
Abstract
Introduction:
Thyroid cancer is one of the most common carcinomas diagnosed in adolescents and young adults, with a rapidly rising incidence for the past three decades. Surgery is the standard treatment for patients with differentiated thyroid carcinoma (DTC), and when indicated, followed by radioactive iodine (RAI) treatment. The aim of this study was to evaluate the possible effects of RAI therapy on ovarian function and fertility in women.
Methods:
The PubMed, Embase, and Web of Science databases were systematically searched up to January 2020. In addition, a meta-analyses were performed for anti-Mullerian hormone (AMH) levels after RAI, comparison of AMH levels prior and 1 year after RAI, and pregnancy rates in patient with thyroid cancer receiving RAI compared with patients with thyroid cancer who did not receive RAI.
Results:
A total of 36 studies were eligible for full-text screening and 22 studies were included. The majority of the studies had a retrospective design. Menstrual irregularities were present in the first year after RAI in 12% and up to 31% of the patients. Approximately 8–16% of the patients experienced amenorrhea in the first year after RAI. Women who received RAI treatment (median dose 3700 MBq [range 1110–40,700 MBq]); had menopause at a slightly younger age compared with women who did not receive RAI treatment, 49.5 and 51 years, respectively (p < 0.001). Pooled AMH of the seven studies reporting AMH concentrations after RAI was 1.79 ng/mL. Of these, four studies reported AMH concentrations prior and 1 year after RAI. The mean difference was 1.50 ng/mL, which was significant. Finally, meta-analysis showed that patients undergoing RAI were not at a decreased risk of becoming pregnant.
Conclusions:
Most of the studies indicate that RAI therapy for DTC is not associated with a long-term decrease in pregnancy rates although meta-analyses show a significant decrease in AMH levels after RAI therapy. Prospective studies are needed to confirm these results. We recommend counseling patients about the possible effects of 131I and incorporate today's knowledge in multidisciplinary counseling.
Introduction
Thyroid carcinoma is the most common endocrine malignancy and its incidence is rapidly rising. In The Netherlands, the incidence has doubled from 340 new patients in 1990 to around 700 in 2018 (1). This increase was more extensive than what would be expected based on population growth and aging. Among adolescents and young adults (AYAs) between 15 and 39 years, thyroid carcinoma is the fifth most frequent type of cancer (2). It occurs more frequently in women than in men and it is most often diagnosed in females at the age of 30 and 39 years (3). Papillary and follicular thyroid carcinomas are referred to as differentiated thyroid carcinomas (DTC) and they comprise about 80–85% of all thyroid tumors. The prognosis of DTC is excellent with a 5-year survival rate near 100% for localized stage and 96% for locoregional disease with lymph node metastasis (4).
Surgery is the standard treatment for patients with DTC, and when indicated this is followed by radioactive iodine (RAI) treatment. Despite international movements toward less aggressive treatment, many guidelines still recommend a total thyroidectomy followed by RAI in all patients with a DTC >1 cm (5). This treatment strategy is associated with significant morbidity rates due to hypothyroidism, hypoparathyroidism, recurrent laryngeal nerve damage, dysgeusia, and xerostomia, resulting in long-term poor quality of life (QoL) (6). The excellent prognosis of DTC suggests overtreatment of a large group of patients with DTC. Many studies are now focusing on de-escalation and selecting patients in whom aggressive management is not warranted.
One of the concerns of the current protocols is the widespread use of RAI for the postsurgical treatment of DTC and its possible effect on reproductive function and fertility in the AYA population. There is growing awareness that temporary or permanent impaired fertility due to cancer treatment may have an important impact on the QoL in young adults. Many cancer survivors desire to have children in the future and prefer their physician to raise fertility issues proactively (7).
In the past, two systematic reviews concerning the effect of RAI therapy on fertility in young women have been performed. These two reviews (performed in 2008 and 2011) concluded that there is limited observational evidence suggesting persistent (>12 months) adverse effects of RAI treatment on gonadal function, fertility, or pregnancy. However, a slightly younger age at menopause was seen in patients treated with RAI.
