
Abstract
Background:
The risk of recurrence in patients with differentiated thyroid cancer (DTC) can be estimated based on their response to initial therapy. The aim of this study was to evaluate an adequate follow-up strategy for DTC patients with an excellent response by assessing the characteristics of structural recurrence.
Methods:
This historical cohort study included 1359 DTC patients who had excellent response to total thyroidectomy with radioactive iodine remnant ablation.
Results:
Among 1359 patients, 703 (54%) patients were classified as stage I according to the seventh tumor node metastasis staging system, and 987 (73%) patients were classified as intermediate risk according to the American Thyroid Association's risk stratification after initial therapy. During a median of 8.7 years of follow-up, only 13 (1%) patients were confirmed to have structural recurrence. All of the recurrences were locoregional disease, and there were no distant metastases. Recurrences were detected late at a median of 5.5 years after the initial surgery (range 3.6–10.7 years). All structural recurrences were detected on neck ultrasonography. Non-stimulated serum thyroglobulin (Tg) was detectable (≥0.2 ng/mL) in four (31%) patients, and serum anti-Tg antibodies were positive in one (8%) patient. However, non-stimulated serum Tg levels were stably low (<0.2 ng/mL) in eight (62%) patients when recurrences were detected. In addition to these 13 patients, 14 patients also presented with biochemical persistent disease at the end of follow-up.
Conclusions:
Recurrences of DTC in patients with an excellent response to initial therapy were detected relatively late. The intensity and frequency of follow-up of neck ultrasonography as well as serum Tg and anti-Tg antibody measurements should be reduced, especially within five years of the initial therapy, in DTC patients who have an excellent response.
Introduction
P
According to a previous study, recurrent DTC disease was detected 5–35 years after initial treatment (5), and thus long-term follow-up is needed for patients with DTC. However, the role of long-term follow-up of patients who were confirmed as having an excellent response to therapy is controversial (6,7). Because of its low recurrence rate, routine neck ultrasonography (US) exams might not be cost-effective and may cause frequent false-positive results (8,9).The ATA's recent management guidelines for DTC recommend that the intensity and frequency of follow-up should be decreased in patients with an excellent response. Clinical examination with regular measurement of non-stimulated thyroglobulin (Tg) at intervals of 12–24 months is recommended, and periodic US exam can also be considered, but this recommendation is weak due to low-quality evidence (2). One study found that all DTC recurrences were diagnosed within eight years after initial therapy with the aid of recently improved technology (10). However, there was not enough evidence to indicate for how long or at what interval patients with an excellent response need to be followed.
This study aimed to evaluate the characteristics of structural recurrent disease detected in patients who have an excellent response to TT with RAI remnant ablation. Excellent response was confirmed by stimulated Tg (sTg) and anti-Tg antibody (TgAb) levels, neck US, and diagnostic whole-body scan (DxWBS). Ultimately, the aim was to define appropriate follow-up strategies for DTC patients who had excellent responses to initial therapy.
Methods
Study subjects
This retrospective cohort study reviewed the medical records of 1801 DTC patients who underwent TT with RAI remnant ablation from 2004 to 2007 at the Asan Medical Center (Seoul, Korea) and who had adequate follow-up data to assess their initial response to therapy. Finally, 1359 patients were determined to have had an excellent response to initial therapy according to the criteria from previous studies (3,4), and were thereby eligible for analysis (Supplementary Fig. S1; Supplementary Data are available online at
Follow-up protocol after initial treatment
All patients included in this study underwent TT with/without prophylactic central neck dissection or therapeutic central and lateral neck dissection. Subsequent RAI remnant ablation was also conducted according to a protocol that has been previously reported (4,11). After initial therapy, patients took levothyroxine for thyrotropin (TSH) suppression and were regularly followed, as previously reported (4,11). Briefly, neck US and DxWBS with measurement of serum sTg and TgAb levels were performed during the first 6–24 months after initial therapy, and the dynamic risk stratification by the response to initial therapy was assessed. For patients classified in the excellent response group, serum Tg and serum TgAb levels were measured, and neck US was performed regularly every 6–24 months with physical examinations and thyroid function tests. Measurements of serum Tg and TgAb levels were done, as previously described (12).
