
Abstract
Background:
Severe maternal iodine deficiency can impact fetal brain development through effects on maternal and/or fetal thyroid hormone availability. The effects of mild-to-moderate iodine deficiency on thyroid function are less clear. The aim was to investigate the association of maternal urinary iodine concentration corrected for creatinine (UI/Creat) with thyroid function and autoantibodies in a mild-to-moderate iodine-deficient pregnant population.
Methods:
This study was embedded within the Swedish Environmental Longitudinal, Mother and child, Asthma and allergy (SELMA) study. Clinical reference ranges were determined by the 2.5th and 97.5th population-based percentile cutoffs. The associations of UI/Creat with thyrotropin (TSH), free thyroxine (fT4), free triiodothyronine (fT3), total T4 (TT4), and total T3 (TT3) were studied using multivariable linear regression in thyroid peroxidase antibody (TPOAb)-negative women. The association of UI/Creat with TPOAb and thyroglobulin antibody (TgAb) positivity was analyzed using multivariable logistic regression.
Results:
Urinary iodine and thyroid function were measured at a median (95% range) gestational age of 10 (6–14) weeks in 2009 women. The median (95% range) UI/Creat was 85 μg/g (36–386) and the UI/Creat was below 150 μg/g in 80.1% of women. Reference ranges did not differ substantially by UI/Creat. A lower UI/Creat was associated with a lower TSH (p = 0.027), a higher TT4 (p = 0.032), and with a corresponding trend toward slightly higher fT4 (p = 0.081), fT3 (p = 0.079), and TT3 (p = 0.10). UI/Creat was not associated with the fT4/fT3 (p = 0.94) or TT4/TT3 ratios (p = 0.63). Women with a UI/Creat of 150–249 μg/g had the lowest prevalence of TPOAb positivity (6.1%), while women with a UI/Creat of <150 μg/g had a higher prevalence (11.0%, odds ratio [OR] confidence interval [95% CI] 1.84 [1.07–3.20], p = 0.029). Women with a UI/Creat ≥500 μg/g showed the highest prevalence and a higher risk of TPOAb positivity, however, only a small proportion of women had such a UI/Creat (12.5%, OR, [95% CI] 2.36 [0.54–10.43], p = 0.26).
Conclusions:
We could not identify any meaningful differences in thyroid function reference ranges. Lower iodine availability was associated with a slightly lower TSH and a higher TT4. Women with adequate iodine intake had the lowest risk of TPOAb positivity.
Introduction
During pregnancy there is an increased demand for maternal thyroid hormone because of the placental transport of thyroid hormone to the fetus, an increase in thyroxine-binding globulin concentrations, and a higher degradation of thyroid hormone due to placental type III iodothyronine deiodinase (1). Iodine is an essential component of thyroid hormone and both low and high iodine intakes may adversely affect thyroid function (2). A considerable increase in preconceptional or gestational daily iodine intake is required to meet the higher demand for thyroid hormone, to compensate for greater iodine losses during pregnancy, and to transfer a sufficient amount of iodine to the fetus (3 –5). The current guidelines of the World Health Organization therefore recommend an iodine intake of 250 μg/day for pregnant and lactating women as opposed to 150 μg/day in an adult nonpregnant state (3). However, data on the effects of iodine availability on maternal thyroid function during pregnancy are inconsistent.
A large Chinese study indicated that in pregnant women, the optimal urinary iodine concentration (UIC) ranged from 150 to 250 μg/L (6). Outside this range there was a higher prevalence of women with thyroid autoimmunity and women with a UIC above this range had a higher risk of subclinical hypothyroidism and isolated hypothyroxinemia (6). A few studies show that a lower UIC during pregnancy is associated with a higher free thyroxine (fT4) (7,8) and free triiodothyronine (fT3) (7 –9), while a higher UIC has been associated with higher thyrotropin (TSH) (8,10) and higher fT3 (11). On the contrary, other studies, of which several are small in size (N < 700) (11 –14), do not report any association of UIC with TSH or fT4 (9,11 –15) and data on (f)T3 are often lacking. While it is recommended that pregnancy TSH and fT4 reference ranges should be calculated in an iodine-sufficient population (4), there is insufficient evidence to determine whether reference ranges are affected by iodine status.
