and sex-matched controls, with little or no possibility of separating the effects of hyperthyroidism from the effects of its treatment. Only one very recent study, on patients treated with radioiodine, attempted to separate the impact of treatment per se, reporting that radioiodine might be associated with a higher risk of cerebrovascular disease (9). To the authors' knowledge, no studies have used thyroidectomized individuals as a reference group.
Furthermore, it is unknown whether the etiology of hyperthyroidism matters. Several studies have shown differences in long-term risk between individuals with Graves' disease and toxic nodular goiter, but their results have not been coherent (5,6,10 –14). There is a substantial gap in mean age between these two diagnoses, which complicates any comparisons.
Over the last three decades, the spectrum of cardiovascular disease has changed in the Western world. For instance, the awareness of atrial fibrillation has increased, and the importance of stroke prevention in this arrhythmia has gained broad recognition (15). Meanwhile, the incidence of ischemic heart disease has been reduced by more than half (16). It is possible that these trends have also affected cardiovascular risk in hyperthyroid subjects.
The present study aimed to investigate whether there is an association between hyperthyroidism and cardiovascular disease in a large and well-characterized cohort. It also explored the impact of the etiology of hyperthyroidism (Graves' disease and toxic nodular goiter) while avoiding confounding due to age differences. The aim was to address this issue in a manner that has, to the best of the authors' knowledge, not been previously attempted, using not only the general population as a reference group, but also patients who had received thyroid surgery for a reason other than hyperthyroidism. In a study from 2005, Franklyn et al. showed that patients who received radioiodine for Graves' disease returned to a “normal” cardiovascular risk if they required levothyroxine substitution after treatment (2). Because many patients with nontoxic goiter may be expected to become hypothyroid after thyroidectomy, they might make more suitable control subjects than the general population.
Materials and Methods
In Sweden, all hospitalizations are registered in the Swedish National Patient Register, which was established in 1964 and reached full coverage in 1987. It is comprised of codes according to the International Classification of Diseases (ICD) for primary and contributing diagnoses, and procedure codes that are given at hospital discharge. There is also a Cause of Death Register where underlying and contributing causes of death are stated. Additionally, the Swedish Board of Health and Welfare supplies open-access, cause-specific morbidity and mortality data for the entire population dating back to 1998. Information on vital status and migration are available from Statistics Sweden, a government agency. Since July 2005, a national prescription register also exists, where data on all dispensed prescription drugs are collected. For some diagnoses and outpatient treatment modalities, more detailed regional registers exist that stretch even further back in time. One of these is the Stockholm Iodine Cohort, which, among other things, includes data on all radioiodine treatments that were given in the greater Stockholm area between 1976 and 2000. This material has been used and described previously (1,17).
Study patients
The Patient Register and the Stockholm Iodine Cohort were used to gather data on all Stockholm residents who had been treated for hyperthyroidism with either radioiodine or thyroidectomy between 1976 and 2000 (data on patients treated with antithyroid drugs were not obtained, since this information was only recently added to the national registers). These subjects were defined as an exposed population. In order to obtain a reference group, information was also collected from the Patient Register on people that had received surgery for nontoxic goiter. Because these individuals had no hyperthyroidism, they were defined as an unexposed population. A similar procedure has been described previously, and it is displayed in Figure 1 (18). Individuals <18 or >90 years of age at the index event were excluded. Linkage with data from Statistics Sweden was also done.