Neck US examination
All patients underwent neck US examination by experienced radiologists using an HDI 5000 or IU22 scanner (Philips Medical Systems, Bothell, WA) with a 12.5 MHz linear phased-array transducer, as previously reported (12). US features suggestive of a metastatic lymph node (LN) were round shape (long-axis to short-axis ratio of <1.5), absence of an echogenic hilum, microcalcification, cystic changes, and peripheral blood flow on color Doppler images. Experienced radiologists also performed US-guided fine-needle aspiration (FNA) on suspicious metastatic or indeterminate cervical lesions whose long diameters in the transverse plane were ≥0.5 cm.
Definitions
An excellent response was defined as levels of serum sTg <1 ng/mL and serum TgAb ≤60 IU/mL with no suspicious metastatic lesions on neck US or DxWBS, which was performed during the first 6–24 months after the initial therapy (2 –4). Patients were also categorized according to the seventh edition of the American Joint Committee on Cancer (AJCC)/International Union against Cancer (UICC) Tumor Node Metastasis (TNM) staging system and ATA initial risk classification (low, intermediate, and high risk of recurrence) (1,13).
Structural recurrent disease was defined as pathologically or cytologically proven metastatic lesions and/or metastatic lesions in other distant organs by imaging studies with elevated Tg levels during follow-up, as previously reported (4,11).
Patients were considered to have no evidence of disease (NED) if they had a serum non-stimulated Tg (ns-Tg) level of <0.2 ng/mL with negative serum TgAb and negative imaging findings at the end of follow-up (2). Patients showing a serum ns-Tg ≥0.2 ng/mL or positive TgAb without evidence of structural disease at the end of follow-up were considered to have biochemical persistent disease, and patients with structural disease confirmed pathologically or cytologically at the end of follow-up were considered to have structural persistent disease (3,4,11).
Statistics
R v3.1.0 and R libraries survival, car, and Cairo were used to analyze data (R Foundation for Statistical Computing;
Results
Baseline characteristics of patients
The baseline characteristics of 1359 patients who had an excellent response to initial therapy for DTC are shown in Table 1. The median age of patients was 49 years (IQR = 41–56 years), and 1196 (88%) patients were female. The majority of patients had the classical variant of papillary thyroid carcinoma (PTC), and the mean tumor size was 1.1 ± 0.8 cm. Cervical LN metastasis was confirmed in 584 (44%) patients after initial surgery. According to the seventh TNM staging system, 703 (54%) patients, four (0.3%) patients, 597 (46%) patients, and 55 (4%) patients were classified as stage I, II, III, and IV, respectively. According to the ATA initial risk stratification, 368 (27%) patients were classified as low risk, 986 (73%) patients were classified as intermediate risk, and five (0.4%) patients were classified as high risk. All patients underwent subsequent RAI remnant ablation, and the median RAI dose was 3.0 GBq (IQR = 1.1–5.6 GBq). During a median 8.7 years of follow-up (IQR = 7.3–9.7 years), only 13 (1%) patients were confirmed to have structural recurrent disease.
Lymph node metastasis and TNM stage were determined by the seventh edition of American Joint Committee on Cancer (AJCC)/International Union against Cancer (UICC) TNM staging system.
SD, standard deviation; PTC, papillary thyroid cancer; FTC, follicular thyroid cancer; TNM, tumor node metastasis; ATA, American Thyroid Association.
Characteristics of patients with recurrence
The clinicopathologic characteristics of 13 patients with structural recurrent disease are summarized in Table 2. All these patients were classified as intermediate risk according to the ATA initial risk stratification. No preoperative or immediate postoperative clinicopathologic characteristics of patients associated with recurrence could be found.
Patient 4 was lost to follow-up right after the diagnosis of the structural recurrence. Patient 8 underwent radiofrequency ablation for the recurred tumor. The size of these recurred tumors was measured by neck US.
