
Abstract
Background:
The American Joint Committee on Cancer Cancer Staging System for differentiated thyroid cancer has been recently revised. The purpose of this study was to compare survival prognostication between the seventh and eighth editions.
Materials and Methods:
We retrospectively reviewed 2579 differentiated thyroid cancer patients who underwent surgery at MD Anderson Cancer Center between 2000 and 2015. Disease-specific survival (DSS) and overall survival were estimated using the Kaplan–Meier method and compared using log rank test. The effect of potential predictor was estimated using Cox proportional hazards model. Power of survival prediction was estimated using Harrell's C concordance index (C-index), and predictive capacities for DSS were estimated using proportion of variance explained (PVE).
Results:
Revision of tumor-node-metastasis (TNM) categories, age cutoff, and stage reassignment in the 8th edition caused reclassification of overall stage compared with the seventh edition. The proportion of patients in stage I and II increased from 62% to 83% and 5% to 12%, respectively, while the proportion of patients in stage III and IV decreased from 20% to 2% and 14% to 3%, respectively. Ten-year DSS for stages I–IV based on the seventh edition were 100%, 97.5%, 98.3%, and 82.6%, respectively, while 10-year DSS for the corresponding stage in the eighth edition were 99.8%, 88.3%, 72.4%, and 71.9%, respectively. In multivariate analysis for both seventh edition (C-index 0.94, PVE 4.6%) and eighth edition (C-index 0.94, PVE 4.8%), the factors predictive of worse outcome for DSS were older age, advanced tumor size category, and distant metastasis while cervical lymph node metastases did not predict worse survival. For the eighth edition, patients <55 years of age with stage II disease had significantly worse DSS (p < 0.001) than patients ≥55 years with stage II disease but appeared to be similar to patients ≥55 years with stage III (p = 0.742) and IV disease (p = 0.566). Patients ≥55 years old with T3a and T3b disease had 10-year DSS of 67% and 92%, respectively (p = 0.390).
Conclusion:
The AJCC eighth edition is similar to the seventh edition in disease-specific survival prediction. Potential modifications that may improve disease-specific survival prediction in future renditions include reconsideration of T3b tumor category and upstaging classification of patients <55 years of age with distant metastases.
Introduction
T
Materials and Methods
After the approval by the institutional review board, a retrospective review of consecutive patients ≥18 years of age with differentiated thyroid cancer who underwent primary surgery between 2000 and 2015 at The University of Texas MD Anderson Cancer Center was conducted. Patients with focal area(s) of poorly differentiated tumor in the primary or lymph nodes were included, but patients with significant poorly differentiated component, or any patient with anaplastic thyroid carcinoma, were excluded. A total of 2579 consecutive patients were identified. Demographics, tumor and treatment characteristics, and follow-up and vital status were collected. Disease-specific survival (DSS) was calculated from the time of surgery to death from thyroid cancer, and overall survival (OS) was defined from the time of surgery to death from any cause. For DSS, patients were censored at the date of last follow-up or date of death from causes other than thyroid cancer, while patients were censored at the date of last follow-up for OS. Patients were staged according to the seventh (2) and eighth (1) editions of the AJCC Cancer Staging System.
Continuous variables are reported as mean (standard deviation) or median (range), and categorical variables were reported as frequencies and proportions. Survival was estimated using the Kaplan–Meier method and was compared using a log-rank test between groups of patients of interest. The effects of potential predictors of DSS were modeled by Cox proportional hazards regression and reported as hazard ratios (HRs) with 95% confident intervals [Cis]. The Harrell's concordance index (C-index) (3), a method to estimate probability of concordance between expected and observed outcomes, was used to assess the predictive power of DSS for the AJCC staging system seventh and eighth editions using stage determinant variables (age, T, N, and metastasis (M) categories) from multivariate analysis. The proportion of variance explained (PVE) (4) was used to estimate predictive capacity of both staging systems. Specifically, PVE was calculated as 1 − e−(LRT/n), where LRT is the likelihood ratio test statistic. A two-sided p-value less than 0.05 was considered statistically significant. All statistical calculations were performed with SPSS statistics software (IBM Corp. version 24.0. Armonk, NY) and Stata/MP software (version 15.0 College Station, TX).
Results
Clinicopathological characteristics are delineated in Table 1. The patient cohort is described according to T and N classification criteria in Supplementary Table S1 (Supplementary Data are available online at
Both papillary and follicular cell carcinoma.
Effect of T category on survival
Revision of the T category criteria resulted in reclassification of much of the T3 category to T1 and T2 categories due to the removal of minimal extrathyroidal extension to the perithyroidal tissue as a criterion for T3 disease. The proportion of patients with T3 tumors decreased from 41% in the seventh edition to 11% in the eighth edition, while the proportion of those with T1 and T2 increased from 43% to 65% and 11% to 20%, respectively. DSS were significantly different between stages for both editions (p < 0.001), with 10-year DSS for T1 to T4 according to the seventh edition 99.9%, 98.7%, 96.6%, and 70.2%, respectively, and 10-year DSS for T1–T4 based on the eighth edition 99.9%, 97.4%, 92.7%, and 70.2%, respectively (Fig. 1).