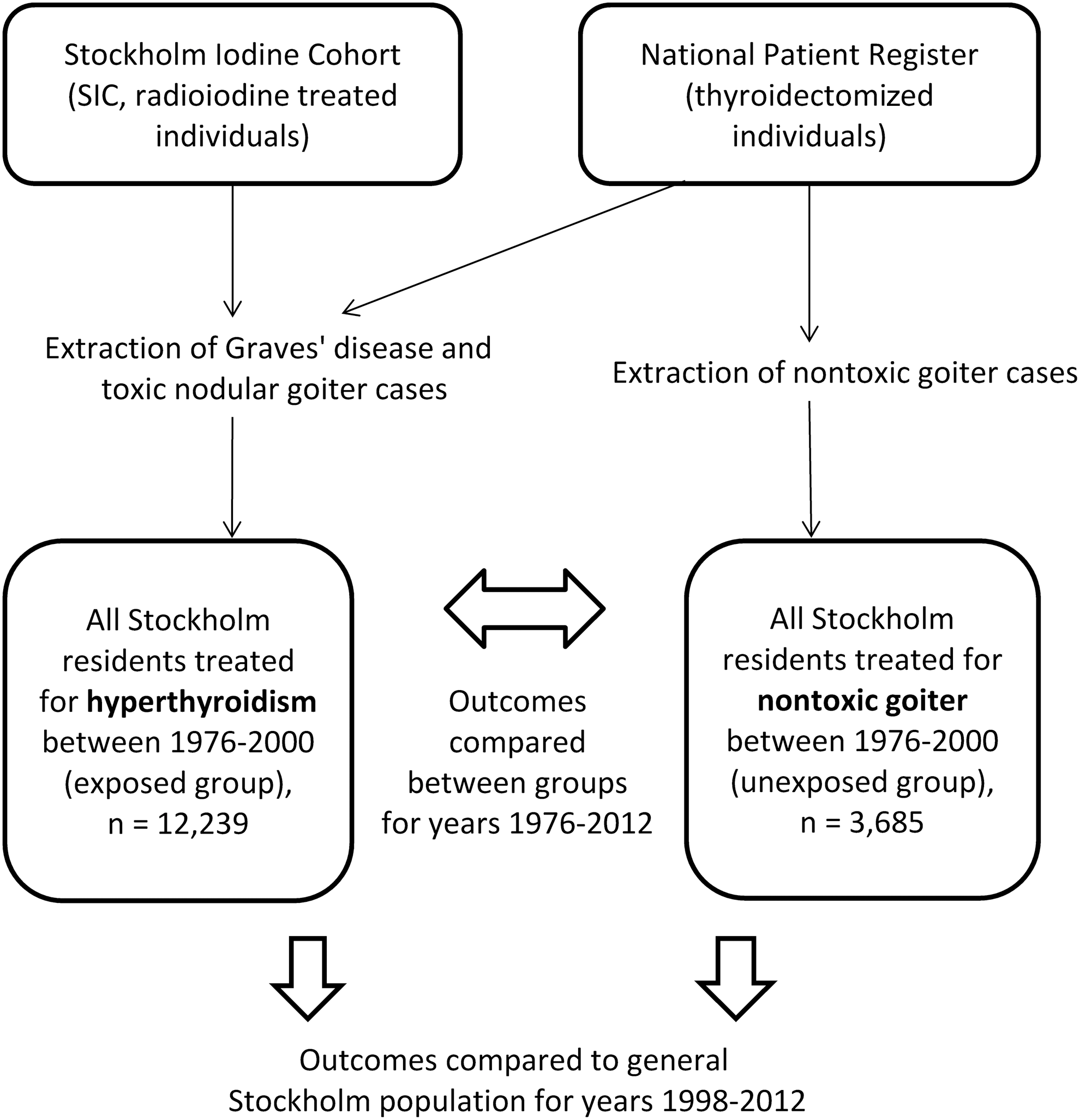
Selection of study cohort.
Baseline comorbidity
Any pre-specified primary diagnosis and up to five secondary diagnoses found in the Patient Register prior to the index event (but not before 1969) were considered baseline comorbidities. Translations between the ICD-8, ICD-9, and ICD-10 classification systems can be found in Supplementary Table 1 (Supplementary Data are available online at
Percentages in relation to whole group with this thyroid disorder. Totals may not sum to 100 due to rounding.
Also included in the overall category of cardiovascular diseases.
Any previous malignancy diagnosis, not specified as ongoing or cured.
p-Values for comparisons between all hyperthyroid patients and nontoxic goiter group.
The pre-specified baseline comorbidities included were diabetes, hypertension, renal failure, chronic obstructive pulmonary disease, rheumatoid arthritis, and psoriasis. These are all recognized risk factors for cardiovascular disease. However, since rheumatoid arthritis and psoriasis may be considered less established risk factors than the other diagnoses mentioned here, a sensitivity analysis excluding these two conditions was also performed (16,19). For each outcome, adjustment was also made for that same prevalent diagnosis.