Patient 6 underwent thyroid hormone withdrawal twice, but thyrotropin levels were all <30 mIU/L. However, non-stimulated Tg levels were steadily <0.2 ng/mL, and the patient was considered as having an excellent response.
The final outcomes could not be assessed in these patients who underwent reoperation within three months.
LN, lymph node; Tg, thyroglobulin; TgAb, anti-thyroglobulin antibody; TT, total thyroidectomy; CND, central neck dissection; MRND, modified radical neck dissection; Y, yes; N, no; N/A, not available.
All of the recurrences were locoregional disease, and there were no distant metastases in these patients. Recurrences in lateral cervical LNs were detected in eight (62%) patients, and the five (36%) remaining patients had a recurrence in the central cervical compartment. In these patients with an excellent response, the recurrences were detected late at a median of 5.5 years after initial surgery (range 3.6–10.7 years), with the majority of recurrences detected five years after initial surgery (Supplementary Fig. S2).
Out of 13 patients, 11 underwent reoperation for recurrent disease, one patient underwent radiofrequency ablation, and one patient was lost to follow-up after diagnosis of the recurrence. After additional treatment for the recurrent disease, eight patients were confirmed to have NED, one patient had biochemical persistent disease with decreasing serum TgAb, and one patient who underwent RFA had structural persistent disease at the end of follow-up. The final outcomes could not be assessed in one patient who was lost to follow-up and two patients who underwent reoperation within three months.
Detection of recurrence
All structural recurrent diseases were detected by neck US. These were all newly detected lesions compared to previous neck US, which was performed at a median 18 months prior (range 6–33 months).
