
Abstract
Background:
The association of metabolic syndrome and its components with the risk of thyroid cancer is unclear. Thus, we conducted a large-scale, nationwide, population-based, cohort study to investigate this relationship.
Methods:
We studied 9,890,917 adults without thyroid cancer from the Korean National Health Insurance health checkup database from January 1 to December 31, 2009. Individuals with at least three of the following five components were diagnosed with metabolic syndrome: abdominal obesity, hypertriglyceridemia, low high-density lipoprotein-cholesterol levels, elevated blood pressure, and hyperglycemia. Multivariate Cox proportional hazards models were used to estimate thyroid cancer risk.
Results:
During the average 7.2 years of follow-up, 77,133 thyroid cancer cases were newly identified. The thyroid cancer risk was higher in the metabolic syndrome group than in the nonmetabolic syndrome group (hazard ratio [HR] 1.15 [95% confidence interval, CI 1.13–1.17]). The association between metabolic syndrome and thyroid cancer risk was significant in the obese group (HR 1.10 [CI 1.07–1.13]) and not in the nonobese group (HR 1.002 [CI 0.98–1.03]). The effect of metabolic syndrome on the risk of thyroid cancer differs according to obesity (p for interaction = 0.017). People with all five components of metabolic syndrome had a 39% higher risk than those without any components (HR 1.39 [CI 1.33–1.44]). The higher risk of thyroid cancer in people with all five components was significant in the obese group (HR 1.29 [CI 1.21–1.38]), but not in the nonobese group (HR 1.06 [CI 0.98–1.14]). There was a significant interaction between the number of metabolic syndrome components and obesity (p for interaction <0.0001). For the combined effect of obesity and metabolic syndrome on the risk of thyroid cancer, obese men with metabolic syndrome had the highest risk of thyroid cancer compared with those without (HR 1.58 [CI 1.52–1.64]), but obese women with metabolic syndrome did not.
Conclusions:
Metabolic syndrome was associated with an increased risk of thyroid cancer in the Korean general population. Metabolic syndrome had a more significant risk of thyroid cancer in the obese group. Metabolic syndrome and obesity were associated with a higher risk of thyroid cancer in men but not in women.
Introduction
The incidence of thyroid cancer has rapidly increased worldwide in the past several decades (1), and it is the third-most common cancer diagnosis in South Korea. Increased detection of subclinical thyroid cancers by increased utilization of ultrasonography and fine-needle biopsies may partly account for the rise in the incidence of thyroid cancer (2,3). However, this does not sufficiently explain the increase in the incidence of large tumors, in all size categories (4). Thus, it has been hypothesized that additional factors, such as changes in lifestyle and environmental factors, may play a role (5).
Meanwhile, the prevalence of obesity and unhealthy metabolic status such as metabolic syndrome has markedly increased during the same time period (6), and this may have contributed to the rise in thyroid cancer incidence (7). Recently, several studies have reported that obesity is positively associated with an increased risk of thyroid cancer (8 –13).
However, the relationship between metabolic syndrome and the risk of thyroid cancer is currently unclear. Metabolic syndrome is an important disorder that is characterized by a cluster of metabolic risk factors, including central obesity, hypertension, hyperglycemia, and dyslipidemia (14). The major mechanism of metabolic syndrome is insulin resistance (14). Few studies have investigated the association between metabolic syndrome and thyroid cancer, and these studies did not reveal any association between them (15 –17). Moreover, the effects of a combination of obesity and metabolic syndrome have been rarely studied. Most of the previous studies evaluated the association between body mass index (BMI) and the risk of thyroid cancer without considering the metabolic status associated with obesity (8 –13).
Therefore, we conducted a nationwide, population-based, large-scale, cohort study to investigate the association between metabolic syndrome and the risk of thyroid cancer, by obesity status.
Materials and Methods
Data source and study population
Our study was based on the entire South Korean population database provided by the National Health Insurance Service (NHIS). The NHIS is the public medical insurance system managed by the Korean government and provides a mandatory universal insurance system covering ∼97% of the South Korean population. In addition, the NHIS provides standardized health screenings every two years to all insured persons. We therefore obtained an extensive health information data set from NHIS, including demographics, medical treatment, procedures, diagnostic codes according to the International Classification of Diseases-10th Revision-Clinical Modification (ICD-10-CM) codes, and health examinations.
Study subjects included 10,490,501 people aged ≥20 years who had undergone a health examination provided by NHIS from January 1 to December 31, 2009. We excluded those who had a prior diagnosis of cancer during the four years of washout period before enrollment (n = 153,878 [1.5%]), those who had any missing variables (n = 417,833 [4.0%]), and those with a follow-up of less than one year (n = 27,873 [0.3%]). Finally, 9,890,917 individuals (5,470,130 men [55.3%] and 4,420,787 women [44.7%]) were included in the study and followed up until the date of development of thyroid cancer, death, or December 31, 2017.