Outcomes
In the internal comparisons, whereby patients with hyperthyroidism were compared to those with nontoxic goiter, Cox proportional hazards models were used for outcome analyses. When Graves' disease or toxic nodular goiter patients were analyzed separately, individuals with unspecified hyperthyroidism (n = 289) were excluded.
Data from Statistics Sweden was used to assess all-cause mortality until December 11, 2013. The Causes of Death Register was used to assess cardiovascular mortality until December 30, 2012, taking only the underlying cause of death (as opposed to any contributing causes) into account.
To estimate the risk of dying for exposed versus unexposed subjects, a Cox proportional hazard regression was fitted, adjusting for sex, age of inclusion (using restricted cubic spline), and year of inclusion (using restricted cubic spline). In order to estimate potential differences in cause-specific hazard ratios, a cause-specific proportional hazards model was used, treating other deaths as censored (20). Because mean age is known to vary substantially across the different etiologies, outcomes were also stratified into quartiles according to age upon inclusion.
The Patient Register was used to identify incident cardiovascular morbidity after the index event, using the same procedure as for prevalent disease but with follow-up until 2012. Because death is a competing event, the notion of cause-specific hazard regression was used, treating death as censored. Stratification according to age was done in the same manner as for mortality.
Comparisons of both morbidity and mortality were also made to the general population of Stockholm. All three groups of thyroid disorders—Graves' disease, toxic nodular goiter, and nontoxic goiter—were compared separately. When mortality was assessed, Standardized Mortality Ratios (SMR) for death due to all-cause mortality, as well as for any cardiovascular disease, were used. The expected number of deaths was calculated by multiplying the mortality rates in the Stockholm population (divided into strata of five-year age groups, sex, and for each of the years between 1976 and 2013) by the stratum-specific person-time in the cohort. Cause-specific SMR was calculated from 1998 to 2012. As for morbidity, standardized incidence rate ratios for the group of cardiovascular diseases as a whole were used. Standardization was done for sex and age groups, and results are presented for each of the years between 1998 and 2012.
It was not possible to adjust for levothyroxine use as a variable that affected outcomes due to the time gap between the last index event (in 2000) and the start of the prescription register (in July 2005). However, prescription data were used to assess hypothyroidism in those patients who were still alive in 2005.
All analyses were performed in Stata v13.1 (StataCorp, College Station, TX). This study was approved by the Ethical Review Board of Stockholm.
Results
Characteristics of the cohort are presented in Table 1. The study group consisted of 15,924 individuals, of whom 12,239 had been treated for hyperthyroidism (exposed) and 3685 for nontoxic goiter (unexposed). Of the hyperthyroid patients, 6248 were treated for Graves' disease, and 5702 were treated for toxic nodular goiter. For 289 individuals treated for hyperthyroidism, the cause had not been specified.
The study population consisted of 84.7% women. The median ages at diagnosis for Graves' disease, toxic nodular goiter, and nontoxic goiter patients were 54.4, 68.6, and 49.1 years, respectively. By 2013, 8457 persons had died. The median follow-up time was 18.4 years, with an interquartile range of 11.7–25.8 years and a total time at risk of 295,246 person-years. Of the 9650 people still alive in July 2005, levothyroxine was prescribed to 93% in the Graves' disease group, 57% in the toxic nodular goiter group, and 63% in the nontoxic goiter group.
All-cause and cardiovascular mortality
Increased all-cause mortality (hazard ratio [HR] = 1.27 [confidence interval (CI) 1.20–1.35]) and cardiovascular mortality (HR = 1.29 [CI 1.17–1.42]) was found when the hyperthyroid group (Graves' disease and toxic nodular goiter) was compared to the nontoxic goiter group. When the etiology of hyperthyroidism was taken into consideration, an increased risk of all-cause mortality was found both for Graves' disease (HR = 1.14 [CI 1.03–1.27]) and for toxic nodular goiter (HR = 1.42 [CI 1.28–1.57]). Significant differences were also seen during the shorter follow-up time of 10 years. Sensitivity analyses excluding rheumatoid arthritis and psoriasis did not alter these findings. The risk of death from ischemic heart disease or cerebrovascular disease—but not heart failure—was significantly increased, regardless of type of hyperthyroidism or duration of follow-up (Fig. 2). When age quartiles were analyzed separately, Graves' disease patients displayed an increased risk of all-cause and cardiovascular mortality only within the age group 59–70 years, while these risks were consistently increased from ≥46 years in patients with toxic nodular goiter (Supplementary Table S2). When the cohort was divided according to time of inclusion (before and after the year 1990), all-cause and cardiovascular mortality were increased in both types of hyperthyroidism for both time intervals, with the highest point estimate found among toxic nodular goiter patients from the latter period (HR = 1.74 [CI 1.36–2.21]) (5).