At the time of confirmation of structural recurrent disease by neck US, serum ns-Tg was detectable (≥0.2 ng/mL) in four (31%) patients, and serum TgAb was positive in one (8%) patient. Changes in serum ns-Tg levels of patients with recurrence during follow-up (except one patient with positive TgAb) are presented in Figure 1. In eight (62%) patients, serum ns-Tg levels were stable and low (<0.2 ng/mL) with negative TgAb when the structural recurrences were detected. In these eight patients, there were no suspicious symptoms of recurrence, and the structural recurrent disease was detected by routine neck US.
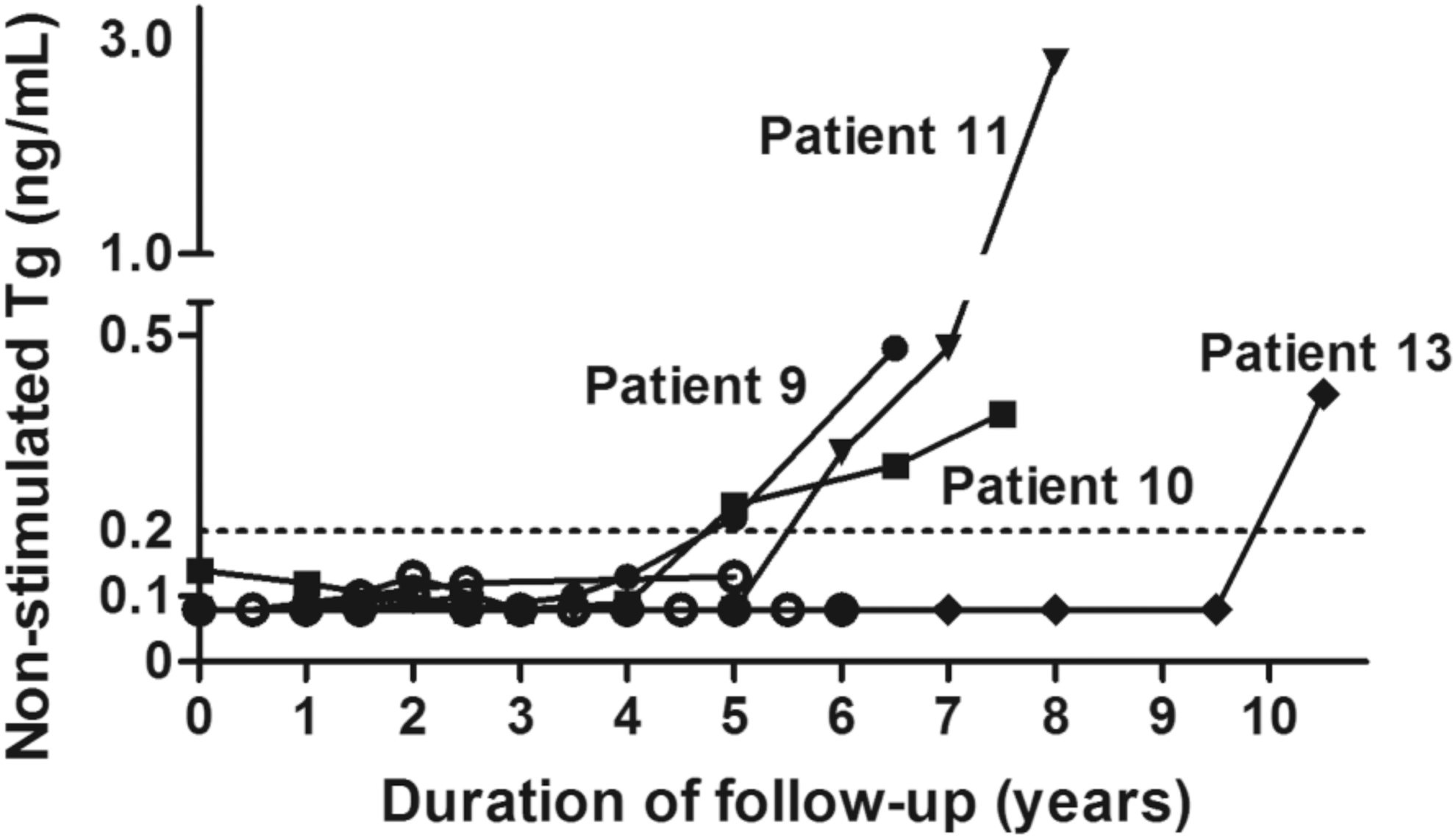
Changes in the serum non-stimulated thyroglobulin (Tg) levels of patients with structural recurrent disease. The serum non-stimulated Tg level was steadily <0.2 ng/mL in eight patients and increased during follow-up in four patients. The serum non-stimulated Tg level of one patient with positive TgAb was not included in this figure.
In four patients who had detectable serum ns-Tg levels when the recurrences were detected, serum ns-Tg levels gradually increased in three patients, and abruptly increased in one patient at 10 years after the initial surgery. One patient with gradually increasing serum ns-Tg presented with a palpable neck mass in the central neck area. One patient with positive TgAb had steadily increasing serum TgAb levels. Five patients, including four patients with detectable serum ns-Tg and positive TgAb, had a longer duration from the initial surgery to the detection of recurrence, and the lesions tended to be multiple and larger compared to the eight patients with undetectable serum ns-Tg levels (Table 2).
Patients with biochemical persistent disease
In addition to the 13 patients who had confirmed structural recurrent disease during follow-up, 14 patients also presented with biochemical persistent disease at the end of follow-up. Three patients had levels of serum ns-Tg ≥0.2 ng/mL. Among them, two patients presented with stably low but detectable serum ns-Tg values. However, one patient had a recent abrupt increase in serum ns-Tg level from 0.08 to 0.98 ng/mL after 10 years from the initial therapy, without any suspicious lesions on US.
Additionally, there were 11 patients with positive serum TgAb without any structural evidence of recurrence. Eight patients presented stable or declining TgAb levels, and three patients had steadily increasing TgAb levels.
