
Abstract
Background:
Total thyroidectomy and cervical lymph node (LN) dissection is generally recommended in patients with medullary thyroid carcinoma (MTC). However, there is no clear evidence for whom to perform prophylactic lateral neck dissection in MTC patients without evident lateral cervical lymph node (LCLN) metastasis in preoperative images. This study evaluated the preoperative features for predicting the LCLN metastasis of MTC.
Methods:
The study included 26 MTC patients with LCLN metastasis at initial surgery (N1b group) and 47 MTC patients without any LN metastasis or recurrence of disease (N0-NED group). The association between LCLN metastasis and preoperative clinical and sonographic characteristics (size, location, solid component, shape, margin, echogenicity, calcification, and subcapsular location of the tumor) were evaluated.
Results:
There were no significant differences in age and sex between the N1b and N0-NED groups. Preoperative serum levels of calcitonin >65 pg/mL were associated with LCLN metastasis (p < 0.001). In preoperative neck ultrasonography (US), patients in the N1b group were more commonly found with a larger tumor (>1.5 cm) of irregular shape with a spiculated margin and a subcapsular location than those in the N0-NED group (p = 0.029, p < 0.001, p < 0.001, and p < 0.001, respectively). Increases in the number of these LCLN metastasis-related features were significantly associated with higher risk for LCLN metastasis (p < 0.001). The presence of two or more predictors was an appropriate cutoff point for predicting LCLN metastasis of MTC with 73.1% sensitivity and 91.5% specificity.
Conclusions:
MTC tumors with high preoperative calcitonin levels (>65 pg/mL), larger size (>1.5 cm), irregular shape, spiculated margins, and subcapsular locations in the neck US are at higher risk for LCLN metastasis. MTC patents with fewer than two predictors might be suitable for treatment without prophylactic LCLN dissection.
Introduction
A
The mainstay treatment of MTC is complete surgical removal of all neoplastic tissue due to the marginal effectiveness of other therapeutic options such as radioactive iodine treatment and chemotherapy (1,8). Most guidelines recommend a total thyroidectomy (TT) with bilateral central neck dissection (CND) for MTCs confined to the thyroid gland that have no evidence of cervical metastasis on an ultrasonography (US) examination and no evidence of distant metastasis (1,4,9). However, the effectiveness of prophylactic lateral LN dissection in clinically LN-negative MTC patients is unclear and still controversial. This makes it difficult for clinicians to decide for whom to perform prophylactic lateral LN dissection. Therefore, it is important to identify preoperative predictors for lateral cervical LN (LCLN) metastasis of MTC.
Preoperative imaging plays an important role in the diagnosis and staging of MTC. Previous studies reported that the US features of MTC are different from those of PTC (10 –12), and malignant-looking MTCs may be associated with a poor prognosis (13,14). It was expected that US findings would be related to the natural properties of MTC, and an attempt was made to find an association between preoperative US findings and LCLN metastasis.
The current analyses evaluated preoperative suspicious features, including US findings on MTC, for predicting LCLN metastasis. A prediction model was also created to optimize decisions on the extent of surgery to balance risks and benefits in MTC patients.
Materials and Methods
Study design and patients
The study protocol was approved by the Institutional Review Board of the Asan Medical Center. This retrospective cohort study investigated the preoperative clinical and US features for predicting LCLN metastasis in sporadic MTC patients. To identify these features, preoperative clinical and US characteristics were compared between an N1b group, which included MTC patients with LCLN metastasis at initial thyroid surgery, and an N0-NED group, which included MTC patients with undetectable calcitonin (Ctn) within the reference range and without any LN metastasis or recurrence during the median 6.2 years (interquartile range [IQR] 4.6–8.9 years) of follow-up after initial treatment. The management and follow-up protocol for MTC patients was shared at the center in order to maintain consistent treatment and follow-up across the patient populations. All patients were administered levothyroxine and were regularly followed-up with physical examination and a thyroid function test. The postoperative serum Ctn were measured every 6–12 months, and neck US was performed during the first 6–12 months after initial therapy and repeated thereafter at 12-to 24-month intervals (15).