All of the studies included in both these reviews were retrospective and the majority involved a small number of patients (8,9). New studies have been published for the past decade focusing on the effects of RAI on ovarian function by evaluating the anti-Mullerian hormone (AMH) levels in women (10 –14). AMH is strongly correlated with antral follicle count and this may be a tool to measure fertility status (15).
By incorporating studies performed after 2011, our aim was to summarize the current best evidence regarding fertility risks in young female thyroid cancer survivors treated with RAI. This will enable clinicians to counsel these women about their risks and potential indication for fertility preservation.
Methods
This systematic review was performed according to the guidelines of the requirements of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist (Supplementary Data S1) (16).
A systematic literature search was performed through Pubmed, Embase, and Web of Science on the 5th of January 2020. Search terms were formulated using the PICO structure and were reviewed by an experienced librarian. Patients (P) included young adult women who underwent treatment for DTC in their fertile years. Intervention (I) included a total thyroidectomy followed by RAI therapy. Comparisons (C) consisted of either women who only had a total thyroidectomy or healthy women. Outcomes (O) included ovarian reserve or function, AMH levels, fertility, menstrual cycle disorders, menopause, and pregnancy outcomes. Database subject terms, such as Mesh terms (Medline) and Emtree terms (Embase), were used when appropriate. Keywords included thyroid carcinoma, thyroid tumor, thyroid papillary carcinoma, thyroid neoplasms, thyroid cancer and RAI, iodine, radioisotope, iodine radioisotopes, 131I and fertility, Mullerian inhibiting factor, follicle stimulating hormone, gonadotropins, follitropin, infertility, pregnancy, spontaneous abortion, menstrual cycle, and menstruation disorder. Detailed search queries are reported in Supplementary Data S2.
Selection of studies
The identified titles were entered in Rayyan QRCI (17) and screened by two independent reviewers based on title and abstract. Subsequently, full-text review of potentially relevant studies was performed, and studies were selected if eligibility criteria were fulfilled (M.W.P. and E.L.P.). Original studies assessing the effects of RAI therapy for DTC on female gonads, AMH levels, menstrual cycles, and pregnancy outcomes were included. Case reports and reviews were excluded. Selection of articles was restricted to English, Dutch, German, and French. Studies published after 1970 were included in this review.
Disagreements were resolved by consensus and when unsuccessful, with the help of a third reviewer (I.M.C.P.). The reason for exclusion of articles were recorded. All included studies were cross-referenced for additional relevant articles. (Supplementary Fig. S1).
Risk of bias
The ROBINS-I tool was used to evaluate the quality of each eligible study (18). The entire scale constituted seven domains for the risk of bias; confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result. Each domain was judged for three levels of bias: low, moderate, or high risk of bias. Full assessment criteria can be found in Supplementary Data S3.
Statistical analysis
Meta-analysis was performed to determine differences in pregnancy rates with 95% confidence intervals (CIs). Pooled postoperative pregnancy rates were determined using random effects model and odds ratio (OR) with CI was used to assess whether patients undergoing RAI were at a decreased risk of becoming pregnant. In addition, meta-analysis was performed to determine AMH levels after RAI. The meta-regression analysis of the different AMH levels were corrected for the follow-up period. Subgroup analysis in studies was performed to compare AMH levels before and 1 year after RAI using mean differences and random effects model. Missing standard deviations from studies were imputed and all meta-analyses were performed using random effects model. p-Values <0.05 were considered statistically significant.
All calculations were performed using RStudio 1.2.5001 (with R version: x64 3.6.3). In addition, statistical packages meta and metaphor were used for all computations of the meta-analyses. Visualization of plots was done using the ggplot2 package.
Results
After excluding duplicates, 689 references were retrieved for review of title or abstract. Thirty-eight articles were selected for review of the full text and 22 were selected for this review (Supplementary Fig. S1) including 36,215 patients. Study characteristics of the included studies are reported in Table 1. The majority of studies were based on single center patient populations and performed retrospectively.
Study Characteristics of Included Studies
Mean age at diagnosis.