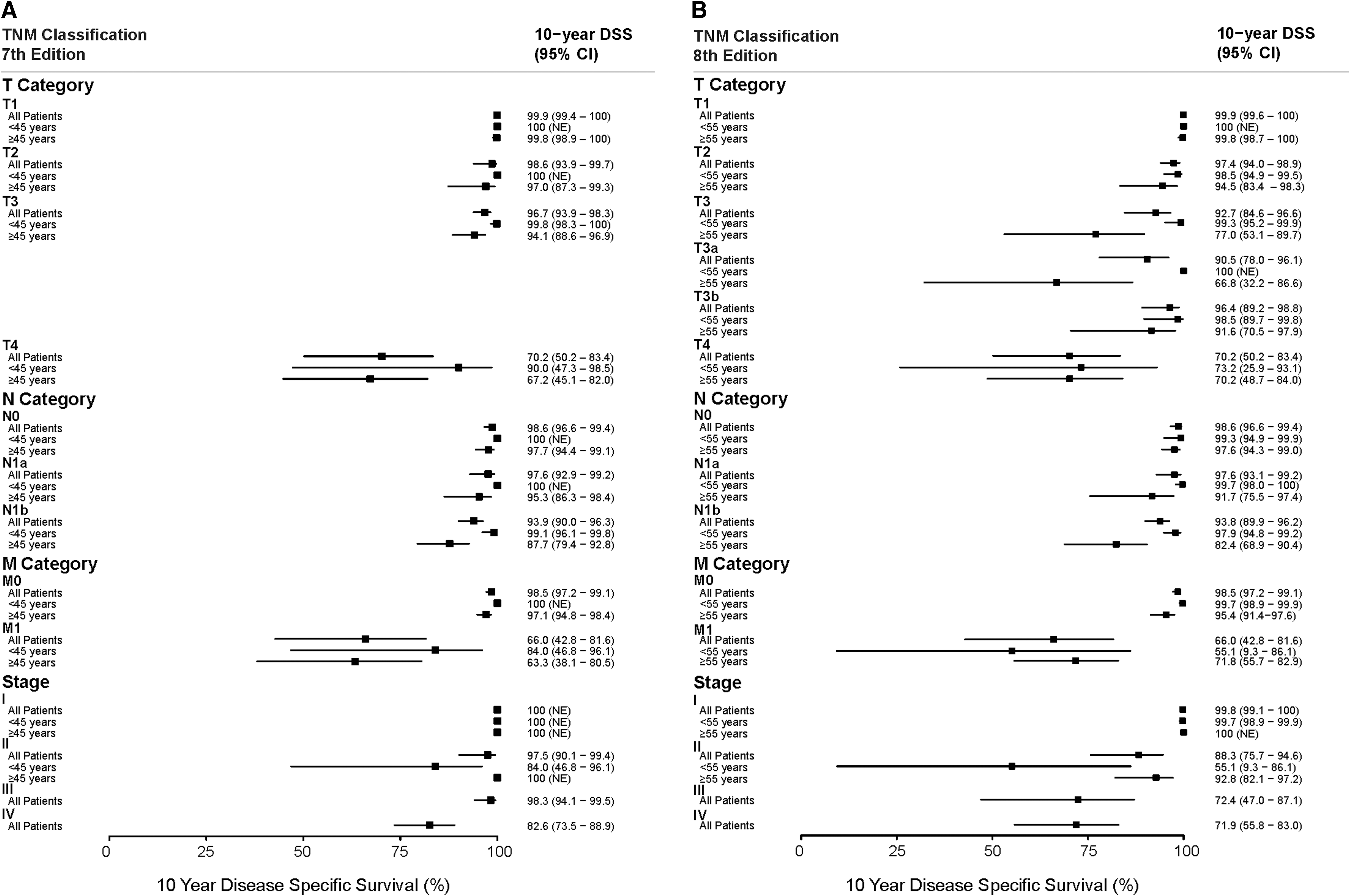
Forest plot of 10-year disease-specific survival for 2579 consecutive surgical patients with differentiated thyroid cancer according to American Joint Committee on Cancer (AJCC) Staging seventh (
Increasing T category predicted worse DSS for both editions. However, based on the seventh edition, the hazard of cancer-related death between T1 and T2 were not significantly different in both univariate analysis (HR 7.86 [%CI 0.71–86.72], p = 0.092) and multivariate analysis (HR 6.90 [CI 0.62–76.63], p = 0.116), while the hazards were significantly different in the eighth edition in both univariate analysis (HR 11.0 [CI 2.28–52.96], p = 0.003) and multivariate analysis (HR 8.35 [CI 1.71–40.80], p = 0.009) (Tables 2 and 3).
Harrell ' s C-index, 0.94; proportion of variance explained, 4.6%.
CI, confidence interval; HR, hazard ratio.