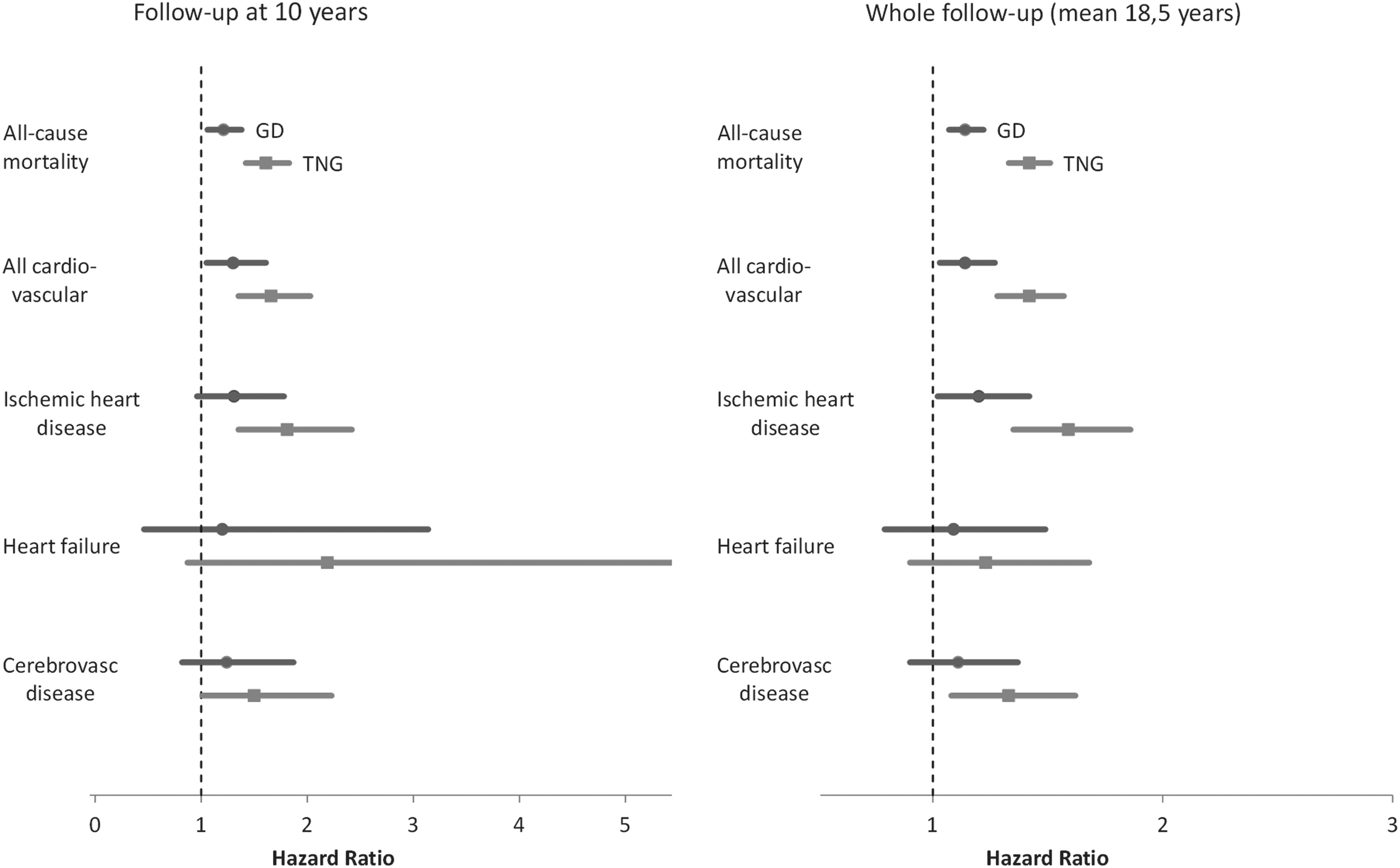
Comparisons of all-cause and cardiovascular mortality for different lengths of follow-up. Horizontal bars denote hazard ratios and confidence intervals for Graves' disease (GD) and toxic nodular goiter (TNG). Dashed vertical line denotes the reference group of nontoxic goiter patients. Adjusted for sex, age, prevalent diabetes, hypertension, renal failure, rheumatoid arthritis, psoriasis, and chronic obstructive pulmonary disease. Each incident diagnosis was also adjusted for its own baseline prevalence.