Dosages in mCi were converted to MBq.
Oxford Level of Evidence (50).
Mean age not mentioned.
HT, hemi thyroidectomy; LT4, levothyroxine (thyroid hormone); RAI, radioactive iodine; TT, total thyroidectomy.
Four studies focused on the effects of RAI therapy on female gonadal function (i.e., amenorrhea, menstrual cycle irregularities, estrogen/progesterone levels, and the age of menopause) (Table 2). Seven studies reported AMH levels in patients with DTC after receiving RAI therapy (Table 3). Fourteen studies evaluated pregnancy outcomes after RAI therapy (Table 4). Some studies focused on multiple outcome measures such as AMH levels and gonadal effects of RAI therapy.
Radioactive Iodine Treatment and Ovarian Function
Significant difference between the RAI- and the control group.
n, number; n.a., evaluation not done.
Effect on Anti-Mullerian Hormone Levels
Significance for paired comparisons relative to baseline.
Significance among groups.
AMH levels were significantly higher before than after RAI therapy.
AMH, anti-Mullerian hormone; CV, coefficient of variation; n.a., evaluation not done.
Radioactive Iodine Treatment and Pregnancy Outcomes
Significant difference between the RAI- and the no RAI group.
Dosages in mCi were converted to MBq.
Scanning RAI = low-dose RAI (≤5 mCi) and ablative RAI = high-dose RAI (>5 mCi).
The ablation dosage was 1.1 or 3 GBq (30 or 80 mCi) and the therapeutic dosage was 8.5–59 GBq (229–1595 mCi).
CI, 95% confidence interval; HR, hazard ratio; NS, no significant differences between the two groups.
Risk of bias assessment
The result of the ROBINS tool revealed that all the included studies were of sufficient quality based on risk-of-bias domains and applicability domains (Supplementary Fig. S2). Specific assessment for each of the studies included in this systematic review and meta-analysis can be found in Supplementary Data S4.
RAI treatment and ovarian function
Four studies focused on the gonadal effects of RAI therapy (Table 2). All studies were observational and in only one study prospective data were collected. The age at first RAI treatment varied from 8 to 45 years and the cumulative dosages of RAI varied from 2997 MBq to 59 GBq (81 to 1595 mCi). In the study by Vini et al., 496 women <40 years were included (19). A full obstetric history was taken and details of the menstrual cycle were noted in the first 2 years after treatment (surgery followed by radioiodine). Menstrual cycle irregularities comprising either lighter menses or changed duration of cycle were documented in 12% of the patients in the first year after RAI. Amenorrhea was depicted in 8% of the patients lasting between 4 and 10 months. Ceccarelli et al. retrospectively compared the menopausal age of DTC patients treated with RAI and suppressive levothyroxine (LT4) (n = 130) with the menopausal age of patients with a goiter (n = 127) treated with suppressive LT4. The first group of women experienced menopause at a slightly younger age than women who did not receive RAI treatment (49.5 vs. 51 years, p < 0.001) (20). Sioka et al. compared 45 females <40 years old who had received RAI therapy for DTC to age-matched control females (n = 83). Significantly more menstrual cycle alterations were seen during the first year after RAI therapy in the group of patients compared with the control group (31.1% vs. 14.5%, p = 0.02) (21).
Acibucu et al. prospectively compared 45 women who received RAI ablation treatment for well-differentiated thyroid cancer in their premenopausal period to 49 healthy females as controls. Transient oligo/anovulation was detected in seven patients (15.6% of the patient group) after RAI treatment (11).