Initially, 123 patients aged >18 years who underwent initial TT with bilateral CND for treatment of sporadic MTC between 1995 and 2013 at the Asan Medical Center, Seoul, Korea, were screened. Sporadic MTC was defined as patients who were confirmed as negative in germline mutational analysis of RET gene (59 patients) or who did not have any family history of multiple endocrine neoplasia (MEN) 2 and did not show any clinical features of MEN2 during follow-up periods (64 patients) (1,16). Only participants with available preoperative US and adequate follow-up were included in the present analysis. Nineteen patients in this initial cohort with pathological N1a disease were excluded from the study. Three patients with initial N0 disease who experienced recurrence after initial treatment were also excluded. In addition, patients who did not have sufficient clinical and US data were excluded. A final cohort of 73 patients was enrolled. All patients underwent TT with bilateral CND, and 54 (74%) patients underwent modified radical neck dissection during the initial surgery. Among the study subjects, 47 (64.4%) patients were placed in the N0-NED group, and 26 (35.6%) patients were placed in the N1b group (Supplementary Fig. S1; Supplementary Data are available online at
Serum Ctn measurements and cutoff value
Serum Ctn was measured by immunoradiometric assay-human calcitonin (IRMA-hCT; CisBio International, Codolet, France), with a functional sensitivity of 1.2 mol/L, detection limit of 0.4 pmol/L, and reference upper limit of 2.9 pmol/L. The intra-assay coefficient of variation of the serum Ctn assay was 1.2–6.7%, and the inter-assay coefficient of variation was 4.3–5.2%. The cutoff value of 65 pg/mL (19 pmol/L) of Ctn was established based on a previous study conducted from the same institution (17).
Neck US examination and diagnosis of MTC
Images of the thyroid gland and neck area were obtained by US using either an iU22 unit (Philips Healthcare, Bothell, WA) or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear high-frequency probe (5–14 MHz), as previously reported (14,18). All thyroid nodules in the US images were evaluated using both transverse and longitudinal planes. Neck US examinations were performed by radiologists under the supervision of two experienced thyroid radiologists (J.H.L. with 12 years' and J.H.B. with 20 years' experience) and retrospectively reviewed by two experienced radiologists (J.H.L. and J.H.B.).
Diagnosis was made by US-guided fine-needle aspiration or core-needle biopsy, according to recommendations (19). US findings, including the size, location, solid component, shape, margin, echogenicity, calcifications, and subcapsular location of the tumor, were evaluated, as previously reported (14,20). Tumor size was defined as the maximum diameter of the MTC on US images. In patients with multifocal MTCs, the dimensions of the largest MTC lesion were used. Tumor location was defined as the upper, mid, or lower third of the thyroid lobe along its long axis, or the isthmus between the lateral margins of the trachea in both transverse and longitudinal images. A pure solid component was defined as a tumor that contains >90% of the solid portion. The shape of the nodule was defined as having an ovoid to round or irregular shape. The margin was defined as smooth, spiculated, or ill-defined. Echogenicity was defined as marked hypoechogenic, hypoechogenic, or other echogenic. The reference echogenicity was that of the thyroid tissue, and the reference echogenicity termed “marked echogenic” was that of the strap muscle. The presence of calcifications was evaluated. When a nodule abutted to the thyroid capsule without any intervening thyroid parenchyma, it was identified as a subcapsular location (14,21 –24).
Statistical analysis
R studio v3.0 and R libraries (R Foundation for Statistical Computing, Vienna, Austria;
Results
Clinical and sonographic characteristics of the study subjects
The median age of the 73 study patients was 51.0 years (IQR 42.0–62.0 years), and 27 (37%) patients were male. The median preoperative serum Ctn level was 297 pg/mL (IQR 48.3–1121.0 pg/mL), and the median tumor size of the MTCs determined by neck US was 1.31 cm (IQR 0.9–2.8 cm). The baseline characteristics of the patients in each group are presented in Table 1. The median age of N0-NED group and N1b group was 53 years (IQR 42.7–63.5 years) and 47.6 years (IQR 42.5–52.2 years), respectively (p = 0.462). There were no significant differences in age or sex between the groups. The preoperative serum levels of Ctn were significantly higher in the N1b group (median 1100 pg/mL) than in the N0-NED group (median 97.9 pg/mL; p < 0.001), and were >65 pg/mL in 96.2% patients of N1b group and 57.4% patients of N0-NED group (p < 0.001). In ROC analysis, the optimal cutoff tumor size in US between the two groups was 1.56 cm (area under the curve [AUC] 0.644, confidence interval (CI) 0.532–0.810). There were significantly more patients with larger MTCs (>1.5 cm) in the N1b group than in the N0-NED group (p = 0.029).
