
Abstract
Background:
The current trend of less aggressive treatment of low-risk differentiated thyroid cancer (DTC) patients was recently challenged by a study reporting >10% disease-related mortality (DRM) in low-risk patients ablated with radioiodine activities below 54 mCi. However, this study and others were limited by incomplete data on disease severity at presentation. Whether patients presenting with low-risk disease are at risk for disease-related mortality is crucial for planning current treatment strategies.
Methods:
Patients with documented DRM from DTC were included from the Rabin thyroid cancer registry and the Davidoff Head and Neck cancer service databases. Disease characteristics at presentation, treatments, disease course, and cause of death were analyzed.
Results:
Of 1374 patients whose charts were reviewed, 56 were confirmed to have died of DTC, and 53 had sufficient data for analysis. Median time from diagnosis to death was 9 years (range 1–36). Cause of death was related to distant metastases in 46 patients and aggressive neck disease in 7 patients. The median age at diagnosis was 62 years (range 22–83, 83% older than 45), and were initially categorized as American Thyroid Association high risk in 89% of cases (in 4 cases due to high thyroglobulin levels), intermediate risk in 6% (3 older patients with N1b disease), misclassification as benign in one case, and none was low risk. Most patients had an advanced disease stage (stage IV, 88%; III, 2%; II, 2%; I, 8%). All patients with stage I disease were <45 years, with aggressive features (1 poorly differentiated, 3 gross extrathyroidal extension). One patient with stage II disease was <45 years and had distant metastases. Detection of distant metastases occurred within the first year in 25 patients and during subsequent follow-up in 25 patients. Overall, aside from one patient who was misdiagnosed as having a benign follicular adenoma at presentation, all patients had aggressive disease features at presentation.
Conclusion:
None of the patients with DRM had low-risk features at presentation, supporting the current paradigm of less aggressive approach in the low-risk group. Studies analyzing mortality from thyroid cancer should stratify patients into the various risk categories based on full baseline data, including postoperative thyroglobulin levels.
Introduction
D
In contrast to studies reporting a very low disease-related mortality (DRM) rates in low-risk DTC patients, a recent study by Verburg et al. (8) reported DRM of more than 10% in low-risk patients treated with radioiodine (RAI) activity of less than 54 mCi and with long-term follow-up. Though this study challenged the recent trend in the 2015 American Thyroid Association (ATA) guidelines of less aggressive treatment in low-risk patients, it was limited by incomplete patient information at baseline. According to their results, the authors recommend a more aggressive approach to treatment of low-risk patients. It is therefore crucial to investigate disease severity at presentation in patients who die of thyroid cancer, and specifically the risk of mortality in low-risk DTC patients.
The objective of our study was therefore to analyze the initial presentation of patients who eventually died from DTC and were treated in a referral center for thyroid cancer.
Patients and Methods
Data on patients with DRM was obtained from two databases: the Rabin Medical Center thyroid cancer registry, containing 1187 patients with DTC, and the database of the head and neck cancer service at the Davidoff Cancer Center, which serves as a regional referral center, including 187 patients with advanced thyroid cancer. The Rabin Medical Center is a tertiary referral center providing comprehensive care for patients with thyroid cancer in a multidisciplinary environment including the ear, nose, and throat, endocrinology, and nuclear medicine departments. In 2005, we started a registry of all patients with nonmedullary thyroid carcinoma followed since 1973 at our Endocrine Institute. Patients entered the registry retrospectively if operated before 2005 and prospectively thereafter. For the present study patients with DRM from DTC were included of the total 1187 patients entered into the registry to date. The Davidoff Head and Neck Oncology Service is a tertiary referral for patients with all types of head and neck cancers. Thyroid cancer patients requiring systemic therapy, palliative care, or external radiation treatment are referred to this service.