Harrell's C-index, 0.94, proportion of variance explained, 4.8%.
Based on the eighth edition, only 278 patients were categorized as T3. Of those, 172 patients (62%) had tumor size larger than 4 cm (T3a), and 121 patients (44%) had tumor invasion into strap muscle (T3b). For patients with T3b, only 15 patients (13%) had tumor size larger than 4 cm, whereas 54 patients (45%) had tumor size ≤2 cm, and 51 patients (42%) had tumor size 2–4 cm. Overall, there was no significant difference in DSS between patients with T3a and T3b (p = 0.623), with 10-year DSS for patients with T3a and T3b category 91% and 96%, respectively. In the subgroup of patients ≥55 years, 10-year DSS for patients with T3a and T3b were 67% and 92%, respectively (Fig. 2), but there was no statistically significant difference in DSS between T3a and T3b (p = 0.390), or between T2 and T3b (p = 0.358).
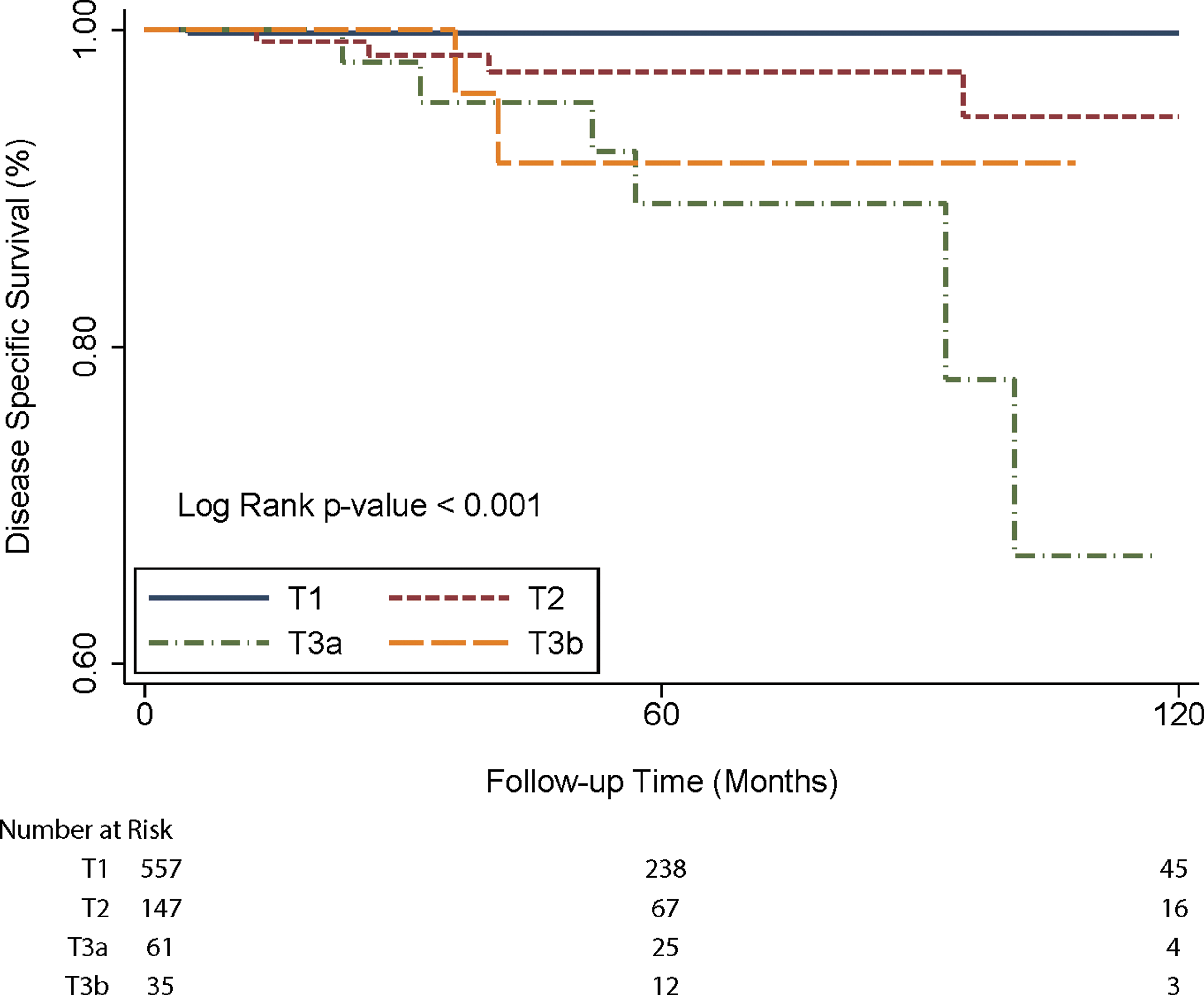
Kaplan–Meier survival plot illustrates disease specific survival of ≥55 year old patients according to the AJCC eighth edition T1–3 categories. Color images available online at
Effect of N category on survival
Only 11 patients (2%) with N1b category according to the seventh edition were downstaged to N1a category according to the eighth edition, based on level VII lymph node metastasis without lateral cervical lymph node metastasis. Ten-year DSS for patients with N0, N1a, and N1b based on the seventh (98.6%, 97.6%, and 93.9%) and eighth (98.6%, 97.6%, and 93.8%) edition N classification were statistically similar (Fig. 1). In univariate analysis using both the seventh and eighth editions, patients with N1a had comparable DSS with N0 category, whereas patients with N1b had significantly worse DSS compared with N0 category. However, N1b category was not considered to be an independent predictive factor for DSS in multivariate analysis using both editions (Tables 2 and 3).
