
Abstract
Background:
It is unknown whether the growth of thyroid nodules with a Bethesda category III cytology (atypia of undetermined significance [AUS]) is predictive of malignancy, especially in cases with architectural atypia (AUS-A). This study evaluated whether tumor growth rates can help distinguish malignant from benign nodules in the AUS-A subcategory.
Methods:
This retrospective, single-center cohort study included 172 patients who underwent diagnostic thyroid surgery because of a nodule with a cytological diagnosis of AUS-A. The growth kinetics of nodules was assessed by serial preoperative neck ultrasonography over a median follow-up of 52.6 months (range 12.7–198.3 months).
Results:
Pathologic examinations showed that 112 (65%) and 60 (35%) patients had benign and malignant nodules, respectively. The largest diameter and volume of both benign and malignant nodules increased gradually (p < 0.001). However, there was no significant difference in the growth rates of benign and malignant nodules based on the largest diameter (p = 0.132) and volume (p = 0.200). The time to tumor growth curves and estimated median time to significant tumor growth from baseline were not significantly different in malignant nodules compared to benign nodules (p = 0.458 and p = 0.568, respectively). The relative risk (RR) of malignancy of growing and stable nodules did not differ significantly based on the largest diameter (RR = 0.5; p = 0.064) and volume (RR = 0.9; p = 0.748).
Conclusions:
The size of thyroid nodules classified as AUS-A increased linearly, regardless whether these nodules were benign or malignant. These results suggest that growth kinetics on serial preoperative neck ultrasonography cannot predict malignancy in the AUS-A subcategory.
Introduction
N
The AUS category combines different alterations, including cases with architectural and/or nuclear atypia insufficient to warrant classification as benign, follicular neoplasm/suspicious for a follicular neoplasm, or suspicious for malignancy (5). In view of this heterogeneity, The 2017 Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) recommends subclassification of the atypia with potential implications for a cytology-based risk of malignancy stratification (5). Several meta-analyses have suggested an impact for subclassification of the AUS category, and nodules classified as AUS with architectural atypia (AUS-A) could be at substantially lower risk for malignancy than those classified as AUS with nuclear atypia (AUS-N) (9,10). In addition, follicular thyroid carcinoma (FTC) is more frequent in the AUS-A subcategory, while the AUS-N subcategory is mainly associated with papillary thyroid carcinoma (PTC), and the diagnosis of PTC is relatively easy because of characteristic sonographic features and FNAC results (11). Therefore, clinical biomarkers that can distinguish malignant from benign nodules within the AUS-A subcategory are helpful in making treatment decisions.
Efforts to improve the management of indeterminate thyroid nodules have focused on identifying clinical characteristics that predict malignancy (12). Although thyroid nodule growth during surveillance has been used to assess the risk of malignancy (4), it is unclear whether growth is a significant predictor of malignancy (13). To the best of the authors' knowledge, there is no report assessing tumor growth for predicting malignancy risk in the AUS-A subcategory.
This study aimed to determine whether the tumor growth rate could distinguish malignant from benign thyroid nodules with AUS-A. The growth kinetics of thyroid nodules based on at least three consecutive US examinations performed over a median follow-up time of 53 months were evaluated, and the growth rates between pathologic proven benign and malignant nodules were compared.
Methods
Patients
This retrospective cohort study included patients who underwent diagnostic thyroid surgery for a thyroid nodule with an AUS-A cytology between January 2014 and November 2017 at the Asan Medical Center, Seoul, Korea. Patients (age ≥18 years) were included if they had at least three serial preoperative neck US examinations during an observation period (>1 year) with a thyroid nodule >10 mm. From the original group, 172 patients were eligible for analysis. During follow-up, 47 (42%) benign and 24 (40%) malignant nodules underwent thyroidectomy because of nodule growth. The remaining patients underwent surgery for various reasons, including large primary tumor size with and without symptoms (n = 17 and n = 18, respectively), suspicious US features (n = 11), repeated results of AUS-A (n = 27), and the presence of RAS mutations (n = 10) with cytological diagnosis of AUS-A. Thirteen patients underwent thyroidectomy due to the patients' desire to have a nodule removed, and five patients delayed their surgery due to comorbidities. The median follow-up duration was 52.6 months (range 12.7–198.3 months). The study protocol was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Korea.
Neck US examination and follow-up protocol
Neck US images were evaluated with an iU22 unit (Philips Healthcare, Bothell, WA) or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear high-frequency probe (5–14 MHz). Neck US examinations were performed by radiologists under the supervision of two experienced thyroid radiologists (J.H.L. and J.H.B.), as described (14). Thyroid nodules on US images were evaluated three-dimensionally to measure tumor volume on both the transverse and longitudinal planes. Inter-observer variations in measurements of the diameter and volume of thyroid nodules were approximately 13% and 7%, respectively (14). All patients were regularly followed up with physical examinations and neck US every 6–24 months before thyroid surgery.