When compared to the general population, all-cause mortality was increased among hyperthyroid subjects with a SMR of 1.22 [CI 1.20–1.25]. The same was true for cardiovascular mortality (SMR = 1.26 [CI 1.20–1.32]). When analyzed separately, both the Graves' disease group and the toxic nodular goiter group showed increased all-cause and cardiovascular mortality. In the nontoxic goiter group, no excess mortality was found compared to the general population (Supplementary Table S3).
Cardiovascular morbidity
The most frequently occurring cardiovascular outcomes, stratified by age upon inclusion divided into quartiles, are displayed in Supplementary Figure S1. Within each age stratum, the toxic nodular goiter group had an increased risk of cardiovascular disease, while no such association was found for the Graves' disease group. The highest cardiovascular risk was seen among toxic nodular goiter patients between the ages of 46 and 58 years (HR = 1.25 [CI 1.12–1.39]), followed by those between the ages of 59 and 70 years (HR = 1.23 [CI 1.11–1.36]). Heart failure and ischemic stroke were the diagnoses with the highest hazard ratios, ranging from 1.33 to 1.61. The risk of atrial fibrillation was significantly increased only among toxic nodular goiter patients aged ≥59 years.
When stratification was done according to time period of inclusion, increased cardiovascular morbidity was seen among toxic nodular goiter patients in both strata. Among Graves' disease patients, morbidity was increased only among those included after 1990 (Fig. 3).
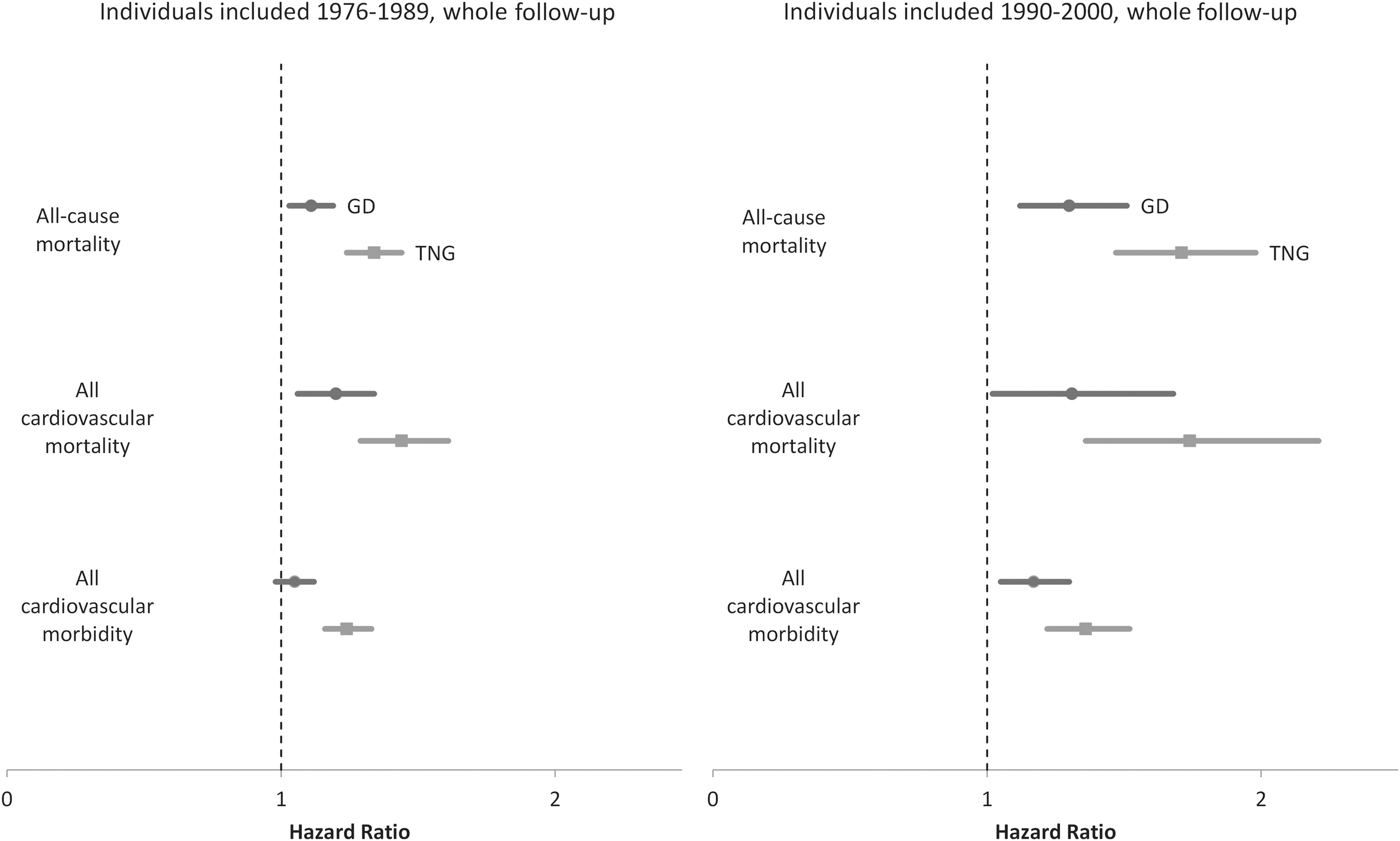
Comparisons of all-cause and cardiovascular mortality, as well as cardiovascular morbidity, stratified according to inclusion time before or after 1990. Horizontal lines represent GD and TNG, with confidence intervals compared to nontoxic goiter (vertical dashed lines). Adjusted for sex, age, prevalent diabetes, hypertension, renal failure, rheumatoid arthritis, psoriasis, and chronic obstructive pulmonary disease. Each incident diagnosis was also adjusted for its own baseline prevalence.
Comparisons of cardiovascular morbidity between the cohort and the general population are displayed as year-by-year standardized incidence rate ratios in Supplementary Figure S2. Point estimates were >1.0 for each of the three groups in all of the years, but these increases were in many cases not statistically significant. The toxic nodular goiter group differed most clearly from the general population, showing significantly increased cardiovascular morbidity in 14/15 years observed.