Therefore, the aim of our study was to analyze the cross-sectional association of maternal iodine status with maternal TSH, fT4, fT3, total T4 (TT4), total T3 (TT3), the fT4/fT3 and TT4/TT3 ratios, thyroid peroxidase antibodies (TPOAbs), and thyroglobulin antibodies (TgAbs), and to determine variation in thyroid function reference ranges according to iodine status.
Materials and Methods
Study population
This study was embedded in the Swedish Environmental Longitudinal, Mother and child, Asthma and allergy (SELMA) study, which is a population-based prospective birth cohort study originating in the county of Värmland, Sweden (16). Sweden is a country with a voluntary fortification program and iodized salt since 1936 (17). Pregnant women who visited an antenatal care center for the first time around week 10, but before week 22 of pregnancy, between September 2007 and March 2010 were invited to participate in the SELMA study. Pregnant women provided written informed consent, and the SELMA study is approved by the Regional Ethics Committee, Uppsala, Sweden (2007-05-02, Dnr: 2007/062). For the current study, women were included if a measure of urinary iodine and creatinine concentration, and thyroid function during pregnancy were available. Exclusion criteria were twin pregnancy, thyroid interfering medication usage, and pre-existing thyroid disease.
Laboratory measurements
Early morning void urine samples were collected at the day for enrollment and stored at −20°C. Urinary iodine was measured by the Sandell–Kolthoff method. Iodine calibration was performed using certified reference materials (CRM), Seronorm urine Levels one and two (Nycomed, Norway), and four EQUIP samples certified for UIC (Centers for Disease Control and Prevention). At a level of 1.7 μmol/L iodine, the within-assay coefficients of variation (CVs) were 5.1% and the between-assay CVs were 14.3% (N = 30). The urinary creatinine concentration was determined by the Jaffe rate method. The UIC corrected for creatinine (UI/Creat) was used as a marker of iodine status.
Nonfasting blood samples were collected at enrollment and were stored frozen at −80°C in a biobank at the Central Hospital in Karlstad, Sweden. Serum TSH, fT4, fT3, TT4, TT3, TPOAbs, and TgAbs were measured using the electrochemiluminescence assay (Cobas e601 platform; Roche Diagnostics, Mannheim, Germany) at the Department of Clinical Chemistry, Máxima Medical Center in Veldhoven, the Netherlands. Human chorionic gonadotropin (hCG) was determined in lithium–heparin plasma using electrochemiluminescence assays (Cobas® e601; Roche Diagnostics). Within-laboratory CVs were 2.1%, 3.5%, 3.8%, 3.8%, and 7.7% for TSH, fT4, fT3, TT4, and TT3, respectively. For hCG, the CV was 2.5% at 4.3 U/L and 2.1% at 171 U/L. The manufacturer's cutoffs for TPOAb and TgAb positivity were at the concentrations of >34 IU/mL or >115 IU/mL, respectively.
Serum cotinine was used as a marker for smoking. Briefly, aliquots of 100 μL serum were added with labeled internal standard and proteins were precipitated by acetonitrile and analyzed using liquid chromatography-tandem mass spectrometry. Participants were categorized as nonsmokers if their cotinine concentrations were <0.2 ng/mL and as active smokers if their cotinine concentrations were ≥15 ng/mL. If their concentrations were in between, participants were considered to be passive smokers.
Covariates
Information on gestational age at blood and urine sampling, maternal age at enrollment, maternal ethnicity (Western, non-Western), and maternal educational level (low = none or primary education; medium = secondary education; high = higher education) was collected through questionnaires. The Swedish National Birth Register was used to collect data on a diagnosis of thyroid disease, parity, and child sex. Information on pregnancy weight and height, which was used to calculate body mass index (BMI), was collected either through a prenatal questionnaire or the Swedish National Birth Register.