Pathologic evaluation
FNA procedures were performed under US guidance by experienced radiologists using a 23-gauge needle connected to a 10 mL syringe. The preoperative FNAC results were classified into six categories by using TBSRTC (5). Based on the recent TBSRTC system, FNAC results with Bethesda category III was assigned to five subcategories, and AUS-A was defined as a predominance of microfollicles in a sparsely cellular aspirate with scant colloid (5). Thus, nodules containing features of nuclear atypia were excluded from this study. If a nodule underwent FNA more than once, the FNAC result was based on the highest Bethesda category. Surgically removed specimens were reviewed and diagnosed using the World Health Organization classification criteria (6). Benign and malignant nodules were confirmed pathologically. All FNAC and surgical specimens were reviewed and diagnosed by an experienced endocrine pathologist (D.E.S.).
Definition of significant tumor growth and growth rate evaluation
The largest diameter and volume of thyroid nodules were retrospectively estimated based on at least three consecutive US images. Each nodule targeted for resection was >10 mm in diameter, and the volume of each nodule was calculated using the ellipsoid formula: length (cm) × width (cm) × depth (cm) × π/6 (13). Significant growth was defined as an increase of ≥20% in at least two nodule dimensions, each representing at least a 2 mm increase from baseline diameter or a >50% increase in nodule volume (1).
Statistical analysis
Data were analyzed using R studio v3.4.0 and the R libraries (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline characteristics
The baseline clinicopathologic characteristics of patients who underwent diagnostic thyroid surgery for an AUS-A thyroid nodule are shown in Table 1. Based on the pathologic results, 112 (65%) patients had benign nodules and 60 (35%) had malignant nodules. Details of pathologic subtypes are described in Supplementary Table S1. Of the 112 benign nodules, 63 were follicular adenomas (FAs), 28 were nodular hyperplasias, and 21 were adenomatous nodules. Of the 60 malignant nodules, 29 were FTCs, and 31 were follicular variant of PTC (FVPTC), including 12 noninvasive encapsulated FVPTCs (NI-EFVPTC/noninvasive follicular thyroid neoplasms with papillary-like nuclear features [NIFTP]), 13 invasive EFVPTCs, and six infiltrative FVPTCs. The median age of the 172 patients at the time of initial neck US was 48 years (IQR 40–56 years), and their median age at the time of thyroid surgery was 53 years (IQR 45–60 years). Age did not differ significantly between the groups of patients with benign and malignant nodules. The proportion of females was not significantly different between the benign and malignancy groups (82% and 73%, respectively; p = 0.247). Median primary tumor sizes were 2.2 cm (IQR 1.7–3.0 cm) on initial US, and 2.9 cm (IQR 2.2–3.7 cm) in surgical specimens, with no significant differences between benign and malignant groups in primary tumor size at the time of initial US (p = 0.796) and surgery (p = 0.793). A total of 29 (17%) patients underwent total thyroidectomy at initial surgery, and initial surgical extent was not significantly different between the two groups (p = 0.264).
Baseline Clinicopathologic Characteristics
Continuous variables are presented as medians (interquartile ranges). Categorical variables are presented as numbers (percentages).
US, ultrasonography.
Growth kinetics of benign and malignant nodules
Figure 1 shows the changes in largest diameter and volume of benign and malignant thyroid nodules over time. The median times between the first and last US evaluation of patients with benign and malignant nodules were 42.7 months (IQR 22.7–75.7 months) and 62.9 months (IQR 45.9–91.3 months), respectively. Both benign and malignant nodules showed a significant increase in largest diameter (p < 0.001 each), while the increasing rate of the largest diameter between the two groups were similar (p = 0.132; Fig. 1A). The volumes of benign and malignant nodules were also significantly increased (p < 0.001 each), but the difference in the rate of increase based on volume was not statistically significant between the two groups (p = 0.200; Fig. 1B).