The study was conducted according to the ethical principles outlined in the Declaration of Helsinki. All study procedures and ethical aspects were approved by the Institutional Review Board (IRB) of Korea University Ansan Hospital (IRB no. 2019AS0014). The requirement for written informed consent was waived by the review board because anonymous and deidentified information was used for the analysis, and none of the patients was contacted.
Assessment and definitions
The health examination provided by NHIS includes anthropometric and laboratory measurements. Height, weight, and waist circumference were measured, and BMI was calculated by dividing weight (kg) by height (m) squared. Obesity was defined as BMI ≥25 kg/m2 based on the World Health Organization recommendations for Asian populations (18). Systolic and diastolic blood pressure was measured in a seated position after at least five minutes of rest. Blood sampling was conducted after overnight fasting, and serum levels of glucose, total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and creatinine were measured. Estimated glomerular filtration rate (eGFR) was calculated using the equation from the Modification of Diet in Renal Disease study: eGFR = 175 × serum creatinine −1.154 × age −0.203, which was further multiplied by 0.742 in case of women (19). We defined eGFR <60 ml/min/1.73 m2 as chronic kidney disease (20).
Information of demographics and lifestyle was obtained through standardized self-administered questionnaires. Smoking status was classified as nonsmoker, ex-smoker, or current smoker. People who consumed ≥30 g of alcohol per day were defined as heavy alcohol drinkers (21). Physical activity was categorized based on the frequency per week of strenuous exercise performed for at least 20 minutes (none, 1–4 times/week, or ≥5 times/week). We analyzed comorbidities, including hypertension (ICD-10-CM codes I10e13 and I15 and claims for antihypertensive agents), diabetes mellitus (ICD-10-CM codes E11eE14 and claims for oral antidiabetic agents or insulin), and dyslipidemia (ICD-10-CM code E78 and claims for agents for dyslipidemia). Income level was dichotomized at the lower 20%.
Predictor and outcome variables
The definition of metabolic syndrome was based on the modified criteria of the National Cholesterol Education Program Adult Treatment Panel III, and the Asian-specific waist circumference cutoff was adopted for abdominal obesity (22). Individuals having at least three of the following five components were diagnosed with metabolic syndrome: (i) abdominal obesity (≥90 cm for men and ≥85 cm for women); (ii) hypertriglyceridemia (triglyceridemia ≥150 mg/dL, or ICD-10-CM code E78 and treatment with lipid-lowering medication); (iii) low HDL-C levels (<40 mg/dL for men and <50 mg/dL for women, or ICD-10-CM code E78 and treatment with lipid-lowering medication); (iv) elevated blood pressure (systolic blood pressure ≥130 and/or diastolic blood pressure ≥85 mmHg, or ICD-10-CM codes I10–13 and I15 and treatment with antihypertensive medication); and (v) hyperglycemia (fasting plasma glucose ≥100 mg/dL, or ICD-10-CM codes E11–E14 and use of hypoglycemic agents). We defined the use of lipid-lowering medication as at least one claim per year for lipid-lowering medication prescription under ICD-10-CM code E78.
The incidence of thyroid cancer was identified based on the presence of hospitalization records for thyroid cancer in the NHIS data from 2009 to 2017. The ICD-10-CM code for thyroid cancer was C73. We excluded patients who were diagnosed with thyroid cancer before the study period.
Statistical analyses
Baseline characteristics were compared using the independent t-test for continuous variables and the chi-squared test for categorical variables. Thyroid cancer incidence rates were calculated by dividing the number of events by 1000 person-years. Multivariate Cox proportional hazards regression models were used for assessing the hazard ratios (HRs) and 95% confidence intervals (CIs) and for investigating the association of metabolic syndrome and its components with the incidence of thyroid cancer. We analyzed the effect of metabolic syndrome on the development of thyroid cancer according to obesity. Interaction tests were also conducted to determine whether the effect of metabolic syndrome on the risk of thyroid cancer differs according to obesity. Model 1 was adjusted for age and sex. Model 2 was additionally adjusted for smoking status, alcohol consumption, physical activity, income, and chronic kidney disease. When analyzing individual metabolic syndrome components, the other four metabolic syndrome components were additionally adjusted. We evaluated the risk of thyroid cancer development according to the number of metabolic syndrome components using multivariate Cox proportional hazards analyses.
To examine the association of the number of metabolic syndrome components with the risk of thyroid cancer, the cumulative incidence probability of thyroid cancer was plotted using the cumulative incidence competing risk method. The cumulative incidence competing risk accounts for all types of events; in the case of competing events, the cumulative incidence function is estimated both for the event of interest and for all competing events, and their estimates depend on each other (21). Because of the competing risks of death for thyroid cancer, the Kaplan–Meier method can overestimate the probabilities. Moreover, we analyzed the combined effects of obesity and metabolic syndrome for thyroid cancer risk. Two-sided p value <0.05 was considered statistically significant. All statistical analyses were performed using SAS software (version 9.3; SAS Institute, Cary, NC).