Statistical analyses
Reference ranges were defined based on the 2.5th and 97.5th percentiles after exclusion of TPOAb-positive women. To check whether reference ranges differed according to iodine status, we defined reference ranges in women subdivided by quartiles of UI/Creat—to have equal numbers of women per category—and by alternative categorization, which broadly relates to cutoff values based on the epidemiological criteria for assessing iodine nutrition in pregnant women (UI/Creat <50, 50–99, 100–149, 150–249, 250–499, and ≥500 μg/g) (3). As a sensitivity analysis, we also defined the reference ranges in women using this alternative categorization based on the UIC.
We studied the association of UI/Creat across the full range with TSH, fT4, fT3, TT4, TT3, and the fT4/fT3 and TT4/TT3 ratios using multivariable linear regression analyses in TPOAb-negative women. Nonlinearity was tested using restricted cubic splines with three knots and we evaluated normality of residuals using histograms.
We studied the association of UI/Creat across the full range with TPOAb and TgAb positivity using multivariable logistic regression. Similar models were used for exploring the association of a UI/Creat of <150 (<50, 50–99, 100–149), 250–499, and ≥500 μg/g with thyroid antibody positivity compared with the reference group of women with a UI/Creat of 150–249 μg/g. This analysis was repeated using the same categorization based on the UIC.
UI/Creat, TSH, and TPOAb concentrations were log-transformed. Back-transformed values are shown in plots for better interpretation. Values in the lowest and highest centile of UI/Creat and thyroid function tests were considered outliers and excluded from the regression analyses when analyzed across the full range. All analyses were adjusted for hCG, gestational age at blood and urine sampling, maternal age, maternal ethnicity, maternal educational level, parity, maternal BMI, smoking status based on the serum cotinine concentration, and child sex. We additionally adjusted for TPOAbs in the analysis of the association between UI/Creat and thyroid function tests. With ANOVA, we tested the null hypothesis that the thyroid hormone concentrations were similar across the full range of the natural logarithm of UI/Creat.
Missing data of covariates were imputed using multiple imputations by chained equations, generating 25 data sets. The statistical analyses were performed using R statistical software version 3.4.3 (R Core team, Vienna, Austria; packages mice and rms).
Results