Fisher's exact test.
Others include predominantly solid, predominantly cystic, and cystic nodule on the neck US.
N0 NED group, patients without any lymph node metastasis or persistent of disease for at least 3 years of follow-up after initial treatment; N1bgroup, patients with lateral cervical lymph node metastasis at initial thyroid surgery; US, ultrasonography.
The preoperative sonographic features of MTCs are also described in Table 1. The kappa values for the intra- and inter-observer agreements of each US feature ranged from 0.81 to 0.97. An irregular tumor shape was more common in the N1b group (61.5%) than in the N0-NED group (14.9%; p < 0.001). Spiculated margins and subcapsular locations of tumors were also significantly more common in the N1b group (p < 0.001 and p < 0.001, respectively). There were no significant differences in the location of the tumor, solid component, echogenicity, or the presence of calcification between the groups.
Preoperative suspicious features of LCLN metastasis of MTC
To define the predictors of LCLN metastasis of MTC, binary logistic regression analyses we performed with preoperative clinical and US features (Table 2). Preoperative serum Ctn levels of >65 pg/mL were significant predictors of LCLN metastasis (odds ratio [OR] = 18.52 [CI 3.46–344.51]; p = 0.006). In the preoperative US analysis, a tumor size >1.5 cm, an irregular shape, a spiculated margin, and a subcapsular location of the tumor were significantly associated with LCLN metastasis in MTC.
OR, odds ratio; CI, confidence interval.
Number of preoperative suspicious features and risk of LCLN metastasis of MTC
The number of these five preoperative suspicious features (preoperative serum Ctn level, primary tumor size, irregular shape, spiculated margin, and subcapsular location of tumor) for predicting LCLN metastasis of MTC was evaluated. The distributions of each preoperative suspicious feature in each group are shown in Figure 1A. In the N0-NED group, most patients (91.5%) had two of fewer preoperative suspicious features, and it is left shifted. On the other hand, most of the patients (96.2%) in the N1b group had two or more preoperative suspicious features, and it is right shifted. The number of suspicious features was significantly different between the two groups (p < 0.001).
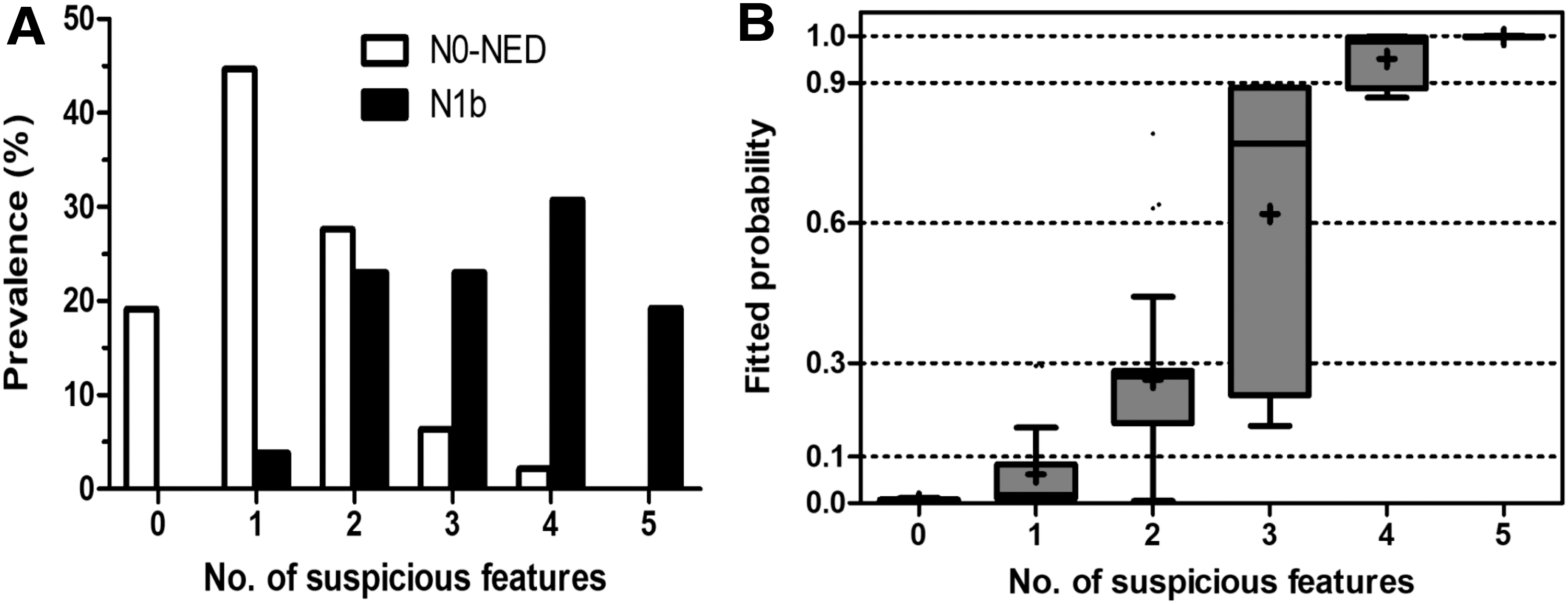
Probability of lateral cervical lymph node (LCLN) metastasis of medullary thyroid carcinoma (MTC) according to the number of suspicious features increase. (
The mean fitted probability score for LCLN metastasis was 0.004 for MTCs without any of these suspicious features, 0.062 for MTCs with one of these suspicious features, 0.264 for MTCs with two of these suspicious features, 0.619 for MTCs with three of these suspicious features, 0.951 for MTCs with four of these suspicious features, and 0.998 for MTCs with all of these suspicious features (p < 0.001; Fig. 1B).