Results
Baseline characteristics of study participants
Table 1 shows the baseline characteristics of the study population according to metabolic syndrome. There were 2,639,084 (26.7%) and 7,251,833 (73.3%) subjects with and without metabolic syndrome, respectively. Mean age was 54.6 ± 13.0 and 44.1 ± 13.4 years in the metabolic syndrome and nonmetabolic syndrome group, respectively.
Baseline Characteristics of Study Participants
Values are presented as mean (SD), n (%), or geometric mean [CI].
Geometric means.
Metabolic syndrome components: high WC (cm), ≥90 cm for men and ≥85 cm for women; high BP, systolic BP ≥130 and/or diastolic BP ≥85 mmHg, or ICD-10-CM codes I10–13 and I15 and treatment with antihypertensive medication; High fasting plasma glucose, fasting plasma glucose ≥100 mg/dL, or ICD-10-CM codes E11–E14 and use of hypoglycemic agents; high serum triglycerides, triglycerides ≥150 mg/dL, or ICD-10-CM code E78 and treatment with lipid-lowering medication; low serum HDL-C, <40 mg/dL for men and <50 mg/dL for women, or ICD-10-CM code E78 and treatment with lipid-lowering medication.
Obesity was defined as BMI ≥25kg/m2.
Low income was defined as a lower quintile of yearly income.
BMI, body mass index; BP, blood pressure; CI, 95% confidence interval; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; ICD-10-CM, International Classification of Diseases-10th Revision-Clinical Modification; LDL-C, low-density lipoprotein cholesterol; SD, standard deviation; WC, waist circumference.
The proportion of men, current smoker, and alcohol drinker was higher in the nonmetabolic syndrome group than the metabolic syndrome group. Individuals with metabolic syndrome exhibited higher mean values of BMI, waist circumference, blood pressure, fasting plasma glucose, serum total cholesterol, triglycerides, and LDL-C, but lower mean values of HDL-C and eGFR than those without metabolic syndrome. Patients in the metabolic syndrome group had a higher prevalence of hypertension, diabetes mellitus, dyslipidemia, and chronic kidney disease than those in the nonmetabolic syndrome group.
Among obese patients, 1,556,983 (49.0%) patients had metabolic syndrome, and among nonobese people, 1,082,101 (16.1%) patients had metabolic syndrome. The number of people with 1, 2, 3, 4, and 5 components of metabolic syndrome was 2,613,989 [26.4%], 2,087,110 [21.1%], 1,441,186 [14.6%], 857,664 [8.7%], and 340,234 [3.4%], respectively.