Discussion
This study confirms the excellent clinical outcomes of DTC patients who were found to have an excellent response to initial therapy (2,14). Structural recurrent disease was detected late, even with regular follow-up of serum Tg, TgAb, and neck US, with 6- to 24-month intervals in these patients. The duration from initial surgery to the detection of the recurrence was between 3.6 and 10.7 years, and the majority was detected five years after initial surgery. This is consistent with a previous study showing that structural disease recurrence was identified at a median of 6.3 years after surgery (8). In the present study, the structural recurrent disease manifestations detected within five years of surgery were all small and single lesions, and these findings might be due to the early detection of the recurrences. The findings suggest that frequent follow-up of serum Tg, TgAb, and neck US within five years of surgery might not be cost-effective. However, long-term regular follow-up might be needed in these patients because newly developed structural recurrent disease can occur 10 years after the initial surgery (6). Furthermore, there were no distant metastases, and all of the structural recurrences were locoregional disease. After additional treatment for structural recurrent disease, most patients finally had NED. This finding suggests that additional imaging studies outside of neck US are not necessary for DTC patients with an excellent response, even if biochemical disease is present during follow-up.
All recurrent lesions were detected by neck US, and only five patients presented with biochemical evidence of recurrent disease at the time of the detection of the structural recurrent disease. These five patients, compared to the other eight patients with undetectable serum ns-Tg (<0.2 ng/mL) and negative TgAb, were likely to have a longer duration from the initial surgery to the detection of the recurrence, and they were also likely to have multiple, larger metastatic lesions. These findings suggest that neck US might be more sensitive to detect recurrences than the measurement of serum ns-Tg and TgAb levels. Regular but infrequent neck US examination might be helpful for earlier detection of recurrence in DTC patients with an excellent response. However, there were also 14 patients with biochemical persistent disease at the end of follow-up. These findings also suggest that the measurement of serum ns-Tg and TgAb levels, and neck US are complementary. These results are different from a recent study suggesting that only periodic measurement of serum Tg levels might be sufficient in follow-up of PTC patients with low or intermediate risk and excellent response to initial therapy (7). The definition of an excellent response in that study was different from the present study, and patients who were classified as having an indeterminate response by the definition in this study might have been classified as having an excellent response. Therefore, recurrences were more prevalent (including one patient with pulmonary metastasis) and detected earlier in that study compared to this study. Differences in the Tg measurement method may also be responsible for the observed differences in results. Even though this study used a radioimmunoassay, the functional sensitivity of the assay was not different from second-generation Tg immunometric assays with a functional sensitivity of 0.2 ng/mL (12,15).
Neck US is sensitive and helpful for the early detection of recurrence. However, there are concerns about false-positive suspicious findings in routine and frequent neck US examinations (8,16). Furthermore, frequent neck US examinations were not cost-effective in a previous study (9). On the contrary, there is also a risk of false-negative results with neck US. Currently, there is no firm evidence of an adequate interval for neck US. In this study, all structural lesions were newly detected compared to the previous neck US, and the median interval of neck US exams was 18 months. Thus, an interval of >18 months could be appropriate for follow-up. However, this interval might be affected by the follow-up protocol because neck US is usually performed regularly every 6–24 months. More confirmatory studies are needed to find an adequate interval for neck US exam in DTC patients with a low risk of recurrence.
This study has limitations due to the nature of its retrospective design and the fact that patients from a single tertiary referral center were used. About 60% of patients in this study had microcarcinomas, and this might cause selection bias. The rate of false-positive suspicious findings from neck US examination during follow-up could not be assessed. Furthermore, there were only four follicular thyroid carcinoma (FTC) patients in this study, and more studies are needed to evaluate the appropriate follow-up of FTC patients. However, this study has advantages with regard to the long-term follow-up duration and the large cohort of patients.
Based on the results of this study, it is possible to suggest an appropriate follow-up strategy for DTC patients who had an excellent response to initial therapy. For patients with a confirmed excellent response after the initial therapy, regular follow-up of thyroid function to tailor TSH levels might be sufficient for the first five years after surgery. During this early period, neck US at an interval of >18 months might be helpful for the early detection of a recurrence, while regular measurements of serum Tg and TgAb levels may not be cost-effective. After five years following surgery, long-term regular follow-up of serum Tg and TgAb levels and neck US are needed, but the frequency and timing should be individualized (Fig. 2). Further studies are needed to confirm the validity of this proposed strategy.