The final study population comprised 2009 pregnant women, in whom data on both UI/Creat and thyroid function were collected at a median (95% range) gestational age of 10 (6 –14) weeks (Fig. 1). The median UI/Creat (95% range) was 85 (36–386) μg/g and the UI/Creat was below 150 μg/g in 80.1% of women. The majority of women were of Western descent (97.3%), nonsmokers (84.9%), and had a secondary (“middle”) or higher (“high”) educational level (33.6% and 54.4%, respectively). Further study population characteristics are shown in Table 1.
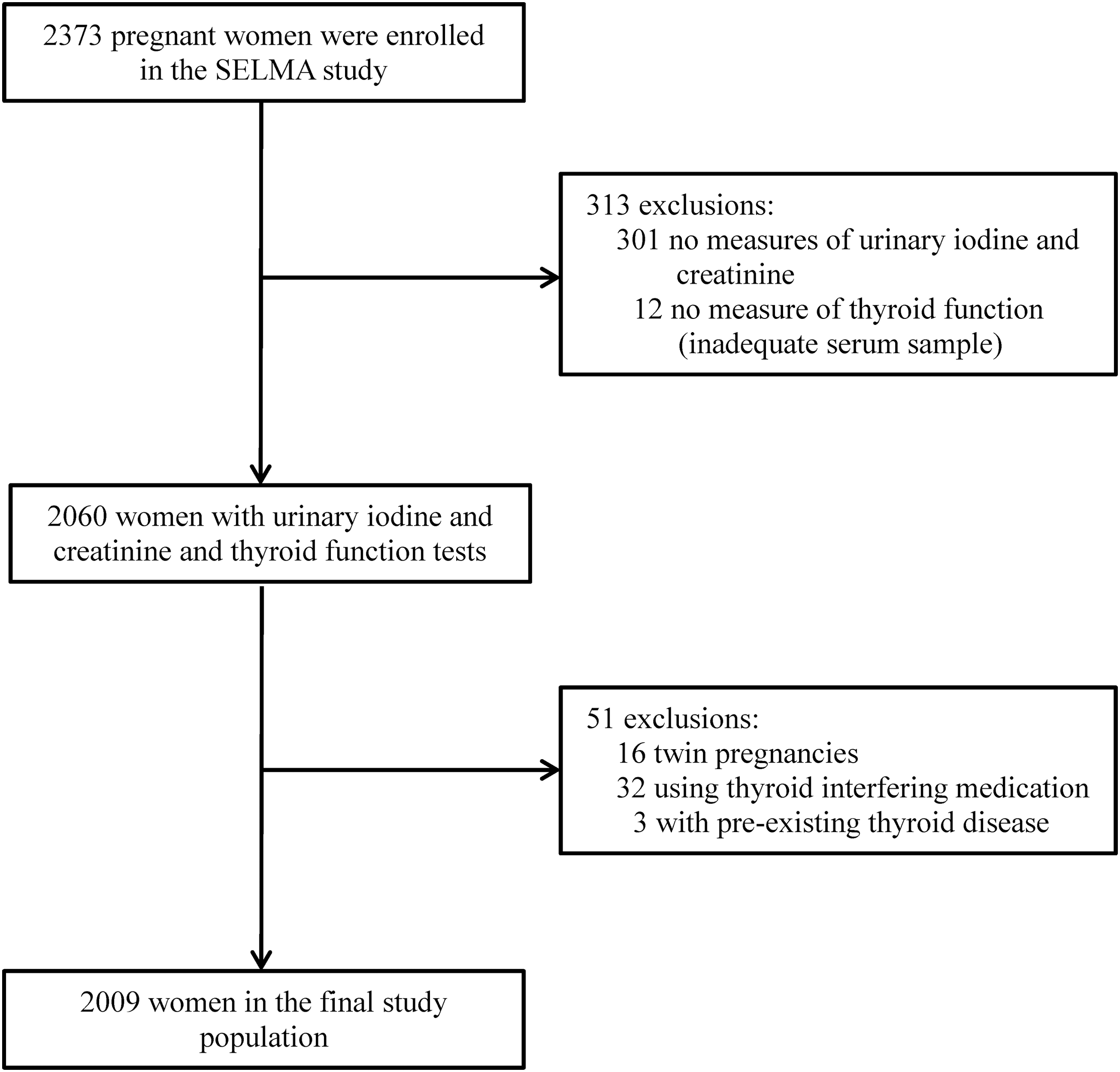
Flowchart of the selection of the study population.
Characteristics of the Study Population (N = 2009)
TPOAb positivity and TgAb positivity were defined as >34 and >115 IU/mL, respectively. Numbers of covariates are based on imputed data.
BMI, body mass index; fT3, free triiodothyronine; fT4, free thyroxine; hCG, human chorionic gonadotropin; T3, triiodothyronine; T4, thyroxine; TT3, total triiodothyronine; TT4, total thyroxine; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin; UIC, urinary iodine concentration; UI/Creat, UIC corrected for creatinine.
Thyroid function reference ranges
Thyroid function reference ranges did not differ substantially according to UI/Creat when analyzed per quartile (Table 2). The relative largest difference in cutoffs for thyroid function reference ranges was for the upper limit of TSH. However, these differences were small in absolute values and there was no clear trend across iodine status. In the lowest quartile of UI/Creat, the upper limit for TSH was 3.24, which is 0.16 mU/L (4.7%) lower than that in the total population. In the highest quartile, the upper limit was 3.26, which was 0.14 mU/L (4.1%) lower than that calculated in the total population. For other cutoffs of UI/Creat or UIC, the number of women with more-than-adequate and excessive values was too small for reliable calculations (Supplementary Tables S1 and S2).
Reference Ranges (2.5th and 97.5th Percentile Values) of Thyroid Function Tests in TPOAb-Negative Women, Stratified by Quartiles of UI/Creat
TPOAb positivity defined as >34 IU/mL. The range of difference of the lower limit is calculated by comparing the 2.5th percentile value of each thyroid function test in the whole study population (“Total”) to the most deviating 2.5th percentile value calculated in women subdivided into the four quartiles of UI/Creat. The range of difference of the upper limit is calculated by comparing the 97.5th percentile value of each thyroid function test in the whole study population (“Total”) to the most deviating 97.5th percentile value calculated in women subdivided into the four quartiles of UI/Creat.