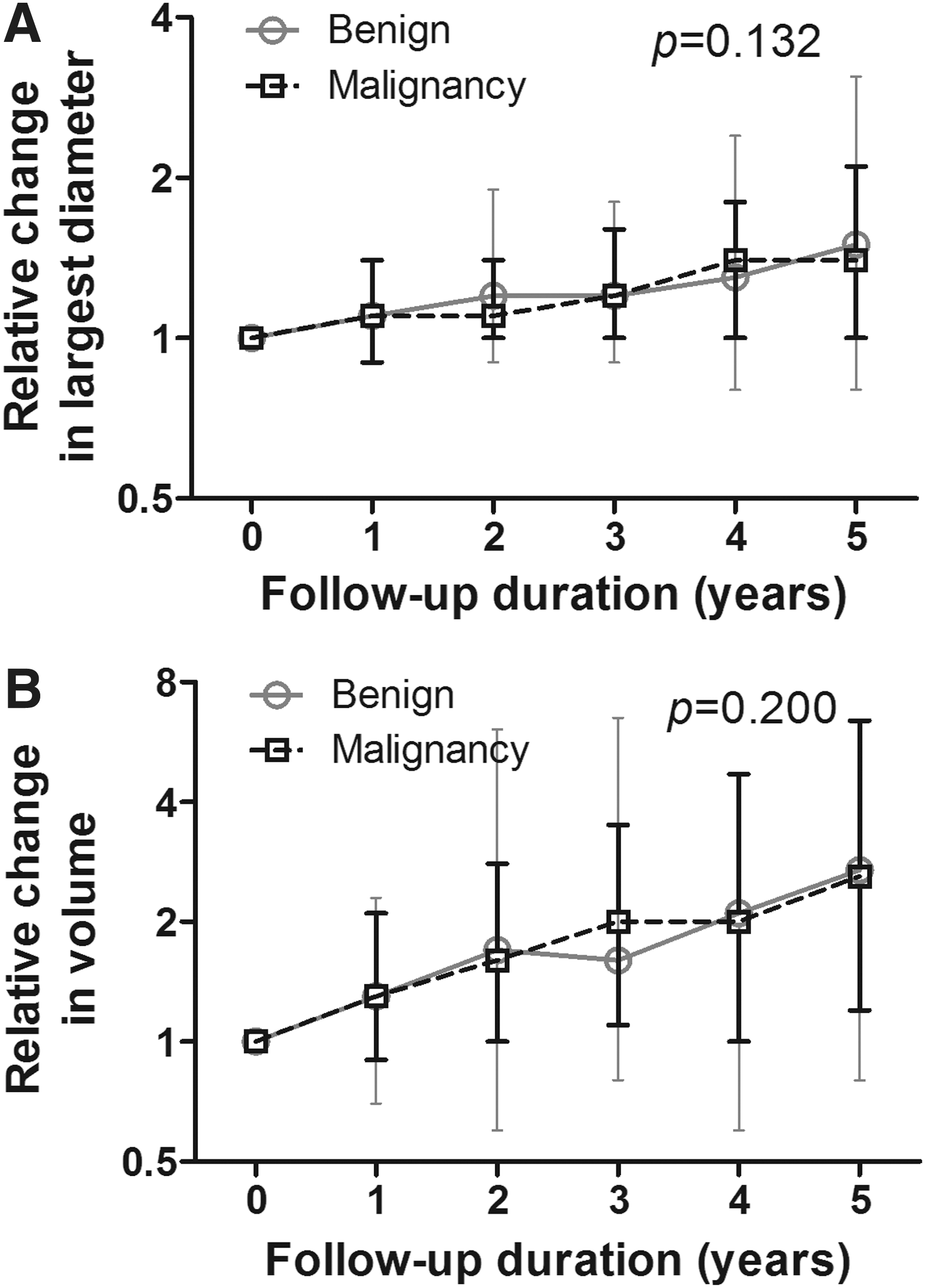
Time-trend changes according to the (
Comparative growth rates of benign and malignant nodules
There was no significant difference in time to significant tumor growth between benign and malignant nodules (p = 0.458; Fig. 2). The median estimated times to significant tumor growth from baseline were not significantly different between benign (1.71 years; IQR 0.86–3.40 years) and malignant (1.92 years; IQR 1.07–3.12 years) nodules (p = 0.568; Table 2). There was also no significant difference in the median estimated time to significant tumor growth according to the pathologic subtypes (p = 0.522; Supplementary Table S2). When NI-EFVPTCs (NIFTP lesions) were analyzed separately, they tended to grow more slowly than malignant tumors (Supplementary Table S3). The median time to tumor growth based on the largest diameter and volume of thyroid nodules was not significantly different between benign and malignant groups (p = 0.467 and p = 0.901, respectively; Table 2).