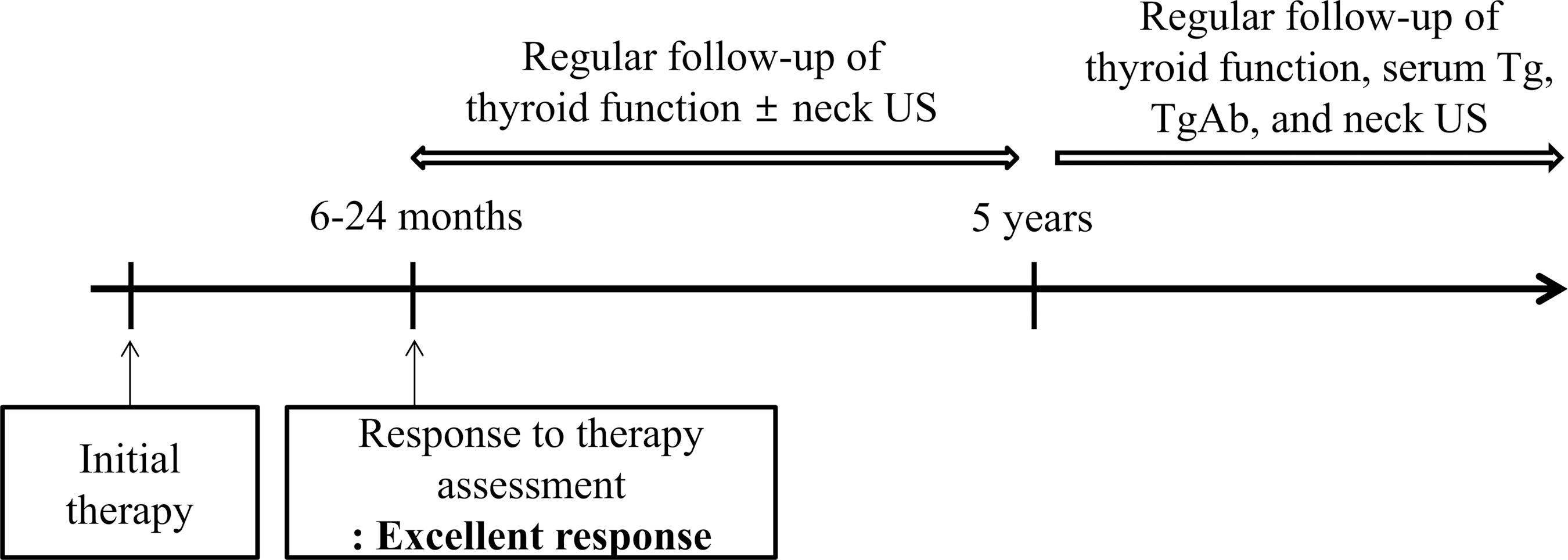
A schematic diagram of a suggested follow-up protocol for patients who were confirmed to have an excellent response to initial therapy.
In conclusion, DTC patients with an excellent response to initial therapy have excellent clinical outcomes with a low recurrence rate. Particularly, the recurrences were detected late at a median of 5.5 years after initial therapy. Regular, frequent follow-up of serum Tg, TgAb, and neck US within five years of surgery may not be necessary. However, long-term regular follow-up of patients with individualized interval and intensity is needed.
Footnotes
Acknowledgments
This study was supported by a grant of the Korean Health Technology R&D project, Ministry of Health & Welfare, Republic of Korea (HC15C3372). The Journal acknowledges that author retains the right to provide an electronic copy of the final peer-reviewed manuscript to Korea PubMed Central (PMC) upon acceptance for publication, and make it publicly available as soon as possible but no later than 12 months after publication.
Author Disclosure Statement
The authors have nothing to disclose.