Disease-related mortality was determined when patients fulfilled all the following criteria: (1) patients with histologically proven thyroid cancer, (2) presence of distant metastases from DTC or persistent local aggressive disease, (3) progressive disease, (4) mortality directly from progressive disease or from complications caused by the disease (e.g., post-obstructive pneumonia). All mortality cases were reviewed by an experienced thyroid cancer specialist (E.R.), who identified 93 patients with DRM: 39 from the Rabin Medical Center registry and 54 from the Davidoff Cancer Center database. Sufficient data required for this study included at least a pathology report or description of the pathology in the patient charts, data on post-radioiodine therapy whole-body scan, and Tg levels plus TgAb in patients without known distant metastases. Forty patients were excluded, due to anaplastic thyroid cancer in 29 cases, medullary thyroid carcinoma in 8 cases, and insufficient data in 3 cases (Fig. 1). Therefore, 53 patients were included in the study.
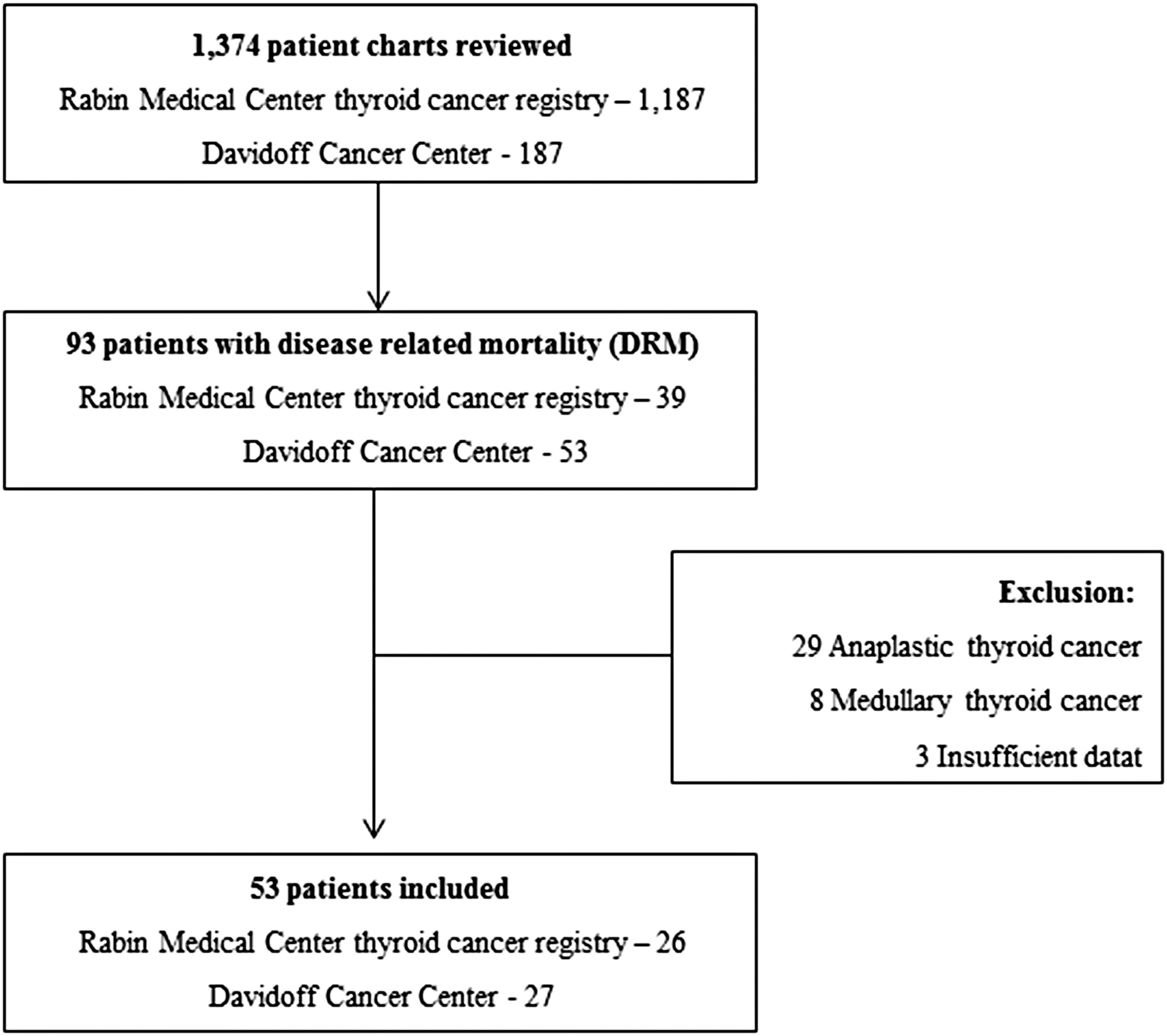
Patient inclusion flow chart.