Metabolic syndrome, its components, and the risk of thyroid cancer according to obesity
The mean follow-up period for the 9,890,917 subjects was 7.2 ± 0.8 years, and a total of 77,133 thyroid cancer cases were newly identified in the study period. The metabolic syndrome group had a higher risk of developing thyroid cancer than the nonmetabolic syndrome group, after multivariate adjustment (HR 1.15 [CI 1.13–1.17]). When we analyzed each component of metabolic syndrome and the risk of thyroid cancer, we further adjusted the other four metabolic syndrome components. As a result, high waist circumference, high blood pressure, and low HDL-C showed a significant association with the incidence of thyroid cancer (Fig. 1 and Supplementary Table S1).
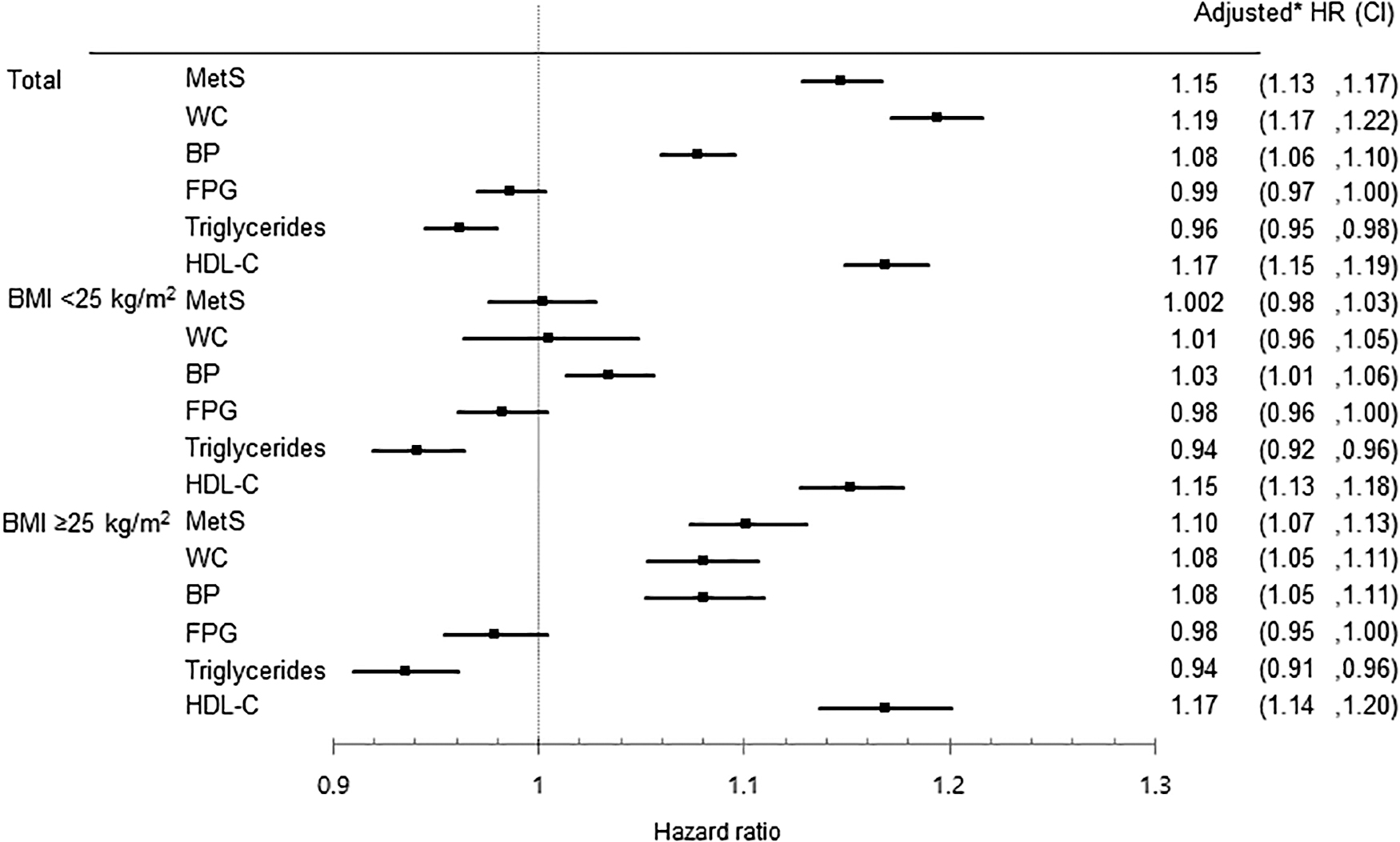
HRs and CIs of thyroid cancer risk according to metabolic syndrome and its components compared with those who do not have metabolic syndrome or its components. *Adjusted for age, sex, smoking status, alcohol consumption, physical activity, income, and chronic kidney disease. BMI, body mass index; BP, blood pressure; CI, 95% confidence interval; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; HR, hazard ratio; WC, waist circumference.
In addition, we analyzed the effect of metabolic syndrome on the development of thyroid cancer according to obesity. Metabolic syndrome was associated with an increased risk of thyroid cancer in the obese group (HR 1.10 [CI 1.07–1.13]), but the results were not significant in the nonobese group (HR 1.002 [CI 0.98–1.03]). There was a significant interaction between metabolic syndrome and obesity (p for interaction = 0.017). The effect of metabolic syndrome on the risk of thyroid cancer differs according to obesity.
High blood pressure and low HDL-C are associated with thyroid cancer risk in both obese and nonobese groups. High waist circumference was associated with thyroid cancer risk only in the obese group.
The number of metabolic syndrome components and incidence and risk of thyroid cancer according to obesity
Using the cumulative incidence competing risk methods, Figure 2 presents the incidence probability of thyroid cancer according to the number of metabolic syndrome components compared with the group without any components. The higher the number of metabolic syndrome components, especially four or more, increased the risk of developing thyroid cancer during the follow-up period.