Discussion
The most important finding from this large, register-based study is that total mortality, cardiovascular mortality, and cardiovascular morbidity were higher in patients with hyperthyroidism compared to patients with nontoxic goiter, as well as compared to the general population. This was true for Graves' disease as well as for toxic nodular goiter, but was most prominent in the latter group, even after both adjustment and stratification for age. The prognosis has not improved over time in contrast to what has been seen for other cardiovascular disorders.
Graves' disease compared to toxic nodular goiter
There is no obvious explanation for the variation seen between different etiologies of hyperthyroidism, with the highest cardiovascular risk being confined to toxic nodular goiter patients. The results of previous smaller register studies have been conflicting (3,5,6,10 –14). As mentioned in a review article by Biondi et al. (21), the pathophysiology behind Graves' disease is not the same as that behind toxic nodular goiter, and the cardiovascular complications are different in both the short and the long term. However, the comorbidities associated with advanced age are more prevalent among toxic nodular goiter patients, since they are generally older, something that also affects the cardiovascular outcomes (21). Interestingly, the cardiovascular risk was found to be highest among toxic nodular goiter patients aged between 46 and 70 years and not in the oldest age quartile.
Among cardiovascular outcomes in terms of morbidity, diagnoses such as atrial fibrillation and heart failure were common in toxic nodular goiter patients. This correlates well with what has been described previously. Apart from the well-known correlation between hyperthyroidism and atrial fibrillation, a well-cited echocardiographic study on hyperthyroid patients has also demonstrated a very strong correlation between atrial fibrillation and heart failure (22,23). Atrial fibrillation is also a known risk factor for stroke, the risk of which was increased in terms of both morbidity and mortality among the toxic nodular goiter cases. This finding is in accordance with previous research on hyperthyroid patients in general (2,3,5,7).