NA, not applicable.
Iodine status and thyroid function
A lower UI/Creat was associated with a lower TSH and a higher TT4 (Fig. 2 and Supplementary Table S3). There was a trend toward an association of a lower UI/Creat with a higher fT4 (p = 0.081), fT3 (p = 0.079), and TT3 (p = 0.10). There was no association of UI/Creat with the TT4/TT3 and fT4/fT3 ratios (Fig. 2 and Supplementary Table S3).
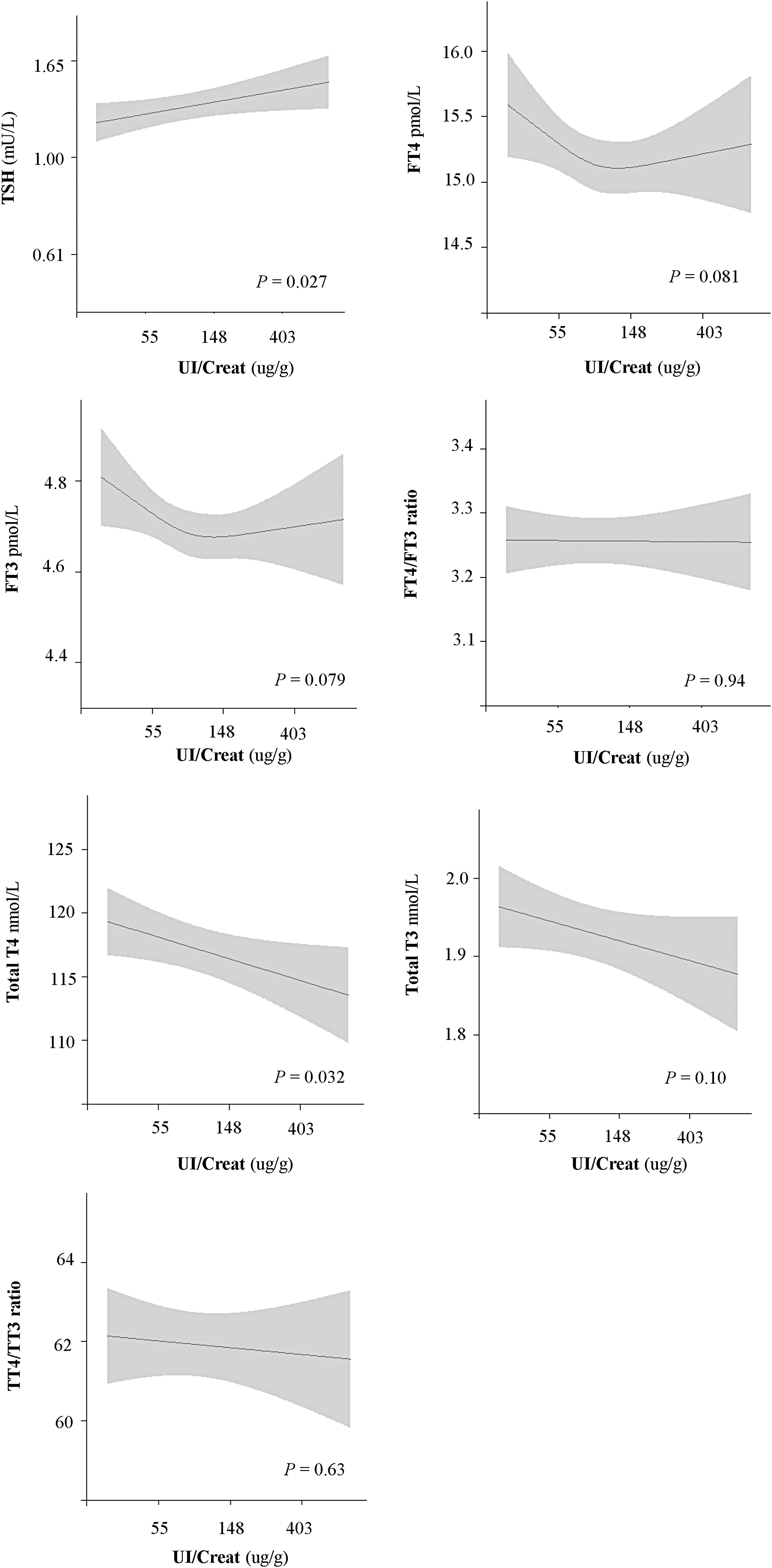
Association between the natural log of UI/Creat and thyroid function tests in TPOAb-negative women. Analyses were performed by multivariable linear regression analyses, adjusted for TPOAb, hCG, gestational age, maternal age, maternal ethnicity, maternal education, parity, maternal BMI, smoking status based on the serum cotinine concentration, and child sex. UI/Creat, TSH, TPOAb, and hCG were log transformed. Back-transformed values are shown in plots for better interpretation. BMI, body mass index; hCG, human chorionic gonadotropin; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin; UI/Creat, urinary iodine concentration corrected for creatinine.