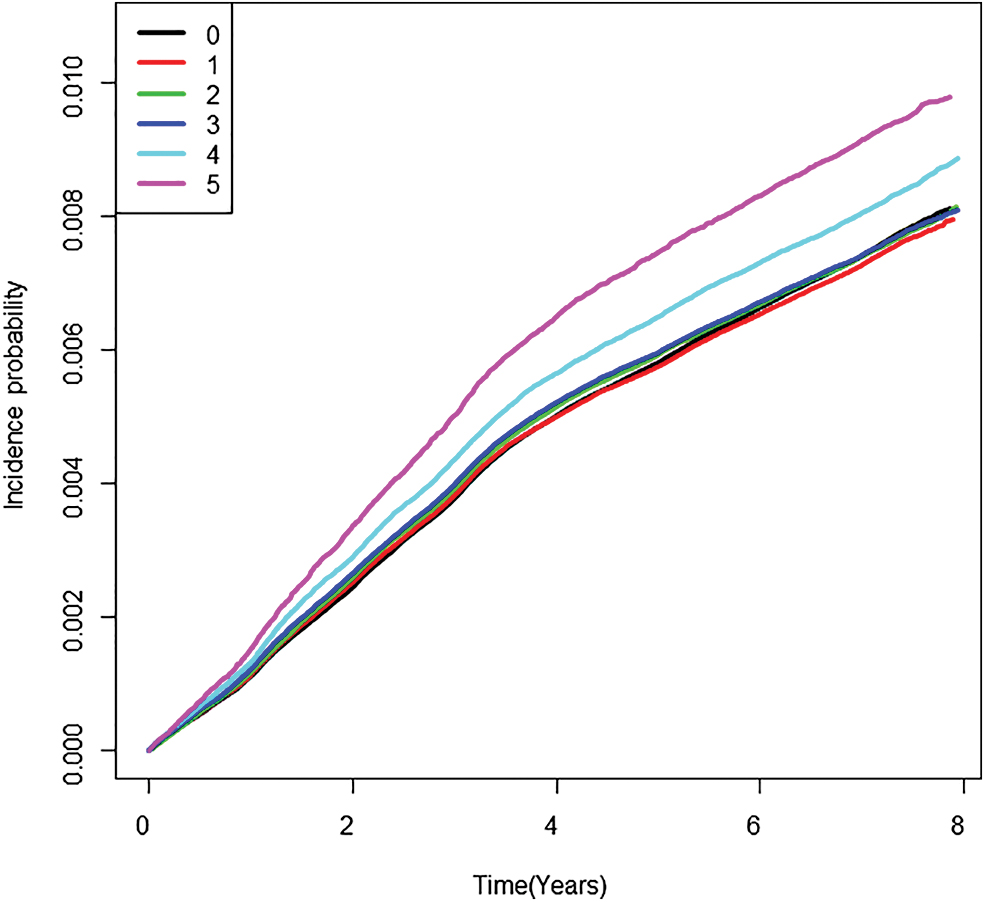
The cumulative incidence probability of thyroid cancer for up to eight years according to the number of MetS components, using the cumulative incidence competing risk method. MetS, metabolic syndrome. Color images are available online.
Figure 3 and Supplementary Table S2 show the longitudinal associations between the number of metabolic syndrome components and thyroid cancer incidence. The HR for the incidence of thyroid cancer gradually increased with the number of metabolic syndrome components (p for trend <0.001). People with all five components had a 39% higher risk than those without any components (model 2, HR 1.39 [CI 1.33–1.44]). The analysis according to obesity showed that the risk of thyroid cancer increased with an increase in the number of metabolic syndrome components in the obese group (p for trend <0.001), but not in the nonobese group.
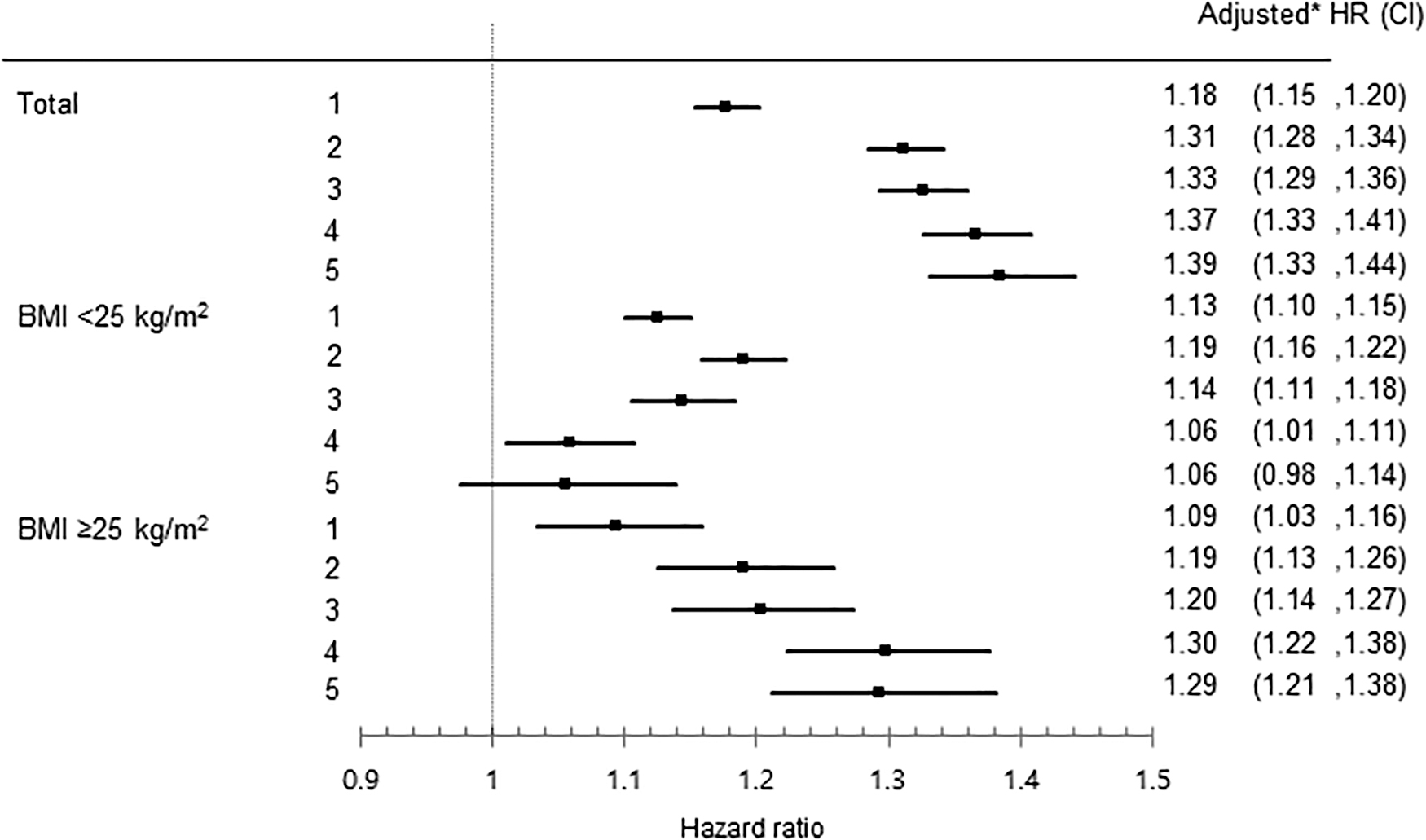
HRs and CIs of thyroid cancer risk according to the number of metabolic syndrome components compared with those who do not have any component. *Adjusted for age, sex, smoking status, alcohol consumption, physical activity, income, and chronic kidney disease.
People with one to four metabolic syndrome components were at higher risk for thyroid cancer in both obese and nonobese groups than those without any component. Those with all five components had a higher risk of thyroid cancer than those without any components in the obese group (HR 1.29 [CI 1.21–1.38]). However, in the nonobese group, those with all five components did not show an increased risk of thyroid cancer compared with those without any component (HR 1.06 [CI 0.98–1.14]). There was a significant interaction between the number of metabolic syndrome components and obesity (p for interaction <0.0001).
Combined effects of metabolic syndrome status and obesity on the risk of thyroid cancer