Effect of changing age cutoff point on survival
Increasing age was associated with increasing risk of cancer-related death. With an age cutoff at 45 years in the seventh edition, DSS was worse in patients ≥45 years (p = 0.001), with 10-year DSS for patients <45 years and ≥45 years as 99.7% and 95.1%, respectively. After multivariate adjustment for sex, T category, N category, and M category based on the eighth edition TNM staging criteria, the hazard of cancer-related death in patients ≥45 year were higher compared with those <45 years (HR 8.29 [CI 1.94–35.40] p = 0.004). In the eighth edition, the age cutoff point has changed to 55 years. Consequently, 581 patients (34%) from the older age group were changed to the younger age group. This age cutoff remained significantly associated with DSS (p < 0.001). Ten-year DSS for patients <55 years and ≥55 years were 99% and 93%, respectively. After multivariate adjustment for sex, T category, N category, and M category based on the eighth TNM staging criteria, the hazard of cancer-related death in the older age group remained higher compared with the younger age group (HR 4.08 [CI 1.70–9.81], p = 0.002).
To investigate the specific age group of patients who were downstaged in the eighth edition, we analyzed survival of patients 45–54 years and compared with patients <45 years and ≥55 years. Ten-year DSS of the 45- to 54-year age group was 97.6%. The hazard of cancer-related death for this group were higher than those of patients <45 years, but the HR between the <45 and 45- to 54-year age group did not reach statistical significance in either univariate (HR 0.21 [CI 0.04–1.10], p = 0.065) or multivariate analyses (HR 0.19 [CI 0.04–1.02], p = 0.052). When comparing patients 45–54 years with those ≥55 years, the hazards were significantly different in univariate analysis (HR 3.97 [CI 1.51–10.16], p = 0.005); however, the difference was not significant in multivariate analysis (HR 1.89 [CI 0.70–5.12], p = 0.211).
Effect of modification of age cutoff, TNM criteria, and overall stage reassignment on survival