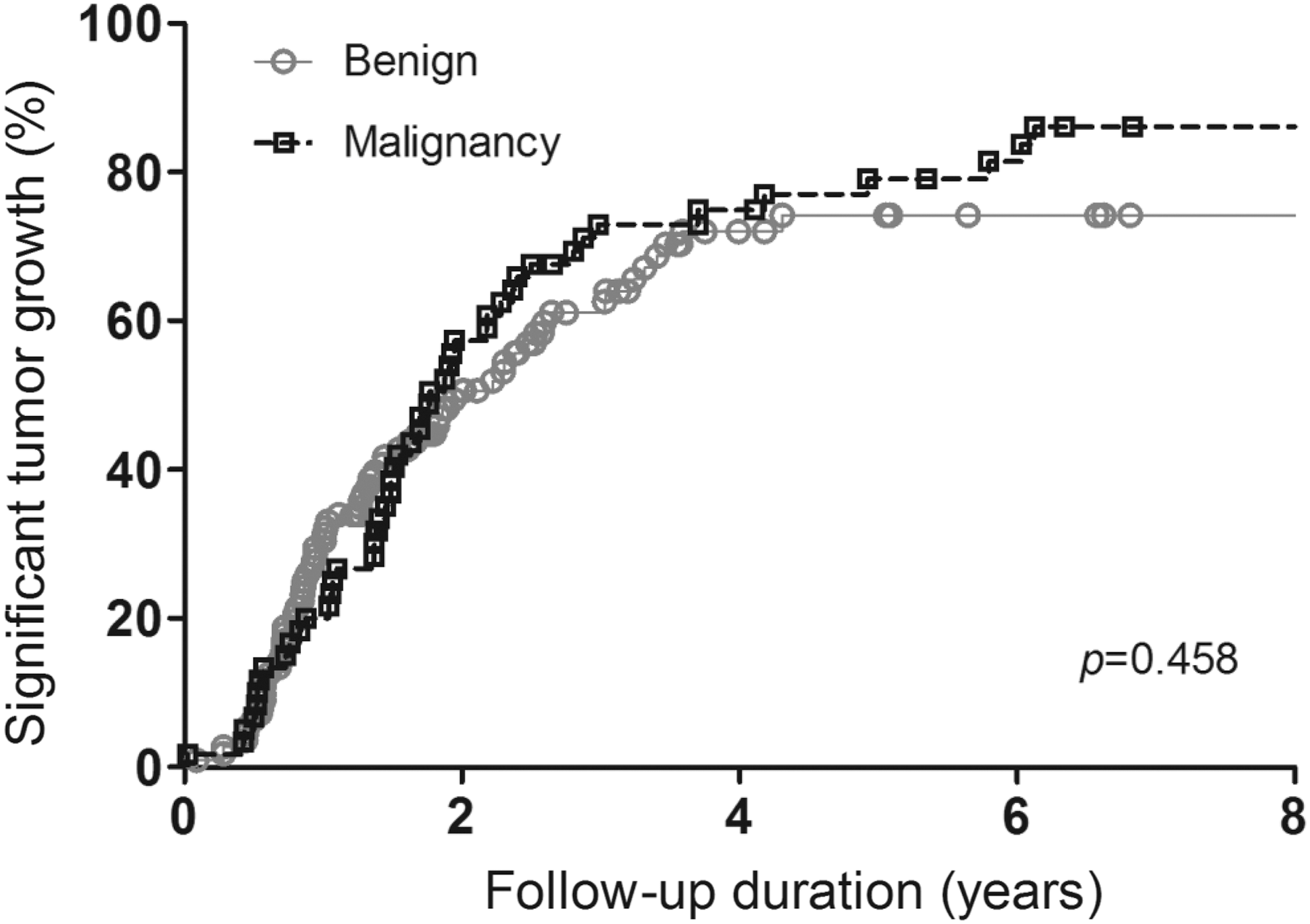
Kaplan–Meier curves about time to significant tumor growth. There was no significant difference in time-to-growth curves between benign and malignant thyroid nodules.
Time to Tumor Growth of Benign and Malignant Thyroid Nodules
Reported as median with interquartile ranges.
Calculated by Mann–Whitney tests.
Defined as an increase of ≥20% in at least two nodule dimensions, each representing at least a 20% increase in baseline diameter or a >50% increase in nodule volume.
An evaluation of annual growth rates of benign and malignant thyroid nodules (Table 3) showed that 19 (17%) and 62 (55%) of benign nodules and 4 (7%) and 32 (53%) of malignant nodules grew >20% in largest diameter and 50% in volume per year, respectively. The RR of malignancy was not significantly higher in growing nodules than in stable nodules based on largest diameter (RR = 0.46 [CI 0.19–1.16]; p = 0.064) and volume (RR = 0.92 [CI 0.62–1.39]; p = 0.748).