Changes over time
In order to evaluate whether cardiovascular risk had changed during the study period, patients were stratified into groups with an index event before and after year 1990. This choice of date was related to the fact that some of the greatest breakthroughs in cardiology occurred during the late 1980s and early 1990s (24,25). Surprisingly, the cardiovascular risk with hyperthyroidism versus nontoxic goiter was not lower after 1990 compared to the time period between 1976 and 1990. There were also no apparent differences over time when comparisons were made to the general population. Among patients treated for hyperthyroidism, several studies have analyzed the impact of different time periods as a continuous variable. None of these have found the calendar year of inclusion to affect outcomes significantly (1,10,11,26,27). To the authors' knowledge, only one other study has divided patients treated for hyperthyroidism into strata based on the time period when they came under observation. Ryödi et al. (14) reported that among 4334 Finnish patients who had undergone thyroidectomy for hyperthyroidism between 1986 and 2007, those receiving surgery after 1996 had a 20% higher risk of cardiovascular hospitalization compared to age- and sex-matched controls, in contrast to a 12% higher risk in those treated before 1996 (14). The present study showed similar results but also demonstrated higher ratios of all-cause and cardiovascular mortality over time. Taken together, these findings indicate a worrying trend that merits further investigation.
Strengths and weaknesses
Apart from this study's size and long follow-up time, one significant strength is its reference group of individuals treated with thyroidectomy for nontoxic goiter. These individuals are more similar to patients treated for hyperthyroidism, as can be seen from the high incidence of hypothyroidism during follow-up in both groups. Potential confounding due to age differences between groups was addressed both by adjusting for age as a continuous variable and by stratifying for age upon inclusion. Another strength of this study is that it is based on data from nationwide registers, with very few patients lost to follow-up. Virtually complete coverage of all patients treated within a specified geographic area reduces the risk of inclusion bias. Furthermore, results from internal comparisons (hyperthyroidism vs. nontoxic goiter) were cross-checked with population-level data.
The main limitation of this study is that it is based on register data that lacked information about individual parameters such as body weight, lipid profile, and smoking. Although the Swedish Patient Register is considered to be reliable with regards to several cardiovascular diagnoses, the Death Register has not been as conclusively validated (28,29). There was no access to information about possible subclinical dysfunction prior to inclusion in the study, and it was not known how patients responded to treatment (although it was known that the proportion of levothyroxine-treated individuals was high in each group in 2005). Also, patients treated with antithyroid drugs were not included because they were not registered in national databases during the time period studied. Furthermore, no one in the unexposed group of nontoxic goiter patients had received radioiodine treatment.
In summary, the limitations of this study are largely the same as those found in other register-based research on the same topic. The most obvious of these are the incompleteness of baseline data and the lack of information about patients treated with antithyroid drugs. Such flaws always introduce the possibility of both confounding and selection bias. Prospective trials will ultimately be necessary to resolve this issue. However, a few specific strengths of this study—most notably its size, but also its recent follow-up data and the novel choice of reference group—separate these results from those made earlier, outweighing the limitations and adding relevant information to what was already known.
In conclusion, this study indicates that the increased cardiovascular risk in hyperthyroid patients is related to the disease itself rather than its treatment. Much of the excess mortality and morbidity is found among individuals treated for toxic nodular goiter. Despite breakthroughs in cardiovascular care during recent decades, hyperthyroidism is still a diagnosis associated with increased cardiovascular risk.
Footnotes
Acknowledgments
This study was supported by funds from the Cardiology Clinic of Danderyds Hospital (Stockholm, Sweden), the Swedish Endocrine Society, the Swedish Heart and Lung Foundation, and Carl Bennet AB. The authors would especially like to thank Professor Per Hall for his important contribution in assembling data for the Stockholm Iodine Cohort. A selection of the preliminary results was presented as an abstract at the 2015 European Society of Cardiology congress in London, under the title “Increased Cardiovascular Risk after Treatment for Hyperthyroidism.”
Author Disclosure Statement
No competing financial interests exist.