Revision of T and N classification, modification of age cutoff, and overall stage reassignment caused reclassification of overall stage. The proportion of patients with stage I and II in the eighth edition compared with the seventh edition increased from 62% to 83% and 5% to 12%, respectively, while the proportion of patients in stage III and IV decreased from 20% to 2% and 14% to 3%, respectively (Fig. 3A and B). As a result of these changes, 99 patients (85%) in stage II were moved to stage I, and all of stage III patients were downstaged to stage I (68%) or stage II (32%). For seventh edition stage IV patients, approximately 80% were downstaged: 96 patients (27%) to stage I, 138 patients (39%) to stage II, and 56 patients (16%) to stage III.
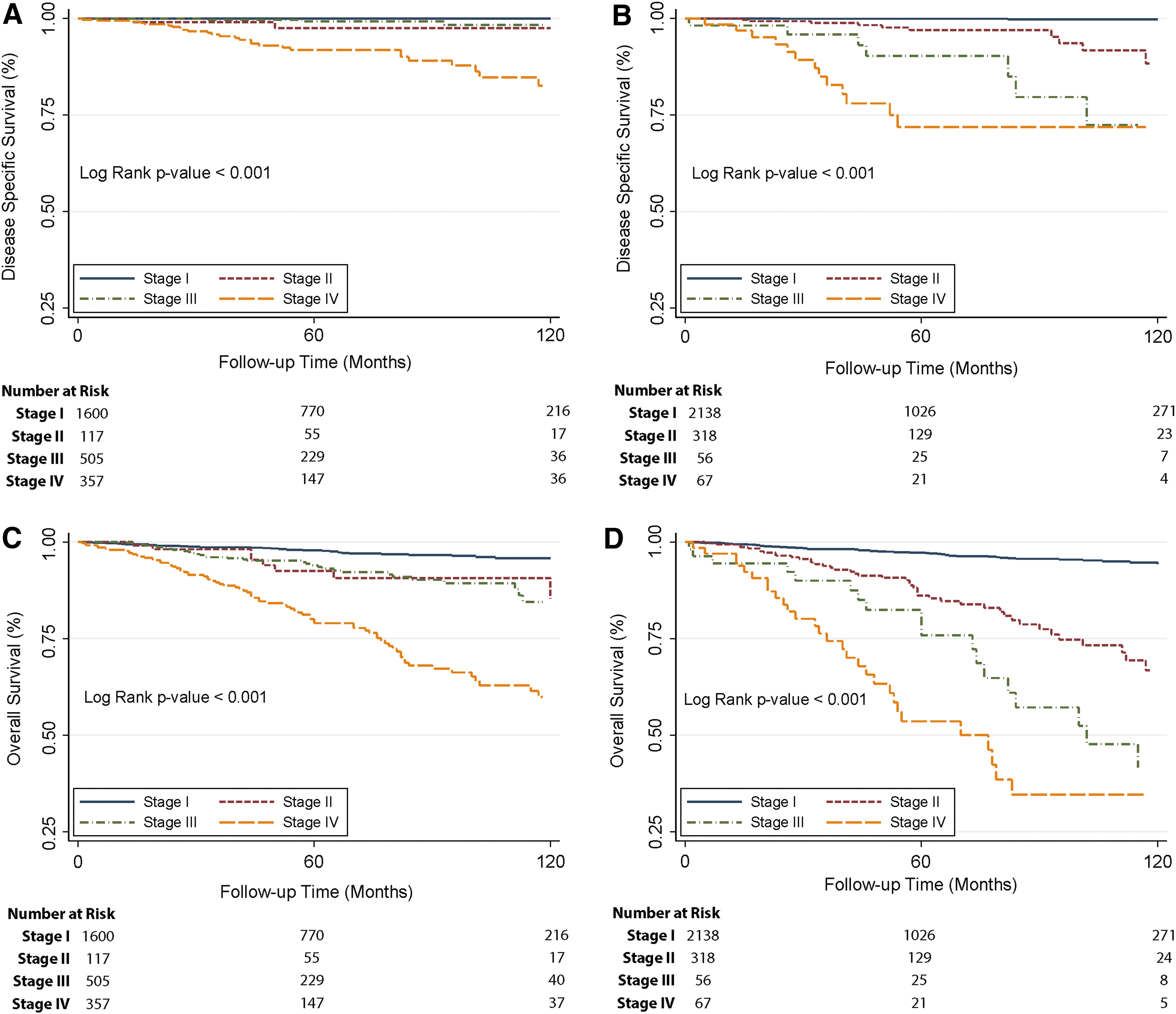
Kaplan–Meier survival plots illustrate disease specific survival for 2579 consecutive surgical patients with differentiated thyroid cancer by stage according to the AJCC Staging seventh edition (
Ten-year DSS for stage I-IV for the seventh edition were 100%, 97.5%, 98.3%, and 82.6%, respectively (p < 0.001), while ten-year DSS for the eighth edition were 99.8%, 88.3%, 72.4%, and 71.9%, respectively (p < 0.001) (Figs. 1 and 4). On pairwise comparisons, DSS was not significantly different between stage II and stage III in the seventh edition (p = 0.398), while there was no significant difference between stage III and stage IV in the eighth edition (p = 0.240). All other pairwise comparisons between stages were significantly different in the seventh and eighth editions. The C-indices were 0.94 for both the AJCC staging system seventh and eighth editions, and PVE were 4.7% and 4.9% for the seventh edition and eighth edition, respectively (Tables 2 and 3). Ten-year OS for stages I–IV based on the seventh edition were 95.8%, 90.7%, 84.4%, and 59.7%, respectively (Fig. 3C), while the corresponding 10-year OS for the eighth edition were 94.3%, 66.8%, 40.6%, and 34.6%, respectively (Fig. 3D).
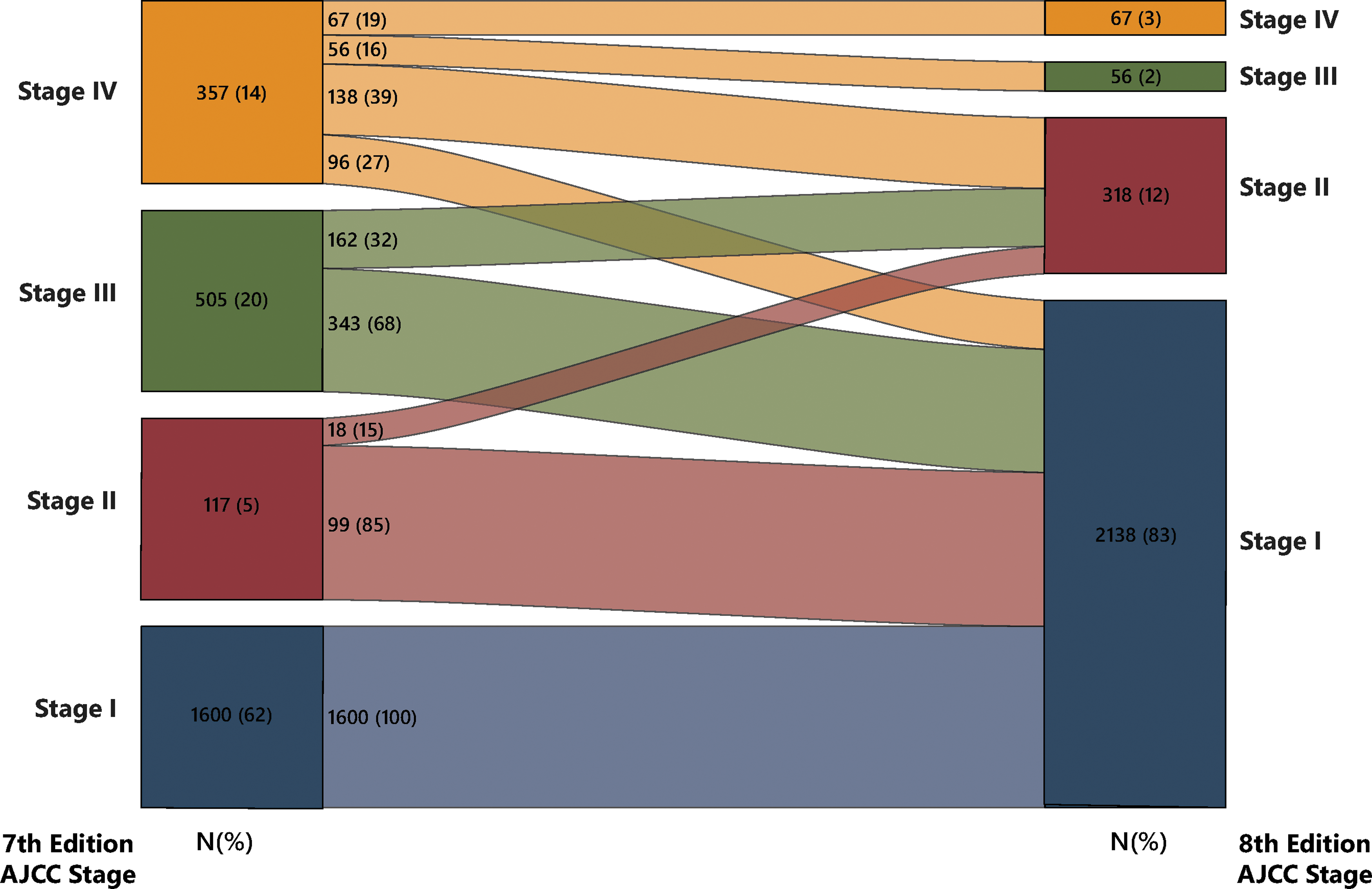
Alluvial diagram of stage reclassification between the AJCC Staging seventh and eighth editions for 2579 consecutive surgical patients with differentiated thyroid cancer. Color images available online at