Data collection included surgical report of the initial surgery; pathology report; imaging from the first year following diagnosis; thyroglobulin levels and antithyroglobulin antibodies titers; radioiodine treatments and whole body scan reports; data of additional surgeries; and additional treatments including external beam radiation; chemotherapy, or targeted systemic therapies; and the cause of death. Data completeness was assessed and documented for each patient. “High-risk features” included distant metastases, gross extrathyroidal extension, poorly differentiated histology, N1b disease in patients over 45 years of age, and postoperative serum thyroglobulin suggestive of distant metastases (>20 ng/mL) within six months of surgery. Patients were categorized according to the revised 2015 ATA risk classification and American Joint Committee on Cancer (AJCC) staging system.
Continuous data are presented either as means and standard deviations or median and ranges, as appropriate for each variable. Categorical comparisons were performed with Fisher's exact test. Analysis was performed using SPSS software (Version 20.0.1; SPSS, Inc., Chicago, IL). A p-value ≤0.05 was considered statistically significant.
Results
Fifty-three patients with DRM diagnosed between 1973 and 2015 were included in the study. Mean time from diagnosis to death, which equals the follow-up time, was 9.2 ± 7.6 years, with a wide distribution from 1 to 36 years (Fig. 2). Year of death was between 2002 and 2016.
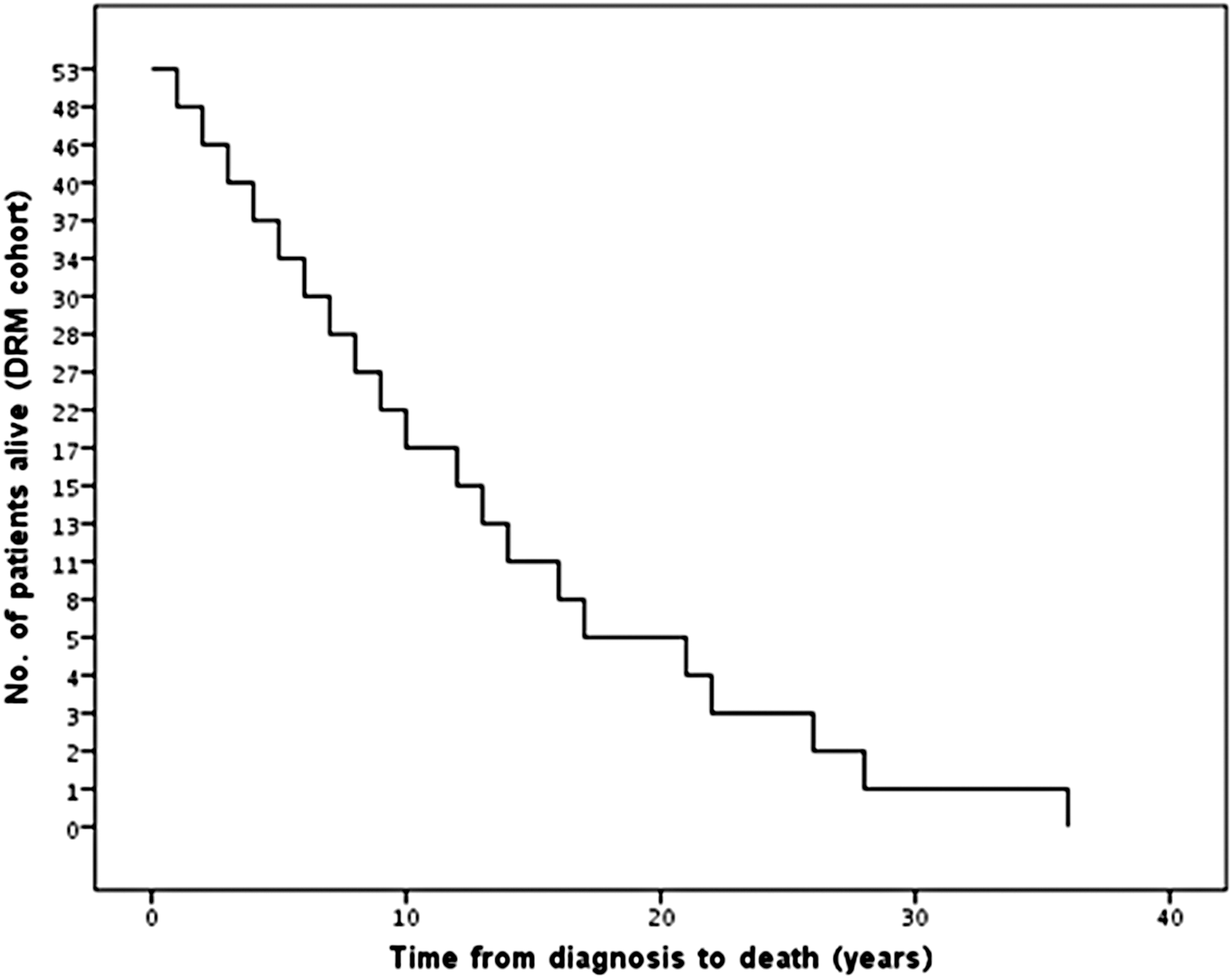
Time to death in patients with disease-related mortality from thyroid cancer. Median time to death was 9 years (range 1–36), with a mean of 9.2 ± 7.6 years.
Initial clinicopathological characteristics