Figure 4 shows the risk of thyroid cancer according to the combination of metabolic syndrome status and obesity, after adjusting for multiple covariates. In both men and women, people with obesity or metabolic syndrome had a significantly higher risk of thyroid cancer than those without obesity and metabolic syndrome. In both groups with and without metabolic syndrome, the obese group had an increased risk of thyroid cancer than the nonobese group. In the nonobese group, both men and women with metabolic syndrome had a higher risk of thyroid cancer than those without metabolic syndrome. However, in the obese group, the effect of metabolic syndrome on the risk of thyroid cancer was different between men and women. Namely, the combined effect of obesity and metabolic syndrome on the risk of thyroid cancer was significant in men but not in women. Men with obesity and metabolic syndrome were the highest, with a 58% higher risk of thyroid cancer when compared with people without obesity and metabolic syndrome (HR 1.58 [CI 1.52–1.64]). On the contrary, obese women with metabolic syndrome did not have a higher risk of thyroid cancer than obese women without metabolic syndrome.
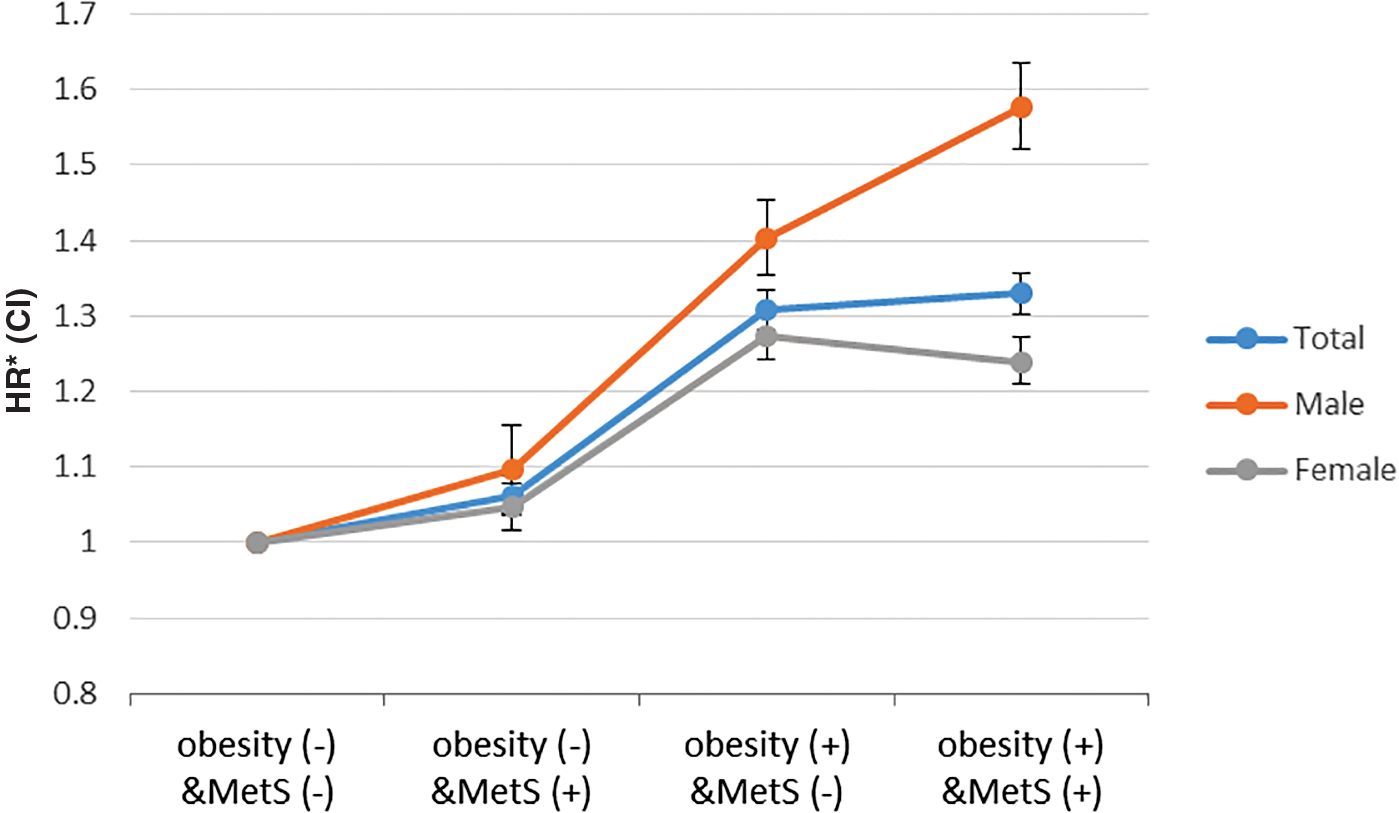
Combined effects of metabolic syndrome and obesity on the risk of thyroid cancer. *Adjusted for age, smoking status, alcohol consumption, physical activity, income, and chronic kidney disease. Color images are available online.
Discussion
This nationwide population-based, large-scale, cohort study revealed that metabolic syndrome was associated with an increased risk of developing thyroid cancer. The risk of thyroid cancer was higher in those who had a greater number of metabolic syndrome components than those without any component. The effect of metabolic syndrome on the risk of thyroid cancer differs according to obesity, which was more significant in the obese group than in the nonobese group. The combined effect of metabolic syndrome and obesity on the risk of thyroid cancer was significant in men and not in women.