Survival comparison by TNM stage grouping
In the eighth edition, TNM stage groupings were modified as compared to the seventh edition. To compare survival difference within the same stage, we analyzed and compared DSS based on age group and TNM category combination within each stage (Table 4). Within stage II, patients <55 years with distant metastases had significantly poorer DSS compared with patients with stage II disease ≥55 years of age (p < 0.001). Similarly, by pairwise comparison, patients <55 years with distant metastases had significantly poorer DSS compared to patients ≥55 years with T1N1M0 disease (p < 0.001) and ≥55 years with T2N1M0 disease (p = 0.017), but not significantly different DSS than patients ≥55 years with T3anyNM0 disease (p = 0.077). Figure 5 illustrates DSS based on age group and stage, with patients <55 years with distant metastases (stage II AJCC eighth edition) closely approximating patients ≥55 years with stage III and IV disease, but significantly poorer DSS compared to patients ≥55 years with stage II disease (p < 0.001).
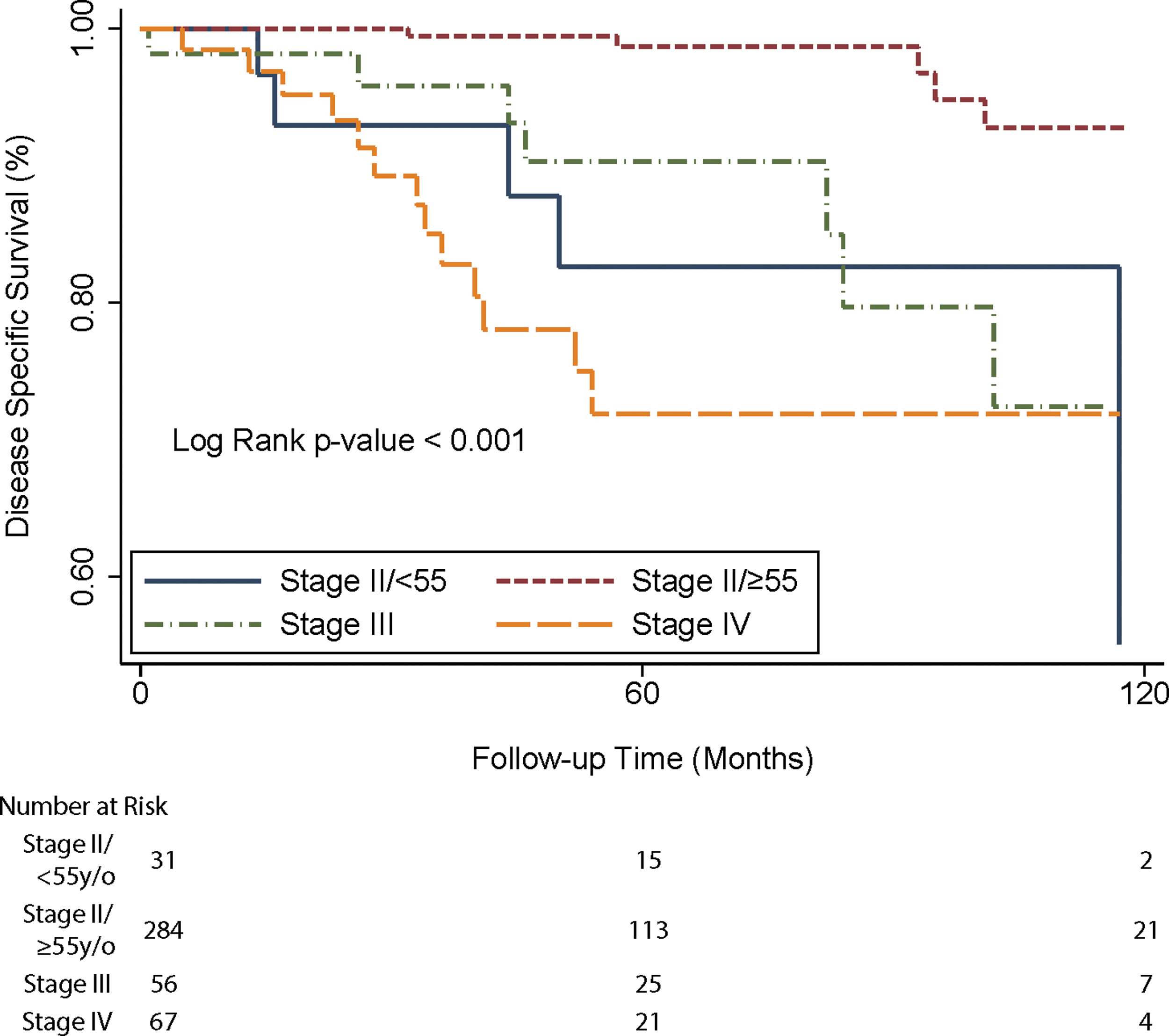
Kaplan-Meier survival plot illustrates disease specific survival for stage II–IV patients with differentiated thyroid cancer according to the AJCC Staging eighth edition, and stratified by age cutoff at 55 years for stage II patients. Color images available online at
Discussion
The purpose of this study was to compare survival prediction between the AJCC Staging seventh and eighth editions for differentiated thyroid cancer among a large contemporary cohort of surgical patients at a single tertiary care institution. The C-index and PVE both indicate the power of survival prediction for DSS of the seventh and the eighth editions as essentially the same, although the 10-year DSS appears more distinguished between stages using the updated eighth edition as compared to the seventh edition.