Apart from one patient who was initially misdiagnosed as follicular adenoma, all patients had high-risk features at diagnosis (Table 1): 70% of patients had gross extrathyroidal extension, 51% had upfront distant metastases, 45% had lateral neck lymph node metastases, and 26% had poorly differentiated thyroid carcinoma. In four patients who did not have these high-risk features initially, postoperative nonstimulated thyroglobulin was markedly elevated (range 138–1900 ng/mL) (Table 2).
PTC, papillary thyroid cancer; FTC, follicular thyroid cancer; ETE, extrathyroidal extension.
This table describes the one most aggressive feature at the time of presentation (e.g., if a patient had distant metastases, lymph node metastases and high Tg levels, then distant metastases are the highest risk feature).
One patient was initially misdiagnosed as benign follicular adenoma, Tg levels were not measured.
T4, thyroxine.
At presentation, 83% of patients had stage IV disease, reflecting their high risk of mortality, but eight patients (15%) had disease stages I to III. All of these patients had high-risk features: One stage III patient had a Tg of 243 ng/mL, which was first measured 6 months after surgery, two patients with stage II disease were younger than 45 years with distant metastases, and five patients with stage I disease were younger than 45 years with gross extrathyroidal extension (ETE) in three patients, and poorly differentiated carcinoma in two patients. Using the 2015 revised ATA risk assessment tool for recurrent/persistent disease, 89% were categorized as high risk, 6% were categorized as intermediate risk, and none had low risk disease (Table 1). Two patients had insufficient data for the ATA categorization, and one patient was initially misdiagnosed as follicular adenoma. All three patients who were categorized as ATA intermediate risk had AJCC stage IV disease due to lateral neck lymph node metastases in patients over 45 years.