To our knowledge, this is the first study to demonstrate that metabolic syndrome may be a risk factor for thyroid cancer. Especially in obese patients and men, the impact of metabolic syndrome on the risk for thyroid cancer can be significant. Therefore, more attention should be paid to the detection of thyroid cancer in these patients with metabolic syndrome. Moreover, this association is important because metabolic syndrome is a modifiable risk factor that can be improved by healthy lifestyle behaviors, such as physical exercise and balanced diets (23).
There is limited prior evidence regarding the impact of metabolic syndrome on the risk of thyroid cancer development. Most of the previous studies evaluated the association between BMI and the risk of thyroid cancer without considering the metabolic status associated with obesity (8 –13). To the best of our knowledge, only one case/control study, one cohort study, and one systematic review have been performed. These studies did not reveal any relationship between metabolic syndrome and thyroid cancer (15 –17). The case/control study by Balkan et al. recruited 41 patients with diffuse thyroid cancer and 41 euthyroid patients with nodular goiter who underwent surgery as a control group (16). They reported that metabolic syndrome was not a significant risk factor for thyroid cancer following logistic regression analysis (p > 0.05). The cohort study by Almquist et al. included people without thyroid cancer (15). They followed 578,700 people for an average of 12 years, and 388 patients developed thyroid cancer. They reported that there was no association between metabolic syndrome and thyroid cancer. Accordingly, the systematic review on the association between thyroid cancer and metabolic syndrome could not conclude whether metabolic syndrome is a risk factor for thyroid cancer, because there were only two eligible studies with heterogeneous study subjects (17).
Therefore, we conducted a large-scale, nationwide, population-based, cohort study targeting the entire Korean population. We followed 9,890,917 people from the general population for an average of 7.2 years, of which 77,133 patients developed thyroid cancer in the study period. Our study is the first to demonstrate that metabolic syndrome is associated with an increased risk of thyroid cancer.