Based on the seventh edition, tumors with ETE were classified as T3 for extension into perithyroidal soft tissue or strap muscle, while T4 for gross extension to the larynx, trachea, esophagus, or recurrent laryngeal nerve. T4 disease has been consistently demonstrated to result in poorer OS and DSS (5 –10). On the other hand, upstaging according to minimal ETE has been challenged by many authors (9 –13) who have suggested that minimal ETE is not associated with worse survival. Consequently, microscopic perithyroidal soft tissue extension is no longer considered as a factor in T categorization in the eighth edition.
In evaluating T3 patients according to the eighth edition in the current study, T3b (ETE to strap muscle regardless of tumor size) appeared to trend toward better DSS relative to those with T3a (tumor size >4 cm), although this did not reach statistical significance, which may be secondary to the T3b category also including a subset of the larger tumors (13% of T3b patients had >4 cm tumors). In addition, there was no statistical difference between T2 and T3b patients. It is important to emphasize that almost 90% of patients in the current study with T3b category status had ≤4 cm tumors; therefore, it was the impact of strap muscle invasion alone that upstaged them to T3b category from what would otherwise have been T1 or T2 categories. In the seventh edition, both invasion into the strap muscles and microscopic perithyroidal soft tissue extension resulted in tumors of any size to be upgraded to T3 category. In the eighth edition, microscopic perithyroidal extension is no longer included in the T3 category, though gross extrathyroidal extension to the strap muscles remains an upgrading factor to T3 category. From a practical standpoint, since strap muscles can be relatively easily resected en bloc with thyroid tumor at the time of surgery, it is not clear as to why specifically invasion into the strap muscle is considered to be a greater risk than otherwise microscopic perithyroidal soft tissue extension. The effect of ETE into strap muscle on survival demands further investigation, as the data in this study suggests that the inclusion of ETE into strap muscle as a T3b upstaging factor may need to be reconsidered.