Treatment and disease course
Initial treatment included total or subtotal thyroidectomy in 94% of patients, with lateral neck dissection in 43% of patients. Three patients had inoperable disease and were treated with external beam radiation to the neck. The median activity of the first radioiodine treatment was 166 ± 58 mCi, with no significant differences in cumulative mean activities administered between 1974 and 1990 (595 ± 363 mCi) and 1990 to 1999 (555 ± 202 mCi), but with lower administered activities between 2000 and 2015 (376 ± 175 mCi, p < 0.01). This difference is due to five patients who had incomplete resection of aggressive locoregional disease, and were initially treated with 30 mCi.
Sixty percent of patients were treated with external beam radiotherapy for tumors with gross ETE, 23% received external beam radiotherapy for bone metastases, and 6% for brain metastases (Table 3). Radiation dose ranged from 50 to 70 Gy for the neck and 20 to 40 Gy for metastases. Only 27% of patients were treated with systemic therapies, as most included patients were treated before the availability of kinase inhibitors for thyroid cancer. Four patients were treated with chemotherapy with no apparent effect, and 10 patients (19%) were treated with Sorafenib.
In patients without known metastases at presentation.
Cause of death
Cause of death was related to distant metastases in 46 patients (87%) and aggressive neck disease in 7 patients (13%). Mean postoperative thyroglobulin was 3166 ± 8920 ng/mL. The immediate cause of death was general deterioration in 33 patients (25 under supportive care, 5 treated with Sorafenib, and 3 treated with chemotherapy); respiratory failure in 9 patients; postobstructive pneumonia in 5 patients; massive hemoptysis or bleeding from tracheostomy in 3 patients; upper airway obstruction in 2 patients; and pulmonary embolism in one patient. Mean age of death was 68.7 ± 12 years.
Discussion
Our study evaluated a rare group of patients with DRM from DTC, allowing us to obtain insights into the long-term perspective of patients with the most severe forms of the disease. The 53 included patients represent 3.8% DRM rate in our cohort (2% in the Rabin Medical Center registry and 14% in the Davidoff cancer patients), which is higher than expected in the general population and represents referral bias of patients with advanced disease to hospital care. However, since virtually all patients who eventually die from DTC are referred to hospital clinics, the unique group of patients included in our study is considered representative of patients with DRM in terms of histology, low or high risk at presentation, and time from diagnosis. In contrast to previous studies suggesting patients with low-risk classification sometimes die from the disease (2,8), our study shows that when full baseline information is available, all patients with DRM had high-risk features at presentation. We expected to find at least some patients with low-risk disease presentation among our cohort since this is the largest risk group (1,9,10), and even if mortality is rare in this group it would be expected to have some representation. The fact that none of the included patients had low-risk disease at presentation is a strong indicator that DRM rate is extremely rare in this group.
According to our data, the potential for misclassification of patients as low-risk in the setting of large databases is significant, since many variables are needed to accurately determine risk level, including imaging studies (pre- and postoperatively), intra-operative findings, high-risk features on pathology report (histologic subtype, extrathyroidal extension, and extent of lymph node involvement), Tg levels, TgAb titers, and posttherapy radioiodine scans. In accordance with previous studies (11,12), 83% of our patients were initially diagnosed with stage IV disease due to gross ETE, N1b disease in older patients, and distant metastases. However, the remaining 13% were initially considered as having stage I to III disease and therefore not necessarily considered at high risk for mortality. These patients were either <45 years old with aggressive locoregional disease, had aggressive histology (poorly differentiated carcinoma), or had high postoperative Tg levels, and therefore had aggressive features warranting more advanced treatments and follow-up. It is important to note that in 7% of patients Tg levels were the first high-risk feature to suggest significant spread of the disease, and Tg should be measured before performing postoperative risk stratification.