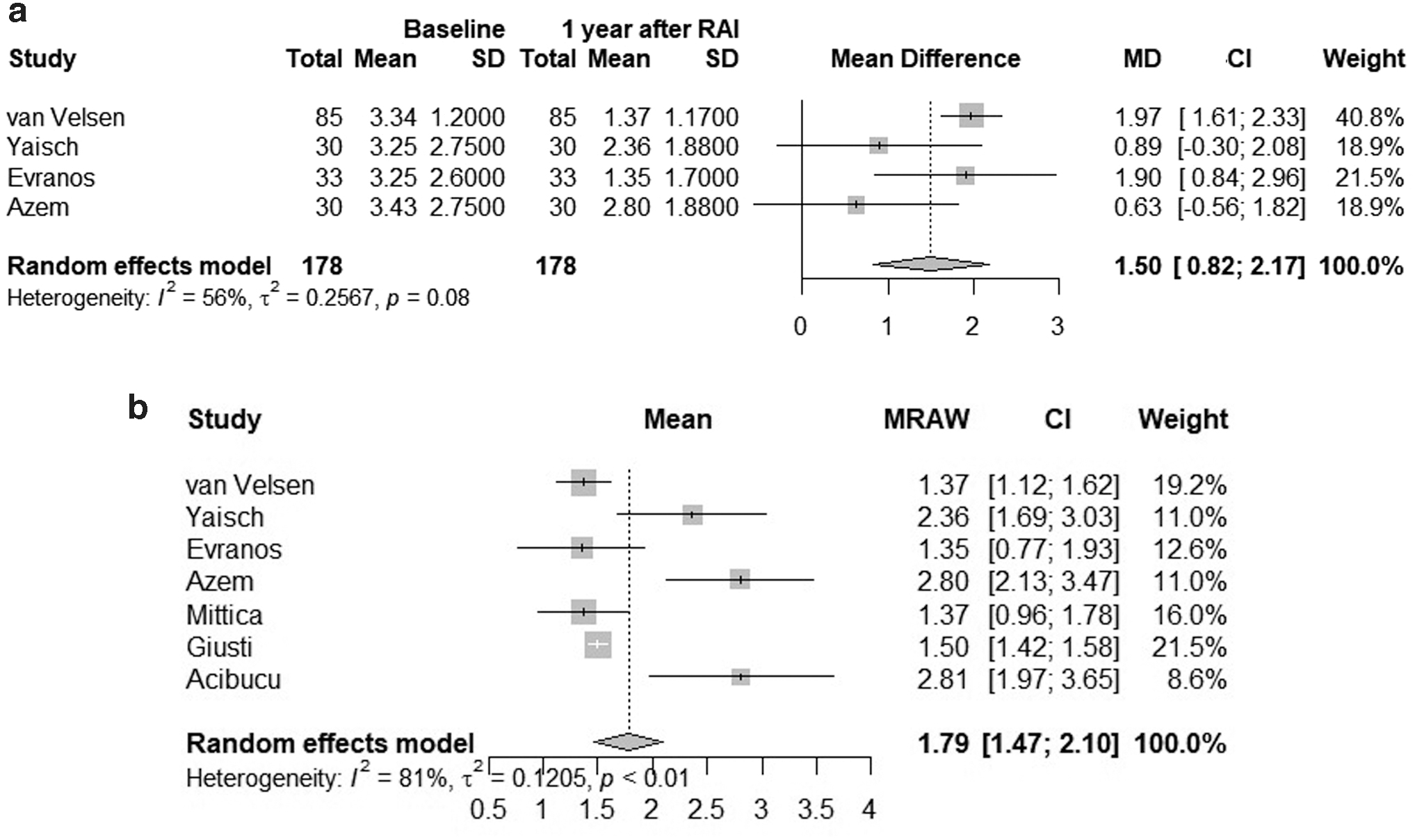
Seven studies examined the effect of RAI treatment on the ovarian reserve by assessing AMH levels after RAI treatment (Table 3) (9 –13,22,23). Yaisch et al. studied 30 women with DTC whom received RAI doses ranging from 1110 to 5550 MBq (30 to 150 mCi) after recombinant human thyrotropin stimulation. RAI treatment resulted in a significant decrease in AMH concentrations at 3 months. Eighty-two percent of the women had final values below baseline levels at 1 year (3.25 ng/mL at baseline and 2.36 ± 1.88 ng/mL after 1 year; p < 0.005). The studies of Azem and Shefer and Evranos et al. confirm these results. In the study of Azem and Shefer, 30 premenopausal women were included who underwent RAI treatment for DTC (dose range 1110–5550 MBq [30–150 mCi]). In the study of Evranos et al., 33 premenopausal women were enrolled who received a high dose of RAI (range 2775–5550 MBq (75–150 mCi). Both studies state that large doses of RAI as adjunct therapy to women with DTC appear to impair ovarian reserve as assessed by AMH levels (Table 3). The lowest point in AMH levels is seen at 3 months after treatment and there is no complete recovery at 1 year. In contrast, lower dosages up to 1110 MBq (30 mCi), such as given for ablation of thyroid remnants, appear to be innocuous.