In our study, each component of the metabolic syndrome was associated with an increased risk of thyroid cancer, which further supports the association between metabolic syndrome and thyroid cancer. Previous studies have reported the association of thyroid cancer with central obesity (24), hypertension (17), hyperglycemia (17), and dyslipidemia (25). These results suggest that metabolic syndrome and its components may contribute to the pathophysiology of thyroid cancer and act as a risk factor for thyroid cancer.
Although there are few studies on metabolic syndrome and thyroid cancer, there are several studies on metabolic syndrome and thyroid nodules. These studies showed that patients with metabolic syndrome had increased risk and size of thyroid nodules (26 –28). These studies may be the basis for the association of metabolic syndrome with thyroid cancer.
Several biologic mechanisms may explain the link between metabolic syndrome and thyroid cancer. The suggested mechanism is, first, that thyrotropin (TSH) is involved in mitogenic pathways of the thyroid gland (29) and suppresses apoptotic cell death (30). Increased serum TSH levels may stimulate thyroid cell proliferation and growth, increase mutation, and promote the development of thyroid cancer (31 –33). Second, insulin resistance is a key factor in the pathophysiology of metabolic syndrome and may be a potential risk factor for thyroid cancer. Insulin resistance and hyperglycemia increased proliferation, angiogenesis, cellular mobility, apoptosis, and damage to DNA molecules by active oxygen forms due to excess glucose (34 –36). Third, insulin-like growth factor-1 (IGF-1), IGF-2, and insulin receptors, which are overstimulated in metabolic syndrome due to insulin resistance, may play a role in thyroid carcinogenesis (37 –39). Fourth, cytokines and bioactive molecules associated with visceral fat and immune cells, such as tumor necrosis factor α, interleukin-6, monocyte chemotactic protein-1, plasminogen activator inhibitor, retinal binding protein-4, leptin, visfatin, and resistin (39), can affect the risk of cancer. Fifth, these molecules are responsible for the low-grade chronic and systemic inflammation, and may affect the increased risk of thyroid cancer (38,40). Sixth, circulating estradiol may be another mechanism for thyroid carcinogenesis. Adipocytes produce estrogens via aromatase activity, and obesity is associated with a high level of estradiol (41). Estrogen is a potent growth factor for malignant thyroid cells (42).
Most of these mechanisms are also related to obesity. Thus, in our study, the effect of metabolic syndrome on thyroid cancer was significant in the total population and the obese group, but not in the nonobese group. Interestingly, the combined effects of metabolic syndrome and obesity on the risk of thyroid cancer were particularly prominent in men. The findings indicate that both metabolic syndrome and obesity may play a more important role in the development of thyroid cancer in men than in women. This may be caused by gender differences in sex hormones. The conversion of androstenedione to estrone in the adipose tissue is the main source of estrogen in men and postmenopausal women (43). Previous studies have shown that the association between obesity and thyroid cancer is more significant in men than in women (17). Moreover, sex differences in fat distribution can make a difference in the development of thyroid cancer. Men predominantly store fat in the visceral area, while women tend to store fat predominantly in the gluteal/femoral region (44). In addition, recent studies addressing the different roles of upper and lower body fat in metabolism have suggested that lower body fat may have disease-protective effects (45,46). Nevertheless, the mechanisms that link these two pathological conditions remain uncertain. Further research is needed to understand the mechanism of the association between metabolic syndrome and thyroid cancer.
Our study has several strengths. First, this was a large-scale, nationwide, cohort study using the NHIS database, which included the entire South Korean population. Our study provides the first evidence that metabolic syndrome and its components are risk factors for thyroid cancer in the general population. Second, this cohort study used systematically and longitudinally collected measurements and laboratory data at the individual level before the incidence of thyroid cancer. Third, we excluded patients who were previously diagnosed with thyroid cancer and identified patients with new-onset thyroid cancer, thus minimizing the reverse causality.
This study has certain limitations. First, there is a possibility of selection bias in the study subjects. All Koreans have the benefit of undergoing medical evaluation every two years, but it is voluntary and not compulsory. Second, we could not consider the histologic subtype, stage, and size of thyroid cancer due to lack of data. Third, we could not use the dietary factors that may be potentially related to metabolic syndrome and its components. Moreover, we could not consider the influence of the duration of metabolic syndrome on the risk of thyroid cancer.
In conclusion, this nationwide cohort study provides evidence for the association between the presence of metabolic syndrome and the development of thyroid cancer, particularly in obese patients. Further research is required to elucidate the possible mechanisms underlying this association. Since metabolic syndrome is a modifiable risk factor, further studies are warranted to determine the effect of metabolic syndrome control on reducing the risk of thyroid cancer.
Footnotes
Data Availability Statement
According to the Korean law, we are not allowed to transfer any data files to a third party. However, data are available from the Korea National Health Insurance Sharing Service Institutional Data Access/Ethics Committee (
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Korea University Ansan Hospital Grant (K1923571). No funding bodies had any role in study design, data collection and analysis, decision to publish, or preparation of the article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2