Optimal number of preoperative predictors for predicting LCLN metastasis
According to ROC curve analysis, the optimal number of preoperative predictors for LCLN metastasis was two (AUC 0.905 [CI 0.839–0.972]). MTCs with two or more preoperative predictors were at high risk for LCLN metastasis. The sensitivity and specificity of the model were 73.1% and 91.5%, respectively. In logistic regression analyses, the OR for the LCLN of MTCs with two or more preoperative predictors was 36.8 ([CI 6.9–686.1]; p = 0.001).
Preoperative predictors in N0-NED group patients with preoperative high Ctn levels (>65 pg/mL)
There were 27 (57.4%) patients who had high preoperative Ctn levels of >65 pg/mL in the N0-NED group. The preoperative suspicious features of these patients are given in Table 3. Among these cases, 18 (66.7%) patients underwent LCLN dissection. The median fitted probability score for this N0-NED group with high Ctn levels (>65 pg/mL) was 0.171 (IQR 0.024–0.271). In the analysis of the five preoperative predictors, 10 (37.0%) patients only had one feature (preoperative Ctn >65 pg/mL) without any other predictors.
Interquartile ranges.
CND, central neck dissection; MRND, modified radical neck dissection.
Discussion
This study is the first to evaluate both preoperative clinical and US features for predicting LCLN metastasis in sporadic MTC patients. Five suspicious features significantly associated with LCLN metastasis of sporadic MTCs were identified: high preoperative Ctn levels (>65 pg/mL) and a larger tumor size (>1.5 cm), irregular shape, spiculated margin, and subcapsular location in neck US. As the number of these predictors increased, the possibility of LCLN metastasis of the MTC also significantly increased. A prediction model has also been proposed, using a number of these predictors. MTCs with two or more predictors had significantly greater risk for LCLN metastases. However, MTCs with fewer than two predictors had little possibility of LCLN metastasis, and prophylactic lateral LN dissection should not be considered without definite evidence.
There are no clear and evident recommendations for deciding the extent of LN dissection in MTC patients with no clinical evidence of LCLN metastasis in preoperative images. Some studies have attempted to evaluate the clinical factors predicting LCLN metastasis of MTC (26 –28). Age, sex, and preoperative Ctn levels were also evaluated as possible predictors. Previous studies have suggested that old age is associated with a poor prognosis in MTC patients and that women have a better prognosis than men (5,29). However, in the current series, age and sex were not found to be associated with LCLN metastasis in MTC. Higher preoperative Ctn levels were considered a strong marker for predicting LCLN metastasis of MTC in the present analyses. This result is consistent with many previous studies that have reported that a high preoperative Ctn level is associated with the extent of LN metastasis and poor clinical outcomes in MTC (1,26,30).