In the study of Acibucu et al., AMH levels of 45 patients after (mean follow-up of 44 months) receiving RAI therapy for DTC were compared with the AMH levels of 40 healthy females. The difference in AMH levels between the patient- and control group was found to be significantly different (2.28 vs. 3.35 ng/mL, p = 0.038). An important drawback of this study is that the AMH levels before RAI treatment were not reported.
Recently, van Velsen et al. conducted a prospective study evaluating AMH levels after RAI for thyroid cancer in female patients (22). AMH concentrations decreased by 50% compared with baseline levels until 12 months after a single RAI treatment and then stabilized. Patients <35 years had a gentler decrease in AMH levels. The authors suggested a less aggressive RAI treatment in low-risk patients, in particular women >35 years with an active child wish.
Giusti et al. found no statistically significant relationship between RAI exposure and AMH levels. They found that AMH levels were only negatively correlated with age in the treatment group (rS −0.58; p = 0.0003) and in the control group (rS −0.81 p < 0.0001). Mittica et al. performed a cross-sectional study comparing 59 women who underwent surgery and RAI for DTC, 30 women only receiving surgery and 141 healthy women (23). In this study, the main factor for lower AMH levels was also age and not the type of treatment.
Despite the reduction in AMH levels, the correlation between AMH levels and fertility was not evident. The study of Evranos et al. reports that AMH levels did not differ among patients with a pregnancy wish, patients without an active child wish and pregnant patients (p > 0.05) (12).
This section indicates that in the first year after RAI therapy women experienced more menstrual cycle irregularities compared with control groups. In four studies, the AMH levels were significantly lower 1 year after RAI treatment compared with baseline levels (mean difference 1.50 ng/mL [CI: 0.82–2.17], see Fig. 1a). Pooled AMH levels of patients undergoing RAI was 1.79 ng/mL (Fig. 1b). The time of AMH measurement after RAI was not a predictor for the level of AMH (OR 0.93 [CI 0.80–1.08]; p = 0.355).
RAI treatment and pregnancy outcomes
Several studies reported on the effects of RAI therapy in women on subsequent pregnancy rates (Table 4) (21,24 –26). Two studies report increased rates of spontaneous and induced abortions in the first year after RAI therapy in 17–18% of the pregnancies (27,28). Fard-Esfahani et al. report an increased incidence of abortions early after the administration of RAI therapy from 16.83% before RAI to 26.19% after RAI (29). However, this increase was related to induced abortions while the risk for spontaneous abortions was reduced from 16.8% to 10.3%. There is little observational evidence that RAI treatment was associated with significantly increased risk of spontaneous abortions. Long-term infertility or neonatal mortality were comparable with various control groups (30,31). Most authors do recommend to avoid pregnancy for at least 1 year after RAI therapy to reduce the possible adverse effects of radiation on gonads and subsequently on the neonates (29,30).