Rate of Thyroid Nodule Growth and Relative Risk of Malignancy in Thyroid Nodules with AUS-A
AUS-A, atypia of undetermined significance with architectural atypia; RR, relative risk; CI, confidence interval.
Discussion
This study included patients who underwent diagnostic thyroid surgery for nodules with AUS-A and who were preoperatively followed up for a sufficient time to estimate the growth of the nodules. This approach allowed the natural course of thyroid nodules with AUS-A to be evaluated. Tumor growth rates and the estimated median times to significant tumor growth from baseline did not differ significantly between malignant and benign nodules. Moreover, the evaluation of the malignancy risk based on the annual growth rates showed no significant differences between growing and stable thyroid nodules with AUS-A. These findings suggest that clinical surveillance to detect significant tumor growth during follow-up has limited value for the management of patients with AUS-A, as demonstrated in this cohort with surgical confirmation of the final pathology.
Although the American Thyroid Association guidelines recommend repeat FNA, molecular testing, or diagnostic surgical resection if the nodule size increases significantly during surveillance, there is little evidence to show that significant tumor growth is a predictor of malignancy, especially in AUS-A cases (1,13,15,16). A small pilot study showed no difference in the growth over 38 months of 15 PTCs and 12 benign thyroid nodules (17). However, FNAC results were not presented in that study, and PTC is diagnosed at a higher frequency in the AUS-N subcategory than among AUS-A lesions. Therefore, those results do not reflect the difference in the growth rates of benign and malignant nodules in the AUS-A subcategory (11). Recent prospective studies have shown that malignant thyroid nodules grow more rapidly than benign nodules that were characterized by cytology (18). Therefore, it is still doubtful whether thyroid nodule growth can clearly distinguish benign and malignant lesions, especially in a subgroup of nodules with indeterminate cytology. A recent study evaluating tumor growth between surgically proven FTCs and FAs suggested that growth kinetics could not predict malignancy (19). Therefore, sonographic assessment of thyroid nodule growth should be performed in clinically relevant subgroups according to cytology results. To the authors' knowledge, this study is the first to evaluate the growth rates of surgically resected nodules with AUS-A objectively based on serial preoperative US results. The findings may provide an evidence-based recommendation for managing patients with thyroid nodules with AUS-A.
In this study, malignancy rates after diagnostic thyroid surgery were 35%. Recently, the revised TBSRTC has reported that the risks of malignancy are 10–30% in the AUS category when NIFTP were regarded as malignant tumors (5). Although this study included NIFTP in the malignant group, the malignancy rate of nodules with AUS-A was slightly higher than that in previous studies (2,5). One possible explanation is that this study only included patients who underwent diagnostic surgery after long-term follow-up. Generally, patients with AUS nodules undergo diagnostic surgery only if worrisome clinical or sonographic features or abnormal results are present on repeat FNAC or molecular testing (1).
This study had several limitations. Its retrospective design may have introduced a selection bias because only surgically resected thyroid nodules were evaluated and a relatively limited number of study patients were included. Although a final pathologic diagnosis is required to compare benign and malignant nodules that display growth, undoubtedly there are many unresected nodules with AUS-A. Patients with high suspicious features of a malignant thyroid nodule are likely to undergo diagnostic surgery immediately after diagnosis with AUS-A to confirm malignancy, regardless of growth rate. However, in this study, patients who underwent early thyroid surgery had to be excluded because the change in tumor volume could not be assessed properly. Patients who underwent early diagnostic surgery were also excluded because their changes in tumor volume could not be analyzed. A previous study showed that benign thyroid nodules bearing RAS mutations grow more rapidly than those with wild-type RAS (20). In this study, RAS mutation analysis was only performed in a small number of patients, and the association between growth rate and RAS mutations could not be evaluated. Nevertheless, this study is the first to evaluate the natural growth kinetics of thyroid nodules cytologically classified as AUS-A over a median of 53 months.
In conclusion, the nodule size of the studied lesions with a cytological diagnosis of AUS-A showed a significant increase over time but without a significant difference in growth rates between benign and malignant thyroid nodules. Clinical surveillance based on changes in size on serial neck US has limited value in patients with AUS-A nodules, especially in those without highly suspicious clinical or sonographic features. Although the nodules of this cohort were not evaluated with molecular markers, tumor growth should probably not be considered a surrogate of benignity in nodules with negative molecular marker test results, as has been recently proposed (21 –23).
Footnotes
Acknowledgments
This study was supported by the National Research Foundation (NRF) of Korea Research Grant (NRF-2018R1D1A1A02085365).
Author Disclosure Statement
No authors have any conflicts of interest in relation to this manuscript.