The preoperative US features of MTCs were evaluated, and their clinical significance for predicting LCLN was analyzed. A larger tumor size on a preoperative US image was considered another predictive factor for LCLN metastasis in MTC. This finding is also consistent with previous studies that have found that larger tumor size is associated with poor clinical outcomes (14,28,30). In the current study, ROC curve analysis determined that 1.5 cm was an appropriate tumor size cutoff for predicting LCLN metastasis. Other sonographic characteristics of MTCs were also evaluated. Previously, the US features of MTC have been reported to be malignant-looking MTCs and benign-looking MTCs (13,14). Malignant-looking MTCs are associated with poor clinical outcomes. This study focused on the predictive US features of LCLN metastasis, and it was found that tumors with an irregular shape and ill-defined margin were significantly associated with LCLN metastasis. The majority of the tumors in the N0-NED group were oval and round (85.1%) and had a smooth margin (55.3%). These findings suggest that differences in the US findings of MTCs may reflect different pathological properties of MTCs.
The presence of extrathyroidal extension (ETE) in MTC is considered a risk factor for aggressive behavior and cervical LN metastasis (29 –31). This study focused on the preoperative features of MTCs and did not evaluate the association between ETE and the risk of LCLN metastasis. However, a subcapsular tumor location, defined as a thyroid nodule abutting the thyroid capsule without intervening thyroid parenchyma, could be a useful preoperative US feature for predicting ETE in pathological reports (32). It was determined that a subcapsular location in preoperative US was significantly associated with LCLN metastasis of MTC. This finding suggests the importance of careful US examination to determine the subcapsular location of MTCs because of its usefulness in predicting ETE and LCLN metastasis.
In the present analysis, the probability of LCLN metastasis increased as the number of suspicious features increased. This indicates that the five preoperative predictors may help to estimate the extent of LN metastasis. When an MTC had one or no positive predictor, the possibility of LCLN metastasis was very low (OR = 0.03 [CI 0.001–0.145]). This indicates that MTC with fewer than one predictor might be appropriate for treatment without prophylactic LCLN dissection. In the American Thyroid Association guidelines, prophylactic LCLN dissection based on the Ctn level is suggested with a Grade I recommendation (recommends neither for nor against it) (1). In the present study, about half of the N0-NED group had high preoperative Ctn levels (>65 pg/mL), although they did not have cervical LN metastasis or recurrence (Table 3). Although their mean fitted probability for LCLN metastasis was only 0.171 in the present model, 66.7% of these patients underwent LCLN dissection. When the five preoperative predictors were evaluated in each patient, 37% of patients had only one positive predictor (high preoperative Ctn level >65 pg/mL). This finding indicates that about 40% of MTC patients could avoid unnecessary prophylactic LCLN dissection if the prediction model is used.
From the initial study cohort, three patients who had recurrent MTC after initial treatment were excluded. These patients initially underwent TT with bilateral CND. When the prediction model was applied, all of these cases would have been candidates for LCLN dissection because they had three or four preoperative predictors. These findings support the usefulness of this model in determining the extent of LN dissection in MTC patients. The mean tumor size of the study subjects was relatively small compared to previous studies (27,33). This might be due to the inclusion criteria resulting in two thirds of patients in the N0-NED group. The mean tumor size of all MTC patients in a previous study was 2.2 ± 1.8 cm (15).
This study has some notable limitations, including those inherent to its retrospective design. It was a single-center historical cohort study, and a relatively small number of patients were included. Therefore, there is a possibility of selection bias, and further studies are necessary to validate the findings in a larger cohort. There is also a potential limitation in defining sonographic characteristics retrospectively because it is a dynamic examination. An attempt was made to apply the general criteria that are commonly used in the description of thyroid nodules on US, and relatively objective criteria were used to determine the sonographic features predicting LCLN metastasis.
Notwithstanding these limitations, the main strength of this study is that only preoperative features were evaluated that would be useful for clinicians in order to decide on whom to perform prophylactic LCLN dissection among patients with clinical N0 MTCs. To the best of the authors' knowledge, this is the first study to evaluate suspicious US features associated with LCLN metastasis of MTC and proposing a prediction model.
In conclusion, high preoperative Ctn levels (>65 pg/mL) and a larger tumor size (>1.5 cm), irregular shape, spiculated margin, and subcapsular location of the tumor in preoperative neck US are significantly associated with LCLN metastases of MTCs. MTCs with two or more predictors are at higher risk for LCLN metastases. MTCs with fewer than two predictors have a very low probability of LCLN metastasis and might be suitable for treatment without prophylactic lateral LN dissection.
Footnotes
Acknowledgments
This study was supported by a Research Grant (NRF-2015R1C1A1A02036597) from the National Research Foundation of Korea.
Author Disclosure Statement
No competing financial interests exist.