In the whole study population, an increase of one unit in the natural logarithm of UI/Creat was associated with a 27% lower risk of TPOAb positivity (odds ratio [OR] 0.73, confidence interval [95% CI] 0.56–0.98, p = 0.034), but not with TgAb positivity [OR 0.83, 95% CI 0.61–1.14, p = 0.25, analyses per quartile in Supplementary Table S4].
While TPOAb positivity was present in 6.1% of women with a UI/Creat of 150–249 μg/g, this was 11.0% in women with a UI/Creat of <150 μg/g [OR 1.84, 95% CI 1.07–3.20, p = 0.029, Table 3]. Women with a UI/Creat of ≥500 μg/g had a higher risk of TPOAb positivity with 12.5% being TPOAb positive. However, only a small proportion of women entered in this category [N = 24; OR 2.36, 95% CI 0.54–10.43, p = 0.26]. Analyses based on the UIC showed similar results (Supplementary Table S5). For TgAb positivity, there was a similar pattern as for TPOAb positivity but with considerably smaller percentage differences (Table 3).
Association Between UI/Creat and Thyroid Autoantibodies
Analyses were performed by multivariable logistic regression analyses, adjusted for hCG, gestational age, maternal age, maternal ethnicity, maternal education, parity, maternal BMI, cotinine, and child sex. TPOAb positivity and TgAb positivity were defined as >34 and >115 IU/mL, respectively.
The total number (%) of women with a UI/Creat <150, 150–249, 250–499, and ≥500 μg/g in the total study population is 1609 (80.1%), 247 (12.3%), 129 (6.4%), and 24 (1.2%), respectively.
Stratified subanalysis TPOAb positivity: UI/Creat <50 μg/g, OR 1.70 [95% CI 0.86–3.37], p = 0.13; 50–99 μg/g, OR 1.92 [1.09–3.40], p = 0.025; 100–149 μg/g, OR 1.74 [0.93–3.25], p = 0.084. Stratified subanalysis TgAb positivity: UI/Creat <50 μg/g, OR 1.79 [0.85–3.78], p = 0.13; 50–99 μg/g, OR 1.62 [0.87–3.01], p = 0.13; 100–149 μg/g, OR 1.66 [0.84–3.26], p = 0.14.
CI, confidence interval, OR, odds ratio.
Discussion
In this study of pregnant women from a mild-to-moderately iodine-deficient population, we studied the association of iodine status with a detailed profile of thyroid function and autoantibodies. Gestational reference ranges for thyroid function tests did not differ substantially by iodine status. We show that a lower UI/Creat was associated with significantly lower TSH, higher TT4, and a higher risk of TPOAb positivity. A lower UI/Creat was also associated with a higher fT4, fT3, and TT3, but these associations did not reach statistical significance (p ≤ 0.10). The fT4/fT3 and TT4/TT3 ratios were stable across the full range of UI/Creat.
Low iodine intakes may trigger mechanisms to counteract any potential thyroidal consequences. These include an increase in the thyroidal uptake of iodine, mainly via stimulation of the sodium–iodide symporter by increasing TSH concentrations (18). This typically occurs from a daily iodine intake of <100 μg/day and results in a lower renal iodine clearance, thus likely reflected by a lower UI/Creat.