The recently published 2015 ATA thyroid cancer guidelines recommend several changes in the treatment of low-risk patients, including lobectomy as an alternative to total thyroidectomy, selective use of radioiodine, and if radioiodine is administered, lower activities are recommended for remnant ablation (30 mCi) compared with activities used for adjuvant therapy (13). It is therefore interesting to examine whether any of the patients with DRM would be undertreated with the implementation of these guidelines. Using the 2015 modified ATA risk classification, all included patients were defined as intermediate (with high-risk features) or high risk of recurrence, necessitating total thyroidectomy with neck dissection as adequate and an adjuvant dose or radioiodine. Of note, one patient was initially misdiagnosed as having follicular adenoma instead of follicular carcinoma. For these cases we now recommend postoperative Tg and TgAb measurement, with occasional repeated measurements during follow-up. Overall, our data confirm the adequacy of the ATA risk classification scheme, the concept that low-risk patients are at extremely low risk of mortality and can be treated less aggressively, and that patients with aggressive disease would receive more advanced treatment (13).
Several previous studies analyzed patients with DRM managed over the past century (11,12,14 –22). Of these studies only three reported baseline information on disease presentation, including sex, age, histology, ETE and lymph node involvement (11,12,21) but none reported postoperative Tg levels. In a study by Smith et al. from the Mayo Clinic published in 1988, 56 lethal papillary thyroid carcinomas were included from 859 patients (7%) (12). The presenting symptoms in the group with DRM were typical of aggressive disease, with palpable disease in 73%, gross ETE in 43%, and mean tumor size of 4.3 cm. However, information regarding distant spread was limited, as only two patients were treated with RAI, and imaging was based on plain chest and bone x-ray. A more recent publication by Nixon et al. from Memorial Sloan Kettering Cancer Center included 17 patients with DRM who were considered free of macroscopic disease after initial treatment (11). Similar to our results, 71% of patients had high-risk disease at presentation, 29% had intermediate risk, and none had low risk disease. A third small study by Grogan et al. included 24 patients who died from thyroid cancer out of a cohort of 269 patients (9%) who were followed for 27 years (21). Of the patients with DRM, 62% had stage IV disease, 29% distant metastases, 21% gross ETE, and 42% locoregional spread. Five patients had stage I disease, but there was no information on their baseline disease characteristics. While most studies reported overall survival, few institutional cohort studies reported disease-specific survival stratified according to risk groups. These studies demonstrated no DRM in patients with papillary microcarcinomas (22), in ATA low-risk patients (23), and in MACIS system (Metastases, Age, Completeness, Invasion, Size) low-risk patients followed since the 1970s at the Mayo Clinic (24), with and without RAI ablation. In one outlier study that reported DRM rates of >10% in low-risk DTC patients treated with RAI activity of less than 54 mCi, there was little data on baseline characteristics, and it thus seemed to be prone to misclassification of patients as low risk. Overall, these studies contain partial information on disease presentation in patients with DRM, supporting the importance our study.
Our study has several limitations. First, mortality from thyroid cancer is rare and may occur many years after initial diagnosis (up to 36 years in our study). It is therefore possible that follow-up of low risk cases diagnosed during the last decade is too short, and they are not well represented in our study. Second, there is a risk for selection bias in patients with DRM. This risk is probably low, as patients with advanced disease are referred to hospital care, irrespective of time of initial diagnosis and tumor histology. For example, while patients with medullary and anaplastic thyroid cancer were excluded from our study, these two rarest forms of thyroid cancer represented 40% of all patients with DRM due to their more aggressive behavior. Third, advances in treatment of advanced disease have evolved during the last decade, which may have changed the landscape of mortality from thyroid cancer. Indeed, 19% of included patients were treated with kinase inhibitors, and 8% with chemotherapy before the availability of kinase inhibitors for thyroid cancer. However, these therapeutic advances for advanced disease have little impact on the study focus, which is disease severity at presentation.
In conclusion, none of the patients who died from DTC had low-risk features at presentation, supporting the current paradigm of less aggressive approach in the low-risk group. Future studies reporting DRM from thyroid cancer should carefully classify patients as low risk, as this requires full baseline information including Tg levels. This would prevent overestimation of risk and overtreatment in this group.
Footnotes
Author Disclosure Statement
No competing financial interests exist.