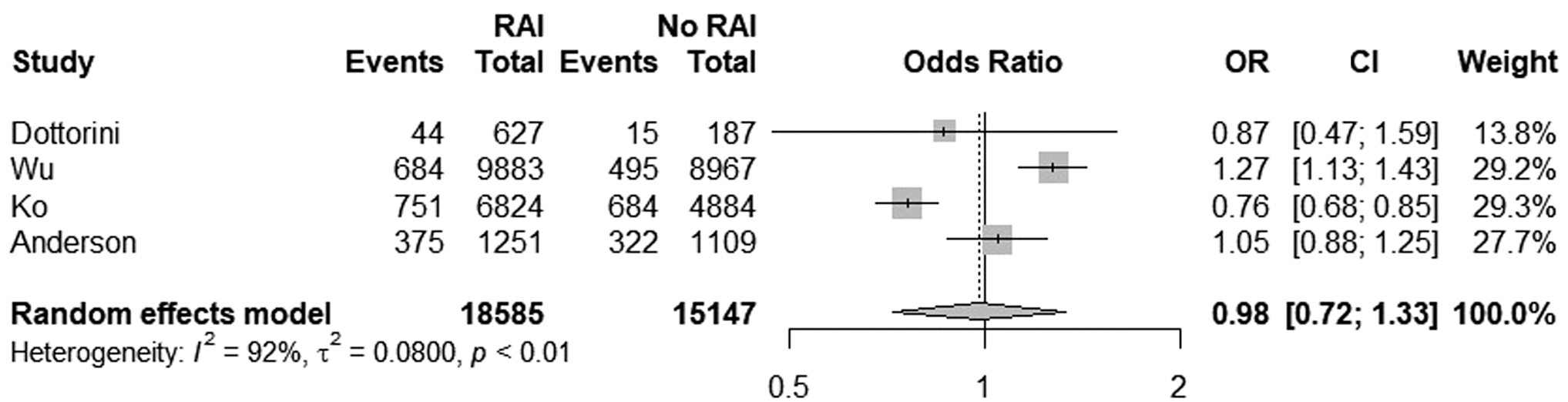
Three large clinical studies were performed to evaluate the effect of RAI therapy on pregnancy rates (32 –34). The study of Ko et al. involved 11,708 women with a mean age of 37.1 years with DTC. The mean follow-up period was 6.4 years. The overall incidence of pregnancy was significantly lower in the RAI cohort (adjusted hazard ratio [HR] = 0.77 [CI: 0.70–0.86], P < 0.001) also after stratification for age (HR = 0.73 [CI: 0.64–0.83], P < 0.05 in 25–34 years; HR = 0.63 [CI: 0.49–0.82], P < 0.05 in 35–44 years). In 2015, Wu and coworkers reported on a large cohort of patients (18,850 women) with DTC using the California Cancer registry with a median follow-up of 4.1 years (31). In a subgroup analysis, the birth rate in women aged 35–39 years who received RAI was significantly lower than in patients who did not receive RAI (11.5 vs. 16.3 births per 1000 woman-years, p < 0.001). They also observed a delay to first live births in women aged 20–39 years (34.5 vs. 26.1 months; p < 0.0001).
This is in contrast to the study of Anderson et al. that described 2360 women, in whom 53% of the patients received RAI treatment. The cumulative incidence of birth at the end of follow-up (maximum 14.5 years) was 30.0% in the RAI cohort compared with 29.3% in the non-RAI group. In this observational cohort, treatment with RAI was thus not associated with a reduced birth rate. The study of Metallo et al. confirms these findings in 54 women and states that the pregnancy rates and the frequency of miscarriages in the RAI cohort are consistent with the French general population (35). Figure 2 showed that patients undergoing RAI were not at a decreased risk of becoming pregnant compared with control group (OR 0.98 [CI: 0.72–1.33]; p = 0.909).
Differences in pregnancy rates between patients undergoing RAI and patients not undergoing RAI.
This section indicates that RAI therapy was not associated with long-term infertility and neonatal mortality.
Dosage RAI therapy and fertility
In total, three studies found a negative relationship between the dosage of RAI therapy and fertility. Vini et al. states that higher dosages of RAI (8473 MBq–59 GBq [229–1595 mCi]) are associated with more menstrual cycle irregularities compared with the group who received lower dosages of RAI. Azem and Shefe found that high dosages of RAI given as a therapeutic dosage in patients with DTC, impair ovarian reserve as assessed by AMH levels. Van Velsen et al. found that after multiple RAI procedures, a further reduction of AMH levels was seen up to 85% of baseline levels in 4 years' time (baseline AMH 3.34 ± 1.20; after 48 months AMH 0.95 ± 1.23 [p < 0.05]) (22).