In the current study, a higher UI/Creat was associated with a higher TSH. This finding has been reported in other pregnant populations as well (6,8). A possible explanation would be that a lower UI/Creat also increases the risk of autonomous thyroid hormone production by nodules/multinodular goiters, which is associated with a lower TSH (19,20). Alternatively, a higher TSH at a higher range of UI/Creat values may also partially reflect the Wolff–Chaikoff effect caused by higher iodine intakes, especially when this increase occurs rapidly (15,21). In rats, a higher TSH was explained by reduced deiodinase type II activity due to excessive iodine intakes (22,23).
The TSH reference ranges in the total population, however, did not deviate much from the reference ranges among groups of UI/Creat, ranging from iodine deficiency to iodine sufficiency, which is in line with a previous study from Norway (7). While it is known that reference ranges differ between populations (24), and that those differences may be partially explained by differences in ethnicity (25 –27), there has been insufficient evidence that iodine status may also affect thyroid function within its normal range.
There is a concern that reference ranges may be affected when calculated in populations with (mild-to-moderate) iodine deficiency. This concern could be ascribed to the association with thyroid autoimmunity, as there may be a higher risk of TPOAb positivity at lower iodine intakes. However, it has already been recommended that the calculation of thyroid function reference ranges should be performed in TPOAb-negative pregnant populations (4). This study therefore calls into question the relevance of the selection criterion of iodine sufficiency for calculating thyroid reference ranges during pregnancy in addition to the criterion of excluding TPOAb-positive women.
Low iodine intake can cause a shift in thyroid hormone availability from T4 to the more biologically active T3 via upregulating peripheral type II deiodinase and by increasing the thyroidal secretion of T3 (28,29). Given this knowledge, we hypothesized that a lower UI/Creat would be associated with a lower TT4 and fT4. In contrast, our analyses show that lower UI/Creat was associated with a higher TT4 and also a trend toward a higher fT4 with UI/Creat lower than roughly 100 μg/g. The results of other studies have also been contra-intuitive with regard to the underlying physiology. Two of those, of which one was performed in an iodine-replete population and the other in a mild-to-moderate iodine-deficient population, also found a negative association between UI/Creat and fT4 (7,8).
Others investigated the potential effect of iodine supplementation on fT4 (7,30). One of these found that women who started iodine supplementation between week 13 and 20 of gestation had lower fT4 than nonusers or women who started supplementation preconceptionally (7). Another study showed that although the majority of women using iodine supplements had an fT4 within the reference range, those who had received iodine supplements in early pregnancy exhibited a faster decline in fT4 than those who had consumed iodized salt for at least two years before pregnancy (30). This could indicate that a more acute increase in iodine intake during pregnancy, rather than prolonged exposure to higher iodine availability, affects the association of UI/Creat with thyroid function, leading to a transient decrease in fT4, for example, via the Wolff–Chaikoff effect (21). Future studies are needed to identify thresholds from which iodine supplementation could affect thyroid function.
Based on the physiological adaptations in thyroid hormone physiology, we expected a priori that a lower UI/Creat would be associated with a higher fT3 and TT3, and possibly would decrease the fT4/fT3 and TT4/TT3 ratios. Our study shows a trend toward an association of UI/Creat—lower than roughly 100 μg/g—with an increase in fT3, but this association did not reach statistical significance. A similar, but statistically significant, association was identified in a study including a population with a slightly lower median UIC than in our population (68 μg/L vs. 90 μg/L in SELMA) and with a larger proportion of women below the recommended cutoff for defining iodine deficiency during pregnancy, i.e., UIC <150 μg/L (86% vs. 78.5% in SELMA) (7).
Other studies show a weak but statistically significant negative correlation between UIC and fT3 conducted in a similarly iodine-insufficient area (median UIC 89 μg/L) (9) and a sufficient area (median UIC 328 μg/L) (8), or oppositely, a positive correlation in a population with a large proportion of women with excessive iodine intakes (11). However, in our study, there was no association of UI/Creat with the fT4/fT3 and TT4/TT3 ratios, which could suggest that iodine availability was not low enough to evoke preferential production of T3 in this population. Possibly in more chronic severe iodine-deficient populations, women are at a higher risk of deplete intrathyroidal iodine storage already at the beginning or during the course of pregnancy, which may cause shifts in these ratios (1).