Regarding N category, the impact of regional lymph node metastasis on DSS remains controversial. The new eighth edition AJCC staging system downstages patients ≥55 years with N1a or N1b category to overall stage II, whereas, previously, seventh edition N1a category patients were overall stage III, and N1b category patients were overall stage IV. In the current study, N1a status did not predict worse DSS compared with N0, while N1b category had poorer DSS in univariate but not in multivariate analysis. Ito et al. (14) studied 1740 patients with similar findings for pathologic N1b status, while patients with clinical N1b status had poorer DSS. In contrast, Smith et al. (15) studied over 10,000 patients from the Surveillance, Epidemiology, and End Results (SEER) database and discovered that both N1a and N1b category increased risk of cancer-related death for patients ≥45 years old, whereas it did not affect survival in younger patients. Furthermore, Ito et al. (16) have previously suggested that other characteristics such as the size, number, and extranodal extension of metastatic lymph nodes influence DSS.
Age at diagnosis is also an important survival predictor and is integrated into almost all thyroid cancer staging systems. For the seventh edition AJCC staging system, age was applied as a categorical variable with cutoff point at 45 years. However, this concept has been challenged by several authors who considered a cutoff point of 45 years to be too young. For example, Mazurat et al. (17) studied 2115 patients, suggesting an age cutoff of 55 years as a better indicator of cancer-related death risk. Similar findings were reported by Kim et al. (18), who studied 35,323 patients from the SEER database and found that the optimum cutoff point for disease-related death was 57 years. Moreover, Nixon et al. (19) studied 9484 patients across several institutions and determined that increasing the age cutoff to 55 years improved both outcome distribution between stages and prognostic information. Consequently, 55 years now represents the new age cutoff point in the eighth edition AJCC staging system. Incorporating this new age cutoff with the other changes in the eighth edition revealed that the HR of cancer-related death between younger and older age groups decreased to approximately 4, as compared to a HR of 8 with the former age cutoff of 45 years. We found that survival of patients 45–54 years was not statistically significantly different from ≥55 year old patients, or <45 year old patients.
Based on our data, survival discrimination power between the seventh and eighth editions AJCC staging systems as indicated by Harrell's C indices were not different, which suggests that both editions contain the same ability to estimate survival among stages. Our data suggest that the seventh edition may not differentiate well between stage II and III, while the eighth edition may not differentiate well between stage III and stage IV, which may account for the overall similar C index. Recently published reports by Kim et al. (20) and Kim et al. (21) both suggest the eighth edition AJCC staging system to have higher C index compared with the seventh edition, although the difference in C index was small in both studies.
With an optimal staging system, varying T, N, and M category combinations that ultimately correlate with the same overall stage should have similar survival. Based on the AJCC eighth edition, the data in this study indicate that DSS for different TNM combinations in stage I were statistically similar, whereas there was a wide range of survival among stage II TNM groupings. Specifically, patients <55 years with distant metastases had significantly worse DSS relative to other stage II TNM combinations. The staging of younger patients with distant metastasis as stage II has been previously studied. Based on the seventh edition, Lundgren et al. (22) compared survival in stage II patients and reported that there was no survival difference between different TNM combinations in this stage. In contrast, and similar to the data herein, Tran Cao et al. (23) demonstrated that survival of younger patients with M1 disease was worse than other stage II TNM groupings, and thus concluded that these patients may be understaged. The data in the current study would support staging patients <55 years with distant metastases as at least overall stage III, as these patients have similar DSS to stage III and IV ≥55 year old patients.
This is a retrospective study with its inherent limitations. Additionally, there may be institutional bias reflecting patients with more advanced disease according to local and national referral patterns. Population-based cohorts may provide improved external validity but are limited in the granularity of their data and may suffer from coding errors. For example, Pontius et al. (24) reported on differences in staging systems using the SEER database. Though comparisons were able to be made using overall survival, the outcome of interest in the AJCC is disease specific survival and was only able to be compared at 5 years in a select cohort of patients. This study also reported on the outcomes using the National Cancer Database, but overall survival was the only outcome available and this database is a hospital-based cohort which may limit the ability to generalize findings to other populations. In our study, 10-year DSS was able to be reported. However, we acknowledge that given the relatively few events for DSS, some 10-year DSS estimates may not be precise, as reflected in the accompanying confidence intervals. This also limited our ability to compare C-indices and PVEs using overall stage. Finally, this article focuses solely on DSS in consideration of staging, while it is well recognized that disease recurrence represents another important prognostic outcome, particularly for patients with thyroid cancer who typically have more favorable DSS. Nevertheless, this article represents a large single institution study of differentiated thyroid cancer patients comparing power of survival prediction between the AJCC Staging seventh and eighth editions, offering some confirmation of the predictive power of the revised eighth edition but suggesting several potential modifications in future editions.
Conclusion
The AJCC eighth edition is similar to the seventh edition in DSS prediction. Potential modifications that may improve DSS prediction in future renditions include upstaging classification of patients <55 years of age with distant metastases to overall stage III, and removal of strap muscle invasion as a factor in upstaging patients to the T3b tumor category.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.