However, four other studies did not detect an association between the RAI dosage and the extent of AMH reduction. Ceccarelli et al. found no relationship between menopausal age and the cumulative RAI dosage received. The studies of Chow et al. and Balenović et al. show that a higher ablative dosage (>2960 MBq (80 mCi) and >3700 MBq (100 mCi) did not significantly alter the pregnancy outcome. Metallo et al. found the frequency of miscarriages was 17% in females from the group receiving >3848 MBq (104 mCi) and 10% in patients with a cumulative RAI dosage <3848 MBq (104 mCi). No birth defects or first year mortality was observed.
This section indicates that the association between RAI dosages and fertility is still controversial.
Discussion
In this systematic review including 22 studies, we evaluated the effect of RAI therapy on ovarian function and fertility in women with DTC who received RAI treatment in their reproductive years. An overview of the currently available literature is provided, enabling clinicians to counsel these women about their risks and potential indication for fertility preservation.
Most of the selected studies indicate that RAI therapy for DTC is not associated with a long-term decrease in pregnancy rates. However, in the first year directly after RAI treatment many women experienced irregularities in their menstrual cycle and some studies found significant lower AMH levels, both possibly leading to a diminished fertility shortly after 131I treatment for DTC. Thus, it might be most prudent for women with an active child wish in their later reproductive years to have counseling of treatment potential effects. This review also shows that women treated with RAI therapy were exposed to menopause at a slightly younger age than women without RAI treatment.
In recent years, AMH has become an outcome of interest as a possible predictor of ovarian reserve (14). In normo-ovulatory women, the serum AMH level is positively correlated with the number of oocytes retrieved (R = 0.6, p < 0.0001) (34). This correlation is of current value in women who undergo in vitro fertilization (IVF) or hyperstimulation to harvest a fair amount of ovarian eggs. The studies included in this review evaluating AMH as a representative of ovarian reserve were prospective with a small number of patients, the majority of included patients did not receive a high dosage or multiple 131I treatments and the follow-up time was relatively short. Nonetheless, these studies suggest a direct relationship to AMH levels and fertility. There are other insights in the literature on this topic. Liebenthron et al. studied the relation between AMH serum levels and follicle densities (FD) and concluded that this hypothesis should be looked at with suspicion (36). In this retrospective study, 830 women treated for several types of malignant (n = 806) and benign (n = 24) diseases were observed who cryopreserved tissue in a single center and in whom AMH levels were tested before and after gonadotoxic therapies. AMH and FD were not correlated in women ≤20 years and weakly to moderately correlated in women 21–40 years (r = 0.24–0.39). It was stated that AMH should be carefully used to estimate ovarian reserve of female cancer patients, especially when used as a single factor.
It must be taken into account that the outcomes of the studies mentioned in this review regarding pregnancy rates, menstrual irregularities, and AMH levels might all be more or less influenced by differences in study design and study population. For example; a 45-year-old woman in Taiwan, a country known for low birth rates due to low socioeconomic circumstances, is expected to have lower AMH levels, an irregular menstrual cycle, and thus a lower chance of pregnancy (32). However, one study has taken these normal biological features into account and still found remarkable differences in favor of women who did not receive 131I treatment (34).
Recently van Velsen et al. investigated the influence of the diagnosis and treatment of thyroid cancer on the desire to have a child (22). In total, 40% of the patients in the single RAI group and 33% of the patients in the multiple RAI group stated that their desire to have a child was influenced by the diagnosis or treatment. Most of the patients did not want a child anymore. These findings might also be an explanation for the lower birth rates in women who received RAI compared with patients without RAI treatment.
Hypothyroidism after cancer treatment is another important reason for worse reproductive outcomes (37). Previous studies show that thyrotropin (TSH) and thyroid hormones act directly on the ovary through binding to their specific receptors and have a specific function during folliculogenesis and ovulation in the healthy state (38). Chin et al. reported that women with hypothyroidism after cancer treatment were twice as likely to fail to achieve their desired family size (adjusted OR [aOR] 1.91 [CI: 1.09–3.33]) and be childless (aOR 2.13 [CI: 1.25–3.65]) (39). Total thyroidectomy causes hypothyroidism by definition and a (sub)total thyroidectomy is associated with postoperative hypothyroidism in 62–87% of cases (40). Therefore, hypothyroidism is another important factor to consider when counseling patients on the risks for impaired fertility.
However, for the past years recombinant human TSH (RhTSH) has been used to provide elevated TSH levels without making patients hypothyroid during the postsurgical follow-up. The use of RhTSH avoids the side effects of hypothyroidism and promotes iodine uptake (41). Of the included studies in this review, only one (Yaisch et al.) mentioned the use of RhTSH (10). It has been shown that TSH levels are negatively correlated with AMH levels in infertile patients. This association suggests a direct beneficial effect of normal TSH levels on follicular recruitment in infertile women (42). Also, it has been observed that TSH levels were significantly higher among women undergoing IVF who produced oocytes that failed to be fertilized (43). As the number of women treated with RhTSH is increasing it will be important to assess the effect of RhTSH on ovarian function and fertility in future studies.
Polycystic ovary syndrome (PCOS) is another heterogenous disorder affecting 6–15% of women in their reproductive years (44). The clinical features of PCOS include reproductive abnormalities such as irregular menses and infertility. It is important to consider that women with PCOS may have higher TSH levels compared with healthy control women (2.29 ± 1.24 vs. 1.86 ± 0.90 mU/L, p < 0.001) (45). There is increasing evidence that higher TSH concentrations in patients also increase the risk for thyroid cancer (46). The percentage of women with PCOS in the studies assessed for this review is not specified. However, this common endocrine disorder in young women might have been present in a percentage of patients with thyroid carcinoma in these studies, possibly leading to a higher percentage of reproductive abnormalities.
Also, it should be taken into account when interpreting the data that patients treated with total thyroidectomy may have low calcium levels. Some observational studies show that vitamin D deficiency is a risk factor for reduced fertility (47 –49). Since vitamin D and calcium status are correlated, this is another factor that should be considered, but such patients are all under close counseling and would be treated for low calcium levels when necessary.
Cancer-related issues in female cancer survivors in their reproductive years such as potential loss of fertility are distressing and for the past few years the awareness of fertility issues in these patients has grown significantly. The incidence of DTC is increasing and more young adults are confronted with such fertility issues. The age of the patients included in this review ranges from 8 to 50 years. This makes that not all the results can be directly extrapolated to the AYA population or specifically women in their reproductive years. Future clinical studies in patients with DTC should aim to collect long term patient reported data on fertility in these patient groups, providing clinicians reliable data to counsel these patients optimally.
The strengths of the review include the comprehensive search strategy, independent screening, and the risk of bias assessment. One of the limitations of this study is that not many studies have described the association of DTC treatments and fertility. However, this study does pool the studies that have described fertility into various meta-analyses showing that pregnancy rates do not change in patients undergoing RAI but AMH concentrations significantly decreases after RAI. Another limitation is that most studies describing AMH concentrations do not describe pregnancy rates and vice versa. Finally, AMH concentrations were measured in the different studies were performed using different types of assays, which could make absolute values difficult to compare. However, within the studies there still is a decrease in AMH concentrations, which means while it is possible that the concentrations might be different because of the different assays used, there still is a steady mean difference in AMH concentration after RAI. More prospective studies are needed to determine whether AMH is a clinically relevant proxy to determine fertility in patients with DTC undergoing RAI.
There is no clear evidence that young adults (AYAs), or otherwise stated all women in their reproductive years, have a long-term diminished fertility after receiving RAI for DTC. It is also not associated with a long-term decrease in pregnancy rates. There is a strong suggestion that RAI negatively influences the menstrual cycle in the first year after treatment. AMH concentrations are frequently reduced in this same period of time potentially effecting ovarian reserve and thus short-term fertility. Further prospective studies are needed. In this current time of awareness of cancer treatment side effects, we believe there is a role for physicians to inform their patients of these literature finding, and especially to counsel women >35 years with an active short-term child wish who are scheduled for RAI treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4