Thyroid autoantibody positivity occurs in 2% to 17% of pregnant women (4). TPOAb positivity is associated with a higher risk of miscarriage (31), preterm birth (31,32), child behavioral problems (33), and lower child IQ (34). In the current study, TPOAb positivity occurred more often in women with low or high UI/Creat. Interestingly, thyroid antibody concentrations tend to decline after the first trimester due to immune tolerance, and this could potentially affect the definition of TPOAb positivity (35 –37). However, in our study, blood samples were collected at a median gestational age of 10 weeks, before such a decrease in TPOAb titers would likely occur.
Women with a UI/Creat of 150–249 μg/g had the lowest prevalence of TPOAb positivity (6.1% vs. 11.0% and 12.5% in women with a UI/Creat of <50 and ≥500 μg/g, respectively). This finding is in line with a large study from an iodine-sufficient area in China, showing similar differences in the prevalence of TPOAb positivity among different UIC groups (6). Also, a study from Norway showed a U-shaped association of iodine intake measured by a food frequency questionnaire with TPOAb positivity in mild-to-moderately iodine-deficient pregnant women (7). That association, however, did not reach statistical significance and no association of urinary iodine with TPOAb positivity was identified (7).
We speculate that owing to the few women in each cohort with excessive iodine intakes, both our study and the Norwegian study did not have sufficient statistical power to show that high iodine intake is also associated with a higher risk of thyroid autoimmunity. Excessive iodine intakes may cause a shift toward proinflammatory cells and a higher generation of radical oxygen species due to increased iodination of thyroglobulin, activating pathways promoting thyrocyte apoptosis and thyroiditis (38,39).
We were able to study the association of iodine status with thyroid function using an extensive data set with multiple thyroid function tests and thyroid autoantibodies, and with a large number of potential confounding variables.
An important limitation for interpreting the results of the current study is that early morning urine void samples tend to underestimate daily iodine excretion (40). Furthermore, it is known that urinary iodine is highly variable from day-to-day and therefore not a good indicator of individual iodine status (41,42). It is important to note that the UI/Creat is a valid measure of iodine status of a population with the same sex and age (43), or large groups of individuals as those that were analyzed in the current study with a standardized sampling of morning void urine, because this reduces the consequences of measurement error. Another limitation is that the use of a single void urine and blood sample to measure iodine status and thyroid function, respectively, did not allow to study iodine status trajectories during pregnancy and subsequent changes in thyroid function.
There was also a lack of data on iodine containing supplement use. It would have been relevant to investigate whether the associations we observed in our study would differ based on supplement use and timing of intake as this could subdivide more acute from chronic changes in iodine intake (7). There are currently no national recommendations in Sweden on iodine supplementation during pregnancy and no data on the use of iodine containing supplements among pregnant women (44). However, a considerable percentage of pregnant women in Nordic countries, such as Norway and Denmark, use iodine containing supplements, which possibly suggests that the use of these supplements may also be substantial in Sweden (7,17). Lastly, the cross-sectional design of this study limits causal inference, and therefore, it is important to interpret these results while taking into account data from interventional and experimental studies.
To conclude, this study did not find any indication that differences in iodine status within the population had a meaningful effect on the reference ranges of thyroid function tests. Furthermore, we found that suboptimal gestational iodine status is associated with lower TSH, and higher TT4, but we found no clear indication of preferential T3 production due to iodine deficiency. Both low and high gestational iodine status may be associated with a higher risk of TPOAb positivity.
Footnotes
Acknowledgment
We thank Sverre Wikström for his help with collecting the data and for his advice on the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project has been supported by the Exchange in Endocrinology Expertise (3E) program of the European Union of Medical Specialists (UEMS), Section and Board of Endocrinology (to T.I.M.K). R.P.P was supported by a ZOnMW VIDI grant (016.176.331) and an Erasmus MC MRACE grant. The SELMA study was funded by grants from the Swedish Research Council (Formas) and the County Council of Värmland